
Abstract
Perfectionism is a vulnerability factor for a wide array of psychopathology. Despite much evidence suggesting dysregulated stress response as an intermediary process that links perfectionism to psychopathology, the lack of a cross-lagged examination deterred researchers from making causal interpretations. This study examined the directionality of effects among perfectionism dimensions, stress reactivity, and depression. A total of 189 participants at time 1 and 94 at time 2 completed an online survey that consisted of measures of perfectionism, stress reactivity, and depression, one month apart. Cross-lagged analysis results showed that personal standards perfectionism predicted later prolonged stress reactivity but not depression at time 2. Self-critical perfectionism predicted later depression but not prolonged stress reactivity at time 2. Rather, prolonged stress reactivity at time 1 predicted self-critical perfectionism at time 2. Findings suggest that perfectionism dimensions are distinct in creating a dysregulated stress process. Future studies could incorporate other stress-related variables (e.g., coping) to further explicate the stress-generation process, in conjunction with stress reactivity.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Perfectionism is a multidimensional personality characteristic that has been of interest to many researchers with varying operationalizations, in part stemming from the rich discussions on appropriate measures to assess the construct (Stoeber, 2018a). The most recent consensus through evidence from a series of factors analyses of multiple perfectionism measures supports that perfectionism is best represented by two higher-order factors of personal standards perfectionism (also commonly referred to as perfectionistic strivings) and self-critical perfectionism (also commonly referred to as perfectionistic concerns) (Stoeber, 2018b). More specifically, personal standards perfectionism or perfectionistic strivings entail self-oriented perfectionism, which reflects setting high expectations and relentlessly striving to meet those expectations (Frost et al., 1993; Stoeber & Otto, 2006). Self-critical perfectionism or perfectionistic concerns entail socially prescribed perfectionism, concerns over mistakes, and having doubts about one’s actions, all of which reflect feeling inadequate, discrepant, and insufficient in meeting high self-set expectations (Stoeber & Otto, 2006; Rice et al., 2014).
Both perfectionism dimensions (or factors) are linked to numerous psychopathology conditions (see Limburg et al., 2017 for a review). More consistently and robustly found are how self-critical perfectionism functions as a vulnerability factor to instigating and maintaining psychopathology (for reviews, see Smith et al., 2016; Smith et al., 2021). In other words, perfectionism causes individuals to be at risk for certain psychological conditions such as depression and anxiety. On the other hand, personal standards perfectionism showed mixed results with some studies reporting its protective function against psychological maladjustment, particularly found in athletes (Garinger et al., 2018; Madigan et al., 2016) and others reporting it being a vulnerability factor to psychopathology (Békés et al., 2015). Recent meta-analytic evidence increasingly supports that personal standards perfectionism may also be a risk factor for psychopathology (Smith et al., 2018).
Of the many indicators of psychopathology, the most frequently examined psychopathology in the perfectionism stress process is depression (Limburg et al., 2017). Distinguishable associative patterns for perfectionism dimensions with depression were also evidenced, detailing the underlying process through which perfectionism affects depression. For example, for self-critical perfectionism, hassles (Dunkley & Blankstein, 2000), stressful life events (Shahar et al., 2004), and daily stress coping and stress appraisal (Mandel et al., 2015) mediated the relationship with depression. For personal standards perfectionism, hassles did not mediate the relationship with depression (Dunkley et al., 2000). In sum, results suggest that personal standards perfectionism and self-critical perfectionism appear to be distinctively associated with stress processes and psychopathology outcomes.
Most of these empirical findings complement theoretical propositions that argue a vulnerability model of perfectionism (Hewitt & Flett, 1993). The vulnerability model outlines that a personality characteristic of perfectionism predisposes people to think, feel, and behave in ways that cause depression (Bagby et al., 2008; Klein et al., 2011). Less examined in exploring the associations between perfectionism and stress process or depression is the complication model or the scar model of personality. These models posit that a personality characteristic such as perfectionism is either a temporary or a permanent outcome of psychopathology such as depression. A few studies have examined the complication/scar model of perfectionism and found reciprocal relations between perfectionism and depression (McGrath et al., 2012), and perfectionism predicting depression only, supporting against the complication/scar model (Sherry et al., 2014). In sum, there is stronger evidence for the vulnerability model of perfectionism in predicting depression.
Unfortunately, the lack of studies employing multiple time-point designs limited drawing conclusive interpretations on whether perfectionism indeed creates certain stress processes that may result in depression. Cross-sectional design limits our understanding of the direction of effects whereas designs such as cross-lagged analysis allow us to identify the directionality of effects (e.g., one variable influencing another variable, reciprocal causation). Particularly, we could not locate any previous cross-lagged design empirical studies that tested whether perfectionism precipitates individuals to be more reactive to stress (stress reactivity) or vice versa. Furthermore, depression, which is one of the most common psychopathologies that both perfectionism and stress reactivity have been linked to (Felsten, 2004; Hewitt et al., 1996), also has not been examined using cross-lagged analysis. The current study addressed the limitations of previous studies by examining the stress process of perfectionism (Hewitt & Flett, 2002) using a two-wave short-term cross-lagged model.
Perfectionism and the Stress Process
Individuals experience stress when they appraise demands as unmanageable (Lazarus, 1966). Individuals with high perfectionistic tendencies are always striving to meet the highest expectations meticulously without mistakes. Particularly, those who set high expectations while harboring a sense of inadequacy (despite mostly good performances) are especially prone to appraise demands as overwhelming and unmanageable. Thus, perfectionism has been theorized as a precursor to subsequent stress processes and experiences. Empirically, the association between perfectionism and stress has been widely documented (D’souza et al., 2011; Rice et al., 2006) with links between perfectionism and different types of stress (Molnar et al., 2020; Rice et al., 2012). Divergent associative patterns with stress and specific perfectionism dimensions were also reported. For instance, personal standards perfectionism negatively predicted stress but self-critical perfectionism positively predicted stress (Achtziger & Bayer, 2013). Although much research examined the associations between perfectionism and stress, possible intermediary processes that may exist in the associations between perfectionism and stress have been relatively less examined.
To explain how perfectionism is involved in the stress process, Hewitt & Flett (2002) outlined several stress process framework models detailing ways in which perfectionism and stress are interrelated, focusing on the role perfectionism has in initiating stress responses and exacerbating stress experiences. For example, some studies examined the stress process of perfectionism by exploring how perfectionism predicts certain stress coping styles (Luo et al., 2016; Vanstone & Hicks, 2019). Other studies examined how individuals respond to stress by referring to it as “emotional reactivity to stress” (Dunkley et al., 2003) among individuals with high perfectionistic tendencies. These findings attempted to elucidate that perfectionism is a risk factor for subsequent psychopathology through a lack of adaptive stress coping and heightened emotional reactivity to stress.
However, these studies had limitations. Studies that examined stress coping to be part of the stress process of perfectionism did not account for how one responds to stress before examining how individuals cope with it. In studies that examined emotional reactivity, emotional reactivity was operationalized as an increase or a decrease in positive and negative affect. Thus, much of this body of research is limited by not directly assessing stress reactivity before exploring how perfectionistic individuals cope with or appraise stress. Another limitation was that there was no comprehensive and formal operationalization of what stress reactivity is. Yet, from the theoretical proposition made by Hewitt & Flett (2002), it was argued that stress reactivity should be examined as a mediator in the link between perfectionism and depressive symptoms. That is, a mechanism by which perfectionism predicts depressive outcomes may be because perfectionistic tendency cognitively biases individuals to respond more negatively to neutral or mildly stressful cues as greatly stressful.
To our knowledge, two studies directly assessed how individuals react to stress (Flett et al., 2016; Mandel et al., 2015) and how such reactivity was linked to depression. However, these two studies were cross-sectional. Thus, there is a need to assess the stress process of perfectionism explicitly and directly, by including stress reactivity as the proximal indicator and by incorporating a cross-lagged analysis.
Stress Reactivity of Perfectionism
Stress reactivity is defined as “an individual’s perceived typical response intensity aggregated across different potentially stressful situations in everyday life” (p. 81, Schlotz et al., 2011). This indicates that there are individual differences in stress reactivity, with some individuals being more reactive to stress than others. Particularly, those with self-critical perfectionism tendencies are likely to biasedly interpret ambiguous situations to warrant perfection (Yiend et al., 2011). They also struggle to withdraw attention from emotionally negative stimuli (Tonta et al., 2019) and often ruminate (O’Connor et al., 2007). Such reactivity to stimuli leaves certain individuals with perfectionistic tendencies in a chronically highly stressed state. Attending to such a characteristic way of reacting to stressors, Flett et al., (2016) referred to the perfectionism-borne stress reactivity as “perfectionistic reactivity.” They argued that individuals with perfectionistic tendencies have characteristic ways of responding to stressors that are ultimately harmful to their well-being.
A few studies directly assessed the chronically heightened stress reactivity of individuals with high perfectionistic tendencies (Flett et al., 2016; Mandel et al., 2015; Richardson et al., 2014). Particularly, Flett et al., (2016) found that stress reactivity (composed of prolonged stress reactivity and social evaluation reactivity) mediated the association between socially prescribed perfectionism and depression. As the authors noted, this suggested that the perception of others constantly evaluating is how those with high perfectionism levels driven by the need to meet others’ expectations end up experiencing depression. The study by Flett et al., (2016) was an important undertaking for explicitly incorporating stress reactivity, but not without limitations. One of the biggest limitations was that cross-sectional data was used to test a mediation model, a practice that can lead to making erroneous causal inferences (Cole & Maxwell, 2003). Another limitation was that the proposed mediation model was only tested with socially prescribed perfectionism. This precluded comparing any similarities or differences in whether and how personal standards perfectionism and self-critical perfectionism predicts stress reactivity. The current study attempts to address these limitations.
Present Study
The present study examined the directional effects among perfectionism, stress reactivity, and depression using a two-wave cross-lagged analysis. The main effects of interest were on the predictive effects of time 1 perfectionism dimensions on time 2 variables of stress reactivity and depression. Based on the perfectionism vulnerability model, we hypothesized that self-critical perfectionism at time 1 will positively predict prolonged stress reactivity and depression at time 2. We also hypothesized that personal standards perfectionism at time 1 will predict depression at time 2, but left the nature of prediction (positive or negative) open given the mixed empirical results. With regards to prolonged stress reactivity, it was hypothesized that it will positively predict depression (Kiecolt-Glaser et al., 2020).
Method
Participants
A total of 189 adults participated in this study. The mean age of participants was 35.36 years old (SD = 16.94). Approximately 71% were women, 28% were men, and less than 1% declined to answer. In terms of race, 77% of participants identified as White, 8% Hispanic, 6% African American, 4% Asian American, 3% multiracial, and 2% as “Other.”
Measures
Perfectionism. The Almost Perfect Scale-Revised (APS-R; Slaney et al., 2001) was used to assess two dimensions of perfectionism. Personal standards perfectionism was assessed by the standards dimension composed of seven items assessing setting high performance expectations for oneself (e.g., “I have a high standard for my performance at work or at school”). Self-critical perfectionism was assessed by the discrepancy dimension composed of 12 items assessing perceived inadequacy in meeting high set expectations (e.g., “My best just never seems to be good enough for me”). Participants responded on a 7-point scale (1 = strongly disagree, 7 = strongly agree) and higher scores indicated a greater perfectionistic tendency in each dimension. Internal consistency has been consistently high across studies (Grzegorek et al., 2004), and convergent validity was supported (Abdollahi et al., 2018).
Prolonged Stress Reactivity. The prolonged reactivity subscale of the Perceived Stress Reactivity Scale (PSRS; Schlotz et al., 2011) was used to assess prolonged stress reactivity. The prolonged reactivity subscale assessed continued activation from stressful situations, distinguished from other subscales in the PSRS that are situation-specific stress reactivity. Four items reflected prolonged stress reactivity. Sample item included, “When tasks and duties accumulate to the extent that they are hard to cope with…” and participants chose one of three options that most accurately described their experiences (My sleep is unaffected, My sleep is slightly disturbed, or My sleep is very disturbed). Each item was rated on a 3-point scale. Higher scores indicated greater prolonged stress reactivity. Convergent validity and internal reliability were supported (Schlotz et al., 2011).
Depressive Symptoms. The depression subscale from the Depression Anxiety Stress Scales-21 (DASS-21; Lovibond & Lovibond, 1995) was used to assess the experience of depression over the past week. The depression subscale consisted of 7 items (e.g., “I couldn’t seem to experience any positive feeling at all”). Items were rated on a 4-point scale (0 = did not apply to me at all, 3 = applied to me very much or most of the time). Higher scores indicated greater depression symptoms. Convergent validity was supported in a nonclinical sample of U. S. adults (Sinclair et al., 2012). Strong internal consistency was reported (Osman et al., 2012).
Procedure
This study was approved by two Institutional Review Boards (a southwestern public university, and a northeastern public university in the U.S.) to maximize data collection. The study was advertised as an online research survey on personality and health. Participants were recruited from campus-wide research study advertisements (courses, social media, student club emails) and through an online research recruitment platform (Research Match). Research Match is a free and secure registry with over 150,000 volunteers, and more than 500 publications have been generated to date using samples of this platform (https://www.researchmatch.org/about/). Participants were compensated either their course research credit or stood a chance to win one of ten $10 Amazon gift cards.
Analytic Strategy
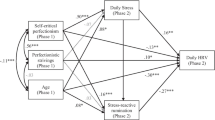
To investigate temporal predictions among perfectionism dimensions, prolonged stress reactivity, and depressive symptoms, a two-wave cross-lagged panel analysis (Kline, 2016; Selig & Little 2012) was performed using the Mplus 7.4 software (Muthén & Muthén, 1998–2015). Data comprised repeated measures of personal standards perfectionism, self-critical perfectionism, prolonged stress reactivity, and depression. Cross-lagged models of the panel data explicitly controls for the autoregression, so-called stability, among variables. In other words, after controlling for the variance attributable to the effect of the preceding variable at time 1, the remaining variance in the change at time 2 is caused by other variables. Thus, the path coefficients that show the cross-lagged relationships between variables are of substantive concern for interpretation. The correlations of pairs of four variables at the same time were also estimated and a saturated model was assumed. All the measures were standardized prior to statistical testing. The maximum likelihood procedure was applied to estimate all parameters. The full information maximum likelihood for missing data was adopted. The tested model is visualized in Fig. 1.
Results
Data Considerations and Descriptive Statistics
Before conducting statistical analyses, a series of statistical tests were performed to address missing values. There was a noticeable drop-out at time 2 (initial sample was n = 189, time 2 sample was n = 94). First, chi-square analyses and t-tests were conducted to examine whether subjects’ demographics (gender, race, and age) and the four measures at time 1 were different between participants who responded at both time points and those who did not respond to the second survey. The results showed that participant retention was not a function of gender, \({\chi }^{2}\) = 2.65, p = .266, race (Hispanic vs. non-Hispanic), \({\chi }^{2}\) = 0.94, p = .625, nor age t = -1.88, p = .062. Moreover, the t-test results also indicated that the four measures at time 1 from two universities were not significantly different; personal standards perfectionism, t = -0.96, p = .338, self-critical perfectionism, t = -1.35, p = .179, prolonged stress reactivity, t = 0.02, p = .984, and depression, t = 1.58, p = .116. Additionally, we conducted Little’s missing completely at random (MCAR) test, and the result was not significant, χ2 (2) = 4.93, p = .085, suggesting that the drop-out at time 2 could be considered random. The values of skewness ( < ± 2.00) and kurtosis ( < ± 3.00) indicated a symmetrical distribution of each measure (Kline, 2015). Descriptive statistics, correlational analyses, and internal consistency for all measures at times 1 and 2 were computed and appear in Table 1. The correlation among tested variables ranged from − 0.01 to 0.79.
Main Analysis
Personal standards perfectionism at time 1 significantly predicted prolonged stress reactivity at time 2 (β = 0.17, p = .046). This indicated that the higher personal standards perfectionism at time 1, the higher prolonged stress reactivity at time 2. However, self-critical perfectionism at time 1 did not significantly predict prolonged stress reactivity at time 2 (β = 0.02, p = .823). On the other hand, prolonged stress reactivity at time 1 was positively predictive of self-critical perfectionism at time 2 (β = 0.19, p = .003), but it did not predict personal standards perfectionism at time 2 (β = 0.06, p = .373). The cross-lagged path and the autoregressive coefficients are presented in Table 2.

Tested Model
Self-critical perfectionism at time 1 significantly positively predicted depression at time 2 (β = 0.20, p = .006). For the rest of paths, the results indicated that there were nonsignificant relationships. Personal standards perfectionism at time 1 did not predict depression at time 2 (β = 0.08, p = .217). Meanwhile, depression at time 1 was not associated with neither later self-critical perfectionism (β = 0.07, p = .468) nor personal standards perfectionism (β = -0.05, p = .701).
Discussion
This study attempted to explicitly assess the role of stress reactivity and compare whether both dimensions of perfectionism similarly function in the subsequent stress process. As such, a central goal of this study was to examine whether the prolonged stress reactivity, a tendency that is theorized to be prominent in individuals with high perfectionism, was created by perfectionism dimensions. Results found that personal standards perfectionism was implicated in later prolonged stress reactivity, but prolonged stress reactivity did not predict later depression. Self-critical perfectionism on the other hand directly conferred risk to later depression without influencing prolonged reactivity. However, earlier prolonged stress reactivity functioned to reinforce later self-critical perfectionistic tendencies.
First, supporting our hypothesis, personal standards perfectionism positively predicted later prolonged stress reactivity. This indicates that because of constant and relentless striving and perceived continuous demands to meet, one cannot relax and rest and have a dysregulated stress response. The internal mental condition of striving for the best creates a default mode of relentless functioning, marked by prolonged stress reactivity. When there is always something to achieve, it is difficult to wind down. This prolonged activation ultimately will wear and tear existing internal resources, manifested through a dysregulated stress modulation. The cognitive stress theory (Lazarus, 1966) asserts that physiological and psychological responses are products of demands that are appraised to be unmanageable or potentially harmful. Individuals high in personal standards perfectionism are overwhelmed with self-set demands, which preclude them from rest, relaxation, and self-care.
The lack of effect from personal standards perfectionism to later depression was against our hypothesis but this result may explain why there are mixed findings on the associative patterns between personal standards perfectionism and depression. Some studies report that personal standards perfectionism is negatively associated with depression (Abdollahi et al., 2018; Levine & Milyavskaya, 2018) whereas others report that they are positively associated (Smith et al., 2016). Our results suggest that personal standards perfectionism itself is not a risk or protective factor of depression. Personal standards perfectionism is often accompanied by adaptive coping strategies, such as problem-focused coping (Prud’homme et al., 2017), which may deter the effects of personal standards perfectionism and dysregulated stress modulation (prolonged stress reactivity) on distal outcomes such as depression.
For self-critical perfectionism, supporting our hypothesis, the presence of an effect on later depression is in line with previous research that argued self-critical perfectionism and depression link (Dunkley et al., 2020; Moroz & Dunkley, 2019). This suggests that self-critical perfectionism itself is a risk factor to depression and can be conceptualized as the maladaptive or unhealthy perfectionism. With a lack of internal resources and appropriate coping strategies, individuals with high self-critical perfectionism are likely to experience depression. Interestingly, against our hypothesis, self-critical perfectionism did not predict prolonged stress reactivity. This finding does not align well with previous studies that identified stress-related processes as an intermediary variable. For instance, in examining the association between perfectionism and depression, Smith et al., (2020) found that social disconnection and stress are intermediary variables that were involved. In another study that examined the role of self-critical perfectionism on depression, Nealis et al., (2020) found support for a dysregulated physiological stress process. Specifically, those with high self-critical perfectionism showed increased waking cortisol in both high and low stress conditions, lending support for physiological stress reactivity. We speculate that our divergent finding against previous findings may be due to how stress reactivity was conceptualized and assessed. Smith et al., (2020) examined stress as opposed to stress reactivity to describe a stress process, and Nealis et al., (2020) assessed a physiological measure of stress reactivity. Perhaps those with self-critical perfectionism tendencies may already be accustomed to being reactive to stress, and thus prolonged stress reactivity may be under-reported when in self-report formats as opposed to objective physiological assessments.
Lastly, prolonged stress reactivity predicted later self-critical perfectionism. One speculative explanation might be that being chronically stress reactive, individuals learn to become perfectionistic, in an attempt to reduce the distress that gets activated when encountering stressors. In other words, individuals learn to become hypervigilant to their shortcomings and inadequacies, because they are always reactive to stress. Learning to self-monitor extensively and excessively thus may be a way of self-protection against potential greater stress for being chronically stress reactive.
As this study concretized the stress process of perfectionism dimensions by identifying directional effects with prolonged stress reactivity, these results could blend well into the existing stress coping literature. Given that individuals with perfectionistic tendencies are less equipped to handle stress, especially when the stressor involves evidencing performance, adaptively coping with stress can be a protective factor against psychological distress. Indeed, Dunkley et al., (2016) tested several models cross-sectionally and longitudinally examining how adopting effective coping strategies can attenuate the perfectionism and distress link. However, to adopt effective coping strategies to stress, exploring any individual differences in how one responds to stressors should precede. Given that perfectionism debilitates one’s stress management capacity through chronic over-activation (Richardson et al., 2014), not only does perfectionism influence physiological reactivity when faced with stressors, but also, perfectionism creates prolonged stress reactivity in the case of personal standards perfectionism. This study bridged this gap in the literature by examining whether stress reactivity mediated the association between perfectionism dimensions and depression.
Limitations and Future Directions
This study has several limitations that should be noted to discuss avenues for future research. First, results are drawn from non-clinical healthy volunteers pre-Covid-19, and no screening was conducted on depression levels. Those with clinical diagnoses may have even elevated levels of stress reactivity and overall depression levels may have changed in the population since the outbreak of Covid-19. Thus, replication of the cross-lagged models with more recent or clinical samples would be fruitful in future studies. Further, while a curvilinear relationship was not found between perfectionism and depression among a clinical sample of depressed psychiatric adolescents (Hewitt et al., 2014), others report curvilinear relationships between perfectionism and certain health outcomes in clinical samples (e.g., Molnar et al., 2012). Examining the role of stress reactivity in linear or curvilinear relations between perfectionism and depression with non-clinical and clinical samples may be interesting. Second, incorporating experimental designs to induce stress and monitor physiological stress reactivity may provide a more comprehensive understanding of the stress reactivity generated by perfectionism. What would be important is to diversify the induction of stress, without only relying on the trier social stress test (TSST; Kirschbaum et al., 1993). The nature of this stress (social) may be different from stress invocation that is more performance- and goal-oriented. Thus, induced stress processes and the nature and magnitude of stress reactivity may not be generalizable. Lastly, assessing constructs such as perfectionism with more than one measure may be a more accurate and holistic reflection of the nature of perfectionism factors in future studies.
Conclusion
To our knowledge, this is the first study that examined and identified the directional effects between perfectionism, prolonged stress reactivity, and depression using a cross-lagged design. Taken together, our results suggest that personal standards perfectionism initiated a stress process but did not distally affect psychopathology outcomes per se. On the other hand, self-critical perfectionism directly influenced depression, suggesting that self-critical perfectionism itself is a risk for depression. This study sets the stage for future studies on perfectionism to consider stress reactivity as an intermediary variable that affects psychological outcomes.
Data Availability
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
References
Abdollahi, A., Hosseinian, S., & Asmundson, G. J. (2018). Coping styles mediate perfectionism associations with depression among undergraduate students. The Journal of General Psychology, 145(1), 93–105.
Achtziger, A., & Bayer, U. C. (2013). Self-control mediates the link between perfectionism and stress. Motivation and Emotion, 37(3), 413–423.
Bagby, R. M., Quilty, L. C., & Ryder, A. C. (2008). Personality and depression. The Canadian Journal of Psychiatry, 53(1), 14–25.
Békés, V., Dunkley, D. M., Taylor, G., Zuroff, D. C., Lewkowski, M., Foley, J. E., & Westreich, R. (2015). Chronic stress and attenuated improvement in depression over 1 year: The moderating role of perfectionism. Behavior Therapy, 46(4), 478–492.
Cole, D. A., & Maxwell, S. E. (2003). Testing mediational models with longitudinal data: Questions and tips in the use of structural equation modeling. Journal of Abnormal Psychology, 112(4), 558–577.
D’souza, F., Egan, S. J., & Rees, C. S. (2011). The relationship between perfectionism, stress and burnout in clinical psychologists. Behaviour Change, 28(1), 17–28.
Dunkley, D. M., & Blankstein, K. R. (2000). Self-critical perfectionism, coping, hassles, and current distress: A structural equation modeling approach. Cognitive Therapy and Research, 24(6), 713–730.
Dunkley, D. M., Blankstein, K. R., Halsall, J., Williams, M., & Winkworth, G. (2000). The relation between perfectionism and distress: Hassles, coping, and perceived social support as mediators and moderators. Journal of Counseling Psychology, 47(4), 437–453.
Dunkley, D. M., Solomon-Krakus, S., & Moroz, M. (2016). Personal standards and self-critical perfectionism and distress: Stress, coping, and perceived social support as mediators and moderators. In F. M. Sirois, & D. S. Molnar (Eds.), Perfectionism, health, and well-being (pp. 157–176). Cham: Springer.
Dunkley, D. M., Starrs, C. J., Gouveia, L., & Moroz, M. (2020). Self-critical perfectionism and lower daily perceived control predict depressive and anxious symptoms over four years. Journal of Counseling Psychology, 67(6), 736–746.
Dunkley, D. M., Zuroff, D. C., & Blankstein, K. R. (2003). Self-critical perfectionism and daily affect: Dispositional and situational influences on stress and coping. Journal of Personality and Social Psychology, 84(1), 234–252.
Felsten, G. (2004). Stress reactivity and vulnerability to depressed mood in college students. Personality and Individual Differences, 36(4), 789–800.
Flett, G. L., Nepon, T., Hewitt, P. L., & Fitzgerald, K. (2016). Perfectionism, components of stress reactivity, and depressive symptoms. Journal of Psychopathology and Behavioral Assessment, 38(4), 645–654.
Frost, R. O., Heimberg, R. G., Holt, C. S., Mattia, J. I., & Neubauer, A. L. (1993). A comparison of two measures of perfectionism. Personality and Individual Differences, 14(1), 119–126.
Grzegorek, J. L., Slaney, R. B., Franze, S., & Rice, K. G. (2004). Self-criticism, dependency, self-esteem, and grade point average satisfaction among clusters of perfectionists and nonperfectionists. Journal of Counseling Psychology, 51(2), 192–200.
Hewitt, P. L., Caelian, C. F., Chen, C., & Flett, G. L. (2014). Perfectionism, stress, daily hassles, hopelessness, and suicide potential in depressed psychiatric adolescents. Journal of Psychopathology and Behavioral Assessment, 36(4), 663–674.
Hewitt, P. L., & Flett, G. L. (2002). Perfectionism and stress processes in psychopathology. In G. L. Flett, & P. L. Hewitt (Eds.), Perfectionism: Theory, research, and treatment (pp. 255–284). American Psychological Association.
Hewitt, P. L., & Flett, G. L. (1993). Dimensions of perfectionism, daily stress, and depression: a test of the specific vulnerability hypothesis. Journal of Abnormal Psychology, 102(1), 58–65.
Hewitt, P. L., Flett, G. L., & Ediger, E. (1996). Perfectionism and depression: Longitudinal assessment of a specific vulnerability hypothesis. Journal of Abnormal Psychology, 105(2), 276–280.
Kirschbaum, C., Pirke, K. M., & Hellhammer, D. H. (1993). The ‘Trier Social Stress Test’–a tool for investigating psychobiological stress responses in a laboratory setting. Neuropsychobiology, 28(1–2), 76–81.
Klein, D. N., Kotov, R., & Bufferd, S. J. (2011). Personality and depression: Explanatory models and review of the evidence. Annual Review of Clinical Psychology, 7, 269–295.
Kline, R. B. (2015). Principles and practice of structural equation modeling. Guilford publications.
Lazarus, R. S. (1966). Psychological stress and the coping process. McGraw-Hill.
Levine, S. L., & Milyavskaya, M. (2018). Domain-specific perfectionism: An examination of perfectionism beyond the trait-level and its link to well-being. Journal of Research in Personality, 74, 56–65
Limburg, K., Watson, H. J., Hagger, M. S., & Egan, S. J. (2017). The relationship between perfectionism and psychopathology: A meta-analysis. Journal of Clinical Psychology, 73(10), 1301–1326.
Lovibond, S. H., & Lovibond, P. F. (1995). Manual for the depression anxiety & stress scales (2nd ed.). Psychology Foundation.
Luo, Y., Wang, Z., Zhang, H., Chen, A., & Quan, S. (2016). The effect of perfectionism on school burnout among adolescence: The mediator of self-esteem and coping style. Personality and Individual Differences, 88, 202–208.
Madigan, D. J., Stoeber, J., & Passfield, L. (2016). Perfectionism and attitudes towards doping in junior athletes. Journal of Sports Sciences, 34(8), 700–706.
Mandel, T., Dunkley, D. M., & Moroz, M. (2015). Self-critical perfectionism and depressive and anxious symptoms over 4 years: The mediating role of daily stress reactivity. Journal of Counseling Psychology, 62(4), 703–717.
McGrath, D. S., Sherry, S. B., Stewart, S. H., Mushquash, A. R., Allen, S. L., Nealis, L. J., & Sherry, D. L. (2012). Reciprocal relations between self-critical perfectionism and depressive symptoms: Evidence from a short-term, four-wave longitudinal study. Canadian Journal of Behavioural Science, 44(3), 169–181.
Molnar, D. S., Janssen, W. F., & Sirois, F. M. (2020). Sleeping perfectly? Trait perfectionism, perceived stress, and sleep quality. Personality and Individual Differences, 167, 110244.
Molnar, D. S., Sadava, S. W., Flett, G. L., & Colautti, J. (2012). Perfectionism and health: A mediational analysis of the roles of stress, social support and health-related behaviours. Psychology & Health, 27(7), 846–864.
Moroz, M., & Dunkley, D. M. (2019). Self-critical perfectionism, experiential avoidance, and depressive and anxious symptoms over two years: A three-wave longitudinal study. Behaviour Research and Therapy, 112, 18–27.
Muthén, L. K., & Muthén, B. O. (1998–2015). Mplus (Version 7.4) [Computer software]. Los Angeles, CA: Muthén & Muthén.
Nealis, L. J., Sherry, S. B., Perrot, T., & Rao, S. (2020). Self-critical perfectionism, depressive symptoms, and HPA-axis dysregulation: Testing emotional and physiological stress reactivity. Journal of Psychopathology & Behavioral Assessment, 42(3), 570–581.
O’Connor, D. B., O’Connor, R. C., & Marshall, R. (2007). Perfectionism and psychological distress: Evidence of the mediating effects of rumination. European Journal of Personality, 21(4), 429–452.
Osman, A., Wong, J. L., Bagge, C. L., Freedenthal, S., Gutierrez, P. M., & Lozano, G. (2012). The depression anxiety stress scales—21 (DASS-21): Further examination of dimensions, scale reliability, and correlates. Journal of Clinical Psychology, 68(12), 1322–1338.
Prud’homme, J., Dunkley, D. M., Bernier, E., Berg, J. L., Ghelerter, A., & Starrs, C. J. (2017). Specific perfectionism components predicting daily stress, coping, and negative affect six months and three years later. Personality and Individual Differences, 111, 134–138.
Rice, K. G., Choi, C. C., Zhang, Y., Morero, Y. I., & Anderson, D. (2012). Self-critical perfectionism, acculturative stress, and depression among international students. The Counseling Psychologist, 40(4), 575–600.
Rice, K. G., Leever, B. A., Christopher, J., & Porter, J. D. (2006). Perfectionism, stress, and social (dis)connection: A short-term study of hopelessness, depression, and academic adjustment among honors students. Journal of Counseling Psychology, 53(4), 524–534.
Rice, K. G., Richardson, C. M., & Tueller, S. (2014). The short form of the revised almost perfect scale. Journal of Personality Assessment, 96(3), 368–379.
Richardson, C. M. E., Rice, K. G., & Devine, D. P. (2014). Perfectionism, emotion regulation, and the cortisol stress response. Journal of Counseling Psychology, 61(1), 110–118.
Schlotz, W., Yim, I. S., Zoccola, P. M., Jansen, L., & Schulz, P. (2011). The perceived stress reactivity scale: Measurement invariance, stability, and validity in three countries. Psychological Assessment, 23(1), 80–94.
Selig, J. P., & Little, T. D. (2012). Autoregressive and cross-lagged panel analysis for longitudinal data. In B. Laursen, T. D. Little, & N. A. Card (Eds.), Handbook of developmental research methods (pp. 265–278). Guilford Press.
Shahar, G., Joiner, T. E. Jr., Zuroff, D. C., & Blatt, S. J. (2004). Personality, interpersonal behavior, and depression: Co-existence of stress-specific moderating and mediating effects. Personality and Individual Differences, 36(7), 1583–1596.
Sherry, S. B., Richards, J. E., Sherry, D. L., & Stewart, S. H. (2014). Self-critical perfectionism is a vulnerability factor for depression but not anxiety: A 12-month, 3-wave longitudinal study. Journal of Research in Personality, 52, 1–5.
Sinclair, S. J., Siefert, C. J., Slavin-Mulford, J. M., Stein, M. B., Renna, M., & Blais, M. A. (2012). Psychometric evaluation and normative data for the depression, anxiety, and stress scales-21 (DASS-21) in a nonclinical sample of US adults. Evaluation & the Health Professions, 35(3), 259–279.
Slaney, R. B., Rice, K. G., Mobley, M., Trippi, J., & Ashby, J. S. (2001). The revised Almost Perfect Scale. Measurement and Evaluation in Counseling and Development, 34(3), 130–145.
Smith, M. M., Sherry, S. B., Chen, S., Saklofske, D. H., Mushquash, C., Flett, G. L., & Hewitt, P. L. (2018). The perniciousness of perfectionism: A meta-analytic review of the perfectionism–suicide relationship. Journal of Personality, 86(3), 522–542.
Smith, M. M., Sherry, S. B., Vidovic, V., Hewitt, P. L., & Flett, G. L. (2020). Why does perfectionism confer risk for depressive symptoms? A meta-analytic test of the mediating role of stress and social disconnection. Journal of Research in Personality, 86, 103954.
Smith, M. M., Sherry, S. B., Ge, S. Y. J., Hewitt, P. L., Flett, G. L., & Baggley, D. L. (2021). Multidimensional perfectionism turns 30: A review of known knowns and known unknowns. Canadian Psychology/Psychologie Canadienne. https://doi.org/10.1037/cap0000288. Advance online publication
Smith, M. M., Sherry, S. B., Rnic, K., Saklofske, D. H., Enns, M., & Gralnick, T. (2016). Are perfectionism dimensions vulnerability factors for depressive symptoms after controlling for neuroticism? A meta-analysis of 10 longitudinal studies. European Journal of Personality, 30(2), 201–212.
Stoeber, J. (2018a). The psychology of perfectionism: Critical issues, open questions, and future directions. In J. Stoeber (Ed.), The psychology of perfectionism: Theory, research, applications (pp. 333–352). London: Routledge.
Stoeber, J. (2018b). The psychology of perfectionism: An introduction. In J. Stoeber (Ed.), The psychology of perfectionism: Theory, research, applications (pp. 3–16). London: Routledge.
Tonta, K. E., Howell, J. A., Hasking, P. A., Boyes, M. E., & Clarke, P. J. (2019). Attention biases in perfectionism: Biased disengagement of attention from emotionally negative stimuli. Journal of Behavior Therapy and Experimental Psychiatry, 64, 72–79.
Vanstone, D. M., & Hicks, R. E. (2019). Transitioning to university: Coping styles as mediators between adaptive-maladaptive perfectionism and test anxiety. Personality and Individual Differences, 141, 68–75.
Yiend, J., Savulich, G., Coughtrey, A., & Shafran, R. (2011). Biased interpretation in perfectionism and its modification. Behaviour Research and Therapy, 49(12), 892–900.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Suh, H., Liou, PY., Jeong, J. et al. Perfectionism, Prolonged Stress Reactivity, and Depression: A Two-Wave Cross-Lagged Analysis. J Rat-Emo Cognitive-Behav Ther 42, 54–68 (2024). https://doi.org/10.1007/s10942-022-00483-x
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10942-022-00483-x