
Abstract
Anti-silencing function 1B (ASF1B) has been reported to be associated with the occurrence of many kinds of tumors. However, the biological effect and action mechanism of ASF1B in pancreatic cancer (PC) tumorigenesis remain unclear. The expression and prognosis value of ASF1B in PC were analyzed using GEPIA, GEO, and Kaplan–Meier plotter databases. The diagnostic value of ASF1B in PC was determined by receiver operating characteristic curve. The relationship between ASF1B expression and the clinical feathers in PC was investigated based on TCGA. qRT-PCR and western blot analyses were used to measure ASF1B expression in PC cells. Cell proliferation was evaluated by MTT and EdU assays, and apoptosis was examined by TUNEL and caspase-3 activity assays. Western blot analysis was utilized to detect the expression of proliferating cell nuclear antigen (PCNA), cyclin D1, Bax, Bcl-2, and phosphatidylinositol 3-kinase (PI3K)/protein kinase B (Akt) signaling proteins. ASF1B was overexpressed in several digestive cancers, including PC. Upregulated ASF1B was correlated with the poor prognosis and clinical features in PC patients. The area under the curve (AUC) value of ASF1B was 0.990. ASF1B was also overexpressed in PC cells. ASF1B silencing inhibited PC cell proliferation, promoted apoptosis, and increased caspase-3 activity, which were accompanied by the reduction of PCNA and cyclin D1 expression and increase of the ratio of Bax/Bcl-2 expression. Additionally, ASF1B silencing suppressed the PI3K/Akt pathway and 740Y-P treatment partially abolished the effects of ASF1B knockdown on PC cells. In conclusion, ASF1B silencing retarded proliferation and promoted apoptosis in PC cells by inactivation of the PI3K/Akt pathway.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
As the most common and aggressive malignancy of the digestive system, pancreatic cancer (PC) is the seventh leading cause of cancer-related deaths worldwide, and the data of cancer statistics showed that there were approximately 48,220 deaths and 60,430 newly diagnosed PC cases in 2021 in the USA [1, 2]. PC is featured by early systemic metastasis and extensive local tumor invasion, leading to a high mortality rate [3]. Generally, the mortality rate is almost similar to the morbidity rate in PC [4]. More importantly, most PC patients are usually diagnosed at the advanced stage due to the inconspicuous typical symptoms in the early stage and the lack of early diagnosis biomarkers [5]. Although the significant improvements in the diagnosis and therapeutic methods of PC have been achieved, PC still lacks effective diagnosis, metastasis, and prognosis biomarkers resulting in the poor prognosis with the five-year survival rate of approximately 5% [6]. Accumulating evidence indicated that the unfavorable clinical outcomes of PC mainly resulted from the high recurrence rate, distant metastasis, resistance to chemotherapy, and ineffective curative treatments [7, 8]. Therefore, it is urgent to explore the pathophysiological mechanism of PC and identify new target genes related to PC pathogenesis for searching the effective treatments of PC.
Histone chaperones mediate nucleosome assembly or disassembly in several DNA-dependent processes and regulate chromatin functions through the assistance of histone modification [9,10,11]. Anti-silencing function 1 (ASF1) is a highly conserved histone H3-H4 chaperone linked to the modulation of cell cycle, DNA damage repair, as well as transcription regulation [12]. Multiple studies have suggested that ASF1 contributed to cancer progression [13]. ASF1 comprises two isoforms ASF1A and ASF1B, which share ∼70% sequence identity, while they are not functionally equivalent. Specifically, ASF1A is primarily beneficial to DNA repair and cell senescence, while ASF1B, which is required for DNA replication and nucleosome formation, preferentially participates in modulating cell proliferation [12, 14]. ASF1B was considered to serve as a potential biomarker of proliferation status for tumor diagnosis and prognosis [15]. It has been well documented that high expression of ASF1B was closely associated with disease development of many kinds of tumors, such as breast cancer and cervical cancer [15, 16]. However, the biological effect and action mechanism of ASF1B in PC tumorigenesis are still undefined.
Herein, we aimed to figure out the specific role of ASF1B in PC. We systematically determined ASF1B expression in PC and its correlation with prognosis and diagnosis based on Gene Expression Profiling Interactive Analysis (GEPIA), Gene Expression Omnibus (GEO), and The Cancer Genome Atlas (TCGA) databases as well as Kaplan–Meier plotter and receiver operating characteristic (ROC) curve analyses. Then, the effect and the underlying mechanism of ASF1B in proliferation and apoptosis of PC cells were investigated.
Materials and methods
GEPIA database
GEPIA (http://gepia.cancer-pku.cn) database is a commonly used interactive website that provides 9736 tumor samples and 8587 normal samples from TCGA data portal (https://cancergenome.nih.gov/) and the Genotype-Tissue Expression (GTEx) projects [17]. Expression pattern of ASF1B between the tumor and normal tissues in 31 different types of human cancers were acquired from GEPIA database. The differential expression of ASF1B in pancreatic adenocarcinoma (PAAD) and normal tissue samples were analyzed using GEPIA database.
Differential expression analysis
Two human PC mRNA expression datasets (GSE16515 and GSE28735) were downloaded from the GEO database (http://www.ncbi.nlm.nih.gov/geo/) [18]. GSE16515 dataset contains 36 PC tissue samples and 16 normal pancreatic tissue samples. GSE28735 includes 45 PC tissue samples and the paired adjacent normal pancreatic tissue samples.
Kaplan–Meier plotter database analysis
We used GEPIA browser to verify the correlation between ASF1B expression and survival, including overall survival (OS) and the disease-free survival (DFS). Kaplan–Meier plotter online database (http://kmplot.com/analysis/) was used to perform the survival analysis.
TCGA analysis
ASF1B mRNA expression (from RNA-seq data) and the clinical information data of PC patients were downloaded from TCGA-PAAD cohort.
Cell culture
Human PC cell lines (BxPc-3, AsPc-1, PANC-1, and SW1990) were obtained from the Cell Repository, Chinese Academy of Sciences (Shanghai, China) and human pancreatic duct epithelial cell line (H6C7) was acquired from KeraFAST, Inc. (Boston, MA, USA). All cells were maintained in Dulbecco’s Modified Eagle Medium (DMEM) (Thermo Fisher Scientific, Waltham, MA, USA) with the addition of 10% fetal bovine serum (FBS) (Kang Yuan Biology, Tianjin, China), 100 U/mL penicillin, and 100 μg/mL streptomycin (Invitrogen, Shanghai, China). These cells were incubated at 37 °C in a water-jacketed incubator with 5% CO2.
Cell transfection
Two small interfering RNAs (siRNAs) against ASF1B (si-ASF1B#1 and si-ASF1B#2) and the scrambled negative control siRNA (si-con) were synthesized by GeneChem Co, Ltd. (Shanghai, China). Lipofectamine 2000 reagent (Invitrogen) was applied to perform transient transfection of the oligonucleotide sequences according to the manufacturer’s instruction. 3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide (MTT) assay.
The MTT kit (Solarbio, Beijing, China) was employed to measure cell proliferative ability. Briefly, SW1990 and PANC-1 cells (5 × 103 cells per well) were seeded into the 96-well plates and transfected with si-ASF1B#1, si-ASF1B#2, or si-con prior to treatment with or without 25 μg/mL 740Y-P (MedChemExpress, Monmouth Junction, NJ, USA), a phosphatidylinositol 3-kinase (PI3K) agonist. Following treatments for 0, 24, 48, and 72 h, the cells were mixed with 20 µL 0.5 mg/ml MTT solution and cultured for another 4 h. Afterward, 150 µL dimethyl sulfoxide (DMSO) (Sigma, St. Louis, MO, USA) was added. The optical density (OD) value was measured at 570 nm using an EnSpire Multimode Plate Reader (PerkinElmer, Waltham, Massachusetts, USA).
5-Ethynyl-2′-deoxyuridine (EdU) cell proliferation assay
Cell proliferation ability was also estimated by the Cell-Light™ EdU imaging detecting kit (Ribobio, Guangzhou, China). After treatments for 48 h, SW1990 and PANC-1 cells were grown into the 24-well plates and incubated with 50 μM EdU reagent for 2 h. Then, the cells were fixed with 4% paraformaldehyde and permeabilized with 0.5% Triton-X 100 for 10 min. After 1 × Apollo® reaction cocktail staining for 30 min, cell nuclei were counterstained with 4’,6-diamidino-2-phenylindole dihydrochloride (DAPI) for 5 min at room temperature. EdU-positive cells were counted in three randomly selected visual fields using a fluorescence microscopy (Nikon, Tokyo, Japan).
Terminal deoxynucleotidyl transferase dUTP nick-end labeling (TUNEL) assay
TUNEL staining was applied to measure the apoptotic DNA fragmentation with the One-step TUNEL apoptosis detection kit (Beyotime, Shanghai, China). Treated SW1990 and PANC-1 cells were plated on sterile coverslips in the 6-well plates and processed consecutively with 4% paraformaldehyde in PBS for 20 min at room temperature. Thereafter, 0.1% Triton-X 100 on ice was added to permeate cells for 2 min. Afterward, the cells were incubated with 50-μL-precooled TUNEL reaction mixture for 1 h prior to nuclear staining with DAPI in the darkness at 37 °C. Cell apoptosis was evaluated by counting the number of TUNEL-positive cells using a fluorescence microscopy (Nikon).
Western blot analysis
Total protein was extracted from the treated SW1990 and PANC-1 cells using the ice-cold RIPA buffer (ComWin, Changzhou, China) and the protein concentration was measured using the bicinchoninic acid (BCA) protein assay (Pierce, Rockford, IL, USA). After separation by 10% SDS-PAGE, the extracted protein samples were transferred onto the polyvinylidene fluoride membranes and incubated with 5% non-fat milk to prevent non-specific binding. Subsequently, the membranes were co-cultured at 4 °C overnight with the primary antibodies: ASF1B (Cell Signaling Technology, Danvers, MA, USA), proliferating cell nuclear antigen (PCNA) (Cell Signaling Technology), cyclin D1 (Cell Signaling Technology), Bax (Cell Signaling Technology), Bcl-2 (Cell Signaling Technology), phospho-PI3K (p-PI3K) (Abcam Technology, Cambridge, MA, USA), PI3K (Abcam Technology), phospho-protein kinase B (p-Akt) (Cell Signaling Technology), Akt (Cell Signaling Technology), and β-actin (Cell Signaling Technology), followed by incubation with the horseradish peroxidase-linked secondary antibody (Cell Signaling Technology) at room temperature for 1 h. Finally, the protein signals were monitored via a chemiluminescence detection system (Bio-Rad lab, Hercules, CA, USA).
Caspase-3 activity assay
Following the indicated treatments, SW1990 and PANC-1 cells were subjected to the measurement of caspase-3 activity using a caspase-3 colorimetric assay kit (MBL, Nagoya, Japan) according to the manufacturer’s protocol.
Statistical analysis
All results are shown as the mean ± standard deviation (SD) from three independent experiments. All statistical analyses were processed by application of GraphPad Prism 7.0 software. Student’s t test and one-way analysis of variance (ANOVA) were used to compare the statistical difference and determine statistical significance. P value < 0.05 was considered as statistically significant.
Results
ASF1B expression was elevated in PC
We analyzed the differential expression of ASF1B in 31 different types of cancers by extracting expression data from GEPIA database, and the data suggested that ASF1B was overexpressed in several digestive cancers, such as colon adenocarcinoma (COAD), esophageal cancer (ESCA), and PAAD (Fig. 1A). The upregulation of ASF1B in PAAD tissues in comparison to that in normal samples analyzed by GEPIA database is shown in Fig. 1B. Consistent with the above results, the data from GSE16515 and GSE28735 datasets indicated that ASF1B expression was increased in PC tissues compared with the normal tissues (Fig. 1C, D).

Expression pattern of ASF1B in PC. A ASF1B expression in pan tumors and the corresponding normal tissues based on GEPIA database. ASF1B expression in PAAD and normal tissue samples was analyzed based on GEPIA (B), GSE16515 (C), and GSE28735 (D) datasets. *P < 0.05, **P < 0.01, ***P < 0.001
Upregulation of ASF1B expression was associated with the clinicopathological factors in PC patients
To evaluate the prognostic value of ASF1B expression in PC, OS and DFS analysis on the basis of ASF1B expression were performed. We found that high ASF1B expression in PC patients was correlated with the worse OS (Fig. 2A) and DFS (Fig. 2B) compared with low ASF1B expression group. To determine the diagnostic value of ASF1B, ROC curve analysis was carried out to calculate the area under the curve (AUC) value of ASF1B. The results showed that the AUC value was 0.990 between the tumor and normal tissues, suggesting a reasonable diagnosis ability of ASF1B (Fig. 2C). To identify the clinical significance of ASF1B in PC, the association between ASF1B expression and clinicopathological parameters was investigated. ASF1B expression was positively correlated with age (Fig. 2D), T stage (Fig. 2E), history of chronic pancreatitis (Fig. 2F), and histologic grade (Fig. 2G). There were no significant differences in ASF1B expression among gender (Fig. 2H) and smoker (Fig. 2I). These data concluded that ASF1B upregulation was correlated with the poor clinical outcome of PC patients.

ASF1B upregulation was correlated with the poor clinical outcome of PC patients. Upregulated ASF1B was associated with the worse OS (A) and DFS (B) in PC. C ROC curve for PC patients based on the expression of ASF1B. Expression of ASF1B in PC patients according to age (D), T stage (F), history of chronic pancreatitis (G), histologic grade (H), gender (E), and smoker (I). *P < 0.05, **P < 0.01
ASF1B expression was increased in PC cells
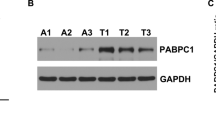
Next, the mRNA and protein levels of ASF1B were determined in PC cell lines. As shown in Fig. 3A–C, ASF1B mRNA and protein levels were significantly upregulated in PC cell lines (BxPc-3, AsPc-1, PANC-1, and SW1990) in comparison to that in human pancreatic duct epithelial cell line (H6C7), particularly in SW1990 and PANC-1 cells. Thus, SW1990 and PANC-1 cells were chosen for the subsequent experiments. To explore the function of ASF1B in PC, ASF1B expression was knocked down in PC cells by transfection with si-ASF1B#1 or si-ASF1B#2. The significant inhibition of ASF1B protein expression was observed in PC cells by transfection of si-ASF1B#1 or si-ASF1B#2 (Fig. 3D, E).

ASF1B expression in PC cells. qRT-PCR (A) and western blot (B and C) analyses of ASF1B mRNA and protein expression in PC cells (BxPc-3, AsPc-1, PANC-1, and SW1990) and human pancreatic duct epithelial cell line (H6C7). D and E Western blot analysis of ASF1B protein level in SW1990 and PANC-1 cells transfected with si-ASF1B#1, si-ASF1B#2, or si-con. *P < 0.05, **P < 0.01, ***P < 0.001
ASF1B silencing inhibited PC cell proliferation
Next, the impact of ASF1B silencing on proliferation of PC cells was evaluated. Using MTT assay, cell proliferation was impeded in PC cells with si-ASF1B#1 or si-ASF1B#2 transfection (Fig. 4A, B). Similar results were observed in the EdU assay (Fig. 4C, D). Consistently, the expression of proliferation-related biomarkers PCNA and cyclin D1 was repressed by ASF1B knockdown in PC cells (Fig. 4E–G). These results collectively demonstrated that cell proliferation was retarded by ASF1B interference in PC cells.

Influence of ASF1B silencing on cell proliferation in PC cells. SW1990 and PANC-1 cells were transfected with si-ASF1B#1, si-ASF1B#2, or si-con, followed by the detection of cell proliferation by MTT (A and B) and EdU cell proliferation (C and D) assays. Scale bar: 100 μm. (E–G) The protein levels of PCNA and cyclin D1 in si-ASF1B#1, si-ASF1B#2, or si-con-transfected SW1990 and PANC-1 cells were determined by western blot analysis. **P < 0.01, ***P < 0.001
ASF1B silencing accelerated apoptosis of PC cells
The effect of ASF1B knockdown on apoptosis of PC cells was further evaluated by TUNEL assay. There was an elevation in the fraction of apoptotic PC cells after si-ASF1B#1 or si-ASF1B#2 transfection compared with si-con group (Fig. 5A–C). Similarly, si-ASF1B#1 or si-ASF1B#2-transfected PC cells exhibited an increased caspase-3 activity relative to si-con-transfected cells (Fig. 5D). Concurrently, the ratio of Bax/Bcl-2 protein expression in PC cells was increased by ASF1B knockdown (Fig. 5E, F). These data suggested that ASF1B knockdown induced apoptosis of PC cells.

Impact of ASF1B knockdown on apoptosis of PC cells. SW1990 and PANC-1 cells were transfected with si-ASF1B#1, si-ASF1B#2, or si-con, followed by the determination of cell apoptosis (A–C), caspase-3 activity (D), and Bax/Bcl-2 protein expression (E and F) by TUNEL, caspase-3 activity assay, and western blot analysis, respectively. Scale bar: 100 μm. **P < 0.01
ASF1B knockdown inhibited the PI3K/Akt pathway in PC cells
Activation of the PI3K/Akt pathway is proposed to be associated with the occurrence and development of tumors, including PC [19, 20]. Therefore, the association between ASF1B knockdown and the PI3K/Akt pathway is worthy of exploration. As depicted in Fig. 6A–D, ASF1B expression was reduced by transfection with si-ASF1B#1, but it was not affected by treatment with 740Y-P, a PI3K agonist. The protein level of p-PI3K/PI3K and p-Akt/Akt was significantly inhibited after ASF1B knockdown in SW1990 and PANC-1 cells. However, treatment with 740Y-P significantly overturned the inhibition of p-PI3K/PI3K and p-Akt/Akt expression induced by ASF1B depletion (Fig. 6A–D). These results demonstrated that the PI3K/Akt pathway was inactivated by ASF1B silencing in PC cells.

Influence of ASF1B silencing on the PI3K/Akt pathway in PC cells. A–D SW1990 and PANC-1 cells were transfected with si-ASF1B#1, si-ASF1B#2, or si-con, followed by treatment with or without 25 μg/mL 740Y-P for 48 h. Then, the protein levels of ASF1B, p-PI3K, PI3K, Akt, and p-Akt were detected by western blot analysis. ns, not significant. **P < 0.01, ***P < 0.001
Activation of the PI3K/Akt pathway reversed the effect of ASF1B silencing on PC cells
Furthermore, we aimed to explore whether ASF1B knockdown affected PC progression via the PI3K/Akt pathway. Using MTT and EdU cell proliferation assays, the inhibition of cell proliferation due to depletion of ASF1B in SW1990 and PANC-1 cells was partially alleviated after the addition of 740Y-P (Fig. 7A–D). Moreover, 740Y-P treatment significantly antagonized ASF1B silencing-induced apoptosis in SW1990 and PANC-1 cells (Fig. 7E, F). These findings proved that ASF1B silencing impeded cell proliferation and promoted cell apoptosis in PC cells via inactivating the PI3K/Akt pathway.

Inactivation of the PI3K/Akt pathway participated in the effects of ASF1B on PC cells. SW1990 and PANC-1 cells were transfected with si-ASF1B#1, si-ASF1B#2, or si-con, or combined with 25 μg/mL 740Y-P and incubated for 24, 48, and 72 h. Cell proliferation was evaluated by MTT (A and B) and EdU (C and D) assays. Scale bar: 100 μm. (E and F) Cell apoptosis was evaluated using TUNEL assay. Scale bar: 100 μm. ***P < 0.001
Discussion
PC is one of the most aggressive human cancers, and the annual mortality rate of PC is nearly equal to the incidence rate [21]. Owing to its aggressiveness, PC remains a serious health issue. The early diagnosis rate of PC patients is low due to the insidious symptoms, resulting in that the patients were mostly diagnosed as the advanced stage with poor prognosis. Thus, a number of researchers aimed to explore genes and signaling pathways involved in PC carcinogenesis, with the hope of developing the possible effective therapeutic targets for PC [22, 23]. In the present study, we demonstrated the upregulation of ASF1B in PC tissues and cells, which was correlated with the poor prognosis in PC patients. Our data evidenced that ASF1B functioned as an oncogenic gene in PC progression via regulating the PI3K/Akt pathway.
It has been demonstrated that deregulation of histone chaperone proteins including ASF1 regulates chromatin function and contributes to the pathogenesis of cancers [9, 13, 24]. ASF1B, one subtype of ASF1, has been reported to be associated with cancer progression [15, 16]. However, little literature has illustrated the biological role of ASF1B in PC. In our study, ASF1B expression data were obtained from the public databases, including GEPIA and GEO databases, and we found that ASF1B was highly expressed in PC tissues. Additionally, ASF1B was also upregulated in PC cells. This finding was in line with the overexpression of ASF1B in prostate, breast, and cervical cancers [15, 25, 26]. According to Kaplan–Meier plotter database, ASF1B overexpression was negatively correlated with both OS and DFS in PC patients. Our results also suggested that upregulated ASF1B might serve as a diagnostic biomarker for PC by ROC curve analysis. Furthermore, the correlation between ASF1B expression and clinicopathological features in PC patients was determined according to TCGA database. The results showed that ASF1B overexpression was positively related to age, T stage, and history of chronic pancreatitis in PC patients. Consistently, it was reported that upregulation of ASF1B was associated with the worse OS, progression-free survival, advanced tumor stage, and tumor development in lung adenocarcinoma [27]. These above results suggested that ASF1B might be closely related to PC pathogenesis. Moreover, ASF1B silencing restrained cell proliferation and triggered cell apoptosis in PC cells, which was partially mediated by inactivation of the PI3K/Akt pathway, suggesting the oncogenic role of ASF1B in PC progression. Similar studies were observed in several tumors. For example, a previous study demonstrated the aberrantly high expression of ASF1B in cervical cancer, which was crucial for maintaining cervical cancer cell tumorigenic activity in vitro and promoting tumor growth in vivo [26]. In clear cell renal cell carcinoma, ASF1B was highly expressed and accelerated cell proliferation and migration through activating the Akt/p70 ribosomal S6 kinase 1 (S6K1) pathway [28].
The PI3K/Akt pathway is one of the classic evolutionarily conserved signaling pathways, which plays a critical role in regulating cell growth, survival, motility, anti-apoptotic signal transduction, and tumorigenesis [29]. Activation of the PI3K/Akt pathway accelerated cell proliferation, inhibited cell apoptosis, and led to an aggressive phenotype of cancer [30, 31]. Meanwhile, activation of the PI3K/Akt pathway was also related to the poor clinical prognosis [32]. In particular, the overactivation of the PI3K/Akt pathway is a common event in the development and progression of PC, suggesting the crucial role of the PI3K/Akt pathway in PC carcinogenesis [19]. Interestingly, our study showed that ASF1B knockdown suppressed the activation of the PI3K/Akt pathway in PC cells. Activation of the PI3K/Akt pathway by 740Y-P partially abolished the effects of ASF1B knockdown on PC cells. These findings indicated that ASF1B knockdown inhibited the activation of the PI3K/Akt pathway, thereby inhibiting cell proliferation and inducing cell apoptosis in PC cells. Consistent with our results, it was previously reported that ASF1B knockdown inhibited the progression of prostate cancer via inactivation of the PI3K/Akt pathway [25].
In summary, the current study showed that ASF1B was upregulated in PC and correlated with the poor prognosis in PC patients. Moreover, ASF1B silencing repressed proliferation and promoted apoptosis in PC cells by inactivation of the PI3K/Akt pathway, which contributed to better understanding the pathogenesis of PC. Our study suggested that targeting the ASF1B/PI3K/Akt axis might be an achievable avenue for the treatment of PC.
Data availability
The experimental data will be available on the request.
Code availability
Not applicable.
References
Park W, Chawla A, O’Reilly EM (2021) Pancreatic cancer: a review. JAMA 326(9):851–862
Siegel RL, Miller KD,Fuchs HE, Jemal A (2021) Cancer statistics. CA Cancer J Clin 71(1):7–33
Paulson AS, Tran Cao HS, Tempero MA, Lowy AM (2013) Therapeutic advances in pancreatic cancer. Gastroenterology 144(6):1316–1326
Wang ZM, Lu J, Zhang LY, Lin XZ, Chen KM, Chen ZJ et al (2015) Biological effects of low-dose-rate irradiation of pancreatic carcinoma cells in vitro using 125I seeds. World J Gastroenterol 21(8):2336–2342
Mohammed S, Van Buren G 2nd, Fisher WE (2014) Pancreatic cancer: advances in treatment. World J Gastroenterol 20(28):9354–9360
Falasca M (1865) Kim M and Casari I (2016) Pancreatic cancer: current research and future directions. Biochim Biophys Acta 2:123–132
Klompmaker S, de Rooij T, Korteweg JJ, van Dieren S, van Lienden KP, van Gulik TM et al (2016) Systematic review of outcomes after distal pancreatectomy with coeliac axis resection for locally advanced pancreatic cancer. Br J Surg 103(8):941–949
Lovecek M, Skalicky P, Chudacek J, Szkorupa M, Svebisova H, Lemstrova R et al (2017) Different clinical presentations of metachronous pulmonary metastases after resection of pancreatic ductal adenocarcinoma: Retrospective study and review of the literature. World J Gastroenterol 23(35):6420–6428
Gurard-Levin ZA, Quivy JP and Almouzni G (2014) Histone chaperones: assisting histone traffic and nucleosome dynamics. Annu Rev Biochem 83:487–517
Adkins MW, Howar SR, Tyler JK (2004) Chromatin disassembly mediated by the histone chaperone Asf1 is essential for transcriptional activation of the yeast PHO5 and PHO8 genes. Mol Cell 14(5):657–666
Munakata T, Adachi N, Yokoyama N, Kuzuhara T, Horikoshi M (2000) A human homologue of yeast anti-silencing factor has histone chaperone activity. Genes Cells 5(3):221–233
Messiaen S, Guiard J, Aigueperse C, Fliniaux I, Tourpin S, Barroca V et al (2016) Loss of the histone chaperone ASF1B reduces female reproductive capacity in mice. Reproduction 151(5):477–489
Seol JH, Song TY, Oh SE, Jo C, Choi A, Kim B et al (2015) Identification of small molecules that inhibit the histone chaperone Asf1 and its chromatin function. BMB Rep 48(12):685–690
Paul PK, Rabaglia ME, Wang CY, Stapleton DS, Leng N, Kendziorski C et al (2016) Histone chaperone ASF1B promotes human β-cell proliferation via recruitment of histone H3.3. Cell Cycle 15(23):3191–3202
Corpet A, De Koning L, Toedling J, Savignoni A, Berger F, Lemaître C et al (2011) Asf1b, the necessary Asf1 isoform for proliferation, is predictive of outcome in breast cancer. EMBO J 30(3):480–493
Rosty C, Sheffer M, Tsafrir D, Stransky N, Tsafrir I, Peter M et al (2005) Identification of a proliferation gene cluster associated with HPV E6/E7 expression level and viral DNA load in invasive cervical carcinoma. Oncogene 24(47):7094–7104
Tang Z, Li C, Kang B, Gao G, Li C, Zhang Z (2017) GEPIA: a web server for cancer and normal gene expression profiling and interactive analyses. Nucleic Acids Res 45(W1):W98-w102
Edgar R, Domrachev M, Lash AE (2002) Gene expression omnibus: NCBI gene expression and hybridization array data repository. Nucleic Acids Res 30(1):207–210
Asano T, Yao Y, Zhu J, Li D, Abbruzzese JL, Reddy SA (2004) The PI 3-kinase/Akt signaling pathway is activated due to aberrant Pten expression and targets transcription factors NF-kappaB and c-Myc in pancreatic cancer cells. Oncogene 23(53):8571–8580
Ng SSW, Tsao MS, Chow S, Hedley DW (2000) Inhibition of phosphatidylinositide 3-kinase enhances gemcitabine-induced apoptosis in human pancreatic cancer cells. Cancer Res 60(19):5451–5455
Bosetti C, Bertuccio P, Negri E, La Vecchia C, Zeegers MP, Boffetta P (2012) Pancreatic cancer: overview of descriptive epidemiology. Mol Carcinog 51(1):3–13
Ouaïssi M, Silvy F, Loncle C, Ferraz da Silva D, Martins Abreu C, Martinez E et al (2014) Further characterization of HDAC and SIRT gene expression patterns in pancreatic cancer and their relation to disease outcome. PLoS ONE 9(9):e108520
Hruban RH, Goggins M, Parsons J, Kern SE (2000) Progression model for pancreatic cancer. Clin Cancer Res 6(8):2969–2972
Avvakumov N, Nourani A, Côté J (2011) Histone chaperones: modulators of chromatin marks. Mol Cell 41(5):502–514
Han G, Zhang X, Liu P, Yu Q, Li Z, Yu Q et al (2018) Knockdown of anti-silencing function 1B histone chaperone induces cell apoptosis via repressing PI3K/Akt pathway in prostate cancer. Int J Oncol 53(5):2056–2066
Liu X, Song J, Zhang Y, Wang H, Sun H, Feng X et al (2020) ASF1B promotes cervical cancer progression through stabilization of CDK9. Cell Death Dis 11(8):705
Feng Z, Zhang J, Zheng Y, Wang Q, Min X, Tian T (2021) Elevated expression of ASF1B correlates with poor prognosis in human lung adenocarcinoma. Personal Med 18(2):115–127
Jiangqiao Z, Tao Q, Zhongbao C, Xiaoxiong M, Long Z, Jilin Z et al (2019) Anti-silencing function 1B histone chaperone promotes cell proliferation and migration via activation of the AKT pathway in clear cell renal cell carcinoma. Biochem Biophys Res Commun 511(1):165–172
Osaki M, Oshimura M, Ito H (2004) PI3K-Akt pathway: its functions and alterations in human cancer. Apoptosis 9(6):667–676
Liu S, Wang XJ, Liu Y, Cui YF (2013) PI3K/AKT/mTOR signaling is involved in (-)-epigallocatechin-3-gallate-induced apoptosis of human pancreatic carcinoma cells. Am J Chin Med 41(3):629–642
Fumarola C, Bonelli MA, Petronini PG, Alfieri RR (2014) Targeting PI3K/AKT/mTOR pathway in non small cell lung cancer. Biochem Pharmacol 90(3):197–207
Ocana A, Vera-Badillo F, Al-Mubarak M, Templeton AJ, Corrales-Sanchez V, Diez-Gonzalez L et al (2014) Activation of the PI3K/mTOR/AKT pathway and survival in solid tumors: systematic review and meta-analysis. PLoS ONE 9(4):e95219
Funding
None.
Author information
Authors and Affiliations
Contributions
KW, ZH, and XF conducted the experiments. XF, WL, and AJ supervised the data collection and analyzed the data. ZH and XH designed the study and prepared the manuscript. All authors have read and approved the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflict of interest.
Consent to participate
Not applicable.
Consent for publication
All authors have approved for the publication of this manuscript.
Ethical approval
Not applicable.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Wang, K., Hao, Z., Fu, X. et al. Involvement of elevated ASF1B in the poor prognosis and tumorigenesis in pancreatic cancer. Mol Cell Biochem 477, 1947–1957 (2022). https://doi.org/10.1007/s11010-022-04404-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11010-022-04404-5