
Abstract
This study examined the relationship between communication avoidance of cancer-related topics with psychological distress, and the mediating role of coping strategies, in women with breast cancer. Women diagnosed with breast cancer (N = 338) completed an online survey including measures of self- and perceived-partner communication avoidance, psychological distress (depression, anxiety and stress), and coping strategies. Linear regression analyses indicated that women’s and perceived-partner’s communication avoidance was associated with anxiety, depression, and stress in the cancer-affected women. Bootstrapping analyses showed significant mediation effects of self- and perceived-partner communication avoidance on all distress outcomes through greater disengagement coping, and on anxiety through lower engagement coping. Emotionally valenced topics (i.e., disease progression and sexuality) were most avoided and practical issues were least avoided. Enhancing couple communication about cancer and women’s adaptive coping skills (i.e., discourage use of disengagement coping strategies and promote use of engagement coping strategies) may be important targets for psychosocial intervention.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Breast cancer is a heterogeneous disease with a highly variable clinical course (Stanton & Revenson, 2011) presenting affected women with myriad physical and psychosocial stressors (Goldsmith et al., 2008; Manne & Badr, 2008). Surgery interventions are often invasive and painful and can result in bodily changes that compromise a woman’s self-esteem and identity and interfere with her sexual functioning (Bartula & Sherman, 2013; Przezdziecki et al., 2013). Established adjuvant treatments such as radiotherapy, chemotherapy, and hormone therapy are often accompanied by long-lasting side effects, such as fatigue, pain, and nausea (Gho et al., 2013). These treatments can significantly impair functioning and disrupt a woman’s social and family roles, challenging her autonomy (Hilton et al., 2000). Intrusive thoughts about disease recurrence or progression are also common, given the considerable uncertainty regarding treatment efficacy and cancer prognosis (Stanton & Revenson, 2011). Not surprisingly, a substantial proportion of women diagnosed with breast cancer experience elevated psychological distress in the form of anxiety, depression, and stress many years after diagnosis and treatment (Bower, 2008). A recent meta-analysis of 43 cohort studies involving over 11,000 breast cancer patients, found the prevalence of clinical depression was 11 % on the basis of diagnostic interviews, and 20 % as measured by self-report interviews (Krebber et al., 2014). Similarly, the prevalence of anxiety disorders among long-term cancer survivors generally has been estimated at 17.9 % (Mitchell et al., 2013).
Research focused on interpersonal dynamics points to the importance of couple communication in women’s psychological adjustment to breast cancer (for review, see Goldsmith et al., 2008). Women dealing with this serious illness often need to talk about their cancer-related thoughts, feelings, and concerns with close others to navigate their illness experience (Lepore & Revenson, 2007; Stanton & Revenson, 2011). Given that spouses are often identified by women with breast cancer as the most important source of social support (Manne et al., 2003), it is not surprising that many women desire to talk with their partners about different aspects of their illness (Mallinger et al., 2006; Manne et al., 2005).
Sparse but emerging literature in this area (Donovan-Kicken & Caughlin, 2011; Goldsmith & Miller, 2013; Goldsmith et al., 2008; Manne & Badr, 2008; Manne et al., 2006) has identified key communication factors associated with women’s psychological distress. Mutually constructive communication (i.e., open discussion of cancer-related topics and expression of feelings) has been associated with greater relationship satisfaction and less anxiety and depression symptoms for both the woman and her partner (Manne et al., 2006), whereas avoidant communication between spouses has been associated with higher levels of anxiety and depression (e.g., Donovan-Kicken & Caughlin, 2011; Figueiredo et al., 2004; Lepore & Revenson, 2007; Manne & Badr, 2008; Manne et al., 2006) and lower relationship satisfaction (Donovan-Kicken & Caughlin, 2010) in women with breast cancer. Research, however, suggests some couples find it difficult to communicate openly and sensitively about breast cancer-related concerns (Goldsmith & Miller, 2013; Goldsmith et al., 2008) for various reasons, such as to protect oneself or one’s partner from the discomfort of discussing difficult cancer-related topics, prevent futile or unproductive discussions, and to maintain normality and optimism (Goldsmith et al., 2008). Some women also avoid cancer-related discussions with their spouses due to experiencing unsupportive partner responses (Manne et al., 2005) that may be overt and coercive (e.g., spouses criticising how a woman is coping with her breast cancer or directly undermining the severity of her illness), or diffused and subtle in nature, such as changing the topic when a woman starts talking about a cancer-related concern (Lepore & Revenson, 2007).
Prior research (e.g., Lewis et al., 2008; Weihs et al., 2008) has tended to use global abstract evaluative questions, such as “have you been able to talk about your feelings and problems with your partner in the last 2 weeks?” or “do you frequently discuss your illness with your spouse?”, to assess communication between couples. These questions lack specificity and sensitivity and have the disadvantage of eliciting responses more reflective of a woman’s general relationship satisfaction with her partner than actual enacted communication behaviours (Goldsmith & Miller, 2013). Some studies have found conflicting responses from participants who report using open communication with their partners in response to global evaluative questions, but then report engaging in high unsupportive and avoidant responses when discussing specific cancer-related topics (e.g., Caughlin et al., 2011; Goldsmith et al., 2008). Furthermore, most previous research has not considered that communication may vary across cancer topics and between partners (Goldsmith & Miller, 2013).
Another limitation of past work is the lack of empirical research examining potential mechanisms that may explain the association between avoidant spousal communication and women’s psychological distress (Donovan-Kicken & Caughlin, 2011; Manne et al., 2005, 2010). A useful theoretical framework for understanding this relationship is the transactional stress and coping paradigm which proposes that an individual’s adaptation to a stressor will vary according to how one cognitively and behaviourally manages the demands posed by the stressor (Folkman & Moskowitz, 2004). Coping strategies can be organised into two broad categories: engagement or disengagement coping strategies (Kvillemo & Bränström, 2014). Engagement coping strategies are defined as active, direct, goal-oriented responses to either reduce the impact of a stressor itself or influence one’s emotional responses or efforts to adapt to the stressor (Tobin et al., 1989). Engagement coping strategies include problem solving, acceptance, seeking support, planning, and positive reframing. Disengagement coping strategies, in contrast, are coping efforts that focus attention away from the stressor or one’s thoughts and feelings about the stressor, and includes emotional, cognitive, and behavioural avoidance strategies such as denial, substance use, and self-blame. Use of engagement coping strategies by women with breast cancer has been associated with lower psychological distress, whereas use of disengagement coping strategies has been associated with higher levels of psychological distress (Donovan-Kicken & Caughlin, 2011; Kim et al., 2010).
Avoiding talk about cancer between spouses may increase a woman’s psychological distress by impeding her coping efforts (Donovan-Kicken & Caughlin, 2011). A woman who avoids sharing cancer-related thoughts, feelings, and concerns with her partner may have fewer opportunities to receive validation and gain helpful perspectives to help her navigate her illness experience (Lepore & Revenson, 2007; Munro et al., 2014; Porter et al., 2005); thereby increasing her propensity to adopt disengagement coping strategies, such as denial, self-blame and behavioural disengagement, exacerbating her psychological distress (Donovan-Kicken & Caughlin, 2011; Lepore & Revenson, 2007). Commonly adopted functional coping behaviours, such as problem-solving, and seeking instrumental and emotional support, are also fundamentally communicative and may offer little benefit or may even be detrimental to the woman when they are enacted without discussion of cancer-related content (Donovan-Kicken & Caughlin, 2011).
Most research in this area has treated coping and communication processes as independent predictors of psychological distress (e.g., Scott et al., 2004) without any consideration for potential mediating effects of coping on the communication–distress relationship. Only one study to date (based in the US, N = 140) has explored possible mediating mechanisms in the breast cancer context, concluding that avoidant communication by cancer-affected women can have significant indirect effects on their psychological distress through greater use of self-blame and less use of emotional support (Donovan-Kicken & Caughlin, 2011). That is, the more a woman avoids talking about cancer-related matters with her spouse, the more likely she is to blame herself for her ill health and the less likely she is to reach out to others for emotional support. Both self-blame and lower use of emotional support were associated with greater psychological distress.
The present study aimed to extend this work by examining in the breast cancer context the association of patient-reported communication avoidance of specific cancer-related topics, as well as perceived partner avoidance of these topics, with women’s coping and psychological distress. Partner communication is important as couple communication is a transactional process and both the woman and her partner’s responses can reciprocally influence each other’s interactions (Lepore & Revenson, 2007). We hypothesised that communication avoidance by the cancer-affected woman and her partner would be associated with her greater depression, anxiety and stress. In addition, it was predicted that both the woman’s and her perceived partner’s communication avoidance would be associated with her psychological outcomes, with effects mediated by her greater use of disengagement coping strategies and less use of engagement strategies. A further aim was to evaluate and characterise the degree of communication avoidance of specific cancer-related topics by the cancer-affected women and their spouses.
Methods
Sample and procedures
Individuals eligible for study participation were: (1) female; (2) over 18 years of age; (3) previously diagnosed with Ductal Carcinoma in Situ (DCIS), or primary stage I, II or III breast cancer within the past 5 years; (4) in a committed relationship with a partner before the breast cancer diagnosis; (5) currently in a relationship and/or cohabiting with the same partner; and, (6) fluent in English. Participants completed the study questionnaire online. Women previously diagnosed with breast cancer or DCIS were approached for study participation through an Australian community-based breast cancer consumer organisation, the Breast Cancer Network of Australia (BCNA). An e-mail invitation was sent by a contact person within the BCNA to 885 members who had previously agreed to receive notifications about research studies. It was the responsibility of the women who received the e-mail to determine their eligibility for the study. A total of 338 women agreed to participate. Following online consent, participants anonymously completed the questionnaire which took <20 min to complete. The conduct of this research was approved by the Macquarie University Human Research Ethics Committee.
Measures
Communication avoidance
Communication avoidance was assessed using a seven-subscale measure reflecting different cancer-related topics (Donovan-Kicken & Caughlin, 2010) that have been identified as important concerns for women with breast cancer (Figueiredo et al., 2004; Goldsmith et al., 2008). The measure was validated on a sample of breast cancer patients for clarity and completeness (Donovan-Kicken, 2008; Donovan-Kicken & Caughlin, 2011). The Death subscale focuses on end of life matters, such as possibility of disease recurrence and future plans (eight items; e.g., “the possibility of the cancer coming back after treatment”; α = .93 for women and α = .94 for partners). Treatment includes items about aspects of medical treatments (five items; e.g., “side effects from medical treatments”; α = .91 for women and α = .93 for partners). Sexuality addresses intimacy and body image concerns (four items; e.g., “physical intimacy”; α = .93 for women and α = .95 for partners). Being a burden includes items about added stressors related to finances, household contribution, and care-taking responsibilities (eight items, e.g., “ability to do household chores”; α = .90 for women and α = .93 for partners). Feeling includes items about expression of concerns and fears related to breast cancer (ten items; e.g., “aspects of cancer and treatment that makes me nervous”; α = .94 for women and α = .96 for partners). Relating includes questions about relationship satisfaction and communication (five items, e.g., “how well we are getting along”; α = .91 for women and α = .95 for partners) and Healthcare addresses experiences with health care providers (four items, e.g., “interactions with my physicians”; α = .96 for women and α = .98 for partners). The women rated on a five-point Likert-type scale (1 = “strongly disagree” to 5 = “strongly agree”) the extent to which they generally avoided discussing various cancer-related topics with their spouse (e.g., “I avoid talking to my partner about plans for the future”), and the extent to which they perceived their partners avoided discussing cancer-related topics with them (e.g., “my partner avoids talking to me about plans for the future”). Item scores were aggregated and averaged to create topic subscale scores. Composite measures of general self- and perceived-partner communication avoidance were created by averaging the respective subscale scores (Goldsmith & Miller, 2013). Scores for the composite measure can range from 1 to 5, with higher scores reflecting greater communication avoidance about cancer. Prior research indicates sufficient evidence for the reliability of this measure between parent and child, romantic and friendship dyads (Caughlin & Afifi, 2004; Donovan-Kicken & Caughlin, 2010, 2011). In the present study, internal consistency for these scales was .98 (self) and .98 (partner), respectively.
Psychological distress
The 21-item short form of the Depression, Anxiety and Stress Scale self-report questionnaire (DASS-21; Lovibond & Lovibond, 1996) was used to assess psychological distress over the previous week. Each scale was measured with items using a four-point Likert-type scale, ranging from 0 (“did not apply to me at all”) to 3 (“applied to me very much, or most of the time”). The DASS has demonstrated good psychometric properties among cancer (α = .98; Beatty et al., 2010) and community populations (Crawford & Henry, 2003). In the present study, internal consistency was high for all subscales (α = .88 Depression; α = .81 Anxiety; α = .89 Stress).
Coping
The Brief COPE (Carver, 1997) was used to assess women’s engagement in coping styles to manage their breast cancer. Cognitive and behavioural coping style was assessed by 28 items reflecting coping styles of: self-distraction, active coping, denial, substance use, emotional support, instrumental support, behavioural disengagement, venting, positive reframing, planning, humor, acceptance, religion, and self-blame. Each coping response was assessed with two items. Respondents were instructed to rate the general frequency of their engagement of these 14 coping styles in relation to their breast cancer diagnosis, using a four-point Likert-type scale, ranging from “I haven’t been doing this at all” (1) to “I’ve been doing this a lot” (4). Subscale scores were created from mean scores of the items contained within each subscale. There is evidence that the factor structure of coping measures, such as the Brief COPE, differs somewhat by the population under investigation (Kvillemo & Bränström, 2014). Moreover, consensus on the higher-order categorisation of coping subscales has not yet been achieved due to the heterogeneous nature of the existing breast cancer-related research (e.g., Silva et al., 2012; Yang et al., 2008). To address these difficulties as well as the large number of related, but distinct, subscales of the Brief COPE (Kvillemo & Bränström, 2014), exploratory factor analysis (EFA) was conducted to identify the underlying constructs of the 14 coping strategies using the maximum likelihood method. The EFA resulted in a Kaiser–Meyer–Olkin measure of sample adequacy of .76 and a Bartlett’s test of sphericity being significant at .001. EFA using oblimin rotation was then conducted to achieve a simpler structure with greater interpretability. Consistent with previous studies (Kershaw et al., 2004; Yang et al., 2008), a two-factor structure was supported when examined for interpretability, parsimony, magnitude of loadings and an adequate model of fit (root mean square error of approximation = .06). One factor, labelled “Engagement coping” included 14 items (α = .84) assessing seven coping strategies: seeking emotional support, instrumental support, planning, active coping, positive reframing, acceptance, and use of religion. The second factor, labelled “Disengagement coping” (α = .77) included four strategies: self-blame, substance use, behavioural disengagement, and denial. Factor scores were created by averaging the respective subscale scores. Two coping strategies (humor and venting) did not load adequately (<.30) into either of the factors and were subsequently analysed as separate coping strategy subscales. One coping strategy, self-distraction had high cross-loadings on both factors and was subsequently removed from further analyses.
Physical functioning
Physical symptom distress, a documented predictor of psychological distress among women with breast cancer (Northouse et al., 2002), was assessed using the seven-item Physical Well-Being Subscale of Functional Assessment of Cancer Therapy self-report questionnaire (FACT-B; Cella et al., 1993). The scale measured physical symptomatology specific to the breast cancer experience over the previous week. All items were rated using a 5-point Likert-type scale, ranging from 0 (“not at all”) to 4 (“very much”). Item scores were averaged with higher subscale scores indicating greater physical functional wellbeing. Internal consistency for the scale was high (α = .82).
Demographic characteristics
Information was gathered on the women’s demographic and disease-related characteristics: age, country of birth, educational level, marital status, relationship length, time since her primary breast cancer diagnosis, and information about cancer treatments that she had received.
Statistical analyses
t Tests, correlation and one-way ANOVA analyses were performed using SPSS (version 21; IBM Corp., 2012) to examine the relationships between patient and partner communication avoidance (overall and topic subscale) and demographic and disease variables. To understand the role of engagement and disengagement coping strategies between topic avoidance and psychological distress, separate mediation analyses were conducted. Pearson’s correlations were initially undertaken to identify any socio-demographic, disease, and treatment variables that were significantly associated with psychological distress variables. All subsequent analyses adjusted for any such covariates. To test the significance of the indirect effects, bootstrapping was performed using the INDIRECT SPSS macro (Preacher & Hayes, 2008). This approach is regarded as being more robust than the more well-known tests of indirect effects in terms of power and Type I error rates (MacKinnon et al., 2002; Preacher & Hayes, 2008), particularly for small and moderate sample sizes (MacKinnon et al., 2004). In this study, significance of indirect effect was indicated when the 95 % confidence interval (CI) derived from 5000 bootstrap distributions did not include zero. A paired-samples t test was also conducted to compare use of engagement coping and disengagement coping by the cancer-affected women.
Results
Sample description
Participants were 338 Australian women who had previously been diagnosed with breast cancer. Sample characteristics are displayed in Table 1. The mean age of the women was 53.5 years (SD = 9.22, range 28 to 81). The women on average were diagnosed with breast cancer 35.9 months prior to study entry (SD = 24.24, range = 6–213), and reported having been in a relationship for 25.9 years (SD = 13.12, range 1.8–63 years). Mean depression, anxiety, and stress scores for the overall sample were within the normal ranges.
Communication avoidance
Bivariate associations between the main variables of interest are displayed in Table 2. Relationship length was negatively correlated with women’s level of communication avoidance scores (r = −.13, p < .05). Physical wellbeing was negatively correlated with both women’s (r = −.20, p < .05) and perceived partner avoidance communication scores (r = −.17, p < .05). The correlation coefficient between self- and perceived-partner communication avoidance was r = .83. Paired samples t tests were used to examine differences in levels of self- and perceived-partner communication avoidance. Results of these analyses indicated that women reported significantly higher levels of perceived partner communication avoidance than their own communication avoidance with their spouses; t(337) = 8.37, p < .0001.
One-way ANOVAs were conducted to examine whether there were any differences in overall and subscale patient and partner communication avoidance by disease stage. No significant differences were found (p’s > .44). Independent t tests were also used to examine whether cancer treatment (women who have completed their cancer treatment vs. women who have yet to commence their treatment) influenced patient and partner communication avoidance (overall and subscale) scores. None of these analyses were significant (all p’s > .17).
Communication avoidance about specific cancer-related topics
Bivariate associations between communication avoidance of specific cancer topic and coping and distress outcomes are shown in Table 3. Overall, cancer-affected women reported moderately low levels of communication avoidance with their spouses (M = 2.31, SD = .84, range 1–5). Average ratings on each topic subscale for the women ranged from 1.84 to 2.65. The highest rated subscales were “expression of cancer-related feelings” which had an average rating of 2.65, followed by “concerns about sexuality” (M = 2.62) and “concerns about disease progression and death” (M = 2.50). The lowest rated subscale was “experiences with health care providers” which had an average rating of 1.84, followed by “cancer treatment” (M = 1.95). The average score for overall partner communication avoidance was 2.55 (SD = .95, range 1–5). Average ratings on each subscale ranged from 2.05 to 3.10. The highest rated subscales were “concerns about disease progress/death” which had an average rating of 3.10, followed by “concerns about sexuality” (M = 2.73), and “expression of cancer-related feelings” (M = 2.67). The lowest rated subscale was “experiences with health care providers”, which was rated 2.05, followed by “cancer treatment” (M = 2.27). Correlations of communication avoidance subscales with the coping and distress outcomes indicated that all topic subscales showed similar patterns of strength and direction with each of the indices of coping and psychological distress outcomes, and were generally small to moderate in size (see Table 3).
Mediation analyses of coping
Women’s communication avoidance and perceived partner communication avoidance were positively correlated with all measures of psychological distress and disengagement coping, and negatively correlated with engagement coping. Disengagement coping was positively correlated with all three distress measures while engagement coping was negatively correlated with only depression (Table 2). Of the potential covariates examined (age, education, time since diagnosis, stage of breast cancer, level of physical wellbeing and current receipt of chemotherapy or radiation therapy), only physical wellbeing significantly correlated with all three distress outcomes and was included in subsequent mediation analyses. Women reported using engagement coping (M = 2.69, SD = .56) significantly more than disengagement coping (M = 1.38, SD = .43); t(337) = 33.62, p < .001.
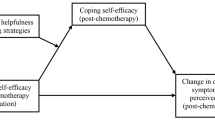
The model for the regression analysis is illustrated in Fig. 1. Table 4 provides results of the bootstrapping analyses. Disengagement coping was a significant mediator of self- and perceived-partner communication avoidance on all psychological distress variables, as the bias-corrected bootstrap confidence interval (BCI) for the indirect effects of disengagement coping based on 5000 bootstrap samples were all above zero and positive. Engagement coping, on the other hand, met criteria as a mediator between self- and partner-communication avoidance on depression only (95 % BCI .092–.577; 95 % BCI .066–.449, respectively). In view of the significant associations between physical symptoms and the communication, distress and coping variables, we tested whether the magnitude and direction of any of these indirect effects were moderated by women’s level of physical wellbeing, using a moderated mediation SPSS macro developed by Preacher et al. (2007). Physical symptoms were not found to moderate any of the relationships between communication avoidance and distress outcomes.

Graphic representation of the mediation model
Discussion
Current understanding of how communication between spouses may influence the psychological distress of individuals with chronic illness is limited. The present study assessed the associations of patient-reported avoidance of specific cancer-related topics, reports of partner avoidance of these topics, and coping and psychological distress among breast cancer survivors.
Utilising a multi-topic measure of communication avoidance (Goldsmith & Miller, 2013), the results indicated moderately low levels of communication avoidance between spouses about cancer overall, but considerable variability in how much women with breast cancer and their spouses avoided discussing cancer-related topics with one another. The women reported significantly higher levels of perceived partner communication avoidance than their own communication avoidance across all cancer topics, raising the possibility that spouses may be less comfortable sharing their cancer-related concerns than the women themselves. The topics most avoided by the cancer-affected women with their partners related to their feelings about their breast cancer, sexuality concerns, and fears about disease progression and death. The topics least avoided by the women pertained to their experiences with health care professionals and concerns about cancer treatment. This pattern of results is not surprising given the considerable taboo attached to topics of death and sex in Western society (Goldsmith et al., 2008). These findings are consistent with previous studies of women with breast cancer (Donovan-Kicken & Caughlin, 2010), gynaecological cancer (Manne et al., 2014), and men with localized prostate cancer (Manne et al., 2011) that have found greater sharing of concerns related to more practical issues such as the patient’s cancer treatment and relationship with health professionals, than for emotionally valenced topics. The topics the spouses were reported to avoid the most followed the same trend to the communication avoidance of cancer-related topics endorsed by the cancer-affected women with their partners. Previous research has found that oncology health professionals also tend to avoid discussing end-of-life and sexuality concerns with cancer-affected women for reasons such as discomfort with the topics and general concerns of boundary crossing (Hordern & Street, 2007). Given the findings of the present study, a greater awareness by oncology health professionals of the various cancer concerns that couples coping with breast cancer commonly avoid may assist these professionals to more sensitively recognise and address couples’ communication needs in clinical practice.
Consistent with previous research of community-based breast cancer populations (Przezdziecki et al., 2013; Soo & Sherman, 2015), the present study confirmed the presence of depression, anxiety, and stress in some breast cancer patients, with at least moderate levels of depressive symptoms reported in 16.1 % of participants, anxiety symptoms in 14.2 % and stress symptoms in 11.5 %. A diversity of factors can contribute to distress among women with breast cancer (Stanton & Revenson, 2011); however, in the present study, greater self- and perceived-partner communication avoidance about cancer topics were associated with poorer mental health outcomes (anxiety, depression, and stress) in the cancer-affected women, consistent with similar results observed in prior research (Donovan-Kicken & Caughlin, 2011; Goldsmith et al., 2008; Lepore & Revenson, 2007; Manne et al., 2006). The study findings are also consistent with the transactional stress and coping paradigm (Folkman & Moskowitz, 2004) and provide support for the view (Donovan-Kicken & Caughlin, 2011) that avoiding talk about cancer may influence the woman’s emotional distress by impeding her coping ability. The woman’s and her perceived partner’s communication avoidance were both associated with her greater maladaptive disengagement coping and lower adaptive engagement coping. Lower engagement coping and higher disengagement coping were also both associated with the woman’s poorer psychological outcomes.
The more a couple avoids talking about cancer-related topics, the less opportunities a woman will have to receive validation and gain helpful perspectives to help her navigate her illness experience (Lepore & Revenson, 2007; Munro et al., 2014; Porter et al., 2005); thereby increasing her propensity to adopt disengagement coping strategies, such as denial and behavioural disengagement, to deal with her cancer (Lepore & Revenson, 2007). Moreover, many coping behaviours, such as problem-solving, and seeking instrumental or emotional support, are fundamentally communicative and may offer little functional benefit or even be detrimental when enacted without disclosure and discussion of cancer-related content (Donovan-Kicken & Caughlin, 2011). Consistent with this interpretation, our mediation results showed significant indirect effects of self- and perceived-partner communication avoidance on all distress outcomes (depression, anxiety and stress) through greater disengagement coping and a significant indirect effect on anxiety through lower engagement coping.
Overall, the present study findings have implications for clinical practice and care of women with breast cancer, as they suggest that minimising communication avoidance of cancer-related matters between spouses and enhancing a woman’s coping capacity may be important targets for psychosocial intervention. Raising the woman’s awareness of how her, and her partner’s communication styles may be contributing to her emotional distress and maladaptive coping may be an important first step. Tailored psycho-education about each woman’s personal vicious cycle of maladaptive communication and coping processes may be more effective than provision of generic psycho-educational information. Oncology nurses, psychologists, social workers, and other professionals who have the requisite competencies to address complex couples’ communication and coping processes would be suited to offer such care.
The results of this study suggesting that couples coping with cancer have more difficulties discussing emotionally valenced topics related to disease progression and death, sexuality, and feelings than more practical concerns such as cancer treatment and relationship with health professionals also hold important clinical implications for screening guidelines and practices. A greater awareness by oncology health professionals of commonly avoided cancer topics between spouses may assist these professionals to more sensitively recognise and address couples’ conversational needs in clinical practice. More targeted screening of women’s communication of specific cancer topics and coping styles may help identify women at risk of developing psychopathology and facilitate more timely referral and access to psychosocial services. It may be good clinical practice for oncology health care providers to routinely question the basis of a woman’s psychological distress and normalise the difficulty of talking about particular cancer-related concerns. The negative correlation between relationship length and women’s level of communication avoidance also suggest that women in less established relationships may have more difficulty talking about cancer with their spouses and require more careful screening by oncology health professionals.
Another key finding that may inform intervention practices is the likely differential mediating effect of engagement and disengagement coping on the communication-distress relationship. Disengagement coping demonstrated a mediating effect of self- and perceived-partner communication avoidance on all psychological distress variables, whereas engagement coping met criteria as a mediator on depression only. This pattern of results is not surprising given the substantial evidence of the detrimental effects of disengagement coping on distress outcomes, as compared to the beneficial effects of engagement coping in breast cancer patients (Yang et al., 2008). Psychosocial interventions for cancer patients typically reinforce the importance of engagement coping strategies, such as seeking social and instrumental support and problem-solving, and not the adverse effects of using disengagement coping strategies, such as denial and self-blame (Yang et al., 2008). Clinically, these findings suggest that delivering support interventions that explicitly aim to both discourage the use of disengagement coping, and promote engagement coping, may be most beneficial for women with breast cancer.
Our finding of the strong association between a woman’s communication avoidance behaviours about cancer and those of her partner also suggests the importance of delivering psychosocial interventions at the dyadic level. While our cross-sectional data do not permit causal interpretation, the high concordance corresponds to communication theories and prior research that emphasise the bi-directional and interdependent influence of communication behaviours between spouses (Lepore & Revenson, 2007).
In the interpretation of these findings, some limitations need to be considered. First, the study employed a cross-sectional design, precluding the confirmation of causal relationships. Clearly, the mediation analyses undertaken in this study can only be suggestive of a true mediating effect. It is well-documented in the clinical research literature that people who are more anxious, stressed, or depressed are more withdrawn and avoid social interactions more often (Pruchno et al., 2009). Accordingly, it is plausible that distress may influence communication, or even in a bidirectional manner such to create a self-perpetuating cycle of greater communication avoidance and reduced adaptive coping efforts that further sustains and worsens the psychological outcomes in the cancer-affected women. The possibility that communication avoidance may mediate coping processes, rather than the reverse, and that psychological symptoms affect both these processes should also be evaluated. Future work on communication, coping processes and distress over time will help clarify the precise directionality of these processes and their underlying mechanisms. Second, couple communication data were obtained using the woman’s self-report of her and partner’s communication, without independent verification. It is possible that some of the women distorted their responses in social desirable ways, confounding research findings. Moreover, perceived partner communication avoidance scores should be interpreted with caution as it may be confounded by the woman’s relationship satisfaction with her partner. Future work should supplement self-report methodology with experimental analyses of couple interactions in laboratory or natural contexts. Third, study participants were all fluent in English, had access to computers and were mostly white, and well-educated. The relative ethnic, educational and socio-demographic homogeneity of the participants may have led to sample-specific patterns in the data, limiting the generalisability of our findings beyond our sample. Nevertheless, the present study sample aligns with the general demographic picture of women diagnosed with breast cancer in Australia (AIHW, 2012) and previous research of similar community-based breast cancer populations (Przezdziecki et al., 2013; Sheehan et al., 2007). Fourth, the present study evaluated only one dimension of communication behaviour: communication avoidance. Future work should evaluate other equally important dimensions of communication behaviour, such as communication openness, constraint or frequency of talk related to specific cancer-related topics, with indices of coping and distress outcomes. Future research that differentiates cancer-specific and general compromised communication processes would also help to clarify the extent to which interventions should focus on broadly improving the way couples communicate and relate to each other or target how they communicate about cancer specifically.
In summary, this study utilised a multi-topic communication measure to assess the associations of patient-reported avoidance of specific cancer-related topics, reports of partner avoidance of these topics, and indices of coping and psychological distress among breast cancer survivors. The results indicate that couples coping with cancer have more difficulties discussing emotionally valenced topics than more practical concerns, holding important clinical implications for screening guidelines and clinical practice. The results also indicate that communication avoidance about cancer between spouses is not only directly associated with more negative psychological consequences for the woman, but may also influence her psychological distress by impeding her coping ability. Enhancing couple communication about cancer and women’s adaptive coping skills (i.e., discourage use of disengagement coping strategies such as self-blame and denial, and promote use of engagement coping strategies such as positive reframing and acceptance) may be important targets for psychosocial intervention. Further research is needed to ascertain the directionality of the communication-distress relationship and the potential mediating role of coping, and to determine the most appropriate psycho-intervention approaches for this situation.
References
AIHW. (2012). Breast cancer in Australia: An overview. Canberra: AIHW.
Bartula, I., & Sherman, K. A. (2013). Screening for sexual dysfunction in women diagnosed with breast cancer: Systematic review and recommendations. Breast Cancer Research and Treatment, 141, 173–185. doi:10.1007/s10549-013-2685-9
Beatty, L. J., Koczwara, B., Rice, J., & Wade, T. D. (2010). A randomised controlled trial to evaluate the effects of a self-help workbook intervention on distress, coping and quality of life after breast cancer diagnosis. Medical Journal of Australia, 193, S68.
Bower, J. E. (2008). Behavioral symptoms in patients with breast cancer and survivors. Journal of Clinical Oncology, 26, 768–777.
Carver, C. S. (1997). You want to measure coping but your protocol’s too long: Consider the brief COPE. International Journal of Behavioral Medicine, 4, 92–100.
Caughlin, J., & Afifi, T. (2004). When is topic avoidance unsatisfying? A more complete investigation into the underlying links between avoidance and dissatisfaction in parent–child and dating relationships. Human Communication Research, 30, 479–513.
Caughlin, J. P., Mikucki-Enyart, S. L., Middleton, A. V., Stone, A. M., & Brown, L. E. (2011). Being open without talking about it: A rhetorical/normative approach to understanding topic avoidance in families after a lung cancer diagnosis. Communication Monographs, 78, 409–436.
Cella, D. F., Tulsky, D. S., Gray, G., Sarafian, B., Linn, E., Bonomi, A. E., et al. (1993). The Functional Assessment of Cancer Therapy scale: Development and validation of the general measure. Journal of Clinical Oncology, 11, 570–579.
Crawford, J. R., & Henry, J. D. (2003). The Depression Anxiety Stress Scales (DASS): Normative data and latent structure in a large non-clinical sample. British Journal of Clinical Psychology, 42, 111–131. doi:10.1348/014466503321903544
Donovan-Kicken, E. (2008). Avoiding communication with partners while coping with breast cancer: Implications for health and relationship satisfaction. (Doctoral dissertation, University of Illinois at Urbana-Champaign, Illinois). Available from ProQuest dissertations and theses database (UMI No. 3337751).
Donovan-Kicken, E., & Caughlin, J. P. (2010). A multiple goals perspective on topic avoidance and relationship satisfaction in the context of breast cancer. Communication Monographs, 77, 231–256. doi:10.1080/03637751003758219
Donovan-Kicken, E., & Caughlin, J. P. (2011). Breast cancer patients’ topic avoidance and psychological distress: The mediating role of coping. Journal of Health Psychology, 16, 596–606. doi:10.1177/1359105310383605
Figueiredo, M. I., Fries, E., & Ingram, K. M. (2004). The role of disclosure patterns and unsupportive social interactions in the well-being of breast cancer patients. Psycho-Oncology, 13, 96–105.
Folkman, S., & Moskowitz, J. T. (2004). Coping: Pitfalls and promise. Annual Review of Psychology, 55, 745–774. doi:10.1146/annurev.psych.55.090902.141456
Gho, S. A., Steele, J. R., Jones, S. C., & Munro, B. J. (2013). Self-reported side effects of breast cancer treatment: A cross-sectional study of incidence, associations, and the influence of exercise. Cancer Causes and Control, 24, 517–528. doi:10.1007/s10552-012-0142-4
Goldsmith, D. J., & Miller, G. A. (2013). Conceptualizing how couples talk about cancer. Health Communication, 29, 37–41. doi:10.1080/10410236.2012.717215
Goldsmith, D. J., Miller, L. E., & Caughlin, J. P. (2008). Openness and avoidance in couples communicating about cancer. Communication Yearbook, 31, 62–115.
Hilton, B. A., Crawford, J. A., & Tarko, M. A. (2000). Men’s perspectives on individual and family coping with their wives’ breast cancer and chemotherapy. Western Journal of Nursing Research, 22, 438–459.
Hordern, A. J., & Street, A. F. (2007). Communicating about patient sexuality and intimacy after cancer: Mismatched expectations and unmet needs. Medical Journal of Australia, 186, 224.
IBM Corp. (2012). IBM Statistical Package for the Social Sciences (SPSS) Statistics for Windows (Version 21) [Computer software]. Armonk, NY: IBM Corp.
Kershaw, T., Northouse, L., Kritpracha, C., Schafenacker, A., & Mood, D. (2004). Coping strategies and quality of life in women with advanced breast cancer and their family caregivers. Psychology & Health, 19, 139–155.
Kim, J., Han, J. Y., Shaw, B., McTavish, F., & Gustafson, D. (2010). The roles of social support and coping strategies in predicting breast cancer patients’ emotional well-being: Testing mediation and moderation models. Journal of Health Psychology, 15, 543–552. doi:10.1177/1359105309355338
Krebber, A., Buffart, L., Kleijn, G., Riepma, I., Bree, R., Leemans, C., et al. (2014). Prevalence of depression in cancer patients: A meta-analysis of diagnostic interviews and self-report instruments. Psycho-Oncology, 23, 121–130.
Kvillemo, P., & Bränström, R. (2014). Coping with breast cancer: A meta-analysis. PLoS One, 9, e112733.
Lepore, S. J., & Revenson, T. A. (2007). Social constraints on disclosure and adjustment to cancer. Social and Personality Psychology Compass, 1, 313–333.
Lewis, F. M., Fletcher, K. A., Cochrane, B. B., & Fann, J. R. (2008). Predictors of depressed mood in spouses of women with breast cancer. Journal of Clinical Oncology, 26, 1289–1295.
Lovibond, S. H., & Lovibond, P. F. (1996). Manual for the depression anxiety stress scales. Sydney: Psychology Foundation of Australia.
MacKinnon, D. P., Lockwood, C. M., Hoffman, J. M., West, S. G., & Sheets, V. (2002). A comparison of methods to test mediation and other intervening variable effects. Psychological Methods, 7, 83.
MacKinnon, D. P., Lockwood, C. M., & Williams, J. (2004). Confidence limits for the indirect effect: Distribution of the product and resampling methods. Multivariate Behavioral Research, 39, 99–128. doi:10.1207/s15327906mbr3901_4
Mallinger, J. B., Griggs, J. J., & Shields, C. G. (2006). Family communication and mental health after breast cancer. European Journal of Cancer Care, 15, 355–361. doi:10.1111/j.1365-2354.2006.00666.x
Manne, S. L., & Badr, H. (2008). Intimacy and relationship processes in couples’ psychosocial adaptation to cancer. Cancer, 112, 2541–2555. doi:10.1002/cncr.23450
Manne, S., Badr, H., Zaider, T., Nelson, C., & Kissane, D. (2010). Cancer-related communication, relationship intimacy, and psychological distress among couples coping with localized prostate cancer. Journal of Cancer Survivorship, 4, 74–85.
Manne, S. L., Kissane, D. W., Nelson, C. J., Mulhall, J. P., Winkel, G., & Zaider, T. (2011). Intimacy-enhancing psychological intervention for men diagnosed with prostate cancer and their partners: A pilot study. The Journal of Sexual Medicine, 8, 1197–1209.
Manne, S., Myers, S., Ozga, M., Kissane, D., Kashy, D., Rubin, S., et al. (2014). Holding back sharing concerns, dispositional emotional expressivity, perceived unsupportive responses and distress among women newly diagnosed with gynecological cancers. General Hospital Psychiatry, 36, 81–87.
Manne, S. L., Ostroff, J. S., Norton, T. R., Fox, K., Goldstein, L., & Grana, G. (2006). Cancer-related relationship communication in couples coping with early stage breast cancer. Psycho-Oncology, 15, 234–247. doi:10.1002/pon.941
Manne, S. L., Ostroff, J. S., Sherman, M., Glassman, M., Ross, S., Goldstein, L., & Fox, K. (2003). Buffering effects of family and friend support on associations between partner unsupportive behaviors and coping among women with breast cancer. Journal of Social and Personal Relationships, 20, 771–792.
Manne, S. L., Ostroff, J., Winkel, G., Grana, G., & Fox, K. (2005). Partner unsupportive responses, avoidant coping, and distress among women with early stage breast cancer: Patient and partner perspectives. Health Psychology, 24, 635–641. doi:10.1037/0278-6133.24.6.635
Mitchell, A. J., Ferguson, D. W., Gill, J., Paul, J., & Symonds, P. (2013). Depression and anxiety in long-term cancer survivors compared with spouses and healthy controls: A systematic review and meta-analysis. The Lancet Oncology, 14, 721–732.
Munro, H., Scott, S. E., King, A., & Grunfeld, E. A. (2014). Patterns and predictors of disclosure of a diagnosis of cancer. Psycho‐Oncology. doi:10.1002/pon.3679.
Northouse, L. L., Mood, D., Kershaw, T., Schafenacker, A., Mellon, S., Walker, J., et al. (2002). Quality of life of women with recurrent breast cancer and their family members. Journal of Clinical Oncology, 20, 4050–4064.
Porter, L. S., Keefe, F. J., Hurwitz, H., & Faber, M. (2005). Disclosure between patients with gastrointestinal cancer and their spouses. Psycho-Oncology, 14, 1030–1042.
Preacher, K. J., & Hayes, A. F. (2008). Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behavior Research Methods, 40, 879–891.
Preacher, K. J., Rucker, D. D., & Hayes, A. F. (2007). Addressing moderated mediation hypotheses: Theory, methods, and prescriptions. Multivariate Behavioral Research, 42, 185–227.
Pruchno, R., Wilson-Genderson, M., & Cartwright, F. P. (2009). Depressive symptoms and marital satisfaction in the context of chronic disease: A longitudinal dyadic analysis. Journal of Family Psychology, 23, 573.
Przezdziecki, A., Sherman, K. A., Baillie, A., Taylor, A., Foley, E., & Stalgis-Bilinski, K. (2013). My changed body: Breast cancer, body image, distress and self-compassion. Psycho-Oncology, 22, 1872–1879. doi:10.1002/pon.3230
Scott, J. L., Halford, W. K., & Ward, B. G. (2004). United we stand? The effects of a couple-coping intervention on adjustment to early stage breast or gynecological cancer. Journal of Consulting and Clinical Psychology, 72, 1122.
Sheehan, J., Sherman, K. A., Lam, T., & Boyages, J. (2007). Association of information satisfaction, psychological distress and monitoring coping style with post-decision regret following breast reconstruction. Psycho-Oncology, 16, 342–351.
Silva, S. M., Crespo, C., & Canavarro, M. C. (2012). Pathways for psychological adjustment in breast cancer: A longitudinal study on coping strategies and posttraumatic growth. Psychology & Health, 27, 1323–1341.
Soo, H., & Sherman, K. (2015). Rumination, psychological distress and post-traumatic growth in women diagnosed with breast cancer. Psycho-Oncology, 24, 70–79.
Stanton, A., & Revenson, T. A. (Eds.). (2011). Adjustment to chronic disease: Progress and promise in research. New York: Oxford University Press.
Tobin, D. L., Holroyd, K. A., Reynolds, R. V., & Wigal, J. K. (1989). The hierarchical factor structure of the coping strategies inventory. Cognitive therapy and Research, 13, 343–361.
Weihs, K. L., Enright, T. M., & Simmens, S. J. (2008). Close relationships and emotional processing predict decreased mortality in women with breast cancer: Preliminary evidence. Psychosomatic Medicine, 70, 117–124.
Yang, H.-C., Brothers, B. M., & Andersen, B. L. (2008). Stress and quality of life in breast cancer recurrence: Moderation or mediation of coping? Annals of Behavioral Medicine, 35, 188–197. doi:10.1007/s12160-008-9016-0
Acknowledgments
The authors wish to acknowledge the assistance of the Breast Cancer Network of Australia.
Conflict of interest
Yisha Yu and Kerry A. Sherman declared that they have no conflict of interest.
Human and animal rights and Informed Consent
All procedures followed were in accordance with ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000. Informed consent was obtained from all patients for being included in the study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Yu, Y., Sherman, K.A. Communication avoidance, coping and psychological distress of women with breast cancer. J Behav Med 38, 565–577 (2015). https://doi.org/10.1007/s10865-015-9636-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10865-015-9636-3