
Abstract
An 82-year-old woman presented to our hospital with a deep skin ulcer in her right lower limb. Although the skin biopsy showed necrosis and neutrophil infiltration, we could not initially detect any pathogen. Chest radiography showed multiple nodules despite the lack of respiratory symptoms or fever, and the serum latex agglutination test for cryptococcus showed an elevated titer (1:512). Considering these findings, we performed additional stains of periodic acid–Schiff reaction and Grocott to the skin-biopsy specimen and detected multiple yeast-like fungi. The cultures of the skin and lung-biopsy specimens revealed Cryptococcus neoformans. In this case, it is suggested that a large deep skin ulcer can be an initial manifestation of systemic cryptococcosis, as, in some cases, pulmonary cryptococcosis may be asymptomatic. Second, cutaneous cryptococcosis of an unexposed area such as the thigh can contribute to the diagnosis of systemic cryptococcal infection because it is attributable to bloodstream dissemination from other organs.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
An 82-year-old woman presented to our hospital with refractory skin ulcers in her right lower limb (Fig. 1), which had appeared approximately 3 months earlier and progressively worsened. She had been treated with glucocorticoids for 2 years under a diagnosis of remitting seronegative symmetrical synovitis with pitting edema syndrome.

Patient’s thigh with refractory skin ulcers
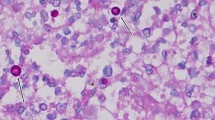
Although the skin biopsy showed necrosis and neutrophil infiltration, we could not initially detect any pathogen. Chest radiography (Fig. 2) showed multiple nodules despite the lack of respiratory symptoms or fever, and the serum latex agglutination test for cryptococcus showed an elevated titer (1:512). Considering these findings, we performed additional stains of periodic acid–Schiff reaction and Grocott to the skin-biopsy specimen and detected multiple yeast-like fungi (Fig. 3). The cultures of the skin- and lung-biopsy specimens revealed Cryptococcus neoformans.

Chest X-ray showing multiple nodules in the right lung

Stains of periodic acid–Schiff reaction (left) and Grocott (right) to the skin-biopsy specimen
After we confirmed that the blood culture was negative for growth and the cerebrospinal fluid examination was normal, we finally diagnosed the patient with systemic Cryptococcus infection of the skin and lung. Her condition improved with intravenous liposomal amphotericin-B and oral flucytosine treatment for 2 weeks followed by oral fluconazole (Fig. 4).

Patient’s skin ulcers improved after antifungal drug treatment
Two important observations can be made based on this case. First, a large deep skin ulcer can be an initial manifestation of systemic cryptococcosis, as, in some cases, pulmonary cryptococcosis may be asymptomatic. Second, cutaneous cryptococcosis of an unexposed area such as the thigh can contribute to the diagnosis of systemic cryptococcal infection because it is attributable to bloodstream dissemination from other organs (e.g., the lungs).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Araki, K., Yoshida, Y., Kohno, H. et al. A Large Deep Skin Ulcer as an Initial Manifestation of Systemic Cryptococcosis. Mycopathologia 184, 341–343 (2019). https://doi.org/10.1007/s11046-019-00322-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11046-019-00322-1