
Abstract
In our companion paper, we described the theoretical basis for tissue lumping in whole-body physiologically based pharmacokinetic (WB-PBPK) models and found that Kdet, a coefficient for determining the number of tissue groups of distinct transit time in WB-PBPK models, was related to the fractional change in the terminal slope (FCT) when tissues were progressively lumped from the longest transit time to shorter ones. This study was conducted to identify the practical threshold of Kdet by applying the lumping theory to plasma/blood concentration-time relationships of 113 model compounds collected from the literature. We found that drugs having Kdet < 0.3 were associated with FCT < 0.1 even when all peripheral tissues were lumped, resulting in comparable plasma concentration-time profiles between one-tissue minimal PBPK (mPBPK) and WB-PBPK models. For drugs with Kdet ≥ 1, WB-PBPK profiles appeared similar with two-tissue mPBPK models by applying the rule of FCT < 0.1 for lumping slowly equilibrating tissues. The two-tissue mPBPK model also appeared appropriate in terms of concentration-time profiles for drugs with 0.3 ≤ Kdet < 1, although, some compounds (15.9% of the total cases), but not all, in this range showed a slight (maximum of 18.9% of the total AUC) deviation from WB-PBPK models, indicating that the two-tissue model, with caution, could still be used for those cases. Comparison of kinetic parameters between traditional (model-fitting) and current (theoretical calculation) mPBPK analyses revealed their significant correlations. Collectively, these observations suggest that the number of tissue groups could be determined based on the Kdet/FCT criteria, and plasma concentration-time profiles from WB-PBPK could be calculated using equations significantly less complex.
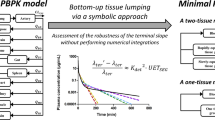
Graphical abstract

Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The most accessible tissue sampled in pharmacokinetic studies is blood/plasma. Those blood/plasma concentration-time data are typically analyzed using either (i) simple kinetic models, such as compartment models [1, 2] and minimal physiologically based pharmacokinetic (mPBPK) models [3], or (ii) more complex whole-body physiologically based pharmacokinetic (WB-PBPK) models [4]. One of the most notable differences between the two approaches would be the mathematical description of the blood/plasma pharmacokinetics, viz., bi-/tri-exponential functions for the simple models versus functions consisting of many exponential terms (e.g., 10 terms for a 9-tissue model) for WB-PBPK models [4]. Since the concentration-time profiles from experiments would graphically resemble the shape of only bi- or tri-exponential functions if drugs are given intravenously [5,6,7], some exponential terms in WB-PBPK models should be capable of being theoretically consolidated and simplified [8, 9] to mPBPK models [3], in light of the presence of similarity in kinetics of drug distribution to tissues. In our companion paper [10], we examined the theoretical basis for the consolidation and simplification of WB-PBPK to the minimal models. In particular, we found that drug-specific parameters, viz., tissue-to-plasma partition coefficient (Kp) and fractional distribution parameter (fd) of multiple tissues in WB-PBPK could be symbolically consolidated into those parameters of the lumped tissue group (i.e., Kp,lum and fd,lum) by Eqs. 1a and 1b:
This principle implies the preservation of the total apparent volume of distribution and distributional clearance for the lumped tissue (i.e., ∑VT ∙ Kp,lum and ∑QT ∙ fd,lum) from those tissues before lumping (i.e., ∑VTKp and ∑QTfd). We also proposed that the appropriateness of tissue lumping could be appraised by evaluating the impact of the lumping procedure (UETSEG, a unitless error term for the construction of SEG) on the terminal phase slope (λter), expressed as the fractional change in λter (FCT) (Eq. 2) [10]:
We showed [10] that Kdet, a drug-specific parameter and a determining coefficient for the number of tissue groups, could be calculated as the ratio of MTTmax (i.e., the maximum MTT value among tissues in WB-PBPK) to MRTB (i.e., the mean residence time in the body).
In this study, we aimed to determine the threshold condition of Kdet for the number of tissue groups when simplifying a WB-PBPK model to a mPBPK model based on the lumping theory proposed in our companion study [10]. We collected plasma/blood concentration-time data of 113 compounds after intravenous administration to rats from the literature and using in silico predictions based on a series of empirical correlations to calculate the Kp and fd values of those model compounds. We report that the systemic pharmacokinetics of drugs having Kdet less than 0.3 may be described by a one-tissue mPBPK model, while drugs having Kdet greater than or equal to 0.3 may be practically described by a two-tissue mPBPK model.
Methods
Collection of Concentration-Time Data from the Literature
To study the adequacy of the theory of tissue lumping proposed in our companion paper [10], we collected the plasma/blood concentration-time information for 113 compounds after intravenous administration to rats from the literature (Supplementary Table SI). The model compounds encompassed 4 types of ionization (i.e., acid, base, neutral, and zwitterion). The 113 compounds have systemic clearance (CLsys) values ranging from 0.0303 to 292 mL/min/kg and steady-state volume of distribution (Vss) values ranging from 0.117 to 19.9 L/kg.
The concentration-time relationships from the literature were first digitized using GetData software (GetData Graph Digitizer version 2.26). Standard non-compartmental analyses, using WinNonlin Professional® 5.0.1 software (Pharsight Corporation, Mountain View, CA), were then conducted using the digitized data to calculate model-independent pharmacokinetic parameters. The digitization process used in this study was assumed to be adequate when the fold-difference of crucial parameters (e.g., Vss and CLsys) were within a factor of 1.5 between the literature value and the current calculation. The adequate datasets were then used for the subsequent pharmacokinetic calculations.
Estimation of Biopharmaceutical Variables of Model Compounds for Use in WB-PBPK Calculations
The physicochemical properties, including log P, log D, the number of hydrogen bond donor and acceptor (HD and HA; ACD/Labs Percepta Platform available from http://www.chemspider.com/), pKa [MarvinSketchTM software version 15.1.11.0 (http://www.chemaxon.com)], and topological polar surface area (TPSA; http://molinspiration.com/), of the 113 compounds were initially estimated from their chemical structure. To predict the free fraction in plasma (fup) of the rat, the human fup values were first calculated [11] by utilizing Simcyp® Version 15 Release 1 (Simcyp Limited, Sheffield, UK) [12]. The rat free fraction is assumed to be identical to the human value [13]. Similarly, human Kb [Eq. 3a; i.e., the ratio of the drug concentration in red blood cells to that in plasma water (Crbc/Cu,plasma)] was assumed to be a reasonable estimate for rat values [14] and, thus, the blood-to-plasma partition coefficient (R) was calculated using the following equation (Eq. 3b) where Hct represents the hematocrit (i.e., 0.45) in rats:
To estimate the parallel artificial membrane permeability assay (PAMPA) value (Papp,PAMPA) [15], the relationship (Eq. 4) between the permeability and physicochemical properties, such as log P, log D, pKa, molecular weight (MW), HD, HA, and TPSA (Supplementary Table SII) was determined using a similar approach to a previous report [16]:
From this empirical relationship (Supplementary Fig. S1), Papp,PAMPA values for the compounds were calculated and used for the estimation of fd in 11 major tissues of rats, depending on the tissue distribution Models 1 and 2 [10, 17].
Assuming symmetrical transport rates into and out of tissues, Kp values for tissues were estimated in silico using the mechanistic prediction methods [18, 19] [i.e., Method 2 in the Simcyp® simulator [12]]. Then Vss for the 113 compounds was then estimated using the following relationship (Eq. 5) [20]:
where Vp and Vrbc are the volume of plasma and red blood cells; and EP is the erythrocyte-to-plasma partition coefficient (i.e., Kb⋅fup). For the elimination kinetics, CLsys, obtained from non-compartmental analyses from the digitized data, was used in differential equations for the arterial blood (for Models A and B, Fig. 1) and the lumped blood pool (for Models C, D, and E, Fig. 1; see below for detailed descriptions of the model structures). The physiological variables, such as VT and QT, required in PBPK calculations, were obtained from the literature [12, 21] and summarized in Table I. These values were essentially comparable to those used in the commercial software such as Simcyp® Version 15 Release 1. Numerical integration, using the fourth-order Runge-Kutta method, was carried out with Berkeley MadonnaTM software (version 8.3.18; University of California, Berkeley, CA, USA). When needed, the calculation of eigenvalues and eigenvectors of PBPK system matrices was conducted using PythonTM version 3.6.0. (www.python.org), based on the assumption of instantaneous drug distribution within the blood pool at time zero.

Schematic representation of PBPK models considered in the tissue lumping procedure: WB-PBPK models a consisting of 11 tissues (viz., adipose, bone, brain, gut, heart, kidney, liver, lung, muscle, skin, and spleen) (Model A), b with a modification of Model A by lumping liver, gut, and spleen into a splanchnic compartment (Model B), c in a shape of mammillary compartment model with the splanchnic and blood pool compartments (Model C); and d two-tissue and e one-tissue mPBPK model structures (Models D and E)
Tissue Lumping Process and Model Evaluation
Our strategy for tissue lumping in WB-PBPK model (Fig. 1a; Model A) could be summarized by 4 sequential steps: lumping of (i) the liver, gut, and spleen (i.e., splanchnic tissues) (Fig. 1b; Model B); (ii) the venous and arterial blood (i.e., the blood pool) (Fig. 1c; Model C, in a form of conventional multi-compartment mammillary model); (iii) the peripheral tissues segregated into SEG or REG using Eqs. 1a, 1b, and 2 (Fig. 1d; Model D, model with two tissue groups); and (iv) all the peripheral tissues consolidated into a single distribution pool (Fig. 1e; Model E, model with one tissue group).
The adequacy of each step of lumping was evaluated for 113 model compounds by monitoring the following ancillary criteria: (i) the terminal phase slope (λter); (ii) the area under the curve of the pharmacokinetic profiles from time 0 to tlast (AUClast); and (iii) the root mean square of logarithmic difference (RMSLD) represented as:
where Cpred and Cobs are the predicted and observed plasma/blood concentrations and n is the number of observed points. When necessary, we also calculated the difference in model predictions using the following equation:
where CWB − PBPK and Clumped are the results of model predictions from WB-PBPK and lumped models, and tlast is the last sampling time. With a dt value fixed to be 0.01 min in Eq. 7, the lumping process was assumed to be adequate when a fold-change of calculated criteria was within a factor of 2 between the simplified model and the WB-PBPK model. When necessary, the FCT [ (λter′ − λter)/λter, Eq. 2] and the ratio of slopes in the initial (λα/λ1) and distributional (λβ/λmajor) phases [10] were also monitored to determine the appropriateness of segregating peripheral tissues into SEG and REG in Model D. In addition, a unitless error term for the construction of REG, UETREG, was calculated to determine the adequacy of lumping of tissues into the REG as shown in our companion paper [10].
In this study, we were also interested in determining the appropriateness of the SEG construction based on the fold-difference in MTT values [22] as an ancillary method. Thus, a sequential lumping, based on Eqs. 1a and 1b, in the direction from the tissue having the longest MTT (MTTmax) to tissue(s) having the shorter MTT(s) was carried out. In addition, the similarity condition of MTT (viz., MTT values that were considered kinetically “equivalent”) was investigated for various cases of each model compound. The three validation criteria (RMSLD, λter, and AUClast); calculated from 1808 simulations after lumping [i.e., 113 compounds × 2 models (Models 1 and 2) × 8 combinations (with 9 peripheral tissues)]; were compared with those from Model C (before lumping), depending on the ratio of the maximum to the minimum MTT (MTTmax/MTTmin) for the tissues included in SEG. In this process, the model predictions were also assumed to be indistinguishable when a fold-change of the criteria between the models fell within a factor of 2.
Determination of Threshold Value of Kdet for Use of One-Tissue mPBPK
In this study, we determined the threshold condition between models having one tissue group and two tissue groups. As proposed in our companion paper [10], Kdet was regarded as a key determinant here. When necessary, we also considered the area ratio of Srec (i.e., area representing the distributional phase in rectangular coordinates, determined by three exponential curves from Model D) to AUC (i.e., area under the curve from time 0 to infinity) as a criterion of the kinetic contribution of the distributional phase to the shape of a comprehensive pharmacokinetic profile [10]. In Model D (i.e., \({C}_p(t)={C}_{\alpha }{e}^{-{\lambda}_{\alpha }t}+{C}_{\beta }{e}^{-{\lambda}_{\beta }t}+{C}_{\gamma }{e}^{-{\lambda}_{\gamma }t}\), under the condition λα > λβ > λγ), Srec could be calculated using the log-trapezoidal method (Eqs. 8a and b):
where three points T1′(t1, Cp(t1)), T2′(t2, Cp(t2)), and T3′(t3, Cp(t3)) represented the intersection points determined by each pair of \({C}_{\alpha }{e}^{-{\lambda}_{\alpha }t}\) and \({C}_{\beta }{e}^{-{\lambda}_{\beta }t}\), \({C}_{\alpha }{e}^{-{\lambda}_{\alpha }t}\) and \({C}_{\gamma }{e}^{-{\lambda}_{\gamma }t}\), and \({C}_{\beta }{e}^{-{\lambda}_{\beta }t}\) and \({C}_{\gamma }{e}^{-{\lambda}_{\gamma }t}\). Using the similar principles to determine Slog [10], we examined the change in Srec/AUC depending on Kdet for the 113 model compounds. If the contribution of Srec to AUC is sufficiently small under a certain range of Kdet, Model D structures would essentially become consistent with Model E structures.
Reconciliation of mPBPK Models Between Bottom-Up and Top-Down Approaches
The simplified models used in this study, Models D and E, were virtually identical to mPBPK structures, except their kinetic parameters were determined by fitting (i.e., traditional mPBPK analyses) or calculation (i.e., the current approach). Based on the lumping criteria proposed in this study (see the “Results” section), the current models (Model D/E) could be written in the format of these mPBPK models (Eqs. 9a and 9b) [3]:
For theoretical calculations of Kp,lum and fd,lum (i.e., bottom-up), Eqs. 1a and 1b were applied using in silico predictions of Kp [18, 19] and model-dependent calculations of fd [17] for rat tissues in WB-PBPK.
To validate the current “bottom-up” approach of tissue lumping, the kinetic parameters from a series of in silico predictions were compared with those determined by the model fitting methods (i.e., top-down) in two ways. First, 101 equally spaced concentration-time points from time 0 to 5 times the terminal phase half-life were theoretically generated using the analytical solution of Model C (i.e., a 10-exponential function for bolus injection) for the 113 model compounds. The number of tissue groups was determined using Kdet and the errorless datasets subjected to nonlinear regression analysis based on Eqs. 9a and 9b depending on their mPBPK models. Second, the experimental data for the 113 compounds were prescreened for which (i) the in silico prediction of Vss was within a factor of 2 and (ii) the terminal phase in the simulated profile was apparently reached at the last sampling time observed in the literature. Based on the above screening method, 31 compounds were selected and their experimental concentration-time data fitted to the appropriate mPBPK models (Eqs. 9a and 9b). When fitting the errorless and experimental datasets to Eqs. 9a and 9b to determine fd,lum values (i.e., top-down), the calculated Kp,lum from Eq. 1a was used. The resulting top-down fd,lum values were then compared with the bottom-up fd,lum values (Eq. 1b). In addition, the three ancillary criteria (λter, AUClast, and RMSLD) were also compared between bottom-up and top-down approaches of mPBPK models.
Results
Calculation of Biopharmaceutical Variables for Model Compounds
The Kp values for 113 model compounds in 11 typical tissues of WB-PBPK were calculated using their estimated fup, R, log P, and pKa values [18, 19] (see Supplementary Material 1 for the preliminary calculation results). To examine the validity of in silico determined Kp values used in this study, Vss values for the 113 model compounds were then estimated using Eq. 5. Despite assuming a lack of species difference in blood partitioning between humans and rats (i.e., fup and R), Vss estimated from the predicted Kp values (Vss,pred) was significantly correlated with Vss calculated from standard moment analyses for the blood/plasma pharmacokinetics (Vss,obs) of the model compounds (Supplementary Fig. S2) (i.e., logVss,obs = 0.972+0.695·logVss,pred, n = 113, R2 = 0.479; Pearson’s test for correlation, p < 0.001). We found that the number of Vss values within factors of 2 and 3 were 59 and 85 out of 113 compounds (52.2% and 75.2%).
In this study, we also determined the validity of in silico predictions for fd values depending on distribution Models 1 and 2. Since the inclusion of fd in WB-PBPK calculations improved the predictability of systemic pharmacokinetics [17], RMSLD (a predictability criterion) calculated using Model A was also evaluated. The number of compounds with RMSLD less than 0.301 and 0.477 (i.e., predictability within a factor of 2 and 3) was 39 and 68 (34.5% and 60.2%) for Model 1, and 43 and 73 (38.1% and 64.6%) for Model 2. Collectively, therefore, it was assumed that Kp and fd values generated by the current methods were practically useful, since the results was fairly reasonable with existing values of Kp [18, 19] and fd [17]. The computational Kp and fd values for the 113 model compounds were then used in subsequent calculations for blood/plasma pharmacokinetic profiles. We noted that some model compounds had relatively poor predictability for Kp and fd, thereby affecting the calculation of concentration-time relationship. However, the primary objective of this study was to compare theoretical pharmacokinetic profiles from Model C to those from Model D/E, rather than to compare actual experimental concentration-time data with model predictions. Therefore, we were more focused on generating a realistic range of physicochemical/biopharmaceutical parameters for the calculations. Those compounds associated with poor predictability for Kp and fd were, therefore, also included in pharmacokinetic calculations. In the real application of the current theoretical approach, experimentally determined Kp and fd values for each compound would have been used resulting in more reasonable prediction of the concentration-time profiles of the compound.
Impact of Tissue Lumping on Shape of Concentration-Time Relationships
Lumping of Splanchnic Tissues
We found that the splanchnic tissues (liver, gut, and spleen) may be mathematically combined, as shown in our companion paper [10], as if they were connected in parallel to the systemic circulation system (e.g., vein and artery). Applying our tissue lumping principle [10], it was evident that in drugs with perfusion-limited distribution to the liver (i.e., fd,LI → 1), distribution in the other splanchnic tissues (e.g., spleen and gut) would have negligible effects to the distribution kinetics to the splanchnic compartment. At the other extreme, when the apparent PAMPA permeability coefficient was sufficiently small (i.e., fupP/R < 1×10-6 cm/s) [17], for the example when Kp values are comparable between the liver, gut, and spleen (Supplementary Fig. S3), reciprocal MTT values for the modified tissues (i.e., 1/MTTSP′ and 1/MTTGU′, both corrected by 1 − fd,LI) [10] would be comparable to 1/MTTLI, regardless of the tissue distribution Models 1 and 2. Even when Kp values for liver, gut, and spleen were significantly different from each other, a significant model deformation with respect to the plasma pharmacokinetics did not appear to occur (Supplementary Material 2; the analytical solutions indistinguishable between Models A and B), since the coefficients for the zero- and first-order expansion terms of fractions in the left-hand sides between Eqs. 11 and 12 (see Appendix A) were retained in most of the tissues including liver, gut, and spleen (i.e., conservation of ∑VTKp and ∑QTfd) [10]. Thus, we found that these tissues could be practically lumped into the splanchnic compartment without causing a significant deviation in the calculation of the concentration-time relationship of Model B from Model A.
Lumping of Blood Pool
After constructing the splanchnic compartment, we then attempted to combine venous and arterial blood into a single blood pool. Calculated parameters, such as RMSLD, λter, and AUClast values (Supplementary Fig. S4), generated using the original Model A and the Model B with combined venous/arterial blood (i.e., Model C) revealed that the predictions were quite comparable between those models. As also shown in Supplementary Material 2, this observation indicates that the lumping of the venous and arterial blood into a single blood pool does not cause a significant deviation in the calculation of the concentration-time relationship except for the difference in the initial concentration (i.e., C0 = 0 for Model B; C0 ≠ 0 for Model C). In line with this, we also considered consolidating the blood pool and lung into a single “systemic circulation” group (i.e., vein-lung-artery connection) by assessing how the inclusion of the lung in the blood pool impacted the calculation of the concentration-time relationship. While the lumping of lung into the blood pool would, in theory [23], affect all eigenvalues of the solution of Model C, it was found that the initial phase slope λ1 was mostly altered by a fold-change in MTTc (i.e., mean transit time through the central compartment) (Supplementary Fig. S5). Considering the alteration of λ1 by lumping of lung into the blood pool, therefore, we ultimately chose to utilize Model C, i.e., the blood pool consisting of arterial and venous blood while the lung was regarded as one of the peripheral tissues, as the reference model to compare with simplified model structures.
Lumping of SEG
In order to determine appropriate criteria for tissue lumping, we considered segregating peripheral tissues into SEG or REG according to FCT. We used FCT as a determinant because the fractional change was a function of both the compound-specific Kdet and the lumping-dependent UETSEG (Eq. 2). Our premise was that peripheral tissues could be progressively lumped into the SEG from the tissue having the longest MTT to tissue(s) having shorter MTT(s) provided that λter does not change significantly. If the change in λter exceeded a certain threshold FCT value, then further lumping of tissues into the SEG ceased and the remaining peripheral tissues could then be collectively lumped into the REG. As shown in Fig. 2, SEG/REG construction with the value of FCT up to 0.1 resulted in comparable concentration-time relationships calculated from Model C (without lumping of peripheral tissues) and those from Model D or E (with lumping of peripheral tissues to SEG/REG) within a factor of two (Eq. 7). Therefore, it was proposed that the condition of FCT at 0.1 was a reasonable threshold for SEG construction.

Discrimination of peripheral tissues into SEG or REG by utilizing FCT as an index of tissue lumping. Segregation of tissues into SEG or REG was carried out by monitoring FCT from various lumping cases generated for the 113 model compounds. Model difference (y-axis) was calculated as Eq. 7, and horizontal dashed line denoted the fold-difference in model predictions with a factor of 2
Determination of the Number of Tissue Groups in Simplified PBPK Model Using Kdet
Since Kdet, the determining coefficient for the number of tissue groups, has not been defined in current literature, the parameter was initially calculated for two compounds (e.g., caffeine and cefazolin) to show how Kdet could play a role in the lumping of peripheral tissues. As shown in Fig. 3a, when a drug had a very low value of Kdet (e.g., 0.0185 for caffeine), λter did not change significantly even when UETSEG value varied up to 15. In contrast, the λter of cefazolin with a Kdet value of approximately 4.97 was quite sensitive to changes to UETSEG. This indicated that a drug with a low Kdet value would have a robust λter which is less sensitive to the change in UETSEG, a parameter that was governed by the lumping of the slow tissue group. The systemic pharmacokinetics of 4 additional compounds: artesunic acid, chlorzoxazone, cilostazol, and docetaxel in Model C (with regard to tissue distribution Model 1) were also shown in Fig. 3b. The data in Fig. 3b for these 6 compounds suggest that, when Kdet is sufficiently low, the contribution of the distributional area Srec to the total AUC becomes kinetically insignificant so that all peripheral tissues could be combined (Model E). Therefore, we aimed to determine the number of tissue groups in the simplified PBPK model (Models D and E) based on Kdet.

a Sensitivity of the terminal phase slope expressed as FCT [(λter′ − λter)/λter] to the effect of SEG construction (UETSEG) (i.e., Kdet2 to be the apparent slope of the plot). Six example compounds for a range of Kdet values were included (e.g., artesunic acid, cefazolin, docetaxel, cilostazol, chlorzoxazone, caffeine). b Graphical presentation of the contribution of distributional area (Srec) to AUC, depending on Kdet. Solid lines denote the systemic pharmacokinetics of the 6 compounds Model C, while dashed lines represent the terminal (\({C}_{10}{e}^{-{\lambda}_{10}t}\)) or initial exponential term (\({C}_1{e}^{-{\lambda}_1t}\)). The plasma concentrations were calculated up to the time at 5-fold of the terminal phase half-life (5 ln 2/λ10)
When all the nine peripheral tissues were deliberately lumped into one tissue group (Model E), the data for the 113 model compounds showed noticeable monotonic increase in FCT values along with their Kdet values (Fig. 4a) (e.g., an empirical correlation between FCT and Kdet up to the Kdet range of 10, logFCT = -0.433+1.14⋅logKdet, R2 = 0.946). However, the apparent linear relationship between FCT and Kdet slightly deviated for model compounds with Kdet values larger than 10. When we considered a threshold condition of Kdet < 0.3, all the compounds satisfying this condition [i.e., 29 cases, ~12.8% of the total 226 cases (113 compounds in two distribution models)] showed FCT values less than 0.1, suggesting that the change in λter remains insensitive even when all the peripheral tissues were lumped into one tissue group (i.e., Fig. 4a). Of note, 6 exceptions (cisplatin and indomethacin for Model 1; acyclovir, cisplatin, erythromycin, and terazosin for Model 2) with Kdet ranging from 0.308 to 0.350 also exhibited FCT less than 0.1. Collectively, this monotonic increase was consistent with the statement that a drug with a low Kdet value, e.g., below 0.3, would have a robust λter so that all peripheral tissues could be lumped into one tissue group.

Impact of Kdet for 113 model compounds on a the FCT assuming one-tissue mPBPK and b the change in Srec/AUC ratio assuming two-tissue mPBPK. Kdet < 0.3 resulted in the robust terminal phase (FCT < 0.1) and the Srec/AUC ratio approximately less than 2% showing the adequate use of one-tissue mPBPK (Model E). Open and closed circles denote simulation results from the tissue distribution Models 1 and 2
On the other end, we also aimed to monitor the contribution of the speculative area, Srec, to AUC depending on Kdet for all 113 model compounds. For the purpose of this calculation, we intentionally divided peripheral tissues into two groups (i.e., two-tissue mPBPK models). To construct Model D from Model C using a method independent of Kdet values, we considered applying an alternative method for the construction of the SEG (i.e., peripheral tissues lumped into an SEG according to the rule of MTTmax/MTTmin < 2; Supplementary Fig. S6) [22]. When the Srec/AUC ratio (Eq. 8b) was plotted against Kdet (Fig. 4b), the kinetic contribution appeared to be negligible when Kdet < 0.3 (e.g., Srec/AUC < 1.35%; for colistin sulfate), supporting the adequacy of Model E in the range. We observed that some compounds with Kdet sufficiently larger than 5 (Fig. 4b) could be associated with a low Srec/AUC ratio; this characteristic may not be interpreted as the evidence that an appropriate model for those compounds would be Model E (i.e., bi-exponential relationship) since a large value of Kdet, e.g., larger than 5, would indicate that any lumping of peripheral tissues drastically altered λter (Fig. 3a). Therefore, even with low Srec/AUC ratios, the systemic pharmacokinetics was more likely to be described by Model D for compounds with such high Kdet values.
Consideration for Lumping of REG
For compounds having Kdet ≥ 0.3, FCT was not likely to be sufficiently robust since, at a certain point of tissue lumping, the terminal phase could be drastically affected. Thus, the construction of the REG became necessary. Initially, we found that the model predictions of Model D (i.e., blood pool plus 2 tissue groups with different equilibrating rates) and that of Model C (i.e., blood pool plus nine peripheral tissues) were almost always within a factor of two where FCT of 0.1 was used as the threshold (Fig. 2). To further determine the adequacy of REG construction with this principle, we evaluated whether λβ in Model D was comparable with λmajor in Model C [10] using the 113 model compounds. As shown in Fig. 5a, it was readily evident that λβ was comparable to λmajor for most compounds having Kdet > 1, indicating that FCT of 0.1 was a reasonable threshold for the segregation of SEG and REG for those compounds.

Comparison between the distributional phase slope of Model D (λβ) and Model C (λmajor) as the ratio of λβ/λmajor, a depending on Kdet, and b predicted by UETREG for the Kdet range between 0.3 and 1, after segregation of 9 peripheral tissues into SEG or REG based on the condition of FCT < 0.1
However, for the compounds having 0.3 ≤ Kdet < 1 [i.e., 63 cases; 27.9% of the total of 226 (113 compounds in two distribution models)] some, but not all, compounds had a significant dissociation between λβ and λmajor (i.e., 36 cases; 15.9% of the total) (Fig. 5a). Since some compounds in this range still had comparable λβ and λmajor values, the rule of FCT at 0.1 remains applicable when determining the appropriateness of the lumping of tissues. Even for those compounds having a significant difference between λβ and λmajor values, however, the calculation results between Models C and D remained fairly accurate (Fig. 2). Furthermore, the contribution of Srec to the total AUC was only approximately 18.9% (i.e., Model 1 for tamoxifen; Fig. 4b) or less for those compounds, suggesting that its effects on the plasma concentration-time relationship is potentially minor. Therefore, for the sake of practicality we cautiously recommend to apply the threshold of FCT at 0.1 for the SEG construction even for those compounds in the range 0.3 ≤ Kdet < 1, while the other remaining peripheral tissues can then be collectively lumped as the REG.
Reconciliation of mPBPK Models Between Bottom-Up and Top-Down Approaches
If the theoretical consideration was adequate, a statistically acceptable correlation would be found between calculated vs. fitted parameters (i.e., bottom-up vs. top-down) for a given set of compounds. Here, such a reconciliatory study was first carried out using PBPK calculations for the 113 model compounds. When the errorless simulation data (i.e., 101 points generated from a 10-exponential function for Model C) were fitted to the mPBPK model structures (Model D for Kdet ≥ 0.3 and Model E for Kdet < 0.3), these top-down fd,lum values were consistent with bottom-up fd,lum values (Fig. 6a; see Supplementary Table SIII for details). In this correlation, a few points did not fall within a factor of 2, which were the cases with Kdet values (for Models 1 and 2) between 0.3 and 1 [e.g., indomethacin (0.339 and 0.322) and ochratoxin (0.402 and 0.376)] or less than 0.3 [e.g., tolbutamide (0.0891 and 0.0863)]. Even for those 3 cases, however, RMSLD was found to be less than 0.0577, indicating that concentration-time profiles generated by bottom-up model predictions were fairly consistent with the corresponding datasets. For 31 compounds with experimental data (Table II), bottom-up fd,lum values were significantly correlated with top-down fd,lum values (Fig. 6b), based on the Pearson’s correlation test (i.e., R2 = 0.367 and 0.379 for Models 1 and 2; p < 0.0001 for both cases). The number of fd,lum values within factors of 2 and 3 were 50 and 68 out of 100 points, while the three criteria (RMSLD, λter, and AUClast) were comparable between the two approaches (Supplementary Fig. S7). Collectively, model predictions from the current bottom-up method appeared comparable with those from the top-down approach for the 113 model compounds.

Relationship between the fractional distributional parameters, fd,lum, calculated by bottom-up and top-down approaches in mPBPK models. The fd,lum values calculated from bottom-up approach was plotted against top-down values fitted to: a the errorless data from Model C for 113 model compounds and b the experimental observations for a subset of 31 compounds. Dashed lines represented the two-fold difference between top-down and bottom-up approaches for the parameters. Open and closed circles denoted calculation results from Models 1 and 2
Discussion
Systemic pharmacokinetics is a manifestation of the intricate operations of drug disposition kinetics (viz., WB-PBPK model) occurring within the body. Despite the theoretical complexity, however, plasma concentration-time data typically follow relatively simple bi- or tri-exponential decay functions [5,6,7] when drugs are given intravenously. As a result, simplified models (e.g., mPBPK and compartment models) were often sufficient for the descriptive analyses of plasma pharmacokinetics. Rationalization for the dissociation between the theoretical complexity in PBPK models and the relative simplicity in actual data has not been clearly delineated in the literature. Theoretical bases for the simplification of WB-PBPK models may ultimately provide the predictive capability of the intuitive calculations of kinetic parameters in the simplified models.
In this study, we found that the concentration-time relationship could be practically calculated by Model D, for the purpose of comparing the initial, distributive, and terminal phase slopes. In particular, we considered the version of Model D that assumes the blood pool and lung are combined [\({C}_p(t)={C_{\alpha}}^{\prime }{e}^{-{\lambda}_{\alpha}\prime t}+{C_{\beta}}^{\prime }{e}^{-{\lambda}_{\beta}\prime t}+{C_{\gamma}}^{\prime }{e}^{-{\lambda}_{\gamma}\prime t}\)] and the version of Model D that assumes separate lung and blood pool [\({C}_p(t)={C}_{\alpha }{e}^{-{\lambda}_{\alpha }t}+{C}_{\beta }{e}^{-{\lambda}_{\beta }t}+{C}_{\gamma }{e}^{-{\lambda}_{\gamma }t}\)], based on the ancillary rule of lumping (MTT ratio of 2). In this comparison, we found that the fold-change in the initial slope (λα′/λα) was directly proportional to the ratio of MTTc/MTTc′ as shown in Supplementary Fig. S8. Furthermore, this relationship was obtained without significant alterations in the ratios of slopes for distributional (λβ′/λβ) and terminal (λγ′/λγ) phases. These observations indicate that the slope at time 0 (e.g., ∑Ciλi/C0), which is mathematically associated with the change of MTTc [23], is mostly governed by the initial slope λα (see also x-intercept for the right-hand side of Eqs. 11 and 12). Therefore, if a rapid decline of plasma concentration profiles in the initial phase is of great importance, it would be useful to monitor the change in MTTc that could lead to a significant alteration of the initial phase slope in model simulations when the lung and blood pool are being lumped as a single group. In the lumping of the lung into the blood pool of Model C, however, some drugs with extremely high permeability coefficients; e.g., colistin methanesulphonate, colistin sulfate, diltiazem, and epigallocatechin-3-gallate; showed deviations between λ1′/λ1 and MTTc/MTTc′ (Supplementary Fig. S5). Therefore, we utilized Model C to compare with simplified model structures where the blood pool consisted of just artery and vein while the lung was regarded as one of the peripheral tissues in the subsequent calculations.
Kdet, a crucial factor governing the number of tissue groups, was theoretically defined in our companion paper [10] and its practical threshold was determined in this study. In particular, we studied the impact of the progressive lumping of tissues in the direction from the tissue with the longest MTT (i.e., MTTmax) on FCT [i.e., (λter′ − λter)/λter]. From Taylor series expansions of Eqs. 11 and 12 in the companion paper [10], it was found that FCT could be mathematically approximated as Kdet2 ⋅UETSEG (Eq. 2). In practice, however, the relationship between FCT and Kdet2 ⋅UETSEG could be much more complex; this is especially true when the difference between O((MTTλ)2) (i.e., the second-order error term by the lumping of SEG, when Eqs. 11 and 12 were expanded) and UETSEG became significant. In fact, the relationship between FCT and UETSEG (Fig. 3a) appeared to more closely follow an exponential relationship (Eq. 10), rather than a simple linear relationship:
We were not able to identify the mathematical basis for this apparent relationship, although the estimates of Kdet were quite consistent with the ratio of MTTmax and MRTB (Supplementary Fig. S9) when the actual calculations from our literature examples were fitted to Eq. 10. For the purpose of this study, however, we were only interested in FCT values of 0.l or less and, thus, the error would be negligible even when FCT was assumed to be directly related to Kdet2 ⋅UETSEG. The consideration of an exponential relationship between FCT and UETSEG (Eq. 10) may not be practically necessary here. When the values of MTTmax (e.g., estimated value based on anatomical/physiological variables and predicted/measured Kp, fd, and R) and MRTB (e.g., standard moment analysis) were evaluated, the robustness of FCT as a determinant for the lumping of tissues into the SEG may be estimated by the determination of Kdet. It should also be noted that, based on the apparent relationship shown in Eq. 10, a slight deviation of the fitted Kdet from MTTmax/MRTB (Supplementary Fig. S9) could occur when the value exceeded 10 (i.e., 16.4% of total points). However, the appropriateness of the relationship Kdet = MTTmax/MRTB as the determining coefficient for the number of tissue groups would still apply since, as described in Fig. 3a, this large value of Kdet, e.g. > 10 would essentially lead to the marked change in FCT (i.e., sensitive to UETSEG) and thus the corollary use of another tissue group of different distribution rate, namely, the REG would be appropriate.
In this study, we proposed that the compounds having Kdet < 0.3 can be reasonably classified as representing a one-tissue model. In the literature, Pilari and Huisinga [24] studied the pharmacokinetics of 25 compounds and determined that only 5 drugs were considered to follow the one-tissue model because of their relatively low MTTmax values. However, when the criterion of Kdet proposed here was applied to the same 25 compounds studied by Pilari and Huisinga, a total of 16 drugs may be categorized to follow the one-tissue model. This discrepancy may arise because the authors considered similarity in the concentration-time profiles of all tissues, some of which may not significantly contribute to the systemic pharmacokinetics. The objective of our study was to provide a theoretical basis for the simplification of WB-PBPK model (Model C) to reduced models (Model D/E) without affecting the plasma pharmacokinetic profiles, rather than reproduce all tissue concentration-time profiles, of the compound being studied.
While most compounds where FCT < 0.1 showed comparable values between λβ and λmajor for Kdet > 1 (Supplementary Fig. S10a) calculated from all the possible combinations of SEG and REG, we found that certain compounds with 0.3 ≤ Kdet < 1 (i.e., 301 out of 504 cases) had λβ/λmajor values exceeding a factor of 2 (Supplementary Fig. S10b). The dissociated λβ/λmajor factor for these compounds indicates that the lumping of tissues into the REG may not be appropriate for these compounds. In this study, we did not directly examine the kinetic/biopharmaceutical reason(s) for the dissociation. However, it could be speculated that the presence of structural error, e.g., the presence of kinetically ambiguous tissue(s) and/or inadequacy of setting up a single “major” tissue representing λβ, might be involved in causing the discrepancy under this condition of 0.3 ≤ Kdet < 1. Unfortunately, the rearrangement of the order of tissues rather than the descending order of MTT (e.g., based on the capability of a candidate tissue for obtaining the minimal UETSEG value when lumping from the longest tissue) did not improve the dissociation between λβ and λmajor for these compounds. Despite this limitation, however, it would be noteworthy that the contribution of Srec to AUC was found to be less than 19% for drugs of 0.3 ≤ Kdet < 1 (Fig. 4b). Therefore, a significant deformation between Models C and D and/or a significant inadequacy of λmajor appeared less likely. For the sake of practicality, for those compounds of 0.3 ≤ Kdet < 1, it is possible that λβ may be slightly deviated from λmajor despite the fact that the contribution of the deviation could be minor to the overall AUC. If necessary, this deviation of λβ from λmajor could be estimated by the use of UETREG (Fig. 5b) [10]. When the pharmacokinetic profile in this phase is of great importance, the use of Model C may be appropriate.
Despite some of such potential deviations in the distributional-phase slopes during the lumping, a reasonable correlation in fd,lum values between bottom-up calculations by Eq. 1b and top-down fitting of Eq. 9a and 9b to the errorless dataset (Fig. 6a) indicated the appropriateness of the current lumping method. According to the currently available tissue lumping methods in the literature [22, 24,25,26,27], visual/numerical assessments were often considered to evaluate the appropriateness of tissue lumping, as also shown in this study (Supplementary Material 2). In addition, statistical evaluation could be also useful for comparisons between WB-PBPK and lumped models [e.g., the prediction error PE = logCpred− logCobs [26]; analogous to Eqs. 6 and 7]. However, since our tissue lumping method was derived on the basis of a symbolic approach, the endpoint criterion for assessing the adequacy of tissue lumping could now be improved to include the simple comparisons of lumped PBPK model parameters, e.g., fd,lum in this study (Fig. 6a).
Based on calculations for the 113 model compounds, it was readily apparent that the distributional phases in terms of plasma pharmacokinetics for the compounds of Kdet ≥ 5 were clearly distinct as evidenced by tissue MTT values [e.g., for metformin, Kdet value was 7.10 for rats where MRTB, MTTSEG and MTTREG values were 23.1, 164, and 13.4 min in mPBPK models [28]]. In contrast, for compounds with lower Kdet values, e.g., 0.3 ≤ Kdet < 1, the distinction between MTTSEG and MTTREG was less apparent, indicating that certain tissue(s) may partially participate in both REG and SEG, as evidenced by some deviations between theoretical and fitted fd values for indomethacin and ochratoxin (Fig. 6a; Supplementary Table SIII).
In this study, the model difference calculated from Eq. 7 was assumed to be practically acceptable under a factor of 2 (i.e., y < 1): Despite the fact that determination of an adequate acceptance level of model difference may be difficult to theoretically set, we found that the model difference y could be related as a function of FCT (Fig. 2) where the FCT less than 0.1 was associated with a 2-fold error (i.e., y < 1). Using perchloroethylene as an example, visual/numerical inspections (Supplementary Material 2) showed indistinguishable profiles between Model D and WB-PBPK models, yet the model difference y was approximately 0.933, a value close to 1 (i.e., 2-fold error), supporting the practical utility of the current conditions (i.e., y < 1 and FCT < 0.1) of SEG lumping.
However, slight deviations between Models D and A/B/C (Supplementary Material 2) were noted in plasma pharmacokinetic profiles for some compounds (i.e., biochanin A, bisphenol A, genistein, glycyrrhetic acid, ipriflavone, paclitaxel, parathion, and propofol). Due to their Kdet values ranging from 3.53 to 73.8, only one tissue (i.e., skin) was capable of being lumped into the SEG (Supplemental Table SIII) while the second-largest tissue (i.e., adipose) and the remaining ones were lumped into the REG (cf. MTTAD/MTT1 ranging from 51.7 to 82.7 for the 8 compounds). Since such high Kdet values would lead to emergence of distinct distributional/terminal phases in plasma profiles depending on the MTTs of WB-PBPK tissues (Supplementary Table SIV), more than 2 tissue groups (e.g., skin, adipose, and the REG) could have been utilized to reproduce all the exponential phases arising from divergent/distinct tissue transit times for those compounds, as evidenced by Supplementary Fig. S11. Despite the practical applicability of the general premise of this study (i.e., WB-PBPK models being represented as bi- or tri-exponential functions) wherein the current lumping criteria (i.e., y < 1 and FCT < 0.1) were applied for the model compounds, cautions would be required especially when Model C could possibly be described by more than 3 exponential terms (i.e., Kdet > 1).
In typical mammillary two-compartment models, the shape of the plasma concentration profile was reported to be dependent on the number of cycles around the central compartment (i.e., CLD/CLsys) [29]. When CLD < CLsys, the terminal phase kinetics was considered to be distribution-limited. This concept of the ratio CLD/CLsys in the literature could be also applied to WB-PBPK. Equation 11 showed that the theoretically possible maximum of λter would be 1/MTTmax. The CLD in the two-compartment model would be analogous to ∑QTfd in the WB-PBPK structure. Where CLD < CLsys, viz., Q9fd9 < CLsys here [30], it was observed that a sufficiently large systemic clearance could result in λter being approximated to be the reciprocal of the longest MTT tissue in WB-PBPK. In many typical pharmacokinetic studies, however, the kinetics in the terminal phase may often remain unaccounted at the last sampling time, most likely due to limitations in the analytical quantification method. From our in silico calculation (e.g., wherein the limitation of sampling times was eliminated), we found that the tissue with the longest MTT was, in most cases (110 out of 113), the skin (exceptions, the brain for chlorzoxazone, muscle for colistin sulfate, and adipose for tamoxifen). The reciprocal of the maximum MTT value for 9 peripheral tissues was highly correlated with λter, the smallest eigenvalue of WB-PBPK (e.g., 68.1% and 71.7% within a factor of 2, for Models 1 and 2) (Supplementary Fig. S12). Therefore, it may be worth attempting a priori calculation of MTT values for various tissues in order to ascertain the possibility of the existence of a kinetically deep tissue compartment (e.g., skin tissue) that could be overlooked in the systemic pharmacokinetics [31].
Conclusions
In summary, we herein propose a biopharmaceutical condition for determining the number of tissue groups in simplified forms of WB-PBPK models. For Kdet < 0.3, the use of Model E (i.e., blood pool plus one lumped peripheral tissue) could be adequate since the FCT would be less than 0.1 even with all peripheral tissues collectively lumped and the Srec/AUC ratio would be less than approximately 2%. For Kdet ≥ 1, the tissue with MTTmax could be progressively lumped with the shorter MTT tissue(s) into the SEG, provided that FCT was less than 0.1. The remaining tissues could then be lumped into the REG (Model D; blood pool plus two lumped tissue groups with different equilibrating rates). Our primary recommendation for the cases of 0.3 ≤ Kdet < 1 was to cautiously apply the same rule of the case of Kdet ≥ 1 (i.e., Model D), considering the fact that the contribution of the distributional area Srec to the AUC was less than approximately 19%. Despite some of such potential deviations in the distributional-phase slopes during the lumping, our tissue lumping method based on a symbolic approach allowed a simple comparison of lumped PBPK model parameters, e.g., fd,lum in this study, whereby a consistent correlation indicated the appropriateness of the current lumping method. Collectively, by using the principles proposed in this study, WB-PBPK could be simplified to mPBPK models without significantly affecting plasma concentration-time profiles. Furthermore, the current approach may enable theoretical calculation of key coefficients of mPBPK models using estimates from in silico/in vitro studies.
References
Levy G, Gibaldi M, Jusko WJ. Multicompartment pharmacokinetic models and pharmacologic effects. J Pharm Sci. 1969;58(4):422–4.
Benet LZ. General treatment of linear mammillary models with elimination from any compartment as used in pharmacokinetics. J Pharm Sci. 1972;61(4):536–41.
Cao Y, Jusko WJ. Applications of minimal physiologically-based pharmacokinetic models. J Pharmacokinet Pharmacodyn. 2012;39(6):711–23. https://doi.org/10.1007/s10928-012-9280-2.
Sager JE, Yu J, Ragueneau-Majlessi I, Isoherranen N. Physiologically based pharmacokinetic (PBPK) modeling and simulation approaches: a systematic review of published models, applications, and model verification. Drug Metab Dispos. 2015;43(11):1823–37.
Riegelman S, Loo J, Rowland M. Shortcomings in pharmacokinetic analysis by conceiving the body to exhibit properties of a single compartment. J Pharm Sci. 1968;57(1):117–23.
Hirtz J. The fate of drugs in the organism. A bibliographic survey complied by the Societe´ Fran¸aise des Sciences et Techniques Pharmaceutique, Working group under the chairmanship of HIRTZ. Dekker New York; 1974.
Segre G. Pharmacokinetics—compartmental representation. Pharmacol Ther. 1982;17(1):111–27.
Vaughan D, Dennis M. Number of exponential terms describing the solution of an N-compartmental mammillary model: Vanishing exponentials. J Pharmacokinet Biopharm. 1979;7(5):511–25.
Wagner JG. Linear pharmacokinetic models and vanishing exponential terms: Implications in pharmacokinetics. J Pharmacokinet Biopharm. 1976;4(5):395–425.
Jeong Y-S, Kim M-S, Chung S-J. Determination of the number of tissue groups of kinetically distinct transit time in whole-body physiologically-based pharmacokinetic (PBPK) models I: Theoretical consideration of bottom-up approach of lumping tissues in whole-body PBPK. AAPS J. 2022. https://doi.org/10.1208/s12248-022-00732-y.
Lobell M, Sivarajah V. In silico prediction of aqueous solubility, human plasma protein binding and volume of distribution of compounds from calculated pKa and AlogP98 values. Mol Diversity. 2003;7(1):69–87.
Jamei M, Marciniak S, Feng K, Barnett A, Tucker G, Rostami-Hodjegan A. The Simcyp® population-based ADME simulator. Expert Opin Drug Metab Toxicol. 2009;5(2):211–23.
Colclough N, Ruston L, Wood JM, MacFaul PA. Species differences in drug plasma protein binding. Med Chem Commun. 2014;5(7):963–7.
Uchimura T, Kato M, Saito T, Kinoshita H. Prediction of human blood-to-plasma drug concentration ratio. Biopharm Drug Dispos. 2010;31(5-6):286–97. https://doi.org/10.1002/bdd.711.
Kerns EH, Di L, Petusky S, Farris M, Ley R, Jupp P. Combined application of parallel artificial membrane permeability assay and Caco-2 permeability assays in drug discovery. J Pharm Sci. 2004;93(6):1440–53.
Fujikawa M, Ano R, Nakao K, Shimizu R, Akamatsu M. Relationships between structure and high-throughput screening permeability of diverse drugs with artificial membranes: application to prediction of Caco-2 cell permeability. Bioorg Med Chem. 2005;13(15):4721–32. https://doi.org/10.1016/j.bmc.2005.04.076.
Jeong Y-S, Yim C-S, Ryu H-M, Noh C-K, Song Y-K, Chung S-J. Estimation of the minimum permeability coefficient in rats for perfusion-limited tissue distribution in whole-body physiologically-based pharmacokinetics. Eur J Pharm Biopharm. 2017;115:1–17.
Rodgers T, Leahy D, Rowland M. Physiologically based pharmacokinetic modeling 1: Predicting the tissue distribution of moderate-to-strong bases. J Pharm Sci. 2005;94(6):1259–76. https://doi.org/10.1002/jps.20322.
Rodgers T, Rowland M. Physiologically based pharmacokinetic modelling 2: predicting the tissue distribution of acids, very weak bases, neutrals and zwitterions. J Pharm Sci. 2006;95(6):1238–57. https://doi.org/10.1002/jps.20502.
Øie S, Tozer TN. Effect of altered plasma protein binding on apparent volume of distribution. J Pharm Sci. 1979;68(9):1203–5.
Brown R, Delp M, Lindstedt S, Rhomberg L, Beliles R. Physiological parameter values for physiologically based pharmacokinetic models. Toxicol Ind Health. 1997;13407:407–84.
Nestorov IA, Aarons LJ, Arundel PA, Rowland M. Lumping of whole-body physiologically based pharmacokinetic models. J Pharmacokinet Biopharm. 1998;26(1):21–46.
Veng-Pedersen P, Gillespie WR. Single pass mean residence time in peripheral tissues: a distribution parameter intrinsic to the tissue affinity of a drug. J Pharm Sci. 1986;75(12):1119–26.
Pilari S, Huisinga W. Lumping of physiologically-based pharmacokinetic models and a mechanistic derivation of classical compartmental models. J Pharmacokinet Pharmacodyn. 2010;37(4):365–405.
Gueorguieva I, Nestorov IA, Rowland M. Reducing whole body physiologically based pharmacokinetic models using global sensitivity analysis: diazepam case study. J Pharmacokinet Pharmacodyn. 2006;33(1):1–27.
Björkman S. Reduction and lumping of physiologically based pharmacokinetic models: prediction of the disposition of fentanyl and pethidine in humans by successively simplified models. J Pharmacokinet Pharmacodyn. 2003;30(4):285–307.
Brochot C, Tóth J, Bois FY. Lumping in pharmacokinetics. J Pharmacokinet Pharmacodyn. 2005;32(5-6):719–36.
Jeong Y-S, Jusko WJ. Meta-assessment of metformin absorption and disposition pharmacokinetics in nine species. Pharmaceuticals. 2021;14(6):545.
Kong AN, Jusko WJ. Definitions and applications of mean transit and residence times in reference to the two-compartment mammillary plasma clearance model. J Pharm Sci. 1988;77(2):157–65.
Berezhkovskiy LM. Prediction of drug terminal half-life and terminal volume of distribution after intravenous dosing based on drug clearance, steady-state volume of distribution, and physiological parameters of the body. J Pharm Sci. 2013;102(2):761–71.
Fleishaker JC, Smith RB. Compartmental model analysis in pharmacokinetics. J Clin Pharmacol. 1987;27(12):922–6.
Funding
This study was supported by the Korea Environment Industry & Technology Institute (KEITI) through the project for BioMarkers TRANSLation of consumer chemicals/ft.life-stage PBPK modeling (BioTranSL/PBPK) (NO. 2022002970003).
Author information
Authors and Affiliations
Contributions
Yoo-Seong Jeong: Conceptualization, methodology, formal analysis, investigation, data curation, writing-original draft, writing-review & editing, visualization
Min-Soo Kim: Methodology, software, formal analysis, data curation, writing-review & editing, visualization
Suk-Jae Chung: Conceptualization, methodology, formal analysis, writing-original draft, writing-review & editing, supervision, project administration, funding acquisition
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendix
Appendix
By applying Gauss elimination of the system matrix A of PBPK Model C [10], 10 eigenvalues were readily determined using Eq. 11:
When the two-tissue mPBPK model (Model D) is applicable, the eigenvalues (in terms of λ′; the roots corresponded to λα, λβ, and λγ) after tissue lumping could be determined by Eq. 12:
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Jeong, YS., Kim, MS. & Chung, SJ. Determination of the Number of Tissue Groups of Kinetically Distinct Transit Time in Whole-Body Physiologically Based Pharmacokinetic (PBPK) Models II: Practical Application of Tissue Lumping Theories for Pharmacokinetics of Various Compounds. AAPS J 24, 91 (2022). https://doi.org/10.1208/s12248-022-00733-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1208/s12248-022-00733-x