
Abstract
The current study examined the associations among dimensions of perfectionism, facets of stress reactivity, and self-reported depressive symptoms in 191 university students. Participants completed the Multidimensional Perfectionism Scale, the Perfectionism Cognitions Inventory, the Perceived Stress Reactivity Scale (PSRS), and a measure of depressive symptoms. The PSRS is a relatively new instrument that measures several distinguishable facets of stress reactivity including prolonged stress reactivity, reactivity to failure, and reactivity to social evaluation. Analyses confirmed that most of the perfectionism measures were associated with stress reactivity to failure experiences. Socially prescribed perfectionism and perfectionistic automatic thoughts were also associated with prolonged stress reactivity and reactivity to social evaluation. Moreover, all facets of stress reactivity were correlated with depressive symptoms. Finally, prolonged stress reactivity and reactivity to social evaluation mediated the links between perfectionism dimensions and depressive symptoms. The current findings provide general support for models of perfectionism and stress, and suggest that perfectionists have heightened sensitivities to stressors related to their self-definitions that are activated when threatening stressors involving these themes are experienced.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Extensive research has now established that individual differences in perfectionism are associated with low emotional adjustment and proneness to health difficulties, including early mortality (e.g., Fry and Debats 2009). One explanation for the difficulties experienced by perfectionists involves the extent to which they are exposed to stress and their reactions to it. Initially, Hewitt and Flett (1993) posited and found empirical support for a diathesis-stress model of perfectionism and psychological distress. Considerable research has subsequently confirmed associations between perfectionism and stress (e.g., Bottos and Dewey 2004). Moreover, several studies have found that stress acts as a mediator or moderator of the link between perfectionism and psychological distress as well as the link between perfectionism and health problems (Dunkley et al. 2003; Enns and Cox 2005; Flett et al. 2012; Mandel et al. 2015; Molnar et al. 2012; Nilsson et al. 2008).
Hewitt and Flett (2002) proposed a comprehensive stress processes framework model that had as its central premise the notion that perfectionism is often accompanied by several stress mechanisms that contribute to psychopathology (i.e., stress generation, stress anticipation, stress perpetuation, and stress enhancement). A central aspect of this model is the notion that perfectionists have a heightened level of stress reactivity, especially when they experience a stressor that connotes a sense of personal failure. Personal failures that are publicly known should be especially stressful for perfectionists.
This model outlined by Hewitt and Flett (2002) has been supplemented recently by the introduction of a concept known as “perfectionistic reactivity.” This reactivity is a tendency for vulnerable perfectionists to react emotionally, cognitively, physiologically, and behaviorally in ways that are less than optimal when the individual has fallen short of personal or prescribed ideals (see Flett and Hewitt 2016). According to this model, vulnerable perfectionistic people react poorly to stressors and other challenging circumstances.
Research over the past two decades has included a number of empirical investigations suggesting that extreme perfectionists do indeed have a high level of stress reactivity and a propensity to experience more extreme negative emotional reactions. For instance, Frost et al. (1995) had students engage in either a relatively easy or a more stressful, challenging Stroop task. Those who scored high on concern over mistakes reacted to the more stressful condition in which more mistakes were actually made with more negative moods, lower confidence, and a lasting sense that they should have done better. Other research has documented perfectionists’ heightened level of responsiveness to stress with physiological measures. Hewitt et al. (2008) showed that perfectionists had prolonged physiological activation when asked to reveal the biggest mistake they had ever made. Similarly, in another laboratory investigation, Besser et al. (2008) found that perfectionists who engaged in a challenging cognitive task experienced significantly elevated levels of blood pressure. Recent longitudinal investigations have continued to illustrate the tendency for vulnerable perfectionists to be chronically stress reactive (e.g., Dunkley et al. 2014; Hawley et al. 2014; Mandel et al. 2015). For example, in one recent study, daily stress reactivity was found to mediate the longitudinal links between self-critical perfectionism and both depressive and anxious symptoms four years later, while controlling for baseline symptoms (Mandel et al. 2015).
Given the central role afforded to stress reactivity in the Hewitt and Flett (2002) stress process framework model and accumulating evidence attesting to the need to focus on perfectionism and stress (see Dunkley et al. 2016), it is surprising that some basic issues involving perfectionism and stress reactivity still need to be examined. For instance, to what extent do the various perfectionism dimensions differ in terms of their links with stress reactivity? Similarly, do perfectionists have a general tendency to be high in stress reactivity or, as suggested by Hewitt and Flett (2002), do individual differences in perfectionism reflect specific vulnerabilities such as a heightened stress reactivity following failures and setbacks? In light of the absence of this basic information, in the current study, we investigated the associations between various dimensions of perfectionism and stress reactivity as assessed by an updated self-report measure of stress reactivity with multiple facets (see Schlotz, Yim, Zoccola, Jansen, & Schulz, 2011). Stress reactivity is defined as “… a disposition that underlies individual differences in physiological and psychological stress responses. It is assumed that perceived stress reactivity is relatively stable over time, across situations and response systems” (Schlotz et al. 2011a). It is assessed by the Perceived Stress Reactivity Scale (PSRS; Schlotz et al. 2011a). The PSRS, in its current form, has five subscales that tap themes that seem highly relevant to an understanding of perfectionism. Specifically, the PSRS assesses: (1) prolonged reactivity to stress; (2) reactivity to failure; (3) reactivity to work overload; (4); reactivity to social evaluations; and (5) reactivity to social conflict. Initial work indicates that the PSRS has an invariant factor structure across gender and is associated with measures of perceived stress and chronic stress (Schlotz et al. 2011a). Research with an earlier version of the measure found in a sample of industrial employees that higher self-reported levels of stress reactivity was associated with several indicators of psychosocial stress and related psychological problems in the workplace (Limm et al. 2010).
The inclusion of the PSRS in the current research was based on our expectation that the use of this measure should illuminate the proposed link between perfectionism and stress reactivity, including how perfectionism relates to specific facets of stress reactivity. It is important to establish whether perfectionism is associated with particular vulnerabilities and tendencies to respond with stress reactivity to failure, stress reactivity to overwork, and stress reactivity to social evaluations. Does perfectionism have a pervasive link with all elements of stress reactivity, or does it have specific associations with components, such as stress reactivity to failure?
Perfectionism was assessed in the current study both in terms of trait perfectionism (i.e., self-oriented, other-oriented, and socially prescribed perfectionism) and in terms of individual differences in the frequency of perfectionistic automatic thoughts (Flett et al. 1998). Self-oriented perfectionism is focused on the striving for exceptionally high personal standards; other-oriented perfectionism assesses high standards for others; and socially prescribed perfectionism involves the perception that others have imposed impossible standards on the self (Hewitt and Flett 1991). Research with the Perfectionism Cognitions Inventory has shown that frequent perfectionistic thoughts account for unique variance in psychological distress beyond the variance attributable to individual differences in the trait perfectionism dimensions (Flett et al. 1998). Perfectionistic cognitions have been linked in recent research with feelings of defeat and entrapment (Sturman 2011) and perfectionistic cognitions have been identified in longitudinal research as potential mediators of the link between trait perfectionism and distress (Wimberly and Stasio 2013).
While trait perfectionism has been evaluated extensively within the context of exposure to life events and daily hassles, there have been few investigations thus far of the extent to which perfectionistic automatic thoughts are associated with the experience of stress and reactivity to stress. Those perfectionists who ruminate about the need to be perfect should be particularly reactive to stress. High levels of perfectionistic automatic thoughts are believed to reflect the activation of an ideal self and a propensity to emotional distress due to being aware that perfection is not being attained (Flett et al. 1998). If stress is experienced within this context, it should elicit a heightened response as the attainment of perfectionism would now seem even less likely for the ruminating perfectionist. Unfortunately, while perfectionistic automatic thoughts have been linked with stress-related conditions such as burnout (Hill and Appleton 2011), few researchers have examined the extent to which perfectionistic automatic thoughts are associated with stress. The primary exception is a recent study showing that perfectionistic automatic thoughts are associated with daily hassles in university students and the experience of daily hassles mediated the link between perfectionistic thoughts and psychosomatic symptoms (Flett et al. 2012). It was expected in the current research that the frequent experience of perfectionistic automatic thoughts would prove to be just as relevant to stress reactivity as trait perfectionism because ruminating about perfectionism and not being perfect should create a state of readiness to respond emotionally with significant intensity when stress is experienced. In addition, as noted above, perfectionistic automatic thoughts have been linked with stress-related conditions (see Hill and Appleton 2011).
Goals and Hypotheses
To our knowledge, the association between perfectionism and specific components of stress reactivity has not been examined in prior research. Accordingly, in the current study, while a general association was expected between various dimensions of perfectionism and stress reactivity, three specific hypotheses were tested. First, it was predicted that trait perfectionism and perfectionistic automatic thoughts would be associated with heightened stress reactivity to failure. This would be in keeping with numerous case descriptions of perfectionists reacting poorly to life setbacks (Flett and Hewitt 2002) as well as with empirical evidence linking trait perfectionism with a measure of inability to tolerate failure (Flett et al. 1991). It is likely that a propensity to readily perceive failures due to associated cognitive tendencies (i.e., all-or-none thinking, overgeneralization) is a core theme underscoring perfectionism, and perfectionists are highly reactive to failure experiences.
Second, it was hypothesized that stress reactivity to social evaluation would be associated with socially prescribed perfectionism due to the sensitivity to social evaluation that underscores socially prescribed perfectionism (Flett et al. 1997; Hewitt and Flett 1991; Nepon et al. 2011). Besser et al. (2010) posited in a conceptual analysis of perfectionism and self-silencing that socially prescribed perfectionists are particularly high in the need for approval and strive to please others in order to avoid interpersonal rejection. As such, people high in socially prescribed perfectionism should have a propensity to be stress reactive in social evaluation situations and this should be particularly evident among those people who feel that they can never please others due to impossible expectations being imposed on them.
Finally, given experimental evidence linking perfectionism with prolonged physiological activation (Hewitt et al. 2008), we also tested the hypothesis that perfectionism in general would be associated with prolonged stress reactivity. An association with prolonged stress reactivity would be in keeping with mounting evidence of the health problems of perfectionists and indications that perfectionists have deficits in cognitive-emotional regulation (Rudolph et al. 2007), as well as the suggestion from Hewitt and Flett (2002) that vulnerable perfectionists have maladaptive tendencies that perpetuate and prolong stressful experiences and related reactions.
Additionally, we examined the association between stress reactivity and depressive symptoms for various reasons, including being able to explore the related possibility that certain facets of stress reactivity mediate the association between perfectionism and symptoms of depression. Hewitt and Flett (2002) posited that stress reactivity is a mediator of the link between perfectionism and symptoms of depression. Our mediational analyses in the current study were guided by conceptual considerations as well as our understanding of the nature of the various perfectionism dimensions. We focused on two elements of stress reactivity in mediational analyses – prolonged reactivity and reactivity to social evaluation. We tested the notion that prolonged reactivity and reactivity to social evaluation are key mediators of the links that both socially prescribed perfectionism and perfectionistic cognitions have with depressive symptoms. We focused on these two facets of the stress reactivity construct instead of the other components due to our belief and empirical evidence indicating that these elements are most relevant to the daily pressures, hassles, and evaluative concerns encountered by people who have elevated scores on socially prescribed perfectionism and who ruminate frequently about the need to be perfect (see Hewitt and Flett 2002).
Method
Participants and Procedure
The sample consisted of 191 university students (106 women and 85 men) with a mean age of 20.5 years (SD = 3.7). Participants were recruited through the Undergraduate Research Participant Pool at a large Canadian university. Most students reported either psychology (32.5 %) or kinesiology (24.6 %) as their intended major. We did not assess certain demographic variables (i.e., race, cultural background) in accordance with provincial laws and regulations. However, we can state that the participants were recruited from a university setting that is associated with significant levels of stress and psychological problems among students. Indeed, Data from our university’s participation in the 2009 American College Health Association Survey found that among the 634 students surveyed, 42.5 % indicated that sometime within the previous year they had felt so depressed that it was difficult to function and 23.6 % indicated that they had felt this way during the past month (see American College Health Association 2009). More than half of the respondents in this survey (54.4 %) reported experiencing greater than average stress or tremendous stress over the past year.
After providing their consent, a series of questionnaires were administered to the participants over the Internet.
Measures
Multidimensional Perfectionism Scale (MPS; Hewitt and Flett 1991)
The MPS is a 45-item measure assessing self-oriented perfectionism (15 items: e.g., “I strive to be as perfect as I can be”); other-oriented perfectionism (15 items: e.g., “Everything that others do must be of top-notch quality”); and socially prescribed perfectionism (15 items: e.g., “People expect nothing less than perfection from me”). Respondents rate their agreement or disagreement with each item on a scale from 1 (Strongly Disagree) to 7 (Strongly Agree). Considerable research has shown that the MPS is a multidimensional scale with high reliability and validity in student and clinical samples (Enns and Cox 2002; Hewitt and Flett 2004).
Perfectionism Cognitions Inventory (PCI; Flett et al. 1998)
The PCI is a 25-item questionnaire that measures the frequency of negative automatic thoughts involving the need to be perfect. Respondents rate how often they have experienced thoughts over the past week, such as “Why can’t I be perfect?” Items are rated on a Likert scale ranging from 0 (not at all) to 4 (all of the time). This scale possesses high internal consistency in student and clinical samples (Flett et al. 1998; Flett et al. 2007). Additionally, the PCI possesses good test-retest reliability and sufficient predictive and concurrent validity (Flett et al. 1998).
Perceived Stress Reactivity Scale (PSRS; Schlotz et al. 2011a)
The PSRS is a 23-item measure composed of five subscales. Four of the five subscales are situation-specific with the exception being the prolonged reactivity subscale, which assesses prolonged activation due to finding it difficult to relax and wind down (4 items: e.g., “When tasks and duties accumulate to the extent that they are hard to cope with... My sleep is unaffected, My sleep is slightly disturbed, My sleep is very disturbed”). The situation-specific subscales assess reactivity to work overload (5 items: e.g., “When tasks and duties build up to the extent that they are hard to manage... I am generally untroubled, I usually feel a little uneasy, I normally get quite nervous”); reactivity to social conflicts (5 items: e.g., “When I argue with other people... I usually calm down quickly, I usually stay upset for some time, It usually takes me a long time until I calm down”); reactivity to failure (4 items: e.g., “When I fail at a task... I usually feel very uncomfortable, I usually feel somewhat uncomfortable, In general, I don’t mind;” reverse-scored); and reactivity to social evaluation (5 items: e.g., “When others criticize me... I generally don’t lose confidence at all, I generally lose a little confidence, I generally feel very unconfident”). The PSRS has demonstrated good reliability over a four-week period (Schlotz et al. 2011a). The validity of this measure is supported by its associations in student and non-student samples with relevant constructs, such as perceived stress and chronic stress (Schlotz et al. 2011a; Schlotz, Phillips, & the Hertfordshire Cohort Study Group, 2013).
Center for Epidemiological Studies-Depression Scale (CES-D; Radloff 1977)
The CES-D is a 20-item scale measuring the current level of depressive symptoms in the general population. This measure assesses both affective (e.g., “I felt lonely”) and somatic (e.g., “I had crying spells”) symptoms. This scale possesses sufficient reliability and validity (Radloff 1977).
Results
Data Analytic Plan
Prior to conducting statistical analyses, we performed a missing values analysis. Across participants, there was a small amount of missing data on the variables of interest (less than 5 %). Little’s MCAR test was not significant and, therefore, the values are likely to be missing in a random way. Missing values were then imputed using the expectation-maximization method in SPSS. Descriptive statistics were calculated for the total sample, which was then followed by correlational analyses to initially examine the associations among dimensions of perfectionism, facets of stress reactivity, and depressive symptoms. The correlational analyses informed the subsequent mediational analysis by helping us to decide which facets of stress reactivity to include as the mediator.
Next, a structural equation model was tested with AMOS Version 18 software using maximum likelihood estimation procedures to explore if aspects of stress reactivity mediate the links that socially prescribed perfectionism and perfectionistic cognitions have with depressive symptoms. Specifically, the mediator was a latent factor composed of prolonged reactivity and reactivity to social evaluation. In order to further examine the significance of the indirect effects, 2000 bootstrap samples were generated to obtain 95 % bias-corrected bootstrap confidence intervals (MacKinnon et al. 2004; Preacher and Hayes 2008). If the confidence intervals do not contain zero, then the indirect effects are considered to be significant.
Descriptive Statistics
The means, standard deviations, and alpha coefficients for all measures are listed in Table 1. Most notably, the PSRS subscales yielded alphas ranging from .56 to .73. While the levels of internal consistency for three subscales were within the ranges reported in the original scale development article, the alphas of .56 for both reactivity to failure and reactivity to social evaluation were lower than expected. The low alphas here may be a result of having few items in each subscale (see Gosling et al. 2003 for a discussion) or perhaps certain items are not tapping into the underlying construct. These reduced levels of internal consistency have implications in terms of constraining the magnitude of the correlations described below. The mean of the CES-D was 19.66, and a score of 16 or higher is considered to be the cut-off for at least mild levels of depression (Radloff 1977).
Correlational Analyses
Table 2 presents the intercorrelations among all of the variables. It can be seen that self-oriented perfectionism was correlated positively with stress reactivity to failure. Socially prescribed perfectionism and perfectionistic cognitions were all positively associated with prolonged reactivity, reactivity to failure, reactivity to social evaluation, as well as with depressive symptoms. There was also a small but significant association between socially prescribed perfectionism and reactivity to work overload. Further, socially prescribed perfectionism and perfectionistic cognitions were associated with greater symptoms of depression. Lastly, all of the subscales of perceived stress reactivity were positively correlated with symptoms of depression.
Mediation Analyses
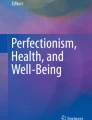
A structural equation model was tested with socially prescribed perfectionism and perfectionistic cognitions as the predictors, a latent factor comprising prolonged reactivity and reactivity to social evaluation as the mediator, and depressive symptoms as the outcome (Fig. 1). Other stress reactivity dimensions (e.g., failure reactivity) were poor fitting on the latent factor and do not necessarily reflect ongoing experience, so they were not included. The correlation between socially prescribed perfectionism and perfectionistic cognitions was also reflected in this model. We screened for normality of the outcome variable (i.e., depression) prior to performing this analysis. Depression was positively skewed, however, the robust bootstrapping method was used and this approach does not impose the assumption of normality. This model was an excellent fit to the data, χ 2 (2) = 0.16, p = .921, CFI = 1.00, TLI = 1.06, SRMR = .005, RMSEA = .00, 90 % CI = .00, .05, p close = .950. Socially prescribed perfectionism was positively associated with stress reactivity which, in turn, was positively related to depressive symptoms. Socially prescribed perfectionism was no longer significantly linked with depressive symptoms when the mediator (i.e., stress reactivity) was included in the model. Without the mediator in the model, socially prescribed perfectionism was significantly linked with depressive symptoms (ß = .22, p < .01), which enabled us to explore possible mediational results. Perfectionistic cognitions was not significantly linked with stress reactivity or with depressive symptoms when socially prescribed perfectionism is accounted for in the model. Both socially prescribed perfectionism and perfectionistic cognitions significantly accounted for 32.1 % of the variance in stress reactivity scores. In addition, both dimensions of perfectionism and stress reactivity significantly accounted for 54.1 % of the variance in depression scores. Lastly, socially prescribed perfectionism and perfectionistic cognitions were positively correlated (r = .49, p < .001), as expected.
To test if the indirect (i.e., mediated) effect of socially prescribed perfectionism on depressive symptoms through stress reactivity was significant, 2000 bootstrap samples were generated to obtain 95 % bias-corrected bootstrap confidence intervals. The 95 % confidence interval for the mediated effect of socially prescribed perfectionism on depressive symptoms through stress reactivity was .14 to 1.29. Because this interval does not contain zero, the indirect effect of socially prescribed perfectionism on depressive symptoms through stress reactivity is significant. The kappa-squared value for the indirect effect is 0.54. Therefore, prolonged reactivity and reactivity to social evaluation mediated the link between socially prescribed perfectionism and symptoms of depression.

Final model of socially prescribed perfectionism and perfectionistic cognitions, stress reactivity, and depressive symptoms. Note. ***p < .001. Standardized parameter estimates are shown. Error terms and the correlation between socially prescribed perfectionism and perfectionistic cognitions have been omitted for ease of presentation
Discussion
The current study had three inter-related goals. First, and foremost, in a university setting in which high levels of depressive symptoms and stress are being experienced in general, we examined the extent to which trait perfectionism and ruminating about the need to be perfect are associated with self-reported facets of stress reactivity with a measure that provided assessments of stress reactivity in situation-specific contexts. Second, the current study evaluated the extent to which both perfectionism and stress reactivity components were associated with depressive symptoms. Third, we evaluated whether theoretically relevant facets of stress reactivity (i.e., prolonged reactivity and reactivity to social evaluation) mediated the links between perfectionism and depressive symptoms in a manner that would be in keeping with predictions derived from the stress processes framework model advanced by Hewitt and Flett (2002).
Our analyses confirmed that trait perfectionism dimensions and the tendency to ruminate about the need to be perfect were associated with key facets of stress reactivity. Most notably, in keeping with past descriptions and empirical evidence linking perfectionism with failure intolerance (Flett et al. 1991), stress reactivity to failure was associated significantly with the perfectionism dimensions with the exception of other-oriented perfectionism. Overall, it seems that perfectionistic individuals have a pervasive tendency to be over-reactive to failure and this is likely accompanied by a tendency to be hypervigilant in looking for failure cues. This stress reactivity has emotional costs given its link with depressive symptoms in the current study, but it also should contribute to the health costs experienced by perfectionists. This conclusion follows from a laboratory investigation showing that stress reactivity to failure is associated with steeper cortisol responses among people exposed to a stressful social evaluation situation (Schlotz et al. 2011b).
The significant link between self-oriented perfectionism and stress reactivity to failure in the current study is particularly noteworthy in that it has been suggested by some authors that self-oriented perfectionism can be adaptive at times (Stoeber and Otto 2006). However, as clearly indicated by Hewitt and Flett (1991, 1993, 2002), extreme self-oriented perfectionism represents a vulnerability factor when repeated achievement failures and setbacks are experienced and it is important to consider life outcomes and extant situational contexts that impinge on this tendency to react strongly and negatively when faced with personal failures. The current results and the interpretation of these results fits nicely with other experimental evidence showing how self-oriented perfectionists feel threatened following a personal failure to the point that effort is withdrawn (Hill et al. 2011).
The obtained correlations between perfectionism and failure reactivity were significant but relatively modest in association, especially if interpreted within the context of the more robust links between depressive symptoms and the stress reactivity factors. However, it is important to note that only a subset of those students with elevated stress reactivity tend to be perfectionists, while other students are stress reactive for a variety of other reasons and this probably limited the magnitude of the correlations in the current study. That is, there will be heterogeneity among those who are high in stress reactivity and other personality and temperament factors need to be taken into account as well. It is for this reason that the link between stress reactivity and perfectionism may actually be underestimated by the magnitude of the correlations found in the present study. Moreover, there were no significant links found between other-oriented perfectionism and any of the PSRS subscales. In general, this is in keeping with past findings that this dimension of trait perfectionism is not significanty linked with indices of stress (see Hewitt and Flett 2002). Perhaps different forms of stress reactivity are related to other-oriented perfectionism, such as the stress when other people are not meeting their exacting standards or more specifically, when they do not receive enough social support.
As expected, socially prescribed perfectionism was associated with heightened stress reactivity to social evaluation. This association was not large in magnitude, perhaps due, at least in part, to the relatively low reliability of the reactivity to social evaluation subscale. Regardless, our finding is in keeping with other evidence illustrating the extreme interpersonal sensitivity inherent in socially prescribed perfectionism (Hewitt and Flett 1991). Intuitively, it seems that socially prescribed perfectionists should be especially reactive to public humiliations and stressful setbacks that convey negative social evaluations. This is important to acknowledge because it is likely a key mechanism that helps account for some of the findings emerging from recent tests of the perfectionism social disconnection model (Hewitt et al. 2006; Nepon et al. 2011). The essence of this model is that individuals with high levels of interpersonal perfectionism become socially isolated and prone to loneliness because of their sensitivity to negative feedback from other people. Socially prescribed perfectionism was the only dimension to be significantly correlated with reactivity to work overload; however, this correlation was small in magnitude.
While there were several unique findings in our correlational results, two findings in particular should be noted. First, socially prescribed perfectionism and perfectionistic cognitions were associated with prolonged reactivity to stress. Our results suggest that when under stress, perfectionists are prone to the kind of chronic and prolonged stress that often results in chronic depressive symptoms and stress-related health problems. Perhaps this is one reason why longitudinal research has established links between trait perfectionism and early mortality (Fry and Debats 2009). Extreme perfectionists are people who not only get exposed to stress on a frequent basis, but the stress reactivity of many perfectionists is prolonged and extensive. This tendency may contribute to a situation in which perfectionists have chronic stress exposure.
Second, research has not extensively examined the association between perfectionistic cognitions and stress, but we found that students with elevated PCI scores also tended to have elevated scores on several indices of stress reactivity. In addition to the already acknowledged link with prolonged stress reactivity, the PCI was linked with higher stress reactivity to social evaluation and stress reactivity to failure experiences. One way of interpreting these results is to suggest that when the need to be perfect is cognitively salient and is a focus of ongoing rumination, perfectionists are particularly likely to react to stress. According to Flett et al. (1998), the experience of frequent thoughts about the need to be perfect reflects the cognitive activity of an ideal self-schema and the individual’s awareness that perfection is not being attained. One possibility is that perhaps high PCI scorers tend to have heightened stress reactivity because the experience of stress is yet another indication that current circumstances and performance outcomes are discrepant from the ideal self. The association between perfectionistic automatic thoughts and stress reactivity is likely quite complex and reciprocal when viewed from a temporal perspective; that is, perfectionistic cognitions likely contribute to heightened stress reactivity but the experience of heightened stress reactivity and associated appraisals probably also contributes to the subsequent experience of perfectionistic thoughts.
Other analyses confirmed that all five PSRS factors were associated with elevated levels of self-reported depressive symptoms. The highest correlation with depressive symptoms was found with stress reactivity to social evaluation. It is evident from this study that students prone to depressive symptoms are highly reactive to stressors and pressures involving social evaluation situations. The associations between elevated CES-D scores and various manifestations of stress reactivity indicate that there is a substantial proportion of students who begin university with a predisposition to react strongly and very negatively to stressful experiences, both in terms of reactivity to failure experiences and situations involving interpersonal evaluations and conflicts. Clearly, these students should benefit substantially from stress management interventions and preventive efforts designed to boost their levels of resilience. There should be substantial merit in focusing on stress reactions to failures and interpersonal problems.
We also found in the current study that socially prescribed perfectionism and perfectionistic cognitions were associated with depressive symptoms. These findings are consistent with prior research demonstrating links between these aspects of perfectionism and depressive symptoms (e.g., Flett et al. 1998; Nepon et al. 2011). These data emphasize that interventions designed for perfectionists to reduce their stress and depressive symptoms should not focus solely on trait perfectionism because it is also important to reduce automatic thoughts about the need to be perfect.
Our mediational analyses indicated that a stress reactivity latent variable comprising prolonged reactivity and reactivity to social evaluation mediated the link between socially prescribed perfectionism and symptoms of depression. Both socially prescribed perfectionism and perfectionistic cognitions were in the same model and only significant mediational results were found with socially prescribed perfectionism. These results with socially prescribed perfectionism indicate that this trait dimension is particularly likely to result in depressive symptoms when there is a proclivity to react strongly to social evaluation pressure and associated stressors. While we did not actually measure stress per se in the current study, our emphasis on reactivity to social evaluation in the mediational analyses was based on our claim that students with high levels of socially prescribed perfectionism experience chronic psychosocial stress as a result of perceiving continuously that other people expect them to be perfect. Implicit in this view is the need to take ongoing stressors and the current life context into account in future research in this area. It follows that the elevated stress reactivity in response to failure will be a key factor among those perfectionists who are actually experiencing ego-involving failures. Similarly, stress reactivity to conflict and perfectionism needs to be examined within interpersonal contexts that may involve an element of conflict.
The current study extended research on perfectionism and stress reactivity in several respects. For instance, it was confirmed that aspects of perfectionism are associated with stress reactivity to failure experiences, perfectionistic cognitions are linked with stress reactivity and this is especially the case with reactivity to social evaluation, and aspects of stress reactivity (i.e., prolonged reactivity and reactivity to social evaluation) mediated the link between socially prescribed perfectionism and symptoms of depression.
The limitations of our investigation should be noted. First, our results were cross-sectional and correlational; as such, it cannot be inferred from these data that perfectionism contributes causally to stress reactivity. Indeed, from a developmental perspective, a heightened level of stress reactivity could result in a child becoming more perfectionistic in an attempt to control his or her reactions and feelings. Second, the present study relied on self-report measures that may not capture key aspects of the link between perfectionism and reactivity to stress. It will be important to examine perfectionism and stress reactivity in specific life contexts focused on the daily experiences of perfectionists (Dunkley et al. 2003). Third, it is evident that the current results may only apply to university students, mostly in their first year, and may not generalize to people from the general population or to the extreme stress and perfectionism found among some people with clinical dysfunction. It is particularly important that perfectionism and stress reactivity be examined in people employed in occupations that vary in terms of their stressfulness. Despite this limitation, university students face difficult challenges when making the transition to university (see Goldstein et al. 2009; Vredenburg et al. 1993) and we felt it was particularly appropriate to focus on students in light of growing concerns about levels of stress, depressive symptoms, and mental health among students (Bayram and Bilgel 2008). Also, undergraduate students have extensive exposure to stressful events and greater stress exposure is associated with psychological distress, trauma symptoms, health problems, lower life satisfaction, and lower grade point average (Anders et al. 2012).
It is also important in future research to show that the links between perfectionism and stress reactivity are still evident after controlling for related individual differences in neuroticism, given that neuroticism is believed to incorporate an emphasis on stress reactivity. Lastly, the PSRS reactivity to failure and social evaluation subscales in the present study had relatively low levels of internal consistency. These values were low even allowing for the tendency noted by the instrument’s creators for North American university students to respond to scale items in a way that results in lower alpha levels (Schlotz et al. 2011a). While it is possible and tempting to use a total score that collapses across the five stress reactivity facets, the links between perfectionism and reactivity to failure are consistent with expectations. Nevertheless, it must be reiterated that because the PSRS subscales tapping stress reactivity to failure and to social evaluation had relatively low alphas, findings involving these subscales should be interpreted with caution. In this instance, it is worth noting that if we had corrected for attenuation, correlations between perfectionism and these facets of stress reactivity would have been much larger in magnitude.
In summary, the results of the current study confirmed past suggestions that perfectionists are high in stress reactivity. We found pervasive links between various dimensions of perfectionism and key facets of stress reactivity. Most of the perfectionism measures were associated with stress reactivity in response to failure. As expected, stress reactivity to social evaluation was correlated with socially prescribed perfectionism and perfectionistic cognitions. Further, most of the perfectionism dimensions were correlated with prolonged reactivity. Additional findings confirmed that all facets of stress reactivity were associated with depressive symptoms, but not to the extent that they are redundant with each other. There was also evidence that prolonged stress reactivity and reactivity to social evaluation mediated the link between socially prescribed perfectionism and symptoms of depression. Collectively, these findings continue to indicate that higher levels of stress exposure and reactivity are implicated in the well-being of extreme perfectionists and it is important to examine perfectionists in stressful contexts that test their ability to withstand stressful life experiences.
References
American College Health Association (2009). York University executive summary spring 2009 American college health assessment National College Health Assessment II. Hanover, MD: American College Health Association.
Anders, S. L., Frazier, P. A., & Shallcross, S. L. (2012). Prevalence and effects of life event exposure among undergraduate and community college students. Journal of Counseling Psychology, 59, 449–457.
Bayram, N., & Bilgel, N. (2008). The prevalence and socio-demographic correlations of depression, anxiety, and stress among a group of university students. Social Psychiatry and Psychiatric Epidemiology, 43, 667–672.
Besser, A., Flett, G. L., Hewitt, P. L., & Guez, J. (2008). Perfectionism and cognitions, affect, self-esteem, and physiological reactions in a performance situation. Journal of Rational-Emotive & Cognitive-Behavior Therapy, 26, 206–228.
Besser, A., Flett, G. L., & Hewitt, P. L. (2010). Silencing the self and personality vulnerabilities associated with depression. In D. Jack & A. Ali (Eds.), Silencing the self across cultures: Depression and gender in the social world (pp. 285–312). London: Oxford University Press.
Bottos, S., & Dewey, D. (2004). Perfectionists’ appraisal of daily hassles and chronic headache. Headache: The Journal of Head and Face Pain, 44, 772–779.
Dunkley, D. M., Zuroff, D. C., & Blankstein, K. R. (2003). Self-critical perfectionism and daily affect: dispositional and situational influences on stress and coping. Journal of Personality and Social Psychology, 84, 234–252.
Dunkley, D. M., Mandel, T., & Ma, D. (2014). Perfectionism, neuroticism, and daily stress reactivity and coping effectiveness 6 months and 3 years later. Journal of Counseling Psychology, 61, 616–633.
Dunkley, D. M., Solomon-Krakus, S., & Moroz, M. (2016). Personal standards and self-critical perfectionism and distress: stress, coping, and perceived social support as mediators and moderators. In F. M. Sirois & D. S. Molnar (Eds.), Perfectionism, health, and well-being (pp. 157–176). Switzerland: Springer International Publishing.
Enns, M. W., & Cox, B. J. (2002). The nature and assessment of perfectionism. In G. L. Flett & P. L. Hewitt (Eds.), Perfectionism: Theory, research, and treatment (pp. 33–62). Washington, DC: American Psychological Association.
Enns, M. W., & Cox, B. J. (2005). Perfectionism, stressful life events, and the 1-year outcome of depression. Cognitive Therapy and Research, 29, 541–553.
Flett, G. L., & Hewitt, P. L. (2002). Perfectionism and maladjustment: an overview of theoretical, definitional, and treatment issues. In G. L. Flett & P. L. Hewitt (Eds.), Perfectionism: Theory, research, and treatment (pp. 5–31). Washington, DC: American Psychological Association.
Flett, G. L., & Hewitt, P. L. (2016). Reflections of perfection and the pressure to be perfect in athletes, dancers, and exercisers: a focus on perfectionistic reactivity in key situations and life contexts. In A. P. Hill (Ed.), The psychology of perfectionism in sport, dance, and exercise. London: Routledge.
Flett, G. L., Hewitt, P. L., Blankstein, K. R., & Mosher, S. W. (1991). Perfectionism, self-actualization, and personal adjustment. Journal of Social Behavior and Personality, 6, 147–160.
Flett, G. L., Hewitt, P. L., Garshowitz, M., & Martin, T. R. (1997). Personality, negative social interactions, and depressive symptoms. Canadian Journal of Behavioural Science, 29, 28–37.
Flett, G. L., Hewitt, P. L., Blankstein, K. R., & Gray, L. (1998). Psychological distress and the frequency of perfectionistic thinking. Journal of Personality and Social Psychology, 75, 1363–1381.
Flett, G. L., Hewitt, P. L., Whelan, T., & Martin, T. R. (2007). The perfectionism cognitions inventory: psychometric properties and associations with distress and deficits in cognitive self-management. Journal of Rational-Emotive & Cognitive-Behavior Therapy, 25, 255–277.
Flett, G. L., Molnar, D. S., Nepon, T., & Hewitt, P. L. (2012). A mediational model of perfectionistic automatic thoughts and psychosomatic symptoms: the roles of negative affect and daily hassles. Personality and Individual Differences, 52, 565–570.
Frost, R. O., Turcotte, T., Heimberg, R. G., & Mattia, J. I. (1995). Reactions to mistakes among subjects high and low in perfectionistic concern over mistakes. Cognitive Therapy and Research, 19, 195–205.
Fry, P. S., & Debats, D. L. (2009). Perfectionism and the five-factor personality traits as predictors of mortality in older adults. Journal of Health Psychology, 14, 513–524.
Goldstein, A. L., Flett, G. L., Wekerle, C., & Wall, A.-M. (2009). Personality, child maltreatment, and substance use: examining correlates of deliberate self-harm among university students. Canadian Journal of Behavioural Science, 41, 241–251.
Gosling, S. D., Rentfrow, P. J., & Swann Jr., W. B. (2003). A very brief measure of the big-five personality domains. Journal of Research in Personality, 37, 504–528.
Hawley, L. L., Zuroff, D. C., Brozina, K., Ho, M.-H. R., & Dobson, K. S. (2014). Stress-critical perfectionism and stress reactivity following cognitive behavioral therapy for depression. International Journal of Cognitive Therapy, 7, 287–303.
Hewitt, P. L., & Flett, G. L. (1991). Perfectionism in the self and social contexts: conceptualization, assessment, and association with psychopathology. Journal of Personality and Social Psychology, 60, 456–470.
Hewitt, P. L., & Flett, G. L. (1993). Dimensions of perfectionism, daily stress, and depression: a test of the specific vulnerability hypothesis. Journal of Abnormal Psychology, 102, 58–65.
Hewitt, P. L., & Flett, G. L. (2002). Perfectionism and stress in psychopathology. In G. L. Flett & P. L. Hewitt (Eds.), Perfectionism: Theory, research, and treatment (pp. 255–284). Washington, DC: American Psychological Association Press.
Hewitt, P. L., & Flett, G. L. (2004). Multidimensional Perfectionism Scale: Technical manual. Toronto, ON: Multi-Health Systems Inc..
Hewitt, P. L., Flett, G. L., Sherry, S. B., & Caelian, C. F. (2006). Trait perfectionism dimensions and suicide behavior. In T. E. Ellis (Ed.), Cognition and suicide: Theory, research, and therapy (pp. 215–235). Washington, DC: American Psychological Association.
Hewitt, P. L., Habke, A. M., Lee-Baggley, D. L., Sherry, S. B., & Flett, G. L. (2008). The impact of perfectionistic self-presentation on the cognitive, affective, and physiological experience of a clinical interview. Psychiatry: Interpersonal and Biological Processes, 71, 93–122.
Hill, A. P., & Appleton, P. R. (2011). The predictive ability of the frequency of perfectionistic cognitions, self-oriented perfectionism, and socially prescribed perfectionism in relation to symptoms of burnout in youth rugby players. Journal of Sports Sciences, 29, 695–703.
Hill, A. P., Hall, H. K., Duda, J. L., & Appleton, P. R. (2011). The cognitive, affective, and behavioural responses of self-oriented perfectionists following successive failure on a muscle endurance task. International Journal of Sport and Exercise Psychology, 9, 189–207.
Limm, H., Angerer, P., Heinmuller, M., Marten-Mittag, B., Nater, U. M., & Guendel, H. (2010). Self-perceived stress reactivity is an indicator of psychosocial impairment in the workplace. BMC Public Health, 10, 252. doi:10.1186/1471-2458-10-252.
MacKinnon, D. P., Lockwood, C. M., & Williams, J. (2004). Confidence limits for the indirect effect: distribution of the product and resampling methods. Multivariate Behavioral Research, 39, 99–128.
Mandel, T., Dunkley, D. M., & Moroz, M. (2015). Self-critical perfectionism and depressive and anxious symptoms over 4 years: the mediating role of daily stress reactivity. Journal of Counseling Psychology, 62, 703–717.
Molnar, D. S., Sadava, S. W., Flett, G. L., & Colautti, J. (2012). Perfectionism and health: a mediational analysis of the role of stress, social support, and health-related behaviours. Psychology and Health, 27, 846–864.
Nepon, T., Flett, G. L., Hewitt, P. L., & Molnar, D. (2011). Perfectionism, negative social feedback, and interpersonal rumination in depression and social anxiety. Canadian Journal of Behavioural Science, 43, 297–308.
Nilsson, J. E., Butler, J., Shouse, S., & Joshi, C. (2008). The relationships among perfectionism, acculturation and stress in Asian international students. Journal of College Counseling, 11, 147–158.
Preacher, K. J., & Hayes, A. F. (2008). Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behavior Research Methods, 40, 879–891.
Radloff, L. S. (1977). The CES-D scale: a self-report depression scale for research in the general population. Applied Psychological Measurement, 1, 385–401.
Rudolph, S. G., Flett, G. L., & Hewitt, P. L. (2007). Perfectionism and deficits in cognitive emotion regulation. Journal of Rational-Emotive & Cognitive-Behavior Therapy, 25, 343–357.
Schlotz, W., Yim, I. S., Zoccola, P. M., Jansen, L., & Schulz, P. (2011a). The perceived stress reactivity scale: measurement invariance, stability, and validity in three countries. Psychological Assessment, 23, 80–94.
Schlotz, W., Hammerfeld, K., Ehlert, V., & Gaab, J. (2011b). Individual differences in the cortisol response to stress in young health men: testing the role of perceived stress reactivity and threat appraisal using multiphase latent growth curve modeling. Biological Psychiatry, 87, 257–264.
Schlotz, W., Phillips, D. I. W., & the Hertfordshire Cohort Study Group (2013). Birth weight and stress reactivity in older age. Stress and Health, 29, 56–63.
Stoeber, J., & Otto, K. (2006). Positive conceptions of perfectionism: approaches, evidence, challenges. Personality and Social Psychology Review, 10, 295–319.
Sturman, E. D. (2011). Involuntary subordination and its relation to personality, mood, and submissive behavior. Psychological Assessment, 23, 262–276.
Vredenburg, K., Flett, G. L., & Krames, L. (1993). Analogue versus clinical depression: a critical re-appraisal. Psychological Bulletin, 113, 327–344.
Wimberly, T. E., & Stasio, M. J. (2013). Perfectionistic thoughts, personal standards, and evaluative concerns: further investigating relationships to psychological distress. Cognitive Therapy and Research, 37, 277–285.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Gordon L. Flett, Taryn Nepon, Paul L. Hewitt and Kristine Fitzgerald declare that they have no conflict of interest.
Experiment Participants
This study has been reviewed and approved for compliance to research ethics protocols by the Human Participants in Research Committee of our institution.
Additional information
This research was supported by a research grant from the Social Sciences and Humanities Research Council (SSHRC) of Canada. The first author was also supported by a Canada Research Chair in Personality and Health.
Rights and permissions
About this article

Cite this article
Flett, G.L., Nepon, T., Hewitt, P.L. et al. Perfectionism, Components of Stress Reactivity, and Depressive Symptoms. J Psychopathol Behav Assess 38, 645–654 (2016). https://doi.org/10.1007/s10862-016-9554-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10862-016-9554-x