
Abstract
Radiation therapy plays a central role in the management of glioblastoma. Although primarily thought of as modality to provide local tumor control through DNA damage, the capacity of ionizing radiation to modulate tumor immune response has long been recognized. The recent emergence of clinically active immunotherapies offers exciting potential for harnessing the immune modulatory effects or radiation through combinatorial strategies designed to enhance clinical outcomes. In this Review, we provide background describing the unique immune environment within the central nervous system, how ionizing radiation may modulate the tumor immune response, preclinical and clinical data testing the combination of radiation and immune modulating agents, and highlight some of the current challenges in extending these findings clinically.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Background
The concept of a tumor antigen recognizable by the host immune system was hypothesized over 50 years ago [1,2,3] and was followed by decades of controversy. The first irrefutable evidence came forward from Thierry Boon’s lab, demonstrating that adoptive transfer of T-cells isolated from tumor rejecting mice provided immunity to lymphodepleted mice [4, 5]. The presence of tumor antigens has since been firmly established in the field, with recent technological innovations allowing the identification of a repertoire neoantigens that arise as a consequence of tumor-specific mutations [6, 7]. Further, the capacity of a tumor to actively evade the host immune response has been identified as a hallmark of cancer [8]. Although known to play an important role in tumorigenesis for decades, strategies designed to harness the host immune response have only recently been successfully translated into the clinic, revolutionizing cancer therapy.
Immune evasion in cancer
Despite the presence of recognizable antigens, tumors are able to actively evade the host immune response through immune tolerance. Immune tolerance is important in normal physiology to both promote self-tolerance and prevent over-reactivity of the immune system to various environmental entities and dysfunction of these immune response “brakes” may lead to a variety of disorders, including autoimmune diseases, asthma, and allergy. Tumors have evolved numerous mechanisms to co-opt these immune signaling pathways, thereby creating a tolerogenic microenvironment. Of these mechanisms, immune checkpoints have received recent attention, including cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) and programmed death-1 (PD-1), which represent negative regulators of T-cell activation. Tumors have evolved mechanisms to elicit sustained activation of these pathways and checkpoint blockade immunotherapy, with such agents as ipilimumab and pembrolizumab, have demonstrated unprecedented clinical activity in a variety of malignancies [9]. Another emerging immune checkpoint with particular relevance to glioblastoma is the indoleamine 2,3-dioxygenase (IDO) and tryptophan 2,3-dioxygenase (TDO) pathway [10, 11], whose most notable physiologic role has been attributed to peripheral immune tolerance and fetal protection from maternal immune rejection in the placenta [12]. IDO and TDO metabolize tryptophan to the metabolite kynurenine, which contributes towards immune tolerance through recruitment of immune suppressive cells such as myeloid derived suppressor cells (MDSCs) and regulatory T-cells. Therefore, targeting the IDO/TDO pathway may serve as another strategy of immunologic checkpoint blockade that is actively being investigated [11].
Immune surveillance in the central nervous system (CNS)
The CNS was previously considered an immune privileged site, largely based on experimental data demonstrating difficulty in initiating a destructive T-cell response from inside the CNS parenchyma. For example, foreign tissue grafts survive for prolonged periods when placed within the parenchyma of the CNS as compared with being placed under the skin [13]. However, such grafts within the parenchymal CNS are rapidly rejected by the immune system after the same tissue is grafted under the skin, demonstrating that T-cells activated outside the CNS can readily detect their antigenic targets even when located within the CNS parenchyma. Further, non-parenchymal sites within the CNS, including ventricles, meninges and the subarachnoid spaces, demonstrate a robust proinflammatory T-cell response to grafted tissue. Although the CNS lacks a traditional lymphatic system, recent findings identified a rich lymphatic network in the dura, able to absorb and transport CSF into the deep cervical lymph nodes, where CNS antigens have been previously reported [14, 15]. A functional immune system in the CNS is further corroborated by the striking radiographic responses that are likely associated with pseudoprogression observed in melanoma brain metastases and glioblastoma following treatment with immune checkpoint inhibitors [16, 17]. In addition to modulating immune checkpoints, glioblastoma produce an array of chemokines such as IL-8, CCL2, CXCL12 [18], CXCL16 [19] that are able to recruit suppressive tumor-associated macrophages (TAMs) and MDSCs, furthering the tolerogenic tumor microenvironment.
Harnessing the immune system in cancer therapy
Various strategies have been utilized to harness the host immune response in cancer treatment. Rather than “releasing the brakes” that contributes towards immune tolerance with checkpoint inhibitors described above, initial immunotherapeutic approaches utilized high dose interleukin 2 (IL-2) to boost the activation of cytotoxic T cells, or in other word, “accelerate” the host immune response. Promising approaches currently under investigation are designed to “educate” a patient’s own immune cells to recognize and attack tumors. One such therapy utilizes adoptive transfer of patient-derived ex vivo cultured dendritic cells (DC) pulsed with tumor-specific peptide. These DCs are then used for vaccinating the patient, resulting in increased innate and adaptive immune response. A similar cell based immunotherapy involves the collection of a patient’s own T-cells that are then genetically engineered to produce tumor-specific antigen receptors on their surface called chimeric antigen receptors (CAR). These engineered CAR T-cells are then expanded in the laboratory and infused back into the patient, serving as a living drug. CAR-T cells show great promise in the clinic, as they are highly specific and are not restricted by the major histocompatibility complex (MHC) [20]. Another promising cell based immunotherapeutic approach is the use of tumor-infiltrating lymphocytes (TILs) isolated from tumor-bearing individuals, expanding them ex vivo, and then administering them back to the patient to strengthen the immune response. Glioblastoma is also known to uniquely express high levels of epidermal growth factor receptor variant III (EGFRvIII), and vaccination against this mutated receptor had initially shown encouraging results [21], but unfortunately, a subsequent Phase III study failed to show a therapeutic benefit from this approach [22]. Another recent therapeutic approach utilizes injection of oncolytic viruses into the tumor site. One such virus that has received recent attention is poliovirus, which can naturally detect CD155 receptors and use it as a guide to enter glioma cells, and genetically engineered to preferentially infect and kill cancer cells [23].
Radiation and immune recognition
Radiation therapy is an established part of the standard of care for many CNS malignancies. Radiation is classically known to function by inducing DNA damage leading to apoptosis or mitotic catastrophe. However, the effects of radiation on tumor cells, stromal cells, and leukocytes within the tumor microenvironment are complex and not yet fully understood. For example, radiation has recently been demonstrated to activate multiple molecular and transcriptional pathways, which can modulate immune responses and change the immunophenotype of tumor cells [24]. These findings have led to an emerging field of harnessing the immunomodulatory effects of CNS radiation to enhance immune response and synergize with immunotherapy. Here, we briefly describe the diverse role that radiation can play in multiple steps of anti-tumor immune responses.
The first steps in developing an immune response are antigen uptake, processing, and presentation by professional antigen presenting cells, namely macrophages, dendritic cells, and B-cells. In this regard, the localized cytotoxic effects of radiation have been shown to cause inflammatory tumor cell death (ICD). Key characteristics of radiation induced ICD include release of ATP, translocation of calreticulin to the cell surface, and release of HMGB1 [25, 26]. Translocation of calreticulin to the tumor cell surface is a potent “eat me” signal and causes APC to rapidly phagocytosize tumor cells and begin to process their antigens. At the same time, the presence of HMGB1 is a critical damage associated molecular pattern or “danger signal” that results in dendritic cell maturation and migration, enhancing immunogenic antigen presentation. Mature dendritic cells can then enter draining lymphatics and migrate back to regional lymph nodes or spleen to present antigens directly to CD4 helper T-cells or cross present tumor antigen to CD8 cytotoxic T-cells to induce antigen specific immune responses [27, 28]. Thus, radiation can play a distinct role in the initial step of priming the immune system to tumor-derived antigens.
The immune stimulatory effects of radiation are not limited to priming, as radiation can also enhance downstream effector immune responses and T-cell mediated cytotoxicity. In order for a T-cell to lyse a tumor cell, it must be able to infiltrate or invade into the tumor microenvironment. Multiple groups have shown that radiation can modulate tumor vasculature and enhance T-cell extravasation leading to increases in TILs. Importantly, radiation induced modulation or permeabilization of the blood–brain barrier may be critical to allow a peripheral T-cell to infiltrate or invade into a CNS tumor. In this regard, focused or stereotactic radiation might even be able to serve as a targeting strategy to allow for localized migration of cytotoxic effector cells. Interestingly, radiation has also been reported to influence expression of cytokines and chemokines, such as IL-1, IL-2, L-6, TNF-alpha, TGF-beta, CXCL-16, as well as Type I and Type II interferons, which may play a key role in modulating immune responses, but may also enhance T-cell directed extravasation via chemokine gradients. Thus in addition to priming immune responses, focused radiation may help to permeablize tumors and enhance T-cell infiltration.
Once a T-cell has entered the tumor microenvironment it may face an uphill battle in attempting to overcome an immunosuppressive tumor microenvironment or direct tumor cell mediated immunosuppression. Thus preconditioning or modifying the tumor immunophenotype may be critical to permitting robust cytotoxic effector immune responses. The primary target for the T-cell receptor is MHC loaded with tumor antigen. Along these lines, multiple different groups have shown that radiation results in dramatic dose dependent upregulation of MHC on the tumor cell surface [27, 29,30,31]. Thus, directly increasing the density of targets for T-cells on the tumor cell surface. Given this, it is not surprising that groups have demonstrated that radiation can cause tumor cells to become intrinsically more susceptible to immune mediated cell death [30,31,32].
Given these multiple effects with radiation alone, there has been a dedicated effort to combine radiation with various immunotherapies with sometimes striking results both within and outside of the radiation field (abscopal responses). Of note, if a systemic immune response is able to be primed with radiation, then it might be expected to have activity outside of the initial radiation field. Intriguingly, some authors have suggested that the therapeutic effects of radiation may depend on the host immune system and anti-tumor immune responses [33,34,35]. Overall these recent findings and developments have spurred great interest in combining radiation with immunotherapy in attempt to enhance local or even systemic disease control. In addition to the studies described below, a number of excellent reviews have also highlighted the potential benefits and ongoing clinical trials of radiation combined with immunotherapy [36,37,38,39,40].
Preclinical studies combining RT with immune modulation
Current strategies have focused on combining vaccines, checkpoint inhibitors, cytokine therapy, adoptive therapies, and toll like receptors with radiation. The various combinations and permutations of combination approaches for immunotherapy highlight the need of preclinical models to study mechanism and efficacy of various immunotherapy strategies.
Preclinical data suggest that radiation augments immunotherapy strategies in glioblastoma [39, 41,42,43]. Checkpoint molecules strategies clearly benefit from the addition of radiation in inducing an anti-tumor immune response in animal models. In a GL261 glioma model, the combination of anti-PD-1 and focal radiation has been shown to be synergistic and induced systemic memory [39]. Other studies looking at the combination of anti-CTLA-4, anti-CD137, anti-GITR, and anti-Tim-3 with radiation also have observed synergy and a durable antitumor immune response [41,42,43]. Other strategies using vaccines, cytokines such as IL-2, toll-like receptors, and adoptive therapies have also benefitted from radiation [44].
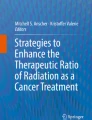
In addition to assessing the efficacy of various immunotherapy strategies, animal models allow us to ask important clinically relevant questions, including sequencing of radiation with immunotherapy. In the setting of anti-CTLA-4, our group demonstrated that the administration of anti-CTLA-4 before or after radiation did not compromise efficacy [41]. As a result, this study allowed us to design our clinical trial to have a window for radiation treatment around the time of checkpoint molecule administration. Figure 1 highlights some different forms of immunotherapy and potential mechanisms underlying its interaction with radiation.

Schematic highlighting different forms of immunotherapy and potential mechanisms underlying their interaction with radiation
Ongoing clinical trials
Given the disappointing results from chemotherapy and targeted therapies, there has been considerible interest in treatment strategies that harness host immune response against glioblastoma. Initial trials have been focused on vaccines, such as the one generated by ex vivo stimulation of autologous dendritic cells with a six-candidate peptide cocktail, ICT-107 [45]. Although well tolerated, the result of a randomized phase II trial of this vaccine has indicated clinical activity only in patients with positive HLA-A2 [45]. A larger randomized phase III trial of this vaccine in patients with newly diagnosed glioblastoma and positive HLA-A2 is ongoing (NCT02546102). Rindopepimut, a vaccine targeting epidermal growth factor variant III (EGFRvIII), had shown encouraging results in small phase II trials in combination with radiation therapy and temozolomide or bevacizumab [46, 47]. However, interim analysis of a large phase III trial (ACT IV) in patients with newly diagnosed glioblastoma harboring EGFRvIII failed to show survival benefit for rindopepimut and the trial was terminated [22].
More recently, major emphasis has been placed on the use of CAR T-cell therapies (NCT01109095, NCT02664363) and blockade of checkpoint proteins such as PD-1/PD-L1. Preliminary results of a phase 1 trial investigating the safety of autologous HER2 CMV bispecific CAR T cells are promising [48]. Infusion of HER2 CMV bispecific CAR T cells have shown to be safe with no severe adverse events or a cytokine release syndrome. One patient achieved partial response (durable for more than 10 months) and five out of 16 patients had stable disease lasting for longer than 10 weeks [48]. However, the CAR T-cell therapies are still in early clinical testing and results are from single institutional trials with small number of highly selected patients.
Expression of PD-1 and PD-L1 is found in the microenvironment of high grade glioma and correlates with worse outcome [49, 50], however the extent of PD-L1 expression remains unclear, with reports ranging between 2.7 and 88% [49, 50]. CheckMate-143 (NCT02017717) is a large, randomized, phase III trial in which patients with first recurrence of glioblastoma are randomized to nivolumab, a fully human IgG4 monoclonal antibody to the PD-1 receptor, vs. bevacizumab. This study included initial safety cohorts that assessed the toxicity of nivolumab alone or in combination with ipilimumab, a fully humanized anti-CTLA-4 IgG1 monoclonal antibody. No new or unexpected adverse events were observed in patients with glioblastoma. As reported in patients with other tumor types, nivolumab monotherapy was associated with lower toxicity in comparison to the combinations of nivolumab and ipilimumab [51]. Nine month survival rate was 60% in the nivolumab monotherapy cohort and one partial response (out of 10 patients) was observed [51]. These promising results led to the initiation of a Phase 3 portion of this trial. Other ongoing trials are investigating the role of anti PD-1/PD-L1 antibodies in combination with anti-angiogenic drugs, vaccines, oncolytic viruses, and other immune-modulating agents.
As discussed previously, an established body of published work has shown that radiotherapy synergizes with check point inhibitors and produces tumor regression and long-term survival in a variety of murine cancer models [39, 52, 53]. Strong pre-clinical data and clinical observation of abscopal effects in patients treated with localized radiation and checkpoint inhibitors provide rationale to study this combinatory regimen in patients with advanced malignancies, including glioblastoma [54]. Several ongoing trials are evaluating the safety and efficacy of combining anti-PD1/PD-L1 antibodies with radiotherapy in glioblastoma and other advanced malignancies. Thus far, these combinations have shown to be safe with limited toxicity. Preliminary results of a phase 1 trial of REGN2810, an IgG4 antibody against PD-1, administered alone or with hypofractionated radiotherapy in patients with advanced solid malignancies has suggested that radiation may shorten time to response and improve responsiveness of tumor types considered refractory to anti-PD1/PD-L1 monotherapy [55].
Anti PD-1/PD-L1 blockade in combination with radiotherapy is currently being investigated in patients with newly diagnosed or recurrent glioblastoma (Table 1). However, the optimal radiation dose, fractionation, and sequencing with immunotherapy remain to be determined. Pre-clinical data have suggested that hypofractionated radiation at a dose of 5–20 Gy per fraction may be better than conventionally fractionated schemes of 1.8–2.2 Gy fractions [24]. Clinical trials investigating the combination of hypofractionated radiotherapy with anti PD1/PD-L1 blockade or IDO inhibitors in glioblastoma patients are underway (NCT02313272, NCT02829931, and NCT02052648). Preliminary data from our phase I trial (NCT02313272) assessing safety and efficacy of hypofractionated radiotherapy (30 Gy delivered in five fractions) with pembrolizumab (100–200 mg every 3 weeks) and bevacizumab (10 mg every 2 weeks) has shown an acceptable toxicity profile with no grade 3–4 treatment related adverse events or radionecrosis. Preliminary data on efficacy are encouraging with durable responses being observed [56].
Current challenges
Although the combination of immunotherapy and radiation holds strong promise, complexities underlying their complementary modes of activity require further understanding to more efficiently exploit the synergy between these modalities. For example, as we identify novel strategies to modulate the host immune response to target glioblastoma, attention must be made for the potential role standard treatment plays in contributing towards immunosuppression. It has recently been demonstrated that severe lymphopenia is common following radiation and temozolomide in malignant glioma and associated with poor prognosis [57], therefore, the efficacy of immunomodulatory strategies could be mitigated in these immunocompromised patients. Although the contributory role of temozolomide on bone marrow suppression is established, radiation alone has also been implicated in lymphopenia in brain tumor patients [58,59,60]. As it is hypothesized that this observed lymphopenia is secondary to eradication of circulating lymphocytes during daily radiation treatments, a variety of radiation delivery strategies may be tested to limit this effect. This includes limiting of the total volume of brain treated by decreasing treatment margins or by using more stringent dosimetric parameters that may be achieved using modern delivery techniques, including proton therapy. Decreasing overall treatment time from 6 weeks of daily therapy to 1–3 weeks using hypofractionated radiation regimens may also influence lymphopenia in brain tumor patients. Implementing radiation protectors and pre-radiation lymphocyte harvesting followed by post-radiation infusion represent additional strategies currently being evaluated to reduce radiation-induced lymphophenia [58, 61]. Interestingly, recent clinical data identified that a potent cellular and humoral immune response can be generated and maintained to an EGFRvIII-targeted peptide vaccine despite lymphopenia in these patients, suggesting further work still needs to be done in this area [62]. However, two recent large clinical trials that compared radiation alone to temozolomide in elderly patients with glioblastoma [63] and low grade glioma [64] both demonstrated far lower levels of radiation-induced immunosuppression, so the influence of standard, fractionated radiation on immunosuppression in glioblastoma patients and its clinical relevance requires further investigation.
Another active area of investigation involves identifying an optimal radiation dose and fractionation schedule to be used in concert with immunotherapy. As it has been suggested that doses greater than the traditional 2 Gy per fraction may elicit a more robust immunogenic response, combinatorial strategies involving hypofractionation regimens holds promise. In addition to exploiting this potential synergy and significantly decreasing overall treatment time for the patient, hypofractionation may result in an additional benefit of decreasing treatment-related lymphopenia, as described above, making it a particularly attractive strategy to explore when combined with immunotherapy. In addition to dose, how best to sequence these treatment modalities needs to be determined and may depend on the specific mechanism of action of an individual agent.
Another challenge when combining immunotherapy and radiation with particular relevance to glioblastoma involves potentiating treatment related effects, often referred to as pseudoprogression. We have learned over the last decade that combining temozolomide with radiation can result in pseudoprogression, with radiographic changes suggesting tumor progression that subsequently resolve on further imaging [65]. A similar phenomenon has been described with immune checkpoint agents alone when used in both glioma and brain metastases [16]. Therefore, the combination of these three modalities may lead to a more robust pseudoprogression. In addition to representing a diagnostic challenge, increases in treatment related effects may also result in a therapeutic challenge, as steroids typically used to treat symptoms associated with pseudoprogression may attenuate the efficacy of the prescribed immune therapy. Therefore, careful consideration of sequencing will be critical for the successful development of clinical strategies testing these various combinations, as any predicted synergies with concurrent treatment will need to be balanced with their possible side effects.
Lastly, applying preclinical models that more accurately recapitulate the breadth of human disease may provide additional insight into the tolerogenic environment of glioblastoma and its interplay with radiation. As an immunocompetant preclinical model is required for such studies, an overwhelming majority of work has been performed using the murine glioma line GL261 grown in C57BL/6 mice. Although such studies provide meaningful direction, applying data generated from a single model will have a limited capacity in guiding personalized therapy using a potential diverse panel of immune modulatory agents. Therefore, extending investigations using adult astrocytic genetically engineered mouse models may complement our current level of understanding. However, a clear limitation with such models is that they are still murine tumors being evaluated in the context of a murine immune system. Recent developments in mouse modeling have generated mice deficient in both adaptive and innate immune systems, including the NOD-scid IL2r null (NSG) strain, which can be engrafted with functional human immune systems [66]. This permits the potential to study a diverse panel of patient derived tumors or tumor initiating cells in vivo in the presence of a human immune system. It can be expected that these novel model systems will provide important direction to help translate laboratory findings into the clinic.
References
Klein G, Sjogren HO, Klein E, Hellstrom KE (1960) Demonstration of resistance against methylcholanthrene-induced sarcomas in the primary autochthonous host. Cancer Res 20:1561–1572
Prehn RT, Main JM (1957) Immunity to methylcholanthrene-induced sarcomas. J Natl Cancer Inst 18:769–778
Burnet M (1957) Cancer; a biological approach. I. The processes of control. Br Med J 1:779–786
Boon T, Kellermann O (1977) Rejection by syngeneic mice of cell variants obtained by mutagenesis of a malignant teratocarcinoma cell line. Proc Natl Acad Sci USA 74:272–275
Uyttenhove C, Snick JV, Boon T (1980) Immunogenic variants obtained by mutagenesis of mouse mastocytoma P815. I. Rejection by syngeneic mice. J Exp Med 152:1175–1183
Rizvi NA, Hellmann MD, Snyder A, Kvistborg P, Makarov V, Havel JJ et al (2015) Mutational landscape determines sensitivity to PD-1 blockade in non–small cell lung cancer. Science 348:124–128
McGranahan N, Furness AJ, Rosenthal R, Ramskov S, Lyngaa R, Saini SK et al (2016) Clonal neoantigens elicit T cell immunoreactivity and sensitivity to immune checkpoint blockade. Science 351:1463–1469
Hanahan D, Weinberg RA (2011) Hallmarks of cancer: the next generation. Cell 144:646–674
Robert C, Schachter J, Long GV, Arance A, Grob JJ, Mortier L et al (2015) Pembrolizumab versus Ipilimumab in advanced melanoma. N Engl J Med 372:2521–2532
Opitz CA, Litzenburger UM, Sahm F, Ott M, Tritschler I, Trump S et al (2011) An endogenous tumour-promoting ligand of the human aryl hydrocarbon receptor. Nature 478:197–203
Wainwright DA, Balyasnikova IV, Chang AL, Ahmed AU, Moon K-S, Auffinger B et al (2012) IDO expression in brain tumors increases the recruitment of regulatory T cells and negatively impacts survival. Clin Cancer Res 18:6110–6121
Munn DH, Zhou M, Attwood JT, Bondarev I, Conway SJ, Marshall B et al (1998) Prevention of allogeneic fetal rejection by tryptophan catabolism. Science 281:1191–1193
Perry VH (1998) A revised view of the central nervous system microenvironment and major histocompatibility complex class II antigen presentation. J Neuroimmunol 90:113–121
Aspelund A, Antila S, Proulx ST, Karlsen TV, Karaman S, Detmar M et al (2015) A dural lymphatic vascular system that drains brain interstitial fluid and macromolecules. J Exp Med 212:991–999
Louveau A, Harris TH, Kipnis J (2015) Revisiting the mechanisms of CNS immune privilege. Trends Immunol 36:569–577
Cohen JV, Alomari AK, Vortmeyer AO, Jilaveanu LB, Goldberg SB, Mahajan A et al (2015) Melanoma brain metastasis pseudoprogression after pembrolizumab treatment. Cancer Immunol Res 4(3):1–4
Okada H, Weller M, Huang R, Finocchiaro G, Gilbert MR, Wick W et al (2015) Immunotherapy response assessment in neuro-oncology: a report of the RANO working group. Lancet Oncol 16:e534–e542
Rempel SA, Dudas S, Ge S, Gutiérrez JA (2000) Identification and localization of the cytokine SDF1 and its receptor, CXC chemokine receptor 4, to regions of necrosis and angiogenesis in human glioblastoma. Clin Cancer Res 6:102–111
Ludwig A, Schulte A, Schnack C, Hundhausen C, Reiss K, Brodway N et al (2005) Enhanced expression and shedding of the transmembrane chemokine CXCL16 by reactive astrocytes and glioma cells. J Neurochem 93:1293–1303
Chow KKH, Naik S, Kakarla S, Brawley VS, Shaffer DR, Yi Z et al (2013) T cells redirected to EphA2 for the immunotherapy of glioblastoma. Mol Ther 21:629–637
Sampson JH, Heimberger AB, Archer GE, Aldape KD, Friedman AH, Friedman HS et al (2010) Immunologic escape after prolonged progression-free survival with epidermal growth factor receptor variant III peptide vaccination in patients with newly diagnosed glioblastoma. J Clin Oncol 28:4722–4729
Weller M, Butowski N, Tran D, Recht L, Lim M, Hirte H, et al (2016) ATIM-03. ACT IV: an international, double-Blind, Phase 3 trial of rindopepimut in newly diagnosed, EGFR vIII-expressing glioblastoma. Neuro Oncol 18:vi17–vi18
Gromeier M, Lachmann S, Rosenfeld MR, Gutin PH, Wimmer E (2000) Intergeneric poliovirus recombinants for the treatment of malignant glioma. Proc Natl Acad Sci USA 97:6803–6808
Sharabi AB, Lim M, DeWeese TL, Drake CG. (2015) Radiation and checkpoint blockade immunotherapy: radiosensitisation and potential mechanisms of synergy. Lancet Oncol 16:e498–e509
Gameiro SR, Jammeh ML, Wattenberg MM, Tsang KY, Ferrone S, Hodge JW (2014) Radiation-induced immunogenic modulation of tumor enhances antigen processing and calreticulin exposure, resulting in enhanced T-cell killing. Oncotarget 5:403–416
Rovere-Querini P, Capobianco A, Scaffidi P, Valentinis B, Catalanotti F, Giazzon M et al (2004) HMGB1 is an endogenous immune adjuvant released by necrotic cells. EMBO Rep 5:825–830
Sharabi AB, Nirschl CJ, Kochel CM, Nirschl TR, Francica BJ, Velarde E, et al (2015) Stereotactic radiation therapy augments antigen-specific PD-1–mediated antitumor immune responses via cross-presentation of tumor antigen. Cancer Immunol Res 3:345–355
Bernstein MB, Garnett CT, Zhang H, Velcich A, Wattenberg MM, Gameiro SR et al (2014) Radiation-induced modulation of costimulatory and coinhibitory T-cell signaling molecules on human prostate carcinoma cells promotes productive antitumor immune interactions. Cancer Biother Radiopharm 29:153–161
Hauser SH, Calorini L, Wazer DE, Gattoni-Celli S (1993) Radiation-enhanced expression of major histocompatibility complex class I antigen H-2Db in B16 melanoma cells. Cancer Res 53:1952–1955
Garnett CT, Palena C, Chakarborty M, Tsang K-Y, Schlom J, Hodge JW (2004) Sublethal irradiation of human tumor cells modulates phenotype resulting in enhanced killing by cytotoxic T lymphocytes. Cancer Res 64:7985–7994
Reits EA, Hodge JW, Herberts CA, Groothuis TA, Chakraborty M, Wansley EK et al (2006) Radiation modulates the peptide repertoire, enhances MHC class I expression, and induces successful antitumor immunotherapy. J Exp Med 203:1259–1271
Chakraborty M, Abrams SI, Camphausen K, Liu K, Scott T, Coleman CN, Hodge JW (2003) Irradiation of tumor cells up-regulates Fas and enhances CTL lytic activity and CTL adoptive immunotherapy. J Immunol 170:6338–6347
Slone HB, Peters LJ, Milas L (1979) Effect of host immune capability on radiocurability and subsequent transplantability of a murine fibrosarcoma. J Natl Cancer Inst 63:1229–1235
Lee Y, Auh SL, Wang Y, Burnette B, Wang Y, Meng Y et al (2009) Therapeutic effects of ablative radiation on local tumor require CD8 + T cells: changing strategies for cancer treatment. Blood 114:589–595
Burnette BC, Liang H, Lee Y, Chlewicki L, Khodarev NN, Weichselbaum RR et al (2011) The efficacy of radiotherapy relies upon induction of type I interferon–dependent innate and adaptive immunity. Cancer Res 71:2488–2496
Friedman EJ (2002) Immune modulation by ionizing radiation and its implications for cancer immunotherapy. Curr Pharm Des 8:1765–1780
Drake C (2011) Radiation induced immune modulation. In: DeWeese TL, Laiho M (eds) Molecular determinants of radiation response. Springer, New York, pp 251–263
Formenti SC, Demaria S (2013) Combining radiotherapy and cancer immunotherapy: a paradigm shift. J Natl Cancer Inst 105:256–265
Zeng J, See AP, Phallen J, Jackson CM, Belcaid Z, Ruzevick J et al (2013) Anti-PD-1 blockade and stereotactic radiation produce long-term survival in mice with intracranial gliomas. Int J Radiat Oncol* Biol* Phys 86:343–349
Demaria S, Pilones KA, Vanpouille-Box C, Golden EB, Formenti SC (2014) The optimal partnership of radiation and immunotherapy: from preclinical studies to clinical translation. Radiat Res 182:170–181
Belcaid Z, Phallen JA, Zeng J, See AP, Mathios D, Gottschalk C et al (2014) Focal radiation therapy combined with 4-1BB activation and CTLA-4 blockade yields long-term survival and a protective antigen-specific memory response in a murine glioma model. PLoS ONE 9:e101764
Kim JE, Patel MA, Mangraviti A, Kim ES, Theodros D, Velarde E et al (2017) Combination therapy with anti-PD-1, anti-TIM-3, and focal radiation results in regression of murine gliomas. Clin Cancer Res 23:124–136
Patel MA, Kim JE, Theodros D, Tam A, Velarde E, Kochel CM et al (2016) Agonist anti-GITR monoclonal antibody and stereotactic radiation induce immune-mediated survival advantage in murine intracranial glioma. J Immunother Cancer 4:28
Nelson MH, Bowers JS, Bailey SR, Diven MA, Fugle CW, Kaiser AD et al (2016) Toll-like receptor agonist therapy can profoundly augment the antitumor activity of adoptively transferred CD8 + T cells without host preconditioning. J Immunother Cancer 4:6
Wen P, Reardon D, Phuphanich S, Aiken R, Landolfi J, Curry W et al (2015) IMCT-20 association of survival and progression-free survival with immune response in HLA-A2 + newly-diagnosed GBM patients in randomized double-blind placebo-controlled phase 2 trial of dendritic cell (dc) immunotherapy with ICT-107. Neuro Oncol 17:v112
Schuster J, Lai RK, Recht LD, Reardon DA, Paleologos NA, Groves MD et al (2015) A phase II, multicenter trial of rindopepimut (CDX-110) in newly diagnosed glioblastoma: the ACT III study. Neuro Oncol 17:854–861
Reardon DA, Schuster JM, Tran DD, Fink KL, Nabors LB, Li G et al (2015) ReACT: overall survival from a randomized phase II study of rindopepimut (CDX-110) plus bevacizumab in relapsed glioblastoma. Neurosurgery 62:198–199
Ahmed N, Brawley V, Hegde M, Bielamowicz K, Wakefield A, Ghazi A et al (2015) Autologous HER2 CMV bispecific CAR T cells are safe and demonstrate clinical benefit for glioblastoma in a Phase I trial. J Immunother Cancer 3:O11
Nduom EK, Wei J, Yaghi NK, Huang N, Kong L-Y, Gabrusiewicz K et al (2016) PD-L1 expression and prognostic impact in glioblastoma. Neuro Oncol 18:195–205
Berghoff AS, Kiesel B, Widhalm G, Rajky O, Ricken G, Wöhrer A et al (2015) Programmed death ligand 1 expression and tumor-infiltrating lymphocytes in glioblastoma. Neuro Oncol 17:1064–1075
Reardon DA, Sampson JH, Sahebjam S, Lim M, Baehring JM, Vlahovic G et al (2016) Safety and activity of nivolumab (nivo) monotherapy and nivo in combination with ipilimumab (ipi) in recurrent glioblastoma (GBM): updated results from checkmate-143. J Clin Oncol 34
Demaria S, Kawashima N, Yang AM, Devitt ML, Babb JS, Allison JP, Formenti SC (2005) Immune-mediated inhibition of metastases after treatment with local radiation and CTLA-4 blockade in a mouse model of breast cancer. Clin Cancer Res 11:728–734
Deng L, Liang H, Burnette B, Beckett M, Darga T, Weichselbaum RR, Fu Y-X (2014) Irradiation and anti–PD-L1 treatment synergistically promote antitumor immunity in mice. J Clin Invest 124:687–695
Golden EB, Demaria S, Schiff PB, Chachoua A, Formenti SC. (2013) An abscopal response to radiation and ipilimumab in a patient with metastatic non–small cell lung cancer. Cancer Immunol Res 1:365–372
Papadopoulos, K, M Crittenden, ML Johnson, AC Lockhart, KN Moore, GS Falchook, S Formenti et al (2016) A first-in-human study of REGN2810, a monoclonal, fully human antibody to programmed death-1 (PD-1), in combination with immunomodulators including hypofractionated radiotherapy (hfrt). ASCO Meet Abstr 34:3024
Sahebjam S, Johnstone PA, Forsyth PA, Arrington J, Vrionis FD, Etame AB et al (2016) Safety and antitumor activity of hypofractionated stereotactic irradiation (HFSRT) with pembrolizumab (Pembro) and bevacizumab (Bev) in patients (pts) with recurrent high grade gliomas: Preliminary results from phase I study. ASCO Meet Abstr 34:2041
Grossman SA, Ye X, Lesser G, Sloan A, Carraway H, Desideri S, Piantadosi S (2011) Immunosuppression in patients with high-grade gliomas treated with radiation and temozolomide. Clin Cancer Res 17:5473–5480
Campian JL, Ye X, Gladstone DE, Ambady P, Nirschl TR, Borrello I et al (2015) Pre-radiation lymphocyte harvesting and post-radiation reinfusion in patients with newly diagnosed high grade gliomas. J Neurooncol 124:307–316
Huang J, DeWees TA, Badiyan SN, Speirs CK, Mullen DF, Fergus S et al (2015) Clinical and dosimetric predictors of acute severe lymphopenia during radiation therapy and concurrent temozolomide for high-grade glioma. Int J Radiat Oncol Biol Phys 92:1000–1007
Yovino S, Grossman SA (2012) Severity, etiology and possible consequences of treatment-related lymphopenia in patients with newly diagnosed high-grade gliomas. CNS Oncol 1:149–154
Razzaghdoust A, Mozdarani H, Mofid B, Aghamiri SMR, Heidari AH (2014) Reduction in radiation-induced lymphocytopenia by famotidine in patients undergoing radiotherapy for prostate cancer. Prostate 74:41–47
Sampson JH, Aldape KD, Archer GE, Coan A, Desjardins A, Friedman AH et al (2011) Greater chemotherapy-induced lymphopenia enhances tumor-specific immune responses that eliminate EGFRvIII-expressing tumor cells in patients with glioblastoma. Neuro Oncol 13:324–333
Wick W, Platten M, Meisner C, Felsberg J, Tabatabai G, Simon M et al (2012) Temozolomide chemotherapy alone versus radiotherapy alone for malignant astrocytoma in the elderly: the NOA-08 randomised, phase 3 trial. Lancet Oncol 13:707–715
Baumert BG, Hegi ME, van den Bent MJ, von Deimling A, Gorlia T, Hoang-Xuan K et al (2016) Temozolomide chemotherapy versus radiotherapy in high-risk low-grade glioma (EORTC 22033–26033): a randomised, open-label, phase 3 intergroup study. Lancet Oncol 17:1521–1532
Brandsma D, Stalpers L, Taal W, Sminia P, van den Bent MJ (2008) Clinical features, mechanisms, and management of pseudoprogression in malignant gliomas. Lancet Oncol 9:453–461
Shultz LD, Goodwin N, Ishikawa F, Hosur V, Lyons BL, Greiner DL (2014) Human cancer growth and therapy in immunodeficient mouse models. Cold Spring Harb Protoc 7:694–708
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Authors have no conflicts of interests to disclose related to this review article.
Rights and permissions
About this article

Cite this article
Sahebjam, S., Sharabi, A., Lim, M. et al. Immunotherapy and radiation in glioblastoma. J Neurooncol 134, 531–539 (2017). https://doi.org/10.1007/s11060-017-2413-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11060-017-2413-0