
Abstract
Introduction
With the 2016 World Health Organization Classification of Tumors of the Central Nervous System (2016 CNS WHO), diagnosis of glioma is based on molecular parameters in addition to histology potentially leading to additional demands on quality of tissue samples. This may challenge the role of minimally invasive biopsy procedures. This study aims to evaluate the diagnostic yield of glioma samples from frameless stereotactic biopsies with focus on molecular information and explore the neuromolecular profile of a glioma biopsy cohort.
Methods
In a case series analysis, 180 consecutive frameless stereotactic biopsies with the Brainlab® Varioguide system from January 2011 to October 2017 were reviewed and patients with suspected or verified glioma were identified. Neuropathological samples were reprocessed in accordance with 2016 CNS WHO standards.
Results
One hundred nineteen glioma patients were identified. Analysis of IDH status could be performed in 95.8% resulting in a cumulative mutation rate of 9.6%. A complete diagnosis according to 2016 CNS WHO including grading and molecular features was achieved in 110 cases (92.4%). Entities were revised in four cases. Most common diagnosis was IDH-wildtype glioblastoma (66.4%) followed by IDH-wildtype anaplastic astrocytoma (21.8%).
Conclusions
A formally complete diagnosis according to 2016 CNS WHO was achieved in the majority of cases. The biopsy cohort showed a prognostically unfavorable distribution of diagnoses and molecular features. Frameless stereotactic biopsy seems to be confirmed as a useful diagnostic tool in contemporary neuro-oncology—however, certain potential limitations should be considered.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The concept of classifying cerebral tumor entities has substantially changed since the previous World Health Organization Classification of Tumors of the Central Nervous System (CNS WHO) of 2007, which had been based on morphological aspects [1]. Advances in understanding molecular alterations and the availability of effective and appropriate methods for their detection have led to a revision of classification of brain tumors [2]. The 2016 CNS WHO incorporates molecular features and propagates the concept of a ‘layered diagnosis’ [1]. Information about both morphological and molecular features is considered the highest diagnostic level.
Biopsy of intracranial lesions is essential to guide further treatment if resection is not considered feasible in the first instance. Different frameless stereotactic biopsy techniques have been established over recent years and were reported to provide a satisfactory diagnostic yield with low complication rate [3,4,5,6], including Brainlab® Varioguide system (Brainlab AG, Munich, Germany)—a neuronavigation-based technique [7,8,9]. Notably, all these studies were based on previous CNS WHO. With the 2016 CNS WHO, the important role of molecular parameters in addition to histology may put additional demands on quality and quantity of tissue samples. Whether samples of frameless stereotactic biopsy procedures suffice the relevant diagnostic criteria of the 2016 CNS WHO has not been investigated yet. Moreover, no demonstration of the molecular profile of a biopsy-only cohort has been demonstrated so far.
The aim of this study was to evaluate the role of frameless stereotactic biopsy procedures in the context of 2016 CNS WHO with particular focus on molecular diagnostic yield. A biopsied glioma cohort is described with molecular features and impact of the new CNS WHO is presented.
Methods
Patients
The study was reported to the local ethics committee (WF-69/17) and was performed in accordance with international ethical standards. Patient consent was not required due to prospectively anonymized patient data.
A consecutive series of 180 frameless stereotactic biopsy procedures at our university medical center from January 2011 to October 2017 was reviewed and cases with suspected or verified glioma were identified (Fig. 1). Patients with a histologically verified lymphoma or metastasis were excluded from this study.

Selection process of the study cohort. The flow chart describes the institutional concept for newly diagnosed intra-axial lesions and the selection criteria of the study cohort
Generally, the treatment strategy for intracranial lesions is discussed in case conferences at our institution. The decision of biopsy in preference to resection was based on general health condition, extension of the lesion, or atypical imaging presentation. Frame-based stereotactic biopsies instead of frameless procedures were performed in infratentorial or very small (maximal diameter of approximately < 5 mm) eloquent lesions and are not considered in this study.
Basic demographic data, modified Rankin Scale (mRS) on admission, procedure duration, recommended oncological concept and major complications (predefined as procedure-related death or clinically relevant hemorrhage or ischemia) were collected for all patients.
Surgical procedure
All frameless stereotactic biopsies were performed with the Brainlab® Varioguide system (Brainlab AG, Munich, Germany) [7]. Neuronavigation was based on a preoperative MRI or CT scan if MRI was contraindicated. A trajectory was planned in advance using iPlan®-Net. All surgical procedures were performed under general anesthesia. The head was 3-point fixed in a Mayfield clamp. The surface was registered until a sufficient accuracy was achieved. After neuronavigational guided skin incision and trepanation, the stereotactic arm was adjusted with satisfactorily accuracy (deviation < 1 mm according to software) and multiple samples were taken mostly at different depths along the trajectory. Frozen section consultation was subject to surgeon’s judgment.
Neuropathological diagnosis
Neuropathological samples were initially processed according to institutional standards and have retrospectively been reassessed to fulfil 2016 CNS WHO standards [2]. This included immunohistochemistry for p.R132H mutant isoform of isocitrate-dehydrogenase-1 (IDH1) for all glioma samples on an automated Ventana HX IHC system (Ventana-Roche Medical systems, Tucson, AZ, USA) following the manufacturer´s instructions. As an antibody, clone H09 with a concentration of 1:20 was used (DIA-H09, Dianova, Hamburg, Germany). If negative, sequencing for IDH1 codon 132 and IDH2 codon 172 gene mutations was performed in all grade II or III tumors or all grade IV tumors with age less than 60 years. For this, DNA was isolated from paraffin-embedded tumor material, followed by a polymerase chain reaction (PCR) to amplify IDH1 exon 4 containing the p.R132 hotspot and IDH2 exon 4 containing the p.R172 hotspot and subsequent Sanger sequencing reactions to identify single nucleotide mutations. 1p/19q codeletion status was performed for samples with oligodendroglial morphology by dual-color florescence in situ hybridization (FISH) on paraffin-embedded tumor material using fluorochrome-labelled probes (1p36/1q25 and 19q13/19p13; VysisLSI, Abbott Park, Illinois, USA). The methylation status of the promotor for the gene for O-6-methylguanine-DNA methyltransferase (MGMT) was assessed by methylation-specific PCR, using primers that include the potentially methylated cytosine residues, thus resulting in methylation-sensitive amplification followed by electrophoretic analysis of the resulting PCR product.
Statistical analysis
For analysis purposes, quality of neuropathological diagnoses was rated according to the predefined following grades. An integrated diagnosis consisting of both phenotypic and genotypic parameters was considered as the highest level of diagnostic yield (Grade A). A histological description without definite WHO grade or insufficient molecular information (not otherwise specified, NOS) was grouped as Grade B. A non-diagnostic biopsy without clear proof of tumor tissue was rated as Grade C.
Univariate analyses were performed to test the influence of patient and procedural variables on diagnostic yield. These included age, sex, mRS on admission, preoperative steroid application within 14 days, burr hole position, side, procedure duration, trajectory length, maximal tumor diameter, contrast enhancement, preoperative imaging modality (MRI vs CT), frozen section consultation and number of collected samples.
Analysis was performed using IBM® SPSS® Statistics Version 24.0 (IBM Corporation, Armonk, NY, USA). Depending on the scale of measurements and under consideration of distribution of values, statistical tests included Pearson Chi-Square test, Fisher’s Exact Test and independent samples T-Test. A level of statistical significance of p < .05 was applied. Missing values were considered to be missing at random and were discarded from analysis. Descriptive data were presented as mean ± standard deviation (SD) unless otherwise specified.
Results
Patient characteristics
One hundred nineteen glioma patients who underwent frameless stereotactic biopsy procedures from January 2011 to October 2017 were identified (Fig. 1). Fifty-five patients were female (46.2%). Mean age was 66.6 ± 13.0 years. Mean procedure duration was 74 ± 24 min. Major complications were intracranial hemorrhage in two cases resulting in worsening of neurological deficits and leading to a severe pneumonia in one during ICU stay. This patient deceased under best supportive care. Minor complications included mild and/or transient motor deficits without a correlating new pathology on CT scans in seven cases. Moreover, visual disturbances were present in two cases, a seizure in one case, brief reactive psychosis possibly related to anesthesia in one case and transient disturbances of consciousness due to cerebral edema in two cases. Table 1 provides an overview about demographic and clinical data.
Diagnostic yield
Grade A—a complete integrated diagnosis according to 2016 CNS WHO including grading and respective molecular information—was achieved in 110 cases (92.4%). Grade B, a histological description without definite classification of entity and WHO grade, was present in four cases (3.4%). In all these cases, an IDH status was available. Five patients (4.2%) had a non-diagnostic histology equaling Grade C. Consequently, analysis of IDH status could be performed in 95.8% and resulted in a cumulative mutation rate of 9.6%. Table 2 provides an overview about Grade B and C cases and further management. Two illustrative cases are depicted in Figs. 2 and 3.

Illustrative case with a Grade B diagnosis. MRI images (T1-weighted sequences with contrast agent) of a patient with a large right peritrigonal lesion (a) are shown. Biopsy was indicated due to the atypical imaging presentation compatible with lymphoma. b demonstrates the trajectory of a frameless stereotactic biopsy. A total of seven samples was collected at two different depths starting with the deepest location. The obtained samples were neuropathologically assessed as a malignant glial neoplasm, most likely an anaplastic astrocytoma. Consequently, resection of the glioma was discussed with the patient and performed afterwards. c, d depict the postoperative status. Histological examination of the resected tissue showed a glioblastoma multiforme, WHO IV

Illustrative case with a Grade C diagnosis. MRI images (T1-weighted sequences with contrast agent) of a case with a non-diagnostic biopsy are demonstrated. a, b show the planned trajectory of an initial frameless stereotactic biopsy of a left thalamic lesion. A total of six samples was taken at two different depths starting in the contrast-enhancing zone. Even though the hypointense biopsied areal can be seen within the anterior part of the lesion in the postoperative imaging (c, d), histological examination only yielded necrosis. e, f demonstrate the trajectory of a subsequent frame-based stereotactic biopsy with a deeper target point. Samples obtained with the second procedure revealed a glioblastoma multiforme, WHO IV, IDHwt
Intraoperative neuropathological examination
A frozen section was sent in 61 (51.3%) cases. It showed pathological changes in 46 cases (75.4%). Overall, diagnosis of the frozen section was congruent to final diagnosis in 48 cases (78.7%). Incongruent results were false negative frozen sections in 12 cases (19.7%). Moreover, in one case, frozen section diagnosis was most likely lymphoma and final diagnosis was glioblastoma. Negative frozen sections with a congruent non-diagnostic final biopsy result (‘true negative’) were present in three cases (4.9%). This results in a negative predictive value of 0.2. There were no false positive frozen sections. Procedures during which a frozen section was obtained were significantly longer (82 ± 26 vs. 65 ± 18 min; p < .001).
2016 CNS WHO diagnoses and molecular specifications
Among Grade A cases, the most common diagnosis was IDH-wildtype glioblastoma (66.4%). Second leading diagnosis was IDH-wildtype anaplastic astrocytoma (21.8%). IDH-mutation rate was 40.0%, 4.0% and 3.9% among WHO II, III and IV astrocytomas, respectively. IDH sequencing in accordance to 2016 CNS WHO recommendations revealed no new IDH mutations in previous R132H IDH1 negative cases. In one case, reprocessing with IDH-sequencing was not possible due to an insufficient amount of tissue. MGMT was successfully determined in 97 of 98 cases with an overall methylation rate of 68%. Table 3 provides more detailed information about Grade A diagnoses.
There were alterations in entity in 3.6% of Grade A cases when applying the 2016 CNS WHO instead of the 2007 CNS WHO. An initial anaplastic oligoastrocytoma was revised to an anaplastic oligodendroglioma, WHO III, IDH-mutant and 1p/19q-codeleted. In another case of oligoastrocytoma, testing for 1p/19q was inconclusive. Immunohistochemistry for ATRX showed retention, so the diagnosis of oligodendroglioma, WHO II, IDH-mutant, ATRX-wildtype, 1p/19q-NOS was given. Two diagnoses of gliomatosis cerebri were revised to diffuse astrocytomas with gliomatosis cerebri growth pattern. Figure 4 summarizes diagnoses given according to CNS WHO 2007 and 2016.

Distribution of 2007 and 2016 CNS WHO diagnoses. The pie charts show the distribution of diagnoses according to 2007 and 2016 CNS WHO. All Grade A diagnoses are included (n = 110). Abbreviations: AA anaplastic astrocytoma, AO anaplastic oligodendroglioma, AOA anaplastic oligoastrocytoma, DA diffuse astrocytoma, GBM glioblastoma, GC gliomatosis cerebri, mut IDH-mutant, O oligodendroglioma, OA oligoastrocytoma, wt IDH-wildtype
Influence of procedural variables on diagnostic yield
Influence of each of age, side, length of trajectory, tumor size, frozen section, imaging modality, contrast enhancement, burr hole position and procedure length on diagnostic yield was investigated using univariate analysis and was not significant (Table 4). Consequently, a multivariate analysis was not deemed useful.
Discussion
Frame-based stereotactic biopsies have been established as a reliable and safe method to obtain tissue samples of intracranial lesions [10]. Later on, frameless methods were introduced and several studies revealed comparable results between frame-based and image-guided frameless procedures regarding diagnostic yield and complication rate [11,12,13,14,15]. Nowadays, most frequently applied systems are the Stealth neuronavigation station™ or Stealth Treon™ (Medtronic Inc., Minneapolis, MN, USA) [12] and the Brainlab® Varioguide system (Brainlab AG, Munich, Germany) [7,8,9, 16], which was applied in the present study. Diagnostic yield of frameless image-guided biopsies has been reported to range between 87.0 and 100% for several techniques [3, 6, 7, 9, 12, 14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30]. A systematic literature review of Khatab et al. revealed a diagnostic yield of 93.8% based on 1628 procedures [31]. Since diagnostic yield has mostly not been defined, the authors proposed a definition which was applied on 235 biopsies [31]. The rate of a conclusive biopsy including type and grade according to 2007 CNS WHO was 72.8% and thus considerably lower than previously reported. Possibly, inconclusive biopsies with either an uncertain tumor type or grade might have been rated as fully diagnostic results in previous studies.
With the 2016 CNS WHO, requirements put on diagnostical information have become more demanding with a special focus on molecular specifications [2]. Ensuing from the previous diagnostic yield definition of Khatab et al. [31], an advanced definition involving basic molecular specifications to meet this development was proposed in this study. In the presented biopsied glioma cohort, diagnostic yield was 92.4%. This corresponds well to the aforementioned cumulative rate in the literature [31]. Likewise, studies also applying the Varioguide system presented similar results of diagnostic yield with 93% [9], 93.8% [7] and 93% [16]. A higher diagnostic yield than reported by Khatab et al. may be due to different baseline characteristics and particularly the exclusion of non-gliomas in the presented study [31]. Moreover, exclusion of cases with infratentorial or exceptional small lesions which have been biopsied with frame-based technique may create an additional bias. Interestingly, molecular processing seemed not to be a limiting factor in any case. Even in samples with inconclusive diagnoses rated as Grade B, information about IDH status was available including one detected mutation.
Univariate analysis identified no statistically significant procedural factors with impact on diagnostic yield in this frameless biopsy cohort. The main difference was a 16 min shorter procedure duration in the non-diagnostic group in contrast to previously reported significantly longer operating time in non-diagnostic procedures [3]. Other factors that were reported to be associated with non-diagnostic biopsies in previous studies include younger age, number of biopsies and infratentorial lesions [12, 31, 32]. Furthermore, intraoperative frozen-section histology has been associated with an increased number of diagnostic biopsy results [3, 10]. We were not able to confirm these findings in our study. The beneficial role of intraoperative neuropathological examination has already been doubted by Shooman et al. [29]. The poor negative predictive value of frozen sections in our retrospective analysis further challenges their routine necessity in frameless image-guided biopsies. An additional influencing factor not considered in this study may be the individual expertise of the neuropathologist.
The procedure related mortality was 0.8% in our study and consistent with the reported rate in the literature of 0.8–1.4% [6, 11, 14, 15, 31]. The rate of symptomatic hemorrhages was 1.7% in our cohort and has been previously described as 1–6% [5,6,7, 12, 20, 22, 30]. The majority of patients with a diagnostic biopsy were recommended for further therapy. Only in 10%, best supportive care was decided. From our understanding, this high rate of therapy initiation emphasizes the importance of neuropathological confirmation of glial neoplasms particularly in times of advancing knowledge about molecular prognostic and therapy-influencing factors [33]. This is in line to a study of Kim et al. demonstrating that stereotactic biopsy led to a change in preoperative presumed diagnosis in 49% and treatment strategy in 27% of cases [10]. Further management of Grade B and C biopsies was best supportive care in 22.2%. A recommendation for a second surgical procedure was given in 66.7% including resection and open or frame-based biopsy. This was conducted in six patients and led to a diagnostic result in all cases.
Entities were revised in four cases (3.4%) after application of the 2016 CNS WHO. This affected two oligoastrocytomas which were revised to oligodendrogliomas. The diagnosis of oligoastrocytoma is strongly discouraged in 2016 CNS WHO since almost every tumor in question can be classified either as an astrocytoma or oligodendroglioma based on molecular genetic testing like ATRX or 1p/19q [2, 34]. Moreover, since the diagnosis was removed from 2016 CNS WHO, two cases of previous gliomatosis cerebri were changed to diffuse astrocytomas with noting their special pattern of spread [2]. Large-scale molecular profiling showed that gliomatosis cerebri seems to be a heterogeneous group of diffuse gliomas rather than a distinct glioma entity [35].
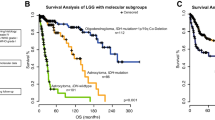
In our biopsy cohort, pathologies with unfavorable prognosis and molecular specifications seemed to be more common than in general glioma cohorts which have been previously reclassified [36, 37]. IDH-wildtype glioblastoma was the most frequent diagnosis with 66.4% followed by IDH-wildtype anaplastic astrocytoma with 21.8%. In historical glioma cohorts, IDH-wildtype glioblastoma was also the most common diagnosis but with a lower rate (27.0–33.1%) and followed by oligodendroglial entities [36, 37]. In contrast, oligodendroglial entities made up only 3.6% of the current study cohort. Moreover, we found a considerably higher IDH-wildtype rate of 60% and 96% in astrocytomas grade II and III, respectively, than it would have been expected from previous studies [38, 39]. This is of particular relevance since a major portion of IDH-wildtype astrocytomas have been shown to exhibit molecular profiles equivalent of glioblastoma (GBM) and such a diagnosis should be given cautiously [40]. The pivotal prognostic role of IDH in WHO II/III astrocytomas and importance of profiling has already been underlined [39, 41]. Since the prognosis in lower-grade astrocytomas seems to be more influenced by IDH status than WHO grade, the importance of a reliable molecular analysis in biopsy samples is emphasized [42].
The deviation in IDH distribution and dominance of more malignant entities between our cohort and the literature is notable and not explainable with certainty. Possibly, the variation might be due to the preselected biopsy cohort in the presented study and resulting differences in underlying patient characteristics including age. Generally, patients with intra-axial lesions more often receive resection without previous biopsy at our institution. The fact that patients in this study were primarily allocated to biopsy and not resection is at least partially attributed to a spatially more widespread and potentially also tumor-biologically more malignant disease. This more aggressive state might also be reflected by a higher rate of IDH-wildtype. However, another explanation would be that sensitivity to detect IDH mutations is lower for stereotactically sampled tissue. This might be due to more marginal tumor sampling or lower quantity of representative material being available for histopathological processing. Possibly, the number of vital tumor cells in already cell depleted diffuse gliomas is insufficient in small biopsy samples. Alternatively, biopsy tissue might not have been taken from histomorphologically representative tumor areas leading to underestimation of WHO grading while a correct molecular status was present. This potential risk of underdiagnosis due to sampling error might have been present in the few diagnoses of IDH-wildtype diffuse astrocytoma in this cohort and should generally be considered when interpreting stereotactically obtained samples.
MGMT methylation status has been identified as an independent prognostic factor and associated with a benefit from temozolomide [43]. In opposition to IDH status, it has not been described as part of the tumor terminology but as additional molecular feature in the 2016 CNS WHO [1]. Therefore, it has not been counted as determining factor for a complete diagnosis in the rating of diagnostic yield. It was tested in 98 samples (95 Grade A samples, 3 Grade B samples) with only one documented case of unsuccessful analysis. Notably, with 68.7% we observed a higher frequency of MGMT methylation in GBM patients than described in the literature [44].
The presented series is limited with regards to case number in comparison to the discussed large-scale studies. To ensure generalizability and confirmation of the presented findings, further case analyses of biopsied glioma patients appear to be useful.
Conclusion
A formally complete diagnosis according to 2016 CNS WHO was achieved in the majority of cases in the demonstrated series. Frameless stereotactic biopsy with the Varioguide system was confirmed to be a safe and reliable procedure. However, inaccurate or non-representative diagnoses in individual cases cannot be precluded. Moreover, a possible sampling error should be considered when interpreting stereotactically obtained tissue. Changes in entity according to the new classification applied only to few cases including oligoastrocytoma and gliomatosis cerebri. Distribution of entities and molecular profile differed from historical glioma populations favoring more malignant diagnoses, potentially reflecting the preselected nature of the cohort with regard to clinical and imaging characteristics.
In summary, frameless stereotactic biopsy seems to remain a useful diagnostic tool in contemporary neuro-oncology. Certain potential limitations should be considered in clinical practice.
Abbreviations
- AA:
-
Anaplastic astrocytoma
- CNS WHO:
-
World Health Organization classification of tumors of the central nervous system
- GBM:
-
Glioblastoma
- ICU:
-
Intensive care unit
- mRS:
-
Modified Rankin Scale
- SD:
-
Standard deviation
References
Banan R, Hartmann C (2017) The new WHO 2016 classification of brain tumors-what neurosurgeons need to know. Acta Neurochir 159(3):403–418. https://doi.org/10.1007/s00701-016-3062-3
Louis DN, Perry A, Reifenberger G, von Deimling A, Figarella-Branger D, Cavenee WK, Ohgaki H, Wiestler OD, Kleihues P, Ellison DW (2016) The 2016 World Health Organization classification of tumors of the central nervous system: a summary. Acta Neuropathol 131(6):803–820. https://doi.org/10.1007/s00401-016-1545-1
Dammers R, Schouten JW, Haitsma IK, Vincent AJ, Kros JM, Dirven CM (2010) Towards improving the safety and diagnostic yield of stereotactic biopsy in a single centre. Acta Neurochir 152(11):1915–1921. https://doi.org/10.1007/s00701-010-0752-0
Harrisson SE, Shooman D, Grundy PL (2012) A prospective study of the safety and efficacy of frameless, pinless electromagnetic image-guided biopsy of cerebral lesions. Neurosurgery 70(1 Suppl Operative):29–33. https://doi.org/10.1227/NEU.0b013e31822d75af. (discussion 33)
Livermore LJ, Ma R, Bojanic S, Pereira EA (2014) Yield and complications of frame-based and frameless stereotactic brain biopsy–the value of intra-operative histological analysis. Br J Neurosurg 28(5):637–644. https://doi.org/10.3109/02688697.2014.887657
Verploegh IS, Volovici V, Haitsma IK, Schouten JW, Dirven CM, Kros JM, Dammers R (2015) Contemporary frameless intracranial biopsy techniques: might variation in safety and efficacy be expected? Acta Neurochir 157(11):2011–2016. https://doi.org/10.1007/s00701-015-2543-0. (discussion 2016)
Gempt J, Buchmann N, Ryang YM, Krieg S, Kreutzer J, Meyer B, Ringel F (2012) Frameless image-guided stereotaxy with real-time visual feedback for brain biopsy. Acta Neurochir 154(9):1663–1667. https://doi.org/10.1007/s00701-012-1425-y
Buchalla R, Hopf-Jensen S, Rubarth O, Borm W (2013) Frameless navigated biopsy with the BrainLAB(R) VarioGuide system: a technical note. J Neurol Surg A 74(5):321–324. https://doi.org/10.1055/s-0032-1315790
Ringel F, Ingerl D, Ott S, Meyer B (2009) VarioGuide: a new frameless image-guided stereotactic system–accuracy study and clinical assessment. Neurosurgery 64(5 Suppl 2):365–371. https://doi.org/10.1227/01.neu.0000341532.15867.1c. (discussion 363–371)
Kim JE, Kim DG, Paek SH, Jung HW (2003) Stereotactic biopsy for intracranial lesions: reliability and its impact on the planning of treatment. Acta Neurochir 145(7):547–554. https://doi.org/10.1007/s00701-003-0048-8. (discussion 545–554)
Paleologos TS, Dorward NL, Wadley JP, Thomas DG (2001) Clinical validation of true frameless stereotactic biopsy: analysis of the first 125 consecutive cases. Neurosurgery 49(4):830–835. (discussion 835–837)
Dammers R, Haitsma IK, Schouten JW, Kros JM, Avezaat CJ, Vincent AJ (2008) Safety and efficacy of frameless and frame-based intracranial biopsy techniques. Acta Neurochir 150(1):23–29. https://doi.org/10.1007/s00701-007-1473-x
Dorward NL, Paleologos TS, Alberti O, Thomas DG (2002) The advantages of frameless stereotactic biopsy over frame-based biopsy. Br J Neurosurg 16(2):110–118
Smith JS, Quinones-Hinojosa A, Barbaro NM, McDermott MW (2005) Frame-based stereotactic biopsy remains an important diagnostic tool with distinct advantages over frameless stereotactic biopsy. J Neurooncol 73(2):173–179. https://doi.org/10.1007/s11060-004-4208-3
Woodworth GF, McGirt MJ, Samdani A, Garonzik I, Olivi A, Weingart JD (2006) Frameless image-guided stereotactic brain biopsy procedure: diagnostic yield, surgical morbidity, and comparison with the frame-based technique. J Neurosurg 104(2):233–237. https://doi.org/10.3171/jns.2006.104.2.233
Bradac O, Steklacova A, Nebrenska K, Vrana J, de Lacy P, Benes V (2017) Accuracy of varioguide frameless stereotactic system against frame-based stereotaxy: prospective, randomized, single-center Study. World Neurosurg 104:831–840. https://doi.org/10.1016/j.wneu.2017.04.104
Air EL, Leach JL, Warnick RE, McPherson CM (2009) Comparing the risks of frameless stereotactic biopsy in eloquent and noneloquent regions of the brain: a retrospective review of 284 cases. J Neurosurg 111(4):820–824. https://doi.org/10.3171/2009.3.jns081695
Bekelis K, Radwan TA, Desai A, Roberts DW (2012) Frameless robotically targeted stereotactic brain biopsy: feasibility, diagnostic yield, and safety. J Neurosurg 116(5):1002–1006. https://doi.org/10.3171/2012.1.jns111746
Czyz M, Tabakow P, Weiser A, Lechowicz-Glogowska BE, Zub LW, Jarmundowicz W (2014) The safety and effectiveness of low field intraoperative MRI guidance in frameless stereotactic biopsies of brain tumours-design and interim analysis of a prospective randomized trial. Neurosurg Rev 37(1):127–137. https://doi.org/10.1007/s10143-013-0486-6
Frati A, Pichierri A, Bastianello S, Raco A, Santoro A, Esposito V, Giangaspero F, Salvati M (2011) Frameless stereotactic cerebral biopsy: our experience in 296 cases. Stereotact Funct Neurosurg 89(4):234–245. https://doi.org/10.1159/000325704
Jain D, Sharma MC, Sarkar C, Gupta D, Singh M, Mahapatra AK (2006) Comparative analysis of diagnostic accuracy of different brain biopsy procedures. Neurol India 54(4):394–398
Lefranc M, Capel C, Pruvot-Occean AS, Fichten A, Desenclos C, Toussaint P, Le Gars D, Peltier J (2015) Frameless robotic stereotactic biopsies: a consecutive series of 100 cases. J Neurosurg 122(2):342–352. https://doi.org/10.3171/2014.9.jns14107
Lu Y, Yeung C, Radmanesh A, Wiemann R, Black PM, Golby AJ (2015) Comparative effectiveness of frame-based, frameless, and intraoperative magnetic resonance imaging-guided brain biopsy techniques. World Neurosurg 83(3):261–268. https://doi.org/10.1016/j.wneu.2014.07.043
Nishihara M, Takeda N, Harada T, Kidoguchi K, Tatsumi S, Tanaka K, Sasayama T, Kohmura E (2014) Diagnostic yield and morbidity by neuronavigation-guided frameless stereotactic biopsy using magnetic resonance imaging and by frame-based computed tomography-guided stereotactic biopsy. Surg Neurol Int 5(Suppl 8):S421–S426. https://doi.org/10.4103/2152-7806.140211
Zhang JS, Qu L, Wang Q, Jin W, Hou YZ, Sun GC, Li FY, Yu XG, Xu BN, Chen XL (2017) Intraoperative visualisation of functional structures facilitates safe frameless stereotactic biopsy in the motor eloquent regions of the brain. Br J Neurosurg. https://doi.org/10.1080/02688697.2017.1416059
Zhang QJ, Wang WH, Wei XP, Yu YG (2013) Safety and efficacy of frameless stereotactic brain biopsy techniques. Chin Med Sci J 28(2):113–116
Willems PW, Noordmans HJ, Ramos LM, Taphoorn MJ, Berkelbach van der Sprenkel JW, Viergever MA, Tulleken CA (2003) Clinical evaluation of stereotactic brain biopsies with an MKM-mounted instrument holder. Acta Neurochir 145(10):889–897. https://doi.org/10.1007/s00701-003-0112-4. (discussion 897)
Zoeller GK, Benveniste RJ, Landy H, Morcos JJ, Jagid J (2009) Outcomes and management strategies after nondiagnostic stereotactic biopsies of brain lesions. Stereotact Funct Neurosurg 87(3):174–181. https://doi.org/10.1159/000222661
Shooman D, Belli A, Grundy PL (2010) Image-guided frameless stereotactic biopsy without intraoperative neuropathological examination. J Neurosurg 113(2):170–178. https://doi.org/10.3171/2009.12.jns09573
Widhalm G, Minchev G, Woehrer A, Preusser M, Kiesel B, Furtner J, Mert A, Di Ieva A, Tomanek B, Prayer D, Marosi C, Hainfellner JA, Knosp E, Wolfsberger S (2012) Strong 5-aminolevulinic acid-induced fluorescence is a novel intraoperative marker for representative tissue samples in stereotactic brain tumor biopsies. Neurosurg Rev 35(3):381–391. https://doi.org/10.1007/s10143-012-0374-5. (discussion 391)
Khatab S, Spliet W, Woerdeman PA (2014) Frameless image-guided stereotactic brain biopsies: emphasis on diagnostic yield. Acta Neurochir 156(8):1441–1450. https://doi.org/10.1007/s00701-014-2145-2
Barnett GH, Miller DW, Weisenberger J (1999) Frameless stereotaxy with scalp-applied fiducial markers for brain biopsy procedures: experience in 218 cases. J Neurosurg 91(4):569–576. https://doi.org/10.3171/jns.1999.91.4.0569
Kondziolka D, Lunsford LD (1999) The role of stereotactic biopsy in the management of gliomas. J Neurooncol 42(3):205–213
Sahm F, Reuss D, Koelsche C, Capper D, Schittenhelm J, Heim S, Jones DT, Pfister SM, Herold-Mende C, Wick W, Mueller W, Hartmann C, Paulus W, von Deimling A (2014) Farewell to oligoastrocytoma: in situ molecular genetics favor classification as either oligodendroglioma or astrocytoma. Acta Neuropathol 128(4):551–559. https://doi.org/10.1007/s00401-014-1326-7
Herrlinger U, Jones DTW, Glas M, Hattingen E, Gramatzki D, Stuplich M, Felsberg J, Bahr O, Gielen GH, Simon M, Wiewrodt D, Schabet M, Hovestadt V, Capper D, Steinbach JP, von Deimling A, Lichter P, Pfister SM, Weller M, Reifenberger G (2016) Gliomatosis cerebri: no evidence for a separate brain tumor entity. Acta Neuropathol 131(2):309–319. https://doi.org/10.1007/s00401-015-1495-z
Tabouret E, Nguyen AT, Dehais C, Carpentier C, Ducray F, Idbaih A, Mokhtari K, Jouvet A, Uro-Coste E, Colin C, Chinot O, Loiseau H, Moyal E, Maurage CA, Polivka M, Lechapt-Zalcman E, Desenclos C, Meyronet D, Delattre JY, Figarella-Branger D (2016) Prognostic impact of the 2016 WHO classification of diffuse gliomas in the French POLA cohort. Acta Neuropathol 132(4):625–634. https://doi.org/10.1007/s00401-016-1611-8
Jiang H, Cui Y, Wang J, Lin S (2017) Impact of epidemiological characteristics of supratentorial gliomas in adults brought about by the 2016 world health organization classification of tumors of the central nervous system. Oncotarget 8(12):20354–20361. https://doi.org/10.18632/oncotarget.13555
Cancer Genome Atlas Research N, Brat DJ, Verhaak RG, Aldape KD, Yung WK, Salama SR, Cooper LA, Rheinbay E, Miller CR, Vitucci M, Morozova O, Robertson AG, Noushmehr H, Laird PW, Cherniack AD, Akbani R, Huse JT, Ciriello G, Poisson LM, Barnholtz-Sloan JS, Berger MS, Brennan C, Colen RR, Colman H, Flanders AE, Giannini C, Grifford M, Iavarone A, Jain R, Joseph I, Kim J, Kasaian K, Mikkelsen T, Murray BA, O’Neill BP, Pachter L, Parsons DW, Sougnez C, Sulman EP, Vandenberg SR, Van Meir EG, von Deimling A, Zhang H, Crain D, Lau K, Mallery D, Morris S, Paulauskis J, Penny R, Shelton T, Sherman M, Yena P, Black A, Bowen J, Dicostanzo K, Gastier-Foster J, Leraas KM, Lichtenberg TM, Pierson CR, Ramirez NC, Taylor C, Weaver S, Wise L, Zmuda E, Davidsen T, Demchok JA, Eley G, Ferguson ML, Hutter CM, Mills Shaw KR, Ozenberger BA, Sheth M, Sofia HJ, Tarnuzzer R, Wang Z, Yang L, Zenklusen JC, Ayala B, Baboud J, Chudamani S, Jensen MA, Liu J, Pihl T, Raman R, Wan Y, Wu Y, Ally A, Auman JT, Balasundaram M, Balu S, Baylin SB, Beroukhim R, Bootwalla MS, Bowlby R, Bristow CA, Brooks D, Butterfield Y, Carlsen R, Carter S, Chin L, Chu A, Chuah E, Cibulskis K, Clarke A, Coetzee SG, Dhalla N, Fennell T, Fisher S, Gabriel S, Getz G, Gibbs R, Guin R, Hadjipanayis A, Hayes DN, Hinoue T, Hoadley K, Holt RA, Hoyle AP, Jefferys SR, Jones S, Jones CD, Kucherlapati R, Lai PH, Lander E, Lee S, Lichtenstein L, Ma Y, Maglinte DT, Mahadeshwar HS, Marra MA, Mayo M, Meng S, Meyerson ML, Mieczkowski PA, Moore RA, Mose LE, Mungall AJ, Pantazi A, Parfenov M, Park PJ, Parker JS, Perou CM, Protopopov A, Ren X, Roach J, Sabedot TS, Schein J, Schumacher SE, Seidman JG, Seth S, Shen H, Simons JV, Sipahimalani P, Soloway MG, Song X, Sun H, Tabak B, Tam A, Tan D, Tang J, Thiessen N, Triche T Jr, Van Den Berg DJ, Veluvolu U, Waring S, Weisenberger DJ, Wilkerson MD, Wong T, Wu J, Xi L, Xu AW, Yang L, Zack TI, Zhang J, Aksoy BA, Arachchi H, Benz C, Bernard B, Carlin D, Cho J, DiCara D, Frazer S, Fuller GN, Gao J, Gehlenborg N, Haussler D, Heiman DI, Iype L, Jacobsen A, Ju Z, Katzman S, Kim H, Knijnenburg T, Kreisberg RB, Lawrence MS, Lee W, Leinonen K, Lin P, Ling S, Liu W, Liu Y, Liu Y, Lu Y, Mills G, Ng S, Noble MS, Paull E, Rao A, Reynolds S, Saksena G, Sanborn Z, Sander C, Schultz N, Senbabaoglu Y, Shen R, Shmulevich I, Sinha R, Stuart J, Sumer SO, Sun Y, Tasman N, Taylor BS, Voet D, Weinhold N, Weinstein JN, Yang D, Yoshihara K, Zheng S, Zhang W, Zou L, Abel T, Sadeghi S, Cohen ML, Eschbacher J, Hattab EM, Raghunathan A, Schniederjan MJ, Aziz D, Barnett G, Barrett W, Bigner DD, Boice L, Brewer C, Calatozzolo C, Campos B, Carlotti CG Jr, Chan TA, Cuppini L, Curley E, Cuzzubbo S, Devine K, DiMeco F, Duell R, Elder JB, Fehrenbach A, Finocchiaro G, Friedman W, Fulop J, Gardner J, Hermes B, Herold-Mende C, Jungk C, Kendler A, Lehman NL, Lipp E, Liu O, Mandt R, McGraw M, McLendon R, McPherson C, Neder L, Nguyen P, Noss A, Nunziata R, Ostrom QT, Palmer C, Perin A, Pollo B, Potapov A, Potapova O, Rathmell WK, Rotin D, Scarpace L, Schilero C, Senecal K, Shimmel K, Shurkhay V, Sifri S, Singh R, Sloan AE, Smolenski K, Staugaitis SM, Steele R, Thorne L, Tirapelli DP, Unterberg A, Vallurupalli M, Wang Y, Warnick R, Williams F, Wolinsky Y, Bell S, Rosenberg M, Stewart C, Huang F, Grimsby JL, Radenbaugh AJ, Zhang J (2015) Comprehensive, integrative genomic analysis of diffuse lower-grade gliomas. New Engl J Med 372(26):2481–2498. https://doi.org/10.1056/NEJMoa1402121
Killela PJ, Pirozzi CJ, Healy P, Reitman ZJ, Lipp E, Rasheed BA, Yang R, Diplas BH, Wang Z, Greer PK, Zhu H, Wang CY, Carpenter AB, Friedman H, Friedman AH, Keir ST, He J, He Y, McLendon RE, Herndon JE 2nd, Yan H, Bigner DD (2014) Mutations in IDH1, IDH2, and in the TERT promoter define clinically distinct subgroups of adult malignant gliomas. Oncotarget 5(6):1515–1525. https://doi.org/10.18632/oncotarget.1765
Reuss DE, Kratz A, Sahm F, Capper D, Schrimpf D, Koelsche C, Hovestadt V, Bewerunge-Hudler M, Jones DT, Schittenhelm J, Mittelbronn M, Rushing E, Simon M, Westphal M, Unterberg A, Platten M, Paulus W, Reifenberger G, Tonn JC, Aldape K, Pfister SM, Korshunov A, Weller M, Herold-Mende C, Wick W, Brandner S, von Deimling A (2015) Adult IDH wild type astrocytomas biologically and clinically resolve into other tumor entities. Acta Neuropathol 130(3):407–417. https://doi.org/10.1007/s00401-015-1454-8
Olar A, Wani KM, Alfaro-Munoz KD, Heathcock LE, van Thuijl HF, Gilbert MR, Armstrong TS, Sulman EP, Cahill DP, Vera-Bolanos E, Yuan Y, Reijneveld JC, Ylstra B, Wesseling P, Aldape KD (2015) IDH mutation status and role of WHO grade and mitotic index in overall survival in grade II-III diffuse gliomas. Acta Neuropathol 129(4):585–596. https://doi.org/10.1007/s00401-015-1398-z
Reuss DE, Mamatjan Y, Schrimpf D, Capper D, Hovestadt V, Kratz A, Sahm F, Koelsche C, Korshunov A, Olar A, Hartmann C, Reijneveld JC, Wesseling P, Unterberg A, Platten M, Wick W, Herold-Mende C, Aldape K, von Deimling A (2015) IDH mutant diffuse and anaplastic astrocytomas have similar age at presentation and little difference in survival: a grading problem for WHO. Acta Neuropathol 129(6):867–873. https://doi.org/10.1007/s00401-015-1438-8
Hegi ME, Diserens AC, Gorlia T, Hamou MF, de Tribolet N, Weller M, Kros JM, Hainfellner JA, Mason W, Mariani L, Bromberg JE, Hau P, Mirimanoff RO, Cairncross JG, Janzer RC, Stupp R (2005) MGMT gene silencing and benefit from temozolomide in glioblastoma. New Engl J Med 352(10):997–1003. https://doi.org/10.1056/NEJMoa043331
Zhang K, Wang XQ, Zhou B, Zhang L (2013) The prognostic value of MGMT promoter methylation in glioblastoma multiforme: a meta-analysis. Fam Cancer 12(3):449–458. https://doi.org/10.1007/s10689-013-9607-1
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. For this type of study formal consent is not required.
Rights and permissions
About this article

Cite this article
Mader, M.MD., Rotermund, R., Martens, T. et al. The role of frameless stereotactic biopsy in contemporary neuro-oncology: molecular specifications and diagnostic yield in biopsied glioma patients. J Neurooncol 141, 183–194 (2019). https://doi.org/10.1007/s11060-018-03024-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11060-018-03024-8