
Abstract
The oxidative modification of low-density lipoprotein (LDL) in the arterial wall plays a pivotal role in the initiation and progression of atherosclerosis which is a complex and progressive disorder. Paraoxonase1 (PON1), which is required for lipid metabolism, is believed to protect LDL from oxidation. The relationship between PON1 gene Leusin55Methionin (L55M) and Glutamine192Arginine (Q192R) polymorphisms in western Iranians with atherosclerosis and its association with enzyme activity and oxidized low-density lipoprotein (oxLDL) were examined in the present study. In this study, blood specimens were collected from 145 healthy individuals and 154 patients with atherosclerosis proven by angiography referred to Shahid Madani Hospital, Khorramabad, Iran. Genomic deoxy ribonucleic acid (DNA) was extracted from whole blood. For all the subjects, restriction fragment length polymorphism-polymerase chain reaction (RFLP-PCR) was carried out for the detection of L55M and Q192R polymorphisms. PON1 enzyme activity and the level of oxLDL were also evaluated. There was a 3.114-fold increase in the risk of developing atherosclerosis in the subjects presenting the PON1L55M, MM genotype compared to those with the LL genotype (OR 3.114; 95% CI 1.412–6.870). PON1Q192R polymorphism in the PON1 gene was not associated with atherosclerosis. Patients with atherosclerosis had significantly higher oxLDL and reduced PON1 enzyme activity (P < 0.05) compared to the controls. There was no association between the type of genotype, enzyme activity, and oxLDL level. It has been concluded that PON1L55M polymorphism and MM genotype are associated with an increased risk of coronary artery disease (CAD) in Iranian patients with atherosclerosis. We did not find any relationship between PON1Q192R polymorphism and atherosclerosis.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Epidemiological studies have indicated that CAD is one of the leading causes of death in developed and developing countries [1]. The global death rate shows that one out of every five patients (more than 20% of global deaths) die due to CAD [2, 3]. In Iran, as one of the third-world countries in which patients are at risk of exposure to hazardous factors, more than half of them die from CAD [4, 5].
The occurrence of atherosclerosis in the cardiovascular system is one of the leading causes of CAD [6, 7]. Among different risk factors, high-density lipoprotein (HDL-cholesterol) is known as one of the essential parameters [8] which increases the risk of developing cardiovascular disease by 2–3% per 1% reduction in HDL [9]. Likewise, the mechanisms underlying the protective effects of HDL have been reported in many studies [10, 11]. The known anti-atherogenic properties of HDL are due to its role as a lipid transporter in the reverse cholesterol transportation pathway. LDL oxidation plays an essential role in atherosclerosis, and HDL can protect it against oxidation by several mechanisms. HDL also reduces the biological activity of oxidızed LDL. These antioxidants and anti-atherogenic properties depend on various proteins associated with HDL such as PON1, platelet-activating factor (PAF) for acetyl hydrazine, and lecithin [12, 13]. PON1 (EC 3.1.8.1, aryldialkylphosphatase) was first identified due to its ability for the hydrolysis of organophosphates. It is a calcium-dependent ester with 355 amino acids and a molecular weight of 43 kDa [14]. It has been shown in many studies that PON1 has two common polymorphisms (L55M, and Q192R) both of which are single-nucleotide polymorphisms (SNPs) [15, 16].
It has been reported that L55M polymorphism could be caused by a change in the CTG codon resulting in the substitution of methionine by leucine (L/M55) at the position 55. L55M polymorphism is associated with stroke [17], coronary artery disease [16], and Parkinson's disease [18]. Although L55M polymorphism does not affect the binding of the enzyme to the substrate, it could change the enzyme level. Research has revealed that individuals with MM genotype have the lowest expression level of the mRNA and serum concentration of PON1 [15].
Q192R polymorphism is caused by a change in the CAA codon. Hence, arginine replaces glutamine at position 192 (Q/R192). Q192R polymorphism seems to alter the PON1 enzyme activity, depending on the substrate. Some substrates like paraoxon are hydrolyzed by R isoforms, while Q isoforms rapidly hydrolyze substrates such as diazoxone. Several recent studies have indicated that R alleles decrease the ability to protect LDL against oxidation compared to the Q allele [19].
The purpose of the present study is to investigate the effect of L55M and Q192R polymorphism on the risk of atherosclerosis and PON1 activity in Western Iran. Furthermore, we examined the potential impact of L55M and Q192R polymorphism and PON1 activity on the level of oxLDL.
Methods
Study design and population
A total of 299 study subjects (154 cases with atherosclerosis and 145 controls) were examined. All participants in this study referred to Cardiology and Angiography Department of Shahid Madani Hospital, Khorramabad, Iran, between December 2016 and May 2017. The disease was confirmed in all subjects by the standard diagnostic angiography.
For all subjects, a permission form containing various clinical information, including age, sex, weight, smoking, family history, hypertension, diabetes mellitus, drug abuse, and alcohol consumption was recorded. The inclusion criterion was the confirmation of coronary atherosclerosis by Gold Angiography. Subjects with congenital heart disease, malignancy, chronic kidney disease, pulmonary obstruction, and the use of steroid hormones as treatments were excluded. Individuals without coronary atherosclerosis were considered healthy controls. They were matched for sex and age. Written informed consent was obtained from all subjects. The study was reviewed and approved by the Lorestan University of Medical Science's Ethics Committee (code: LUMS.REC.1395.123). The study was administered following the Declaration of Helsinki and its following revisions [20].
Biochemical measurements
Two types of blood samples were collected, one without anticoagulants (for biochemical assays) and another with Ethylenediaminetetraacetic acid (EDTA) (for genetic polymorphism evaluations), each one in a volume of 5 ml. The lipid profile was assessed using Auto Analyzer (BT-1000, USA). The blood samples were stored at 4 °C and transferred to the laboratory. Subsequently, the WBC was isolated at the same time and was saved at minus 70 °C.
Small dense LDL (SdLDL) was measured using the method proposed by Hirano et al. As follows: lipoproteins (1.044 g/ml density) were precipitated via a reagent containing 40 U/ml heparin sodium salt and 30 mmol/l MgCl2 and then LDL-cholesterol was measured using LDL assay kits (Pishtaz Teb, Iran) [21]. OxLDL was measured using an ELISA kit (Mercodia, Sweden). Moreover, the measurement of PON1 enzyme activity was evaluated using the method developed by Paragh et al. In this method, the enzyme activity is measured using a paraoxon substrate. For this assay, 50 μl of serum was added to 1 cc of the ready-to-use solution, including Tris/HCl buffer (100 mmol/l pH 8), calcium chloride (2 mmol/l) and paraoxon (5 mmol/l). The speed of 4-nitrophenol production was measured at 412 nm and 25 °C using a spectrophotometer [22].
DNA extraction and PCR methodology
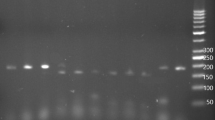
PON1 genotypes were determined by polymerase chain reaction (PCR) using a slightly altered version of the protocols proposed by Mackness et al. (Table 1). All PCR steps and the type of primer have been listed in Table 1. The PCR product of PON1Q192R polymorphisms was 99 bp, which was digested by 5U Alw l restriction enzyme (Thermo, Lithuania) in 5 h at 37 C. The products were separated by electrophoresis on a 3% agarose gel. The R allele contained a site for the Alw l restriction enzyme from which 66 and 33 bp products were made, but the Q allele did not [23]. (Fig. 1).

PON1Q192R polymorphisms genotypes
For the PON1L55M polymorphism, the PCR condition was the same as what was mentioned above except that 40 cycles were carried out. The PCR product (170 bp) was digested by Nla 111 (Thermo, Lithuania) and the digested products were separated via electrophoresis on a 2% agarose gel. The L allele did not contain the Nla 111 restriction site, but the M allele contained a restriction site that produced 126 bp and 44 bp [24]. (Fig. 2).

PON L55M polymorphisms genotypes
Statistical analysis
The normality of the data was tested using the Kolmogorov–Smirnov test. The data of the numerical variable have been presented as mean ± SD. Accordingly, a t-test was used to compare continuous data, and the Chi-square test was used to recognize the significance of the difference between the proportions. Moreover, the age and gender between the two groups of case and control were matched. Logistic regression analysis was used for testing the independent association of various variables. Data were analyzed using SPSS software version 16 (SPSS Inc., Chicago, IL, USA). P-values of less than 0.05 were regarded as statistically significant.
Results
Subjects characteristics
The baseline characteristics of the 299 subjects have been indicated in Table 2. Our results showed a considerable distinction in age (P < 0.001), weight (P = 0.045) and diagnosis age (P < 0.001) between the cases and control groups but there was no significant difference in height (P = 0.112), BMI (P = 0.390), systolic blood pressure (P = 0.140) and diastolic blood pressure (P = 0.147) between the two groups. The biochemical characteristics of the participants with reference ranges have been presented in Table 3. A significant distinction was observed in lipid profile, Sd-LDL (P < 0.001), Ox-LDL (P < 0.001), serum glucose (P < 0.001), and PON1 activity (P < 0.001) between the cases and control groups. We also found a significant distinction between the family history of CAD, hypertension, cigarette smoking, and diabetes mellitus in the two groups (Table 2).
Genotype distribution and genotype frequencies
In the present study, a total of 299 participants (145 controls, 154 cases) were included. The results of the genotype of the PON1 gene and its relationship with atherosclerosis have been indicated in Table3. In the study groups, there were 128 (42.8%), 135 (45.7%) and 36 (12%) subjects with the LL genotype, the LM genotype, and the MM genotype respectively. Moreover, LM genotype distribution in the cases group was 1.71 times higher than healthy individuals (P = 0.031; OR 1.71; CI 1.051–2.791), and MM genotype distribution in the cases group was 3.114 times higher than healthy individuals (P = 0.005; OR 3.114; CI 1.412–6.780).
Furthermore, there were 164 (54.8%), 108 (36.1%) and 27(9%) subjects with the QQ genotype, the QR genotype, and the RR genotype respectively. Distribution of QR genotype in the cases group was 0.952 times higher than the control group (P = 0.844; OR 0.952; CI 0.586–1.548), and RR genotype distribution in the cases group was 1.38 times higher than the healthy individuals (P = 0.44; OR 1.38; CI 0.606–3.166). Although we did not find any significant distinction between PON1Q192R polymorphism genotypes and alleles frequency in the cases and control groups, we found a significant relation between PON1L55M polymorphism genotypes and the alleles in the two groups (Table 3).
The controls with LL and LM genotype exhibited higher (P < 0.05) PON1 activity compared to the cases with LL and LM genotype respectively, but there was no significant difference between PON1 activity and MM genotype (P = 0.012) between the two groups. All subjects in the control group with PON1Q192R polymorphism showed higher PON1 activity compared to the cases group. However, this relationship was not significant between PON1 activity and RR genotype (P = 0.018) in comparison with the control group. The difference between the levels of enzyme activity in the different PON1Q192R polymorphism genotypes of the cases group is statistically significant. Nevertheless, it was not substantial in the control group. In this study, our results did not show any correlation between PON1L55M and PON1Q192R polymorphisms genotypes and enzyme activity in contrast with the control group. The results also indicated that the relationship between MM and LM genotypes interaction and PON1 activity in increasing the chances of developing atherosclerosis was significant.
In the present study, the serum levels of oxLDL in the cases and control groups were evaluated based on PON1L55M and PONQ192R polymorphism genotypes. In both polymorphisms, the mean serum level of oxLDL in the cases group was significantly different compared to the control group. However, there was no remarkable distinction between the ox-LDL level and PON1L55M and PONQ192R polymorphism genotypes in the two groups. The present research also revealed that the interactive effects of PON1L55M and PON1Q192R polymorphism among different genotypes of control and cases, and PON1 activity on oxLDL levels were statistically significant (Table 4).
Using the multivariable logistic regression, the effects of PON1L55M and PONQ192R polymorphism genotypes on age, sex, history of blood pressure, smoking, and CAD were simultaneously examined. The results have been presented in Table 5. The results indicate significant variables such as MM (P = 0.011), tobacco (P < 0.001), history of CAD (P < 0.001), and age (P < 0.001). The chance of developing atherosclerosis in subjects with MM genotype is higher than those with LL genotype, which is statistically significant (P = 0.011; OR 3.39; CI 1.8–32.73). The risk of developing the disease in females is 70% higher than males but it is not statistically significant (P = 0.092; OR 1.7; CI 0.91–3.16). In terms of age, the risk of developing the disease is enhanced by 0.8% per 1-year-old increase, which is statistically significant (P < 0.001; OR 1.08, CI 1.05–1.11). With regard to the history of cardiovascular disease, the risk of cardiovascular disease is 3.36 times greater than those without an account, which is statistically significant (P < 0.001; OR 3.36, CI 2–6.33) (Table 5).
Discussion
This research was planned to investigate the association between PON1L55M and PON1Q192R polymorphisms and the risk of developing atherosclerosis. In this Study, LM and MM genotypes of PON1L55M polymorphism had a meaningful relationship with the development of atherosclerosis, but we did not find any significant association between PON1Q192R polymorphism and atherosclerosis.
In our study population of Western Iran, the analysis of PON1L55M polymorphism showed that in the control group, 74 people had LL genotype, 60 people had LM genotype and 11 people had MM genotype. Moreover, in the cases group, 54 people with LL genotype, 75 people with LM genotype and 25 people with MM genotype were observed. Analysis of PON1Q192R polymorphism also showed 80 people with QQ genotype, 54 people with RQ genotype and 11 people with RR genotype in the control group and 84 people with QQ genotype, 54 people with RQ genotype and 16 people with RR genotype in the cases group. Hence, according to the analysis, people with LM and MM genotypes are more likely to get the disease while no significant results were found for PON1Q192R polymorphism.
Various studies, including this research, have found a meaningful relationship between the development of atherosclerosis and some determinants such as smoking [25, 26], obesity, and diabetes [27, 28]. Epidemiological studies have indicated that high levels of LDL cholesterol and triglyceride and low levels of HDL-cholesterol are among of the most influential risk factors for atherosclerosis [29, 30]. It was found out that PON1 is likely to prevent cardiovascular disease by inhibiting the oxidative damage of LDL through HDL [30, 31]. Due to the role of PON1 in the metabolism of lipids, various studies have shown evidence of a link between PON1Q192R and PON1 L55M polymorphism with CAD risk [17, 32, 33]. The activity of PON1 in the healthy subjects was higher than that of the cases, and it was statistically significant. However, no relationship was found between genotypes and enzyme activity.
Studies conducted by Özkök et al. and Kaman et al. indicated the association between PONQ192R and PONL55M polymorphism and the risk of developing cardiovascular disease. These studies revealed that individuals with MM genotype have lower enzyme activity and a higher risk of developing the disease [34, 35]. Moreover, a research carried out by Schmidt et al. on the Australian population showed a strong association between PONL55M polymorphism and atherosclerosis [36]. Odawara et al. indicated an association between PONQ192R polymorphism and cardiovascular disease in patients with diabetes mellitus. They also showed that individuals with RR genotype are exposed to a higher risk of developing atherosclerosis [37]. Furthermore, studies by Sanghera et al., Pati et al., and Agraval et al. confirm the association between PONQ192R polymorphism and the risk of cardiovascular disease in the Indian population. Both of these studies found that individuals with RR genotype and R allele have lower enzyme activity and a higher risk of the disease [16, 38, 39].
However, some studies have failed to find an association between the PON1 gene polymorphism and the increased risk of atherosclerosis. Several researches were conducted by Ferre et al. on the Spanish population but none of them found any correlation between PONQ192R and PONL55M polymorphisms and the incidence of the disease in individuals [40]. Furthermore, the studies carried out by Robertson and Lawlor studies did not show any relationship between PONQ192R and PONL55M polymorphisms and the risk of developing the illness in the British population [41, 42]. The studies conducted by Hong et al. on the community of Korea [43], Arca et al., on the Italian population [44], and Balcerzyk et al. on the Dutch population [45] also reported similar results observed in previous investigations. Distinct results from multiple studies could be due to the complex interactions between genotype-genotype, genotype-phenotype, and genotype-environment.
There are shreds of evidence that LDL peroxidation is one of the most critical risk factors for atherosclerosis. LDL oxidation seems to be the most crucial trigger for the development of atherosclerosis. Oxidative damage is a significant contributor to vascular wall damage and oxidative changes in LDL. Hence, it is an essential factor in the development of atherosclerosis [11, 39].
In the present study, the level of oxLDL was significantly higher in the cases group in contrast with the control group. Furthermore, we did not find a significant difference in the levels of oxLDL in PONQ192R and PONL55M polymorphism genotypes. Lakshmy et al. launched an investigation into oxLDL levels in cases with cardiovascular disease. The results showed that the oxLDL level was significantly higher in cases than in the control group, and the total antioxidant capacity in the cases was lower. In this research, the relationship between the PONL55M and PONQ192R polymorphism genotypes and the level of oxLDL was also investigated, but no significant correlation was found [46].
In addition to genetic testing, we investigated biochemical parameters. In this study, we measured factors such as blood sugar levels, lipid profiles, systolic and diastolic blood pressure, as well as sdLDL levels. As expected, the levels of these factors in the patient group were higher than the control, which was consistent with previous studies [47]. Moreover, other factors such as age, gender, weight, history of smoking, family history of the disease and blood pressure were also examined in this study. Our research also revealed that people with the MM genotype were more likely to develop the disease due to the simultaneous effects of these risk factors.
Limitations
The limitations that can be mentioned in this study include: At first, this study only collected samples from several western provinces in Iran. However, due to the genetic diversity and racial differences in different populations in Iran, this study could have broader examine the relationship between this SNP and various ethnic groups in Iran, which may have different outcomes in diverse communities. Moreover, this study did not investigate the effects of environmental pollution factors, which, given Iran's third world, is affected by numerous contaminating factors such as air pollution, which, by increasing the amount of oxidative stress, can affect the development of heart disease.
Conclusion
To sum up, it can be mentioned that LDL peroxidation is one of the most critical risk factors for atherosclerosis, and our results confirmed that. It has been concluded that LM and MM genotypes were associated with an increased risk of coronary artery disease in Iranian patients with atherosclerosis. We did not find any relationship between PON1Q192R polymorphism and atherosclerosis. There was no association between the type of genotypes, enzyme activity, and oxLDL level. On the other hand, to investigate the risk factors in the population, biochemical factors were examined, which showed a significant relationship.
Data availability
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- CAD:
-
Coronary artery disease
- HDL:
-
High-density lipoprotein
- LDL:
-
Low-density lipoprotein
- oxLDL:
-
Oxidized LDL
- PON1:
-
Serum paraoxonase1
- SNPs:
-
Single-nucleotide polymorphisms
- EDTA:
-
Ethylenediaminetetraacetic acid
- SdLDL:
-
Small dense LDL
- PAF:
-
Platelet-activating factor
- FBS:
-
Fasting blood glucose
- L55M:
-
Leusin55Methionin
- Q192R:
-
Glutamine192Arginine
- DNA:
-
Deoxy ribonucleic acid
- RFLP-PCR:
-
Restriction fragment length polymorphism-polymerase chain reaction
- PCR:
-
Polymerase chain reaction
References
Mack M, Gopal A (2016) Epidemiology, traditional and novel risk factors in coronary artery disease. Heart Fail Clin 12(1):1–10
Herrington W et al (2016) Epidemiology of atherosclerosis and the potential to reduce the global burden of atherothrombotic disease. Circ Res 118(4):535–546
Benjamin EJ et al (2018) Heart disease and stroke statistics-2018 update: a report from the American Heart Association. Circulation 137(12):e67–e492
Sanchis-Gomar F et al (2016) Epidemiology of coronary heart disease and acute coronary syndrome. Ann Transl Med 4(13):256–256
Najafipour H, Afshari M, Rostamzadeh F (2018) Prevalence of multiple coronary artery disease risk factors in Kerman: a population-based study in Southeast Iran. Iran J Med Sci 43(2):140–149
Mozaffarian D et al (2015) Heart disease and stroke statistics—2016 update: a report from the American Heart Association. Circulation. https://doi.org/10.1161/CIR.0000000000000350
Dai X et al (2016) Genetics of coronary artery disease and myocardial infarction. World J Cardiol 8(1):1–23
Castelli WP (1996) Lipids, risk factors and ischaemic heart disease. Atherosclerosis 124:S1–S9
Gordon DJ et al (1989) High-density lipoprotein cholesterol and cardiovascular disease. Four prospective American studies. Circulation 79(1):8–15
Shabana NA et al (2018) Genetic risk score (GRS) constructed from polymorphisms in the PON1, IL-6, ITGB3, and ALDH2 genes is associated with the risk of coronary artery disease in Pakistani subjects. Lipids Health Dis 17(1):224–224
Variji A et al (2019) The combined utility of myeloperoxidase (MPO) and paraoxonase 1 (PON1) as two important HDL-associated enzymes in coronary artery disease: Which has a stronger predictive role? Atherosclerosis 280:7–13
Navab M et al (2000) Normal high density lipoprotein inhibits three steps in the formation of mildly oxidized low density lipoprotein: steps 2 and 3. J Lipid Res 41(9):1495–1508
Nouryazdan N et al (2019) Study of angiotensin-converting enzyme insertion/deletion polymorphism, enzyme activity and oxidized low density lipoprotein in Western Iranians with atherosclerosis: a case-control study. BMC Cardiovasc Disord 19(1):184
Hassett C et al (1991) Characterization of cDNA clones encoding rabbit and human serum paraoxonase: the mature protein retains its signal sequence. Biochemistry 30(42):10141–10149
Leviev I, James RW (2000) Promoter polymorphisms of human paraoxonase PON1 gene and serum paraoxonase activities and concentrations. Arterioscler Thromb Vasc Biol 20(2):516–521
Pati N, Pati U (1998) Paraoxonase gene polymorphism and coronary artery disease in Indian subjects. Int J Cardiol 66(2):165–168
Shao P et al (2015) Association between PON1 L55M polymorphism and ischemic stroke: a systematic review and meta-analysis. Int J Clin Exp Med 8(3):3429–3437
Paul KC et al (2017) Organophosphate pesticides and PON1 L55M in Parkinson's disease progression. Environ Int 107:75–81
Abelló D et al (2014) Exploring the role of paraoxonases in the pathogenesis of coronary artery disease: a systematic review. Int J Mol Sci 15(11):20997–21010
Carlson RV, Boyd KM, Webb DJ (2004) The revision of the Declaration of Helsinki: past, present and future. Br J Clin Pharmacol 57(6):695–713
Hirano T et al (2003) A novel and simple method for quantification of small, dense LDL. J Lipid Res 44(11):2193–2201
Paragh G et al (1999) Serum paraoxonase activity changes in uremic and kidney-transplanted patients. Nephron 83(2):126–131
Mackness B et al (1998) Serum paraoxonase (PON1) 55 and 192 polymorphism and paraoxonase activity and concentration in non-insulin dependent diabetes mellitus. Atherosclerosis 139(2):341–349
Sayin Kocakap DB et al (2016) The association of paraoxonase 1 gene L55M polymorphism with the extent and severity of coronary artery disease in the Turkish population and its dependence on gender. Anatol J Cardiol 16(3):175–182
Merhi M et al (2015) Impact of inflammation, gene variants, and cigarette smoking on coronary artery disease risk. Inflamm Res 64(6):415–422
Iwanicka J et al (2017) Relationship between rs854560 PON1 gene polymorphism and tobacco smoking with coronary artery disease. Dis Markers 2017:1540949–1540949
Shen Y et al (2015) Association of elevated apoA-I glycation and reduced HDL-associated paraoxonase1, 3 activity, and their interaction with angiographic severity of coronary artery disease in patients with type 2 diabetes mellitus. Cardiovasc Diabetol 14(1):52
Elnoamany MF et al (2018) P613Paraoxonase 1 gene (Gln192-Arg) polymorphism and the risk of coronary artery disease in type 2 diabetes mellitus. Eur Heart J 39(suppl_1):ehy564.P613
Zheng L et al (2004) Apolipoprotein AI is a selective target for myeloperoxidase-catalyzed oxidation and functional impairment in subjects with cardiovascular disease. J Clin Invest 114(4):529–541
Chen H et al (2018) Association of rs662799 in APOA5 with CAD in Chinese Han population. BMC Cardiov Disord 18(1):2
Mackness MI, Arrol S, Durrington PN (1991) Paraoxonase prevents accumulation of lipoperoxides in low-density lipoprotein. FEBS Lett 286(1–2):152–154
Rainwater DL et al (2009) Determinants of variation in human serum paraoxonase activity. Heredity 102(2):147
Sayın KD et al (2016) The association of paraoxonase 1 gene L55M polymorphism with the extent and severity of coronary artery disease in the Turkish population and its dependence on gender. Anatol J Cardiol 16(3):175
Ozkok E et al (2008) Combined impact of matrix metalloproteinase-3 and paraoxonase 1 55/192 gene variants on coronary artery disease in Turkish patients. Med Sci Monit 14(10):CR536–CR542
Kaman D et al (2009) A preliminary study of human paraoxonase and PON 1 L/M55–PON 1 Q/R 192 polymorphisms in Turkish patients with coronary artery disease. Cell Biochem Funct 27(2):88–92
Schmidt H et al (1998) Paraoxonase PON1 polymorphism leu-Met54 is associated with carotid atherosclerosis: results of the Austrian Stroke Prevention Study. Stroke 29(10):2043–2048
Odawara M, Tachi Y, Yamashita K (1997) Paraoxonase polymorphism (Gln192-Arg) is associated with coronary heart disease in Japanese noninsulin-dependent diabetes mellitus. J Clin Endocrinol Metab 82(7):2257–2260
Sanghera DK et al (1997) Genetic polymorphism of paraoxonase and the risk of coronary heart disease. Arterioscler Thromb Vasc Biol 17(6):1067–1073
Agrawal S et al (2009) Paraoxonase 1 gene polymorphisms contribute to coronary artery disease risk among north Indians. Indian J Med Sci 63(8):335–344. https://doi.org/10.4103/0019-5359.55884
Ferré N et al (2002) Paraoxonase Gln-Arg (192) and Leu-Met (55) gene polymorphisms and enzyme activity in a population with a low rate of coronary heart disease. Clin Biochem 35(3):197–203
Robertson KS et al (2003) Human paraoxonase gene cluster polymorphisms as predictors of coronary heart disease risk in the prospective Northwick Park Heart Study II. Biochim Biophys Acta 1639(3):203–212
Lawlor DA et al (2004) The association of the PON1 Q192R polymorphism with coronary heart disease: findings from the British Women's Heart and Health cohort study and a meta-analysis. BMC Genet 5(1):17
Hong SH et al (2001) Genetic variations of the paraoxonase gene in patients with coronary artery disease. Clin Biochem 34(6):475–481
Arca M et al (2002) PON1 L55M polymorphism is not a predictor of coronary atherosclerosis either alone or in combination with Q192R polymorphism in an Italian population. Eur J Clin Invest 32(1):9–15
Balcerzyk A, Zak I, Krauze J (2007) Synergistic effects between Q192R polymorphism of paraoxonase 1 gene and some conventional risk factors in premature coronary artery disease. Med Res Arch 38(5):545–550
Lakshmy R et al (2010) Paraoxonase gene Q192R & L55M polymorphisms in Indians with acute myocardial infarction & association with oxidized low density lipoprotein. Indian J Med Res 131(4):522
Renuka M et al (2018) Association between paraoxonase 1(PON1) gene polymorphisms and PON1 enzyme activity in Indian patients with coronary artery disease (CAD). Curr Pharmacogenomics Person Med 16(3):219–229
Acknowledgements
The authors would like to thank all those involved in the study and with their support, we were encouraged to do this project. We also gratefully acknowledge all the staff at Shahid Madani Hospital and all the people participating in this study.
Funding
The funders had no role in study design, data collection, and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
All authors contributed extensively to the study presented in this paper. Dr. GS was responsible for the design and management of the project and also the final edition of the paper. NN played a practical role in collect samples, performed the experiments and wrote the paper. Dr. MB analyzed the data. GA contributed to the writing and editing of the article.
Corresponding author
Ethics declarations
Conflict of interests
All authors declare that they have no competing interests.
Ethical approval
This study was approved by the Ethics Committee at Shahid Madani Hospital, Khorramabad, Iran and Lorestan University of Medical Science. All participants in this study received a permission form.
Informed consent
All participants in this study referred to Cardiology and Angiography Department of Shahid Madani Hospital, Khorramabad, Iran, between 2016 December and 2017 May. Written informed consent was obtained from all subjects. The study was reviewed and approved by the Lorestan University of Medical Science's Ethics Committee (code: LUMS.REC.1395.123). The study was administered following the Declaration of Helsinki and its following revisions. Consent for publication was obtained from each subject.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Shahsavari, G., Nouryazdan, N., Adibhesami, G. et al. Genetic associations and serum paraoxonase levels with atherosclerosis in western Iranian patients. Mol Biol Rep 47, 5137–5144 (2020). https://doi.org/10.1007/s11033-020-05585-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11033-020-05585-2