
Abstract
Purpose
Immunoglobulin(Ig)G-subclass deficiency and specific polysaccharide antibody deficiency (SPAD) are among the most frequent causes of recurrent respiratory infections in children. Little is known about their prevalence, clinical presentation and prognosis. No study has been published in a Western-European nor in a mainly non-tertiary cohort until now. Therefore, we performed this observational cohort study in children recruited from secondary and tertiary pediatric practices all over The Netherlands.
Methods
Dutch pediatricians were monthly asked to report patients with IgG-subclass deficiency and/or SPAD. Demographic, clinical and laboratory characteristics were collected. Separate informed consent was asked from parents and children (≥12 years of age) for annual update of the medical status.
Results
49 children with confirmed IgG-subclass deficiency and/or SPAD were included. The majority of children (69 %) was reported by four (out of 12) secondary hospitals with a pediatric immunologist in the staff. 45 children had ≥1 low IgG-subclass level and 11 had SPAD. IgG2 deficiency was the most prevalent IgG-subclass deficiency (37/49;76 %). 10 % of these children already showed bronchiectasis. Two-thirds were male (33/49;67 %, p = 0.015). From 10 years of age, only boys were left and only boys showed progressive immunodeficiency during follow-up (11/24; 46 %).
Conclusions
This is the first Western-European mainly non-tertiary cohort of children with IgG-subclass deficiency and/or SPAD. The disease course is not always benign, especially in boys. Most children were reported and managed in secondary hospitals with a pediatric immunologist in the staff. To identify more patients, the awareness of these diseases among general pediatricians should increase.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Young children often suffer from respiratory infections, which are usually innocent and self-limiting. However, in some cases these infections are a sign of underlying primary immunodeficiency. It is difficult for pediatricians to decide in which children further investigations are warranted. Among primary immunodeficiencies, ‘predominantly antibody deficiency’ forms by far the largest subgroup [1]. Immunoglobulin (Ig) G-subclass deficiency and specific polysaccharide antibody deficiency (SPAD) are among the most common forms found in children who are analysed because of the clinical presentation of recurrent ear-nose-throat (ENT) and airway infections [2, 3].
IgG-subclass deficiency is defined as a deficiency in one or more IgG-subclasses (>2 SD below age- matched reference values) with normal or near normal IgG concentration. SPAD is diagnosed when there is profound alteration of the antibody response to polysaccharide antigens, either after documented invasive infection with e.g. S. pneumoniae or after test immunization with an unconjugated pneumococcal (or other) polysaccharide vaccine. For both diagnoses, T cell and more severe B cell defects should be excluded [4]. Children with IgG-subclass deficiency or SPAD can be asymptomatic, but if not typically present with increased susceptibility to bacterial ENT and respiratory tract infections, more often so when both IgG-subclass deficiency and SPAD are present in the same child [5]. Identifying children with IgG-subclass deficiency and/or SPAD among the many children seen in everyday practice can be challenging. Healthy young children can have up to 11 respiratory infections per year [6–8], so it is difficult to decide which children with recurrent infections are at the end of the normal spectrum and which children need further immunological work-up. Furthermore, it is not known which child with IgG-subclass deficiency and/or SPAD is just showing delayed maturation of the immune system with spontaneous resolve of the immunodeficiency within a few years, and in which child it is the first sign of a lasting primary antibody deficiency, or maybe even a development into a more severe one, like common variable immunodeficiency disorders (CVID).
Little is known about the prevalence, clinical presentation and prognosis of IgG-subclass deficiency and/or SPAD in children. An Australian study in a cohort from a tertiary center showed SPAD in 11/74 (15 %) children with recurrent infections. SPAD was found in 10/91 (11 %) children with recurrent infections in a Finnish cohort from a tertiary center [9, 10]. Both studies excluded children with concomitant other immunodeficiencies. SPAD was associated with allergic rhinitis and chronic otorrhea in these children, independent of age. In a retrospective study among 59 Turkish children with IgG-subclass deficiency from a tertiary center, IgG3-deficiency was most commonly found; 30 % of these children reached normal values around the age of 6 years. In contrast, children with an isolated IgG2-deficiency in this cohort (9 %) all remained IgG2-deficient during follow-up [11]. In a group of Thai children with recurrent infections recruited in a tertiary care hospital, 7/55 (13 %) had an IgG-subclass deficiency. The most common presenting symptom was recurrent sinusitis (84 %). Again, IgG3-deficiency was the most common IgG-subclass deficiency found (56 %) [12]. All of these studies were carried out in tertiary center cohorts and therefore in a highly selective population of children. No study has been published in a Western-European cohort until now, nor have children followed outside tertiary centers been included. Therefore, we performed this observational cohort study for IgG-subclass deficiency and/or SPAD in children recruited from secondary and tertiary pediatric practices all over The Netherlands, using The Netherlands Pediatric Surveillance Unit system to identify cases. More than one third of these children were only seen by a general pediatrician.
Methods
The objective of this study was to describe the number, geographical distribution, age, gender, clinical and laboratory characteristics of Dutch children diagnosed with IgG-subclass deficiency and/or SPAD, reported to The Netherlands Pediatric Surveillance Unit (“Nederlands Signalerings Centrum voor Kindergeneeskunde” [NSCK]). The NSCK monthly asks all pediatricians in The Netherlands to report certain selected cases which they have seen during that past month in their hospital (in- as well as outpatient clinic). Between March 1, 2009, and November 1, 2011, all Dutch pediatricians were monthly asked to report all children they had seen with both newly and previously diagnosed IgG-subclass deficiency and/or SPAD (case definition in Table 1).
Demographic, clinical and laboratory characteristics were collected from all reported patients and stored in a database using Research Manager® software developed by Cloud9 Health Solutions. Patient data were encrypted and saved on a protected server; these data did not contain information that enabled identification of the identity of the patients. Separate informed consent was asked from parents and children (≥12 years of age) for annual update of the medical status. The Medical Ethical Committee Brabant approved the study.
For the interpretation of the Ig levels, age-matched reference values were used [13]. Diagnosis of SPAD was made using the criteria displayed in Table 1. In The Netherlands, pneumococcal antibodies are only determined in certain laboratories, that use their own reference values. Until 2009, only three serotypes were determined using ELISA (conform an international standard protocol, referred to as the WHO protocol [14]), including the strongly-intermediate immunogenic serotypes 3, 4 and 9 [15, 16]. Since 2009, pneumococcal antibodies are determined using the Luminex system [17, 18] (initially 10 serotypes; 7 serotypes since 2014). In our cohort, 10 patients were diagnosed using the old method (3 serotypes) and 11 using the new method (10 or 7 serotypes).
One-sample tests (Chi-Square, Kolmogorov-Smirnov) were carried out with SPSS, version 21, to test age and gender distributions.
Results
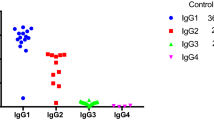
In total, 116 potential study participants were reported to the NSCK by pediatricians from 36 different hospitals. After analysis of the data quality and completeness, 49 children with confirmed IgG-subclass deficiency and/or SPAD were included in the study (Fig. 1). In this group, 45 children had ≥1 low IgG-subclass level and 11 children had SPAD (7 SPAD children had both IgG-subclass deficiency and SPAD, 1 child had SPAD and low-normal total IgG, and 3 children had only SPAD). Fourteen children had more than one IgG-subclass deficiency; IgG2 deficiency was most prevalent (Fig. 2). Five children also had IgA deficiency, 5 other children had slightly decreased IgG levels and 4 children had additional IgA deficiency as well as slightly decreased IgG levels. None of the children had additional IgM deficiency (Fig. 3).

Study flowchart

Combination of IgG-subclass deficiencies

Levels of Immunoglobulin isotypes. a IgG in g/l; b IgA in g/l; c IgM in g/l. Every dot represents a patient. The bold black line is the lower limit of normal according to age-matched reference values (ref de Vries E. Clin Exp Immunol 2012;167(1):108–19)
The median age of the 49 children was 5.6 years (mean age 7.1 years, range 2–18 years). Two-thirds of these children were male (33/49; 67 %, One-Sample Chi-Square test, p = 0.015). From ten years of age, only boys were left (Fig. 4). The age distribution for girls between 2 and 9 years-of-age is not uniform (One-Sample Kolmogorov-Smirnov test, p = .05). The same applies to boys (p = .039). This seems to suggest an age effect with a decreasing number of children in the age range between 2 and 9 years of age, but more data are needed to corroborate such an effect.

Distribution of age and gender
The majority (n = 34; 69 %) of these 49 children was reported from a secondary hospital with a pediatric immunologist in the staff (Fig. 1). The clinical problems the children encountered in the last year before entering the study are shown in Table 2. A striking ten percent of children (4 boys, 1 girl) already showed bronchiectasis. In 32 children (63 %) chronic use of medication was reported, mostly asthma medication (n = 20) or prophylactic antibiotics (n = 19). Four children received immunoglobulin substitution.
Follow-up data of 24 children were available with a median follow-up period of 40 months (range 12–65 months): 19 patients with IgG-subclass deficiency and 5 patients with IgG-subclass deficiency and SPAD. Nineteen children (79 %) were followed in a secondary hospital with a pediatric immunologist in the staff (Fig. 1). Six children (25 %) did not suffer from recurrent infections anymore, and in 3 of them the IgG-subclasses had reached normal values for age (the other 3 children were not re-tested). Seven children (29 %) showed a similar clinical picture as at baseline, their IgG-subclass deficiency and/or SPAD had persisted, but had not worsened either. Progression of the immunodeficiency was reported in 11 children (46 %), these were all boys: 1 boy developed decreased IgA levels, 3 boys developed decreased IgG levels, 3 boys developed decreased IgA and IgG levels, and 4 boys developed full-blown CVID. Eight children (33 %; all of them boys) received immunoglobulin substitution therapy at follow-up: 4 of them had initially presented with IgG-subclass deficiency combined with SPAD, 3 of them already had immunoglobulin substitution at the time of reporting.
Discussion
The human IgG-subclasses were first described in the 1960’s by Terry and Fahey [19] and the first report of patients with IgG-subclasses deficiency was published in 1974 [20]. Since then, several cases and cohorts of patients with IgG-subclass deficiency have been described (for example [21]). It was found that co-occurrence of IgA and IgG-subclass deficiency leads to more and more severe recurrent infections [22–24]. Also, children with IgG2-subclass deficiency showed decreased responses to immunization with polysaccharide antibodies [25].
We describe a cohort of 49 children with IgG-subclass deficiency and/or SPAD collected from secondary and tertiary hospitals all over The Netherlands using The Netherlands Pediatric Surveillance Unit system. The majority of the children (69 %) in our cohort were reported by four secondary hospitals with a pediatric immunologist in the staff. Our cohort contained only 1 child from a tertiary center. This means that most children with IgG-subclass deficiencies and/or SPAD are not referred to a tertiary center (at least in The Netherlands), probably because their disease is not considered to be very severe. It is unlikely that children with IgG-subclass deficiency and/or SPAD live in clusters around pediatric immunologists practising in secondary hospitals. Apparently, children with IgG-subclass deficiency and/or SPAD are often not recognized by general pediatricians. But is this important? Young children with ‘milder’ antibody deficiencies often recover. What they show is in fact a delayed maturation of the immune system, transient hypogammaglobulinemia of infancy, not an intrinsic immunodeficiency. This is seen in IgG-subclass deficiency and/or SPAD, but also in IgA deficiency, where 23 % of the patients diagnosed with IgA deficiency at the age of 4 years achieve serum IgA levels above 0.07 g/L during follow-up [26]. However, in some children the immunodeficiency persists or even develops into a more severe form, and recurrent pulmonary infections can lead to chronic pulmonary damage [27]. A study among 55 patients (27 children and 28 adults) with specific antibody deficiency or CVID showed that immunoglobulin class concentrations do not predict bronchiectasis, but percentages and absolute numbers of CD19+CD27+IgD− memory switched B cells do [28]. This was not determined in most patients in our cohort, but 5 children (10 %) in our cohort showed bronchiectasis at the time of inclusion. In three of them follow-up data were available; none had improved, and one had developed full-blown CVID. Also, significantly more boys (67 %) than girls were reported. After the age of 9, only boys were reported, and only boys (11/33 boys at baseline) showed progressive immunodeficiency during follow-up. This confirms the predominance of boys as was described by us before in a European cohort of children with hypogammaglobulinemia from the ESID online Registry (63 % male). Boys with hypogammaglobulinemia in the ESID online Registry were younger at diagnosis than girls and suffered more disease complications [2]. This is in contrast to the paper by Boyle et al. who did not find male sex to be a risk factor for developing SPAD [9]. Furthermore, van Winkle et al. showed that transient hypogammaglobulinemia resolved more quickly in male infants [29], but that cohort did not include older children. This gender difference is an important issue. Unidentified X-linked disease may play a role in boys with antibody deficiency; if so, this should influence treatment decisions, and it has consequences for potential recurrence in the family.
Twenty-five percent of the children with IgG-subclass deficiency and/or SPAD in our prospectively followed cohort recovered during follow-up. This is less than seen in other, retrospective studies of children with IgG-subclass deficiency (recovery 30–67 %) or unclassified hypogammaglobulinemia (recovery 49 %) [11, 30, 31]. However, follow-up data for our cohort were available in only half the children. This may have lead to an underrepresentation of recovered children during follow-up, because parents of children without persisting medical problems are probably less motivated to participate in a follow-up study.
The most prevalent IgG-subclass deficiency in our cohort was IgG2 deficiency: 24 children had isolated IgG2 deficiency, 5 children had IgG1 and IgG2 deficiency, 5 children had IgG2 and IgG3 deficiency and 3 children had IgG1, IgG2 and IgG3 deficiency. This is in contrast with other published cohorts: IgG3 deficiency was most prevalent in cohorts of Thai and Turkish children with IgG-subclass deficiency [11, 12, 30]. In the Turkish studies 78–90 %, and in the Thai study 86 % of the patients received prophylactic treatment to prevent infections, versus 47 % in our cohort, suggesting a more severe phenotype in these tertiary populations. Additional data in a broad, much larger cohort are needed to assess whether IgG3 deficiency is indeed more severe than IgG2 deficiency; the ESID online Registry would be a good tool for this.
Anti-polysaccharide antibodies were only examined in 21 children in our cohort (14 children from a secondary hospital with a pediatric immunologist in the staff). This means that 28 children did not undergo a complete analysis. The clinical relevance of selected IgG-subclass deficiency is controversial and determining the ability to produce specific antibodies is considered to be more important [32]. IgG subclasses can however easily be determined in daily practice with a single venipuncture during the patient’s visit to the clinic. The production of specific antibodies requires two venipunctures and vaccination. Also, the interpretation of the vaccine response is difficult; it requires sufficient experience, since reference values are lacking.
Our study has several limitations. We collected our cohort by using The Netherlands Pediatric Surveillance Unit system. Therefore, we depended on the pediatricians in the different hospitals for the quality of the reported data. We could not confirm the diagnosis of IgG-subclass deficiency and/or SPAD in 41 out of 90 (46 %) reported children. This was due to missing data in 35 children. In 6 children, all laboratory values were available but normal when using age-matched reference values. Possibly, their pediatricians had used different, non-age-specific, reference values. This is an important issue for educational improvement.
Finally, IgG subclass deficiency can also be found in asymptomatic patients. Analysis of IgG subclasses among 8015 adult blood donors demonstrated that there were more individuals with low IgG2 concentrations than predicted by the log-normal distribution [33]. Also, 11 out of a cohort of 575 healthy children showed IgG2 concentrations >2SD below the mean for age. These asymptomatic children with subnormal IgG2 levels showed normal antibody responses to immunization with Haemophilus influenza type B polysaccharide antigens [34]. However, the children in our cohort were analyzed by their pediatrician because of their clinical presentation, and therefore were not asymptomatic.
Conclusion
This is the first description of a Western-European cohort of children with IgG-subclass deficiency and/or SPAD collected by pediatricians from secondary as well as tertiary hospitals; it was collected in The Netherlands. We show that IgG-subclass deficiency and/or SPAD are not always benign diseases: 10 % of the children already showed bronchiectasis. There was an overrepresentation of boys and only boys showed immunological decline during follow-up. So, unidentified X-linked disease may play a role in boys with antibody deficiency. Most IgG-subclass deficiencies and/or SPAD were reported and managed in secondary hospitals with a pediatric immunologist in the staff, which raises the question if these patients are missed in general pediatric secondary hospitals. If we want to identify more patients, probably the awareness of these diseases among general pediatricians should increase.
Abbreviations
- CVID:
-
Common variable immunodeficiency disorders
- ENT:
-
Ear-Nose-Throat
- Ig:
-
Immunoglobulin
- NSCK:
-
Netherlands Pediatric Surveillance Unit (“Nederlands Signalerings Centrum voor Kindergeneeskunde”)
- SPAD:
-
Specific Polysaccharide Antibody Deficiency
References
Gathmann B, Grimbacher B, Beaute J, Dudoit Y, Mahlaoui N, Fischer A, et al. The European internet-based patient and research database for primary immunodeficiencies: results 2006-2008. Clin Exp Immunol. 2009;157(Suppl 1):3–11.
Schatorje EJ, Gathmann B, van Hout RW, de Vries E. The PedPAD study: boys predominate in the hypogammaglobulinaemia registry of the ESID online database. Clin Exp Immunol. 2014;176(3):387–93.
Stiehm RE. The four most common pediatric immunodeficiencies. Adv Exp Med Biol. 2007;601:15–26.
www.esid.org - ESID registry – working definitions for clinical diagnosis of PID.
Sanders LA, Rijkers GT, Tenbergen-Meekes AM, Voorhorst-Ogink MM, Zegers BJ. Immunoglobulin isotype-specific antibody responses to pneumococcal polysaccharide vaccine in patients with recurrent bacterial respiratory tract infections. Pediatr Res. 1995;37(6):812–9.
Fleming DW, Cochi SL, Hightower AW, Broome CV. Childhood upper respiratory tract infections: to what degree is incidence affected by day-care attendance? Pediatrics. 1987;79(1):55–60.
Glocker E, Ehl S, Grimbacher B. Common variable immunodeficiency in children. Curr Opin Pediatr. 2007;19(6):685–92.
Monto AS, Napier JA, Metzner HL. The Tecumseh study of respiratory illness. I. Plan of study and observations on syndromes of acute respiratory disease. Am J Epidemiol. 1971;94(3):269–79.
Boyle RJ, Le C, Balloch A, Tang ML. The clinical syndrome of specific antibody deficiency in children. Clin Exp Immunol. 2006;146(3):486–92.
Ruuskanen O, Nurkka A, Helminen M, Viljanen MK, Kayhty H, Kainulainen L. Specific antibody deficiency in children with recurrent respiratory infections: a controlled study with follow-up. Clin Exp Immunol. 2012;172(2):238–44.
Karaca NE, Karadeniz C, Aksu G, Kutukculer N. Clinical and laboratory evaluation of periodically monitored Turkish children with IgG subclass deficiencies. Asian Pac J Allergy Immunol. 2009;27(1):43–8.
Visitsunthorn N, Hengcrawit W, Jirapongsananuruk O, Luangwedchakam V. Immunoglobulin G (IgG) subclass deficiency in Thai children. Asian Pac J Allergy Immunol. 2011;29(4):332–7.
Protocol for Diagnosing Primary Immunodeficiency. (de Vries E Patient-centred screening for primary immunodeficiency, a multi-stage diagnostic protocol designed for non-immunologists: 2011 update Clin Exp Immunol 2012; 167(1):108–19). [Adapted from: Vademecum diagnostisch onderzoek Sanquin, 2008, pp 90. Clinical chemistry 1982, 28:127. European Journal of Clinical Chemistry and Clinical Biochemistry 1996; 34–517.].
Elberse KE, Tcherniaeva I, Berbers GA, Schouls LM. Optimization and application of a multiplex bead-based assay to quantify serotype-specific IgG against Streptococcus pneumoniae polysaccharides: response to the booster vaccine after immunization with the pneumococcal 7-valent conjugate vaccine. Clin Vaccine Immunol. 2010;17(4):674–82.
Go ES, Ballas ZK. Anti-pneumococcal antibody response in normal subjects: a meta-analysis. J Allergy Clin Immunol. 1996;98(1):205–15.
Sanders LA, Rijkers GT, Kuis W, Tenbergen-Meekes AJ, de Graeff-Meeder BR, Hiemstra I, et al. Defective antipneumococcal polysaccharide antibody response in children with recurrent respiratory tract infections. J Allergy Clin Immunol. 1993;91(1 Pt 1):110–9.
Janssen WJ, Bloem AC, Vellekoop P, Driessen GJ, Boes M, van Montfrans JM. Measurement of pneumococcal polysaccharide vaccine responses for immunodeficiency diagnostics: combined IgG responses compared to serotype specific IgG responses. J Clin Immunol. 2014;34(1):3–6.
Rodenburg GD, Sanders EA, van Gils EJ, Veenhoven RH, Zborowski T, van den Dobbelsteen GP, et al. Salivary immune responses to the 7-valent pneumococcal conjugate vaccine in the first 2 years of life. PLoS ONE. 2012;7(10):e46916.
Terry WD, Fahey JL. Subclasses of human gamma-2-globulin based on differences in the heavy polypeptide chains. Science. 1964;146(3642):400–1.
Oxelius VA. Chronic infections in a family with hereditary deficiency of IgG2 and IgG4. Clin Exp Immunol. 1974;17(1):19–27.
Stanley PJ, Corbo G, Cole PJ. Serum IgG subclasses in chronic and recurrent respiratory infections. Clin Exp Immunol. 1984;58(3):703–8.
Oxelius VA, Laurell AB, Lindquist B, Golebiowska H, Axelsson U, Bjorkander J, et al. IgG subclasses in selective IgA deficiency: importance of IgG2-IgA deficiency. N Engl J Med. 1981;304(24):1476–7.
Morell A, Muehlheim E, Schaad U, Skvaril F, Rossi E. Susceptibility to infections in children with selective IgA- and IgA-IgG subclass deficiency. Eur J Pediatr. 1986;145(3):199–203.
Beard LJ, Ferrante A, Oxelius VA, Maxwell GM. IgG subclass deficiency in children with IgA deficiency presenting with recurrent or severe respiratory infections. Pediatr Res. 1986;20(10):937–42.
Umetsu DT, Ambrosino DM, Quinti I, Siber GR, Geha RS. Recurrent sinopulmonary infection and impaired antibody response to bacterial capsular polysaccharide antigen in children with selective IgG-subclass deficiency. N Engl J Med. 1985;313(20):1247–51.
Lim CK, Dahle C, Elvin K, Andersson BA, Rönnelid J, Melén E, Bergström A, Truedsson L, Hammarström L. Reversal of Immunoglobulin A Deficiency in Children. J Clin Immunol. 2014. doi:10.1007/s10875-014-0112-6.
Ozkan H, Atlihan F, Genel F, Targan S, Gunvar T. IgA and/or IgG subclass deficiency in children with recurrent respiratory infections and its relationship with chronic pulmonary damage. J Investig Allergol Clin Immunol. 2005;15(1):69–74.
Alachkar H, Taubenheim N, Haeney MR, Durandy A, Arkwright PD. Memory switched B cell percentage and not serum immunoglobulin concentration is associated with clinical complications in children and adults with specific antibody deficiency and common variable immunodeficiency. Clin Immunol. 2006;120(3):310–8.
Van Winkle RC, Hauck WW, McGeady SJ. Phenotypic parameters predict time to normalization in infants with hypogammaglobulinemia. J Clin Immunol. 2013;33(8):1336–40.
Kutukculer N, Karaca NE, Demircioglu O, Aksu G. Increases in serum immunoglobulins to age-related normal levels in children with IgA and/or IgG subclass deficiency. Pediatr Allergy Immunol. 2007;18(2):167–73.
Kutukculer N, Gulez N. The outcome of patients with unclassified hypogammaglobulinemia in early childhood. Pediatr Allergy Immunol. 2009;20(7):693–8.
Buckley RH. Immunoglobulin G subclass deficiency: fact or fancy? Curr Allergy Asthma Rep 2002; 2(5):356–360.
Madassery JV, Kwon OH, Lee SY, Nahm MH. IgG2 subclass deficiency: IgG subclass assays and IgG2 concentrations among 8015 blood donors. Clin Chem. 1988;34(7):1407–13.
Shackelford PG, Granoff DM, Madassery JV, Scott MG, Nahm MH. Clinical and immunologic characteristics of healthy children with subnormal serum concentrations of IgG2. Pediatr Res. 1990;27(1):16–21.
Acknowledgments
We would like to thank the following pediatricians for reporting patients: E.J.A. Gerritsen (Admiraal de Ruyter Ziekenhuis), T.C.J. Sas (Albert Schweitzer Ziekenhuis), A.A.P.H. Vaessen-Verberne (Amphia Ziekenhuis), M.L. Brouwer (Canisius Wilhelmina Ziekenhuis), C.J. Miedema (Catharina Ziekenhuis), J. van der Deure (Deventer Ziekenhuis), G.J.A. Driessen (Erasmus MC Sophia), A. Dings-Lammertink (Gelre Ziekenhuizen), I. Heuts-van de Kragt (Ikazia Ziekenhuis), C.R.W. Korver (Kennemergasthuis), R.G.M. Bredius (Leids Universitair Medisch Centrum), A.C. Engelberts (Maaslandziekenhuis), W.P. Vogt (MC Groep), G. Brinkhorst (Medisch Centrum Alkmaar), N. de Vries/T.E. Faber/E. van Pinxteren-Nagler (Medisch Centrum Leeuwarden), E. van den Berg (Medisch Spectrum Twente), A. van Kempen (Onze Lieve Vrouwe Gasthuis), A. Warris (Radboud UMC), G. Meppelink/S. Nowak (Refaja Ziekenhuis), A.W. Colijn/G. Nolles/A.L.T. van Overbeek-van Gils (Scheper Ziekenhuis), H.H. Kiezebrink-Lindenhovius (Spaarne Ziekenhuis), M. van Dongen-van Baal (St. Antonius Ziekenhuis), J.F.M. Bruinenberg (St. Elisabeth Ziekenhuis), J. Raaijmakers (St. Laurentius Ziekenhuis), S. Kapteijns-van Kordelaar (St. Jansgasthuis), A. Kaldi (Talma Sionsbergziekenhuis), B. van Ewijk (Tergooi Ziekenhuizen), J.A. Gerrits-Kuiper (van Weel Bethesda Ziekenhuis), C.A.M. van Wijk (Vlietland Ziekenhuis), S. Broekhuizen-den Haan (Wilhemina Ziekenhuis), pediatricians from Ziekenhuis Amstelland, G.H. van Leeuwen (Ziekenhuis Bethesda), K.A. Zwager-Ankone (Ziekenhuis Coevorden-Hardenberg), A.J. Janse (Ziekenhuis Gelderse Vallei), W. Corijn (Ziekenhuisgroep Zeeuws-Vlaanderen).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
We received an unrestricted research grant from Sanquin for this study. Also the Jeroen Bosch Hospital funded this study.
Conflict of Interest
Prof. de Vries received unrestricted research grants from Sanquin and CSL Behring. The other authors have no potential conflicts of interest to report.
Rights and permissions
About this article

Cite this article
Schatorjé, E.J.H., de Jong, E., van Hout, R.W.N.M. et al. The Challenge of Immunoglobulin-G Subclass Deficiency and Specific Polysaccharide Antibody Deficiency – a Dutch Pediatric Cohort Study. J Clin Immunol 36, 141–148 (2016). https://doi.org/10.1007/s10875-016-0236-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10875-016-0236-y