
Abstract
Aseptic implant loosening due to inflammatory reactions to wear debris is the main reason for the revision of total knee replacements (TKR). Hence, the decrease in polyethylene wear particle generation from the articulating surfaces is aimed at improving implant design and material. For preclinical testing of new TKR systems standardized wear tests are required. However, these wear tests do not reproduce the entire in vivo situation, since the pattern and amount of wear and subsequent implant failure are underestimated. Therefore, daily activity, kinematics, implant aging and position, third-body-wear and surface properties have to be considered to estimate the wear of implant components in vivo. Hence, severe test conditions are in demand for a better reproduction of the in vivo situation of TKR. In the present article an overview of different experimental wear test scenarios considering clinically relevant polyethylene wear situations using severe test conditions is presented.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
1 Introduction
For preclinical testing of new total knee replacement (TKR) systems and material innovations, an adequate experimental test set-up is required. It should reproduce the conditions of implant systems in order to simulate the in vivo wear situation of total joint replacements (TJR). Therefore, experimental wear testing of TJR systems has become a successful tool used for the evaluation of different bearing materials. In this context, standardization of the wear testing parameters is necessary to enable the comparison of the wear data of different implant systems and materials [1]. The forces, kinematics and environmental conditions during wear simulation of knee replacement are defined in ISO standard 14243 [2, 3] and should ensure definite experimental boundary conditions with identical implantations and patient related influencing factors (e.g. anatomy, kinematic). The results of the wear tests are intended to compare different implant designs and material combinations and are necessary for approval tests for manufactures.
Wear of the ultra high molecular weight polyethylene (UHMW-PE) inserts depends on TKR design (e.g. fixed or mobile bearing), UHMW-PE material (conventional and cross-linked UHMW-PE), material of the femoral component (metal, ceramic and coated), knee simulator and test parameters. Wear pattern of UHMW-PE after standard wear testing showed typical wear characteristics (e.g. burnishing, pitting and scratches), but in a clearly underestimated extent compared with in vivo wear. There are clinical observations which describe inadequate reproduction of clinical implant failure and wear patterns by experimental wear simulation according to the ISO standards [4–6].
Besides wear testing methods, the kind of bearing material of TKR systems clearly affects the amount of wear. UHMW-PE articulating against metallic or ceramic femoral components, plays the primary role in total knee arthroplasty. Alternative bearings like ceramic-on-ceramic or metal-on-metal are not available for total knee replacement today. For long-term survivorship of TKR systems of 90 % after 10 years, the use of UHMW-PE has become standard and no other material with such good frictional and adequate mechanical properties for the total knee joints is available so far.
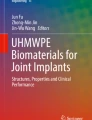
However, wear of UHMW-PE is one of the main reasons for implant failure [7, 8], limiting longevity. The in vivo measurement of UHMW-PE wear at the knee is difficult and no standard procedure is available, therefore, only retrieved inserts can indicate failure mechanisms. Typical characteristics of UHMW-PE damage are burnishing (Fig. 1a), pitting (Fig. 1b), delamination (Fig. 1c), scratching (Fig. 1d), deformation (creep) (Fig. 1e) and embedded debris (Fig. 1f), which are described in several retrieval studies [5, 9–11], but, as described above, are difficult to reproduce by means of knee simulator tests. Hence, some wear simulator tests have been adapted to more realistic test conditions in order to understand the in vivo wear mechanisms of UHMW-PE for further implant material and design improvements.

UHMW-PE wear characteristics, burnishing (a), pitting (b), delamination (c), scratching (d), creeping (e), embedded metal debris (f). Arrows show the specific wear characteristic
The present article gives an overview of clinically relevant conditions for severe test situations adopting to experimental wear testing using simulators. Hence, current experimental test set-ups with regard to severe test conditions and wear test data of UHMW-PE inserts are presented. Various research groups have conducted wear simulations investigating different severe conditions like severe kinematics, accelerated aging of polyethylene, malpositioning of the implant and third-body wear conditions. These studies demonstrated higher amounts of wear compared with standard wear test conditions.
The present overview of the severe test conditions is divided into four sections. At the beginning of each section the clinical situation, regarding the specific severe test parameter, is demonstrated to point out its relevance to the UHMW-PE wear. The Sect. 2: Aging of UHMW-PE deals with the oxidation of UHMW-PE and its influence on wear propagation. Due to decreased mechanical properties of the oxidized material, aging generally influences the wear behaviour of UHMW-PE. Artificial aged samples are often used in combination with other severe test conditions. The Sect. 3: Kinematic conditions of wear testing, deals with different daily life activities, e.g. stair climbing, sitting down, standing up, overloading or changes and starting and stopping different movements, as well as different ligamentous situations, which are not reproduced by current test standards. Because of the complexity of kinematic conditions, we divided the Sect. 3.2: Influence of joint force and movements pointing out simulator studies with different loads and movements compared with the standard tests; Sect. 3.3: Influence of resting periods considering the influence of non-uniform wear tests; and Sect. 3.4: Influence of ligament simulation in knee wear testing regarding different knee ligament models during wear test. As malpositioning of the implants (Sect. 4) often occurrs during implant surgery, an ideal implant position is hardly achievable. The implant position in turn has direct influence on the implant kinematic and the ligament situation visible on enlarged or unbalanced wear regions on the UHMW-PE. In this section the malalignment of the implants is emphasized. Third-body wear (Sect. 5) represents a relevant clinical situation. After total knee arthroplasty third-body particles like bone cement may be present in the knee joint and influence the wear of UHMW-PE, by means of direct abrasion or roughening of the articulating surfaces, indirectly influencing wear propagation.
2 Aging of UHMW-PE
2.1 Clinical situation
Delamination and cracking are the most common clinical failures of conventional tibial UHMW-PE inserts [12] (Fig. 2a–c), which cannot be reproduced with the ISO standard wear test (Fig. 2d) [13]. Medel et al. [14] found that delamination can be directly associated with oxidative degeneration of the analyzed retrieved UHMW-PE. Due to oxidation, aging is associated with the loss of mechanical properties [15, 16] and hence greater wear and failure of the UHMW-PE [17]. A common method to measure the oxidative degeneration of UHMW-PE, and therefore to determine the aging process, is to analyze the oxidation index (OI). The OI for retrieved inserts were detected with up to 5 [18], whereas new inserts only show an OI near zero [15].

Examples of severe worn UHMW-PE retrievals, in vivo duration (a) 12 years, (b) 14 years, (c) 14 years, (d) standard wear simulator test 5 million load cycles
2.2 Standard wear test
The ISO standard tests do not stipulate a special age of the test components. Usually, the test components are taken from original packaging without exceeding the expiration date, or manufactured with specific parameters and immediately used for wear tests.
2.3 Wear tests with accelerated aged UHMW-PE
Aging of the implant components applies particularly to UHMW-PE. The natural aging process of UHMW-PE in vivo takes a long time, but techniques have been developed (e.g. ASTM F2003-02 [19]) to accelerate the aging process for in vitro investigations. The OI is also used to determine the oxidation process. However, differences between natural in vivo and accelerated aging have been identified [20]. Kurtz et al. [21] identified large differences in the measuring of the OI and recommanded new OI measurement and accelerating aging standards. Knee wear simulator studies with accelerated aged tibial UHMW-PE inserts showed increased OI (0.8 [13], 1.9 [15]), increased wear and that the wear patterns, like delamination, could be better reproduced [13, 15, 22, 23]. Stoller et al. [22] found wear rates of 14.2 ± 2.6 mg/106 cycles for aged conventional and 4.1 ± 1.1 mg/106 cycles for aged cross-linked UHMW-PE; the wear reduction was statistically significant. Furthermore, Muratoglu et al. [13] demonstrated higher resistance against delamination of aged cross-linked UHMW-PE compared with conventional. Nonetheless, accelerated aging is an appropriate method to investigate wear behavior of UHMW-PE with regard to natural in vivo aging and should be considered in knee wear simulations. With new material innovations (cross-linked and antioxidant stabilized UHMW-PE), improved sterilization and storage methods (absence of oxygen), the oxidation of UHMW-PE can be reduced and amount of wear as well as delamination decreased consecutively [18, 22, 24]. With artificial aged UHMW-PE the delamination of the UHMW-PE inserts can be reproduced during wear simulator testing. This demonstrates the impact of changed material properties due to oxidation of the UHMW-PE and an adequate aging of the samples should be considered for wear simulator tests.
3 Kinematic conditions of wear testing
3.1 Clinical situation
Patients provided with TKR differ in body weight from normal weight up to obesity, influencing the loads transferring to the implants. Furthermore, kinematics (flexion, rotation, anterior posterior movement) of the knee joint differs individually, which is proved with fluoroscopy and radiostereometry [25, 26]. The activity of patients supplied with a TKR for everyday living is a sequence of different activities with regular periods without movement [27]. During these activities, dynamic motions alternate continuously with static periods and most of the day is spent in passive periods without joint motions [27]. Further, patients provided with TKR have a broad range of individual restraint characteristics [28–33]. However, ligamentous instabilities often occur in a complex manner, often related to several structures due to degenerative or traumatic changes [34].
3.2 Influence of joint forces and movements
3.2.1 Standard wear test
Preclinical wear testing of TKR is currently based on simulation of the axial load, flexion angle and an anterior-posterior and internal-external kinematic for level walking of an idealized average person. This can be done with a displacement controlled [3] or a load controlled wear simulator [2], where the kinematics of the latter is based on the applied loads and implant geometry [35, 36].
3.2.2 Wear tests with changed kinematics
Beyond the ISO standard further load profiles and joint kinematics have been described [37–39], and different strategies have been developed to simulate wear propagation with intensified kinematic conditions to evaluate the influence of biomechanical variance and to simulate additional failure mechanisms. Amplification of the data for level walking, especially in the internal-external and anterior-posterior direction, increases the amount of cross shear [40–42]. Barnett et al. [43], Knight et al. [44] and McEwen et al. [45] investigated an increase of the internal-external rotation from ±2.5° to ±5° and the anterior-posterior displacement from 5 mm to 10 mm, resulting in higher amounts of abrasive wear and enlarged wear regions on the UHMW-PE inserts.
Higher loads at higher flexion angles were applied during the simulation of going up and down stairs by Benson et al. [46]. By integrating stair descent in the simulator kinematics with a ratio of 1:70 (walking), the wear rate increased by a factor of 5 [46]. This result was not confirmed in a later study by Cottrell et al. [47] with the same ratio of walking and stair ascent. Amplification of the flexion angle during the stance phase, anterior posterior and axial load by Bell et al. [35], and internal-external torque increase the wear for a mobile bearing design, but have no significant influence on the wear of a (CR) design. The influence of an increased axial load, simulating an obese patient, was investigated by Schaerer et al. [48] After simulating a patient with a BMI of 45 by scaling the axial load 1.4 times compared with an average patient weight, the wear of a cruciate retaining (CR) total knee design was not significantly affected for conventional and cross-linked UHMW-PE material in a displacement controlled test set up according to ISO 14243-3. Different designs and materials can account for the difference in the outcome, as well as the differences in the kinematic input. The influence of material and design on the wear process was detected by Essner et al. [49] simulating stair climbing conditions for two million cycles in a displacement controlled simulator. In addition to stair ascend and descend, more complex test scenarios incorporating squatting and chair rising have been proposed [38, 50–53]. Jennings et al. [54] and Burton et al. [55] investigated the design influence with a simulation of condylar lift-off. The condylar lift off was achieved by introducing an adduction/abduction rotation torque and was performed every cylce. The lift off lead to a two- and threefold increase of wear at fixed and mobile bearing systems, repectively.
Additional topics related to the simulation of the surrounding structures are discussed in Sect. 3.4. All these different kinematic conditions are intended to simulate the wear behavior of knee implants in a more realistic way. One clinically observed failure which is not reproduced with standard wear test conditions is the structural failure of the UHMW-PE components. This failure mechanism termed delamination (see Sect. 2) is a combination of chemical degradation of the material properties and load concentration beneath the surface [56]. With a more physiological loading regime and a reduced amount of test cycles compared with previous test protocols [23, 57–59], in our study [60] and that of Popoola et al. [51] delamination (Fig. 3) can be generated when combined with artificial aging of the UHMW-PE.

Example of delamination at the articulating surface of the polyethylene insert after severe artificial aging and simulation of highly demanding daily activities (scaling 1 mm)
The kinematics chosen must be appropriate for the particular implant being tested. Although a standard protocol for displacement controlled tests is available [3] the standardization of kinematics for any kind of implants may be difficult as, for example, the displacements and rotations for highly conforming implant designs are expected to be lower in comparison with flat implant designs. Therefore, kinematic data should be individually obtained from calculations or from fluoroscopy if the particular implant is already in clinical use [61]. In force-controlled simulation [2], translations and rotations will be a function of the applied forces and torques, the shape of the bearing surfaces, as well as frictional forces [61–64].
3.3 Influence of resting periods
3.3.1 Standard wear test
Knee wear simulator studies are typically carried out continuously [65–67] without considering resting periods. This condition, however, does not reflect the versatile daily activities of a patient.
3.3.2 Wear tests considering different resting periods
In simplified tribological studies, it has been shown that shear force peaks are generated at motion initiation and that sticking effects may occur after resting periods [68]. Thus, the implementation of resting periods within the repetitive articulation in a wear simulator may cause an increase in wear of the implant. It is therefore important to know whether and to what extent resting periods may have an effect on the wear behavior of a TKR as tested in a wear simulator. Consequently, we have studied the effect of resting periods on the UHMW-PE wear behavior of TKR in a wear simulator study [69]. In that study, a continuous simulation was compared with a condition in which four active gait cycles were followed by a resting period of one second. All other conditions were the same in both tests. The wear rates are shown in Fig. 4.

Wear rates of the UHMW-PE during continuous and implemented resting periods wear tests [69]
Despite an increase in friction after motion initiation [68], resting periods seem to have no increasing effect on the wear rate of a TKR. This is in agreement with Shorez et al. [70], reporting on a decreased wear rates in hip wear testing when implementing resting periods into simulation. There are several reasons for these seemingly contradictory results. During a gait cycle several points of inflection in the different directions of motion occur. For example, when motion reverses at maximum internal rotation into external rotation, the relative velocity becomes zero and may be considered a resting period regarding rotation. At about 13 % of the gait cycle during simulation an inversion of all motion directions occurs, therefore, in each gait cycle resting periods may already be considered. Other aspects of resting periods which may have a wear reducing effect are better lubrication due to a prolonged period with small axial loading and a prolonged testing period for the same number of cycles which is known to have a wear reducing effect [71].
3.4 Influence of ligament simulation in knee wear testing
3.4.1 Standard wear test
Therefore, the ISO standards provides two different ligamentous restraint systems for testing, representing clinically the most commonly seen settings: testing with intact posterior cruciate ligament for cruciate retaining knee designs and testing with absence/insufficiency of the posterior cruciate ligament for coupled designs (posterior stabilized or posterior substituting designs). In force-controlled simulations, the motion range has to be restrained in a similar way as it is the in vivo condition, which is regulated by the soft tissues and ligaments. Soft tissue and ligament restrain are known to act in a non-linear manner. Until 2009, the ISO standard for force-controlled knee wear testing (ISO 14243:2002) was based on a linear ligament model. The definition of the ligament model was renewed in 2009 (ISO 14243:2009) [2] to include a biphasic ligament model and recent studies have confirmed the impact and relevance of the ligament simulation regarding PE wear and implant kinematics [72, 73]. However, standardized wear testing does not consider ligamentous instabilities which may become relevant in clinical practice.
3.4.2 Wear tests with different ligament situation
In a knee wear simulator study, we studied the effect of different ligament models as regards UHMW-PE wear and implant kinematics [74]. In this study, a non-linear elastic ligament model was chosen based on biomechanical studies [28–33] and compared with a simplified linear-elastic ligament model in accordance with ISO 14243-1:2002. A virtual soft tissue control system was implemented in order to simulate different motion restraints. Regarding the resulting UHMW-PE wear rate, a significant influence of the applied ligament model has been shown (Fig. 5). Furthermore, the resulting kinematics was significantly increased under the application of the non-linear ligament model (Fig. 6). This study clearly shows that simulation of an appropriate ligament model influences implant kinematics during a wear test and, subsequently, influences the UHMW-PE wear rate. In a recent publication [75], we analyzed the wear behavior of a high-conforming knee design under stable and unstable ligamentous conditions. Unstable conditions were related to cruciate (absence of anterior and posterior cruciate ligaments) as well as collateral ligaments (insufficiency of medial collateral ligament). Under stable conditions only the anterior cruciate ligament was absent. Wear testing revealed an increase of 83 % in wear rate, which was related to the insufficient compensatory stabilization via implant design. Wear testing should not only consider the most frequent loading situation but also the most severe condition which may arise clinically.

Results of different ligament models regarding the UHMW-PE-wear rate

Kinematics depending on the test conditions applied
In general, the application of more complex ligament models in order to appropriately simulate the function of the human knee joint and to evaluate wear behavior of TKR is recommended.
4 Malpositioning of implant components
4.1 Clinical situation
Several clinical studies have demonstrated inaccurate intraoperative positioning of total knee implants [76, 77], and the revision rates of TKR implanted with e.g. varus malalignment are significantly higher than with the recommended implant position [78–80]. As a result of malpositioned implants, the bone stock, the adjacent soft tissue and the implant components can be overloaded due to displaced load transfer, and the amount of wear particles released from the implant components can be increased. A retrieval investigation of Srivastava et al. [81] determined a direct correlation between varus-malalignment and wear of UHMW-PE. Unbalanced worn UHMW-PE inserts retrieved in case of malpositioning are shown in Fig. 7.

Retrievals with unbalanced worn UHMW-PE, a wear region is characterized by delamination and creep and is displaced only to the posterior side (arrows); b wear region is characterized by delamination, massive abrasion and a one-sided worn-through of the UHMW-PE (arrow)
4.2 Standard wear test
For standard wear testing of TKR alignment of the femoral and tibial components are defined in ISO standard [2, 3]. The axes of axial and anterior-posterior forces and rotations have to be ideal parallel or perpendicular to the respective toward axes, and the axial force axis should be offset into medial direction, to reproduce the ideal load transfer and function of the TKR. However, individual deviations caused by the manual implantation procedure or anatomic features are not considered and UHMW-PE show design dependent uniform worn regions.
4.3 Wear tests with malpositioned knee implants
In the case of malaligned total knee implants experimental testing has demonstrated higher loading of the implant components, poor implant survival rates and increased amounts of wear. Concerning increased loads, Werner et al. [82] investigated the load distribution of varus/valgus malaligned TKR, and Cheng et al. [83] investigated medial–lateral and anterior-posterior maltranslation and rotational mismatch. Both studies found higher loads on the malaligned relevant implant positions, indicating increased wear of UHMW-PE. Finite element analysis has also confirmed the higher stresses on malaligned knee components [84]. We investigated the influence of varus (6°) and internal rotation (9°) malalignment separately in a wear knee simulator [85]. Malaligned total knee implants showed a significantly increased wear rate and deviating worn regions on the insert compared with the normal implant position (Fig. 8) [85]. D’Lima et al. [86] found similar results with varus malalignment using wear simulation; the malaligned group even induce higher wear rates than the group with higher loads, axial rotation and anterior-posterior translation. The influence of tibial slope on UHMW-PE wear was investigated by Weber et al. [87] in unicondylar knee replacement; wear was decreased with higher tibial slope.

Wear rate of the polyethlylene inserts of normal positioned versus malaligned TKR and the corresponding wear regions [85], retrieved UHMW-PE of the same implant design used for wear tests with in vivo duration of 19 month (a), normal implant position (b), 6° varus malalignment (c), the arrows show the displaced wear region compared with the normal implant position (d)
The significance of implant position has been demonstrated by the described simulator tests, with the limitation that only a single parameter was analyzed. The wear regions on the UHMW-PE differ from the normal positioned standard tests depending on the malaligned parameter, but in none of the groups tested separately malaligned positions described retrieval occurring wear pattern and insert damage. Hermida et al. [17] analysed in a wear simulator study the influence of varus and rotational malalignment as well as a displaced mediolateral load distribution at the same time. Combining all malalignments and using aged UHMW-PE, delamination and massive wear of the non-cross-linked inserts could be generated to match more the retrieval observations. In case of specific anatomical conditions or bone defects, an optimal implant position cannot always be achieved. Obviously, not all malalignment conditions can be tested by wear simulation, but the frequently used implant positions, varus/valgus, rotation and translation should be considered to indicate the influence of implant design and material on malpositioning. Due to cross-linking and mobile bearing systems the UHMW-PE seems to be more resistant against malaligned implant components than conventional UHMW-PE and fixed bearing systems, respectively [17, 83].
5 Third-body wear
5.1 Clinical situation
Following several attempts to explain the phenomenon of early TKR revision, third-body wear is believed to increase wear and therefore accelerate wear-associated aseptic loosening and early implant failure [88–90]. Severe osteolysis after elevated wear generation due to third-body wear could be demonstrated in a retrieval study as well [91]. In particular, damaged metal heads after total hip arthroplasty seem to produce more UHMW-PE wear than damaged ceramic heads [92]. Nevertheless, UHMW-PE and metal bearing surfaces remain the material of choice in knee replacement. In case of revision saline lavage of cemented TKR bone, bone cement and metal particles have been detected [93, 94], which remained in the knee joint after insufficient pulse lavage and acted as third-bodies in the bearing. Bone and bone cement particles with a size of 200–240 and 250–340 µm were detected [93], whereas detected metal particles are considerably smaller with 1–2 µm [95]. In cases of unicondylar knee replacement, minimally invasive approaches increase the chance of overlooking third-body particles (Fig. 9), especially in a cemented technique [96]. As free particles in the joint or embedded in the UHMW-PE the residual particles cause abrasion and roughening and generate deep scratches on the bearing surfaces. Scratches and embedded debris on UHMW-PE retrievals are common, and, consequently, suggest the presence of third-body particles in vivo (Fig. 10). Muratoglu et al. [97] found scratches on retrieved femoral components with considerable roughening of the bearing surface.

The lateral radiograph of the knee after UKA shows a bone cement third body in the posterior joint space (asterisk)

SEM picture of a retrieved UHMW-PE insert with embedded metal third-body particles
5.2 Standard wear test
As lubricant the ISO standard provides calf serum, which is filtered through a 2 µm filter before wear test and the lubricant is replaced every 500.000 cycles. Consequently, the medium should be free of particles >2 µm during the wear test. This ensures that every implant system is tested in clean lubricant and the results are comparable.
5.3 Third-body wear tests
In a wear simulator test by Muratoglu et al. [97] retrieved scratched femoral components, due to third-body wear particles, were investigated with regard to UHMW-PE wear. They found a significant increase of the UHMW-PE wear compared with unscratched femoral components, and an advantage of cross-linked PE [97]. Several wear simulator studies investigating the direct effect of third-body wear particles at knee replacement are available, using bone, bone cement and metal particles. Davidson et al. [88] found in a simulator based study that third-bodies are capable of causing increased abrasive wear of UHMW-PE, and that abrasion of the hard bearing surfaces will occur if the hardness of the third-body debris exceeds the hardness of the metal or ceramic bearing surface. It seems that ceramic is more resistant against third-body wear particles [88]. This was confirmed in our study [98] investigating the effect of bone cement particles (≤30 µm) on bicondylar TKR, comparing cobalt-chromium and ceramic femoral components. The third-body particles were rubbed-in into the UHMW-PE before filling with test lubrication. This study demonstrated that the wear of UHMW-PE inserts under third-body wear conditions, in combination with ceramic femoral components, increased compared with standard test conditions, but significantly lower than with metallic femoral components [98]. The difference of the effect of bone (mean 670 µm) and bone cement particles (mean 640 µm) on unicondylar knee endoprostheses with conventional UHMW-PE inserts was investigated by Schroeder et al. [99]. Interestingly, after adding the porcine bone particles to the test lubrication, the wear rate decreased from 4.4 ± 0.91 mm3/106 cycles steady state wear without third-body particles to 3.0 ± 1.27 mm3/106 cycles. Cement particles led to a significantly higher wear rate of 25.0 ± 16.93 mm3/106 cycles [99]. In contrast, bone particles as third-bodies are suggested to have a less critical influence on the measured wear rate [99]. The results of the described studies certainly show the effect of third-bodies on the wear rate. However, the used particles, their sizes and amounts as well as the particle insertion (added to the lubrication or rubbed into the UHMW-PE) differ and no consistent methods for investigating the influence of third-bodies are available. Furthermore, the gravimetrical wear measurement of the UHMW-PE could be falsified by embedded particles, despite complex cleaning of the inserts.
A standardization of the third-body particles with respect to the in vivo situation, corresponding to particles found in vivo, their insertion during the wear test and an adequate method for wear measurement, could prove the resistance of different bearing materials against third-bodies, which was demonstrated with the advantage of ceramic over metal. An investigation of different UHMW-PE (cross-linked, antioxidant stabilized) with third-bodies at TKR could demonstrate an increased wear resistance against third-bodies [97]. Based on the results of the wear simulator studies and clinical observations of the past decades, third-body particles should be avoided and removed if noted at any cost to avoid elevated wear rates and therefore, early implant failure.
6 Conclusion
Wear testing of TKR according to the ISO standards is an appropriate method to compare the wear behavior of different implant designs and can classify material and design innovations with existing products under reproducible test methods and conditions. However, different wear patterns and failure modes of the implant components occur in vivo. In vivo wear is a complex process influenced by multiple and patient individual parameters, e.g. different daily activities of TKR patients in addition to walking, soft tissue conditions, implant position, third-body wear particles, aging and surface properties can affect wear. These conditions are not considered in standard wear testing methods. Under in vivo conditions, a combination of these severe wear test conditions is assumed. At present, only implant retrievals and post-mortem analysis can provide substantial data about the amount and pattern of polyethylene wear in vivo.
However, not all in vivo situations associated with an increased wear of UHMW-PE could be reproduced in experimental wear tests. Nevertheless, innovations of bearing materials (e.g. cross-linking of UHMW-PE) which are more resistant against wear and oxidation—surgical methods (e.g. navigated/computer-assisted surgery) or TKR designs to reduce the impact of implant alignment (e.g. mobile bearing)—could be proved to decrease polyethylene wear.
Most of the presented literature demonstrated increased wear using severe test conditions. It seems that using amplified kinematics combined with aged UHMW-PE during knee wear simulation is most suitable to reproduce the observed delamination on UHMW-PE retrievals, the most severe wear pattern clinically. In comparison third-body wear and malpositioning at knee simulator wear tests demonstrate more abrasive wear, similar wear pattern, like pitting and scratches, as well as unbalanced overloading of the UHMW-PE and a larger contact area of the bearing, but not in such a distinctive characteristic as in retrievals. Beyond the standard wear tests, new wear simulator test concepts are in demand to reproduce the realistic patient´s daily activities and kinematics and loading on implant components, including soft tissue conditions.
References
McKellop HA, D’Lima DD. How have wear testing and joint simulator studies helped to discriminate among materials and designs? J Am Acad Orthop Surg. 2008;16(Suppl 1):S111–9.
ISO 14243-1:2009, implants for surgery—wear of total knee-joint prostheses—Part 1: loading and displacement parameters for wear-testing machines with load control and corresponding environmental conditions for test. 2009.
ISO 14243-3:2004, implants for surgery—wear of total knee-joint prostheses—Part 3: loading and displacement parameters for wear-testing machines with displacement control and corresponding environmental conditions for test. 2004.
Harman MK, DesJardins J, Benson L, Banks SA, LaBerge M, Hodge WA. Comparison of polyethylene tibial insert damage from in vivo function and in vitro wear simulation. J Orthop Res. 2009;27(4):540–8.
Rawlinson JJ, Furman BD, Li S, Wright TM, Bartel DL. Retrieval, experimental, and computational assessment of the performance of total knee replacements. J Orthop Res. 2006;24(7):1384–94.
Harman M, Affatato S, Spinelli M, Zavalloni M, Stea S, Toni A. Polyethylene insert damage in unicondylar knee replacement: a comparison of in vivo function and in vitro simulation. Proc Inst Mech Eng H. 2010;224(7):823–30.
Schroer WC, Berend KR, Lombardi AV, Barnes CL, Bolognesi MP, Berend ME, Ritter MA, Nunley RM. Why are total knees failing today? Etiology of total knee revision in 2010 and 2011. J Arthroplasty. 2013;28(8 Suppl):116–9.
Dalury DF, Pomeroy DL, Gorab RS, Adams MJ. Why are total knee arthroplasties being revised? J Arthroplasty. 2013;28(8 Suppl):120–1.
Pang HN, Jamieson P, Teeter MG, McCalden RW, Naudie DD, MacDonald SJ. Retrieval analysis of posterior stabilized polyethylene tibial inserts and its clinical relevance. J Arthroplasty. 2014;29(2):365–8.
Manson TT, Kelly NH, Lipman JD, Wright TM, Westrich GH. Unicondylar knee retrieval analysis. J Arthroplasty. 2010;25(6 Suppl):108–11.
Oonishi H, Ueno M, Kim SC, Oonishi H, Iwamoto M, Kyomoto M. Ceramic versus cobalt-chrome femoral components; wear of polyethylene insert in total knee prosthesis. J Arthroplasty. 2009;24(3):374–82.
Collier JP, Sperling DK, Currier JH, Sutula LC, Saum KA, Mayor MB. Impact of gamma sterilization on clinical performance of polyethylene in the knee. J Arthroplasty. 1996;11(4):377–89.
Muratoglu OK, Bragdon CR, Jasty M, O’Connor DO, Von Knoch RS, Harris WH. Knee-simulator testing of conventional and cross-linked polyethylene tibial inserts. J Arthroplasty. 2004;19(7):887–97.
Medel FJ, Kurtz SM, Parvizi J, Klein GR, Kraay MJ, Rimnac CM. In vivo oxidation contributes to delamination but not pitting in polyethylene components for total knee arthroplasty. J Arthroplasty. 2011;26(5):802–10.
Haider H, Weisenburger JN, Kurtz SM, Rimnac CM, Freedman J, Schroeder DW, Garvin KL. Does vitamin E-stabilized ultrahigh-molecular-weight polyethylene address concerns of cross-linked polyethylene in total knee arthroplasty? J Arthroplasty. 2012;27(3):461–9.
Micheli BR, Wannomae KK, Lozynsky AJ, Christensen SD, Muratoglu OK. Knee simulator wear of vitamin E stabilized irradiated ultrahigh molecular weight polyethylene. J Arthroplasty. 2012;27(1):95–104.
Hermida JC, Fischler A, Colwell CW, D’Lima DD. The effect of oxidative aging on the wear performance of highly crosslinked polyethylene knee inserts under conditions of severe malalignment. J Orthop Res. 2008;26(12):1585–90.
Medel FJ, Rimnac CM, Kurtz SM. On the assessment of oxidative and microstructural changes after in vivo degradation of historical UHMWPE knee components by means of vibrational spectroscopies and nanoindentation. J Biomed Mater Res A. 2009;89(2):530–8.
ASTM Standard F2003-02. Standard practice for accelerated aging of ultra-high molecular weight polyethylene after gamma irradiation in air. 2008.
Edidin AA, Jewett CW, Kalinowski A, Kwarteng K, Kurtz SM. Degradation of mechanical behavior in UHMWPE after natural and accelerated aging. Biomaterials. 2000;21(14):1451–60.
Kurtz SM, Muratoglu OK, Buchanan F, Currier B, Gsell R, Greer K, Gualtieri G, Johnson R, Schaffner S, Sevo K, Spiegelberg S, Shen FW, Yau SS. Interlaboratory reproducibility of standard accelerated aging methods for oxidation of UHMWPE. Biomaterials. 2001;22(13):1731–7.
Stoller AP, Johnson TS, Popoola OO, Humphrey SM, Blanchard CR. Highly crosslinked polyethylene in posterior-stabilized total knee arthroplasty: in vitro performance evaluation of wear, delamination, and tibial post durability. J Arthroplasty. 2011;26(3):483–91.
Walker PS, Blunn GW, Perry JP, Bell CJ, Sathasivam S, Andriacchi TP, Paul JP, Haider H, Campbell PA. Methodology for long-term wear testing of total knee replacements. Clin Orthop Relat Res. 2000;372:290–301.
Kester MA, Herrera L, Wang A, Essner A. Knee bearing technology: where is technology taking us? J Arthroplasty. 2007;22(7 Suppl 3):16–20.
Uvehammer J, Kärrholm J, Brandsson S. In vivo kinematics of total knee arthroplasty. Concave versus posterior-stabilised tibial joint surface. J Bone Joint Surg Br. 2000;82(4):499–505.
Schmidt R, Komistek RD, Blaha JD, Penenberg BL, Maloney WJ. Fluoroscopic analyses of cruciate-retaining and medial pivot knee implants. Clin Orthop Relat Res. 2003;410:139–47.
Morlock M, Schneider E, Bluhm A, Vollmer M, Bergmann G, Muller V, Honl M. Duration and frequency of every day activities in total hip patients. J Biomech. 2001;34(7):873–81.
Shoemaker SC, Markolf KL. Effects of joint load on the stiffness and laxity of ligament-deficient knees. An in vitro study of the anterior cruciate and medial collateral ligaments. J Bone Joint Surg Am. 1985;67(1):136–46.
Fukubayashi T, Torzilli PA, Sherman MF, Warren RF. An in vitro biomechanical evaluation of anterior-posterior motion of the knee. Tibial displacement, rotation, and torque. J Bone Joint Surg Am. 1982;64(2):258–64.
Markolf KL, Kochan A, Amstutz HC. Measurement of knee stiffness and laxity in patients with documented absence of the anterior cruciate ligament. J Bone Joint Surg Am. 1984;66(2):242–52.
Kanamori A, Zeminski J, Rudy TW, Li G, Fu FH, Woo SL. The effect of axial tibial torque on the function of the anterior cruciate ligament: a biomechanical study of a simulated pivot shift test. Arthroscopy. 2002;18(4):394–8.
Butler DL, Noyes FR, Grood ES. Ligamentous restraints to anterior-posterior drawer in the human knee. A biomechanical study. J Bone Joint Surg Am. 1980;62(2):259–70.
Woo SL, Kanamori A, Zeminski J, Yagi M, Papageorgiou C, Fu FH. The effectiveness of reconstruction of the anterior cruciate ligament with hamstrings and patellar tendon. A cadaveric study comparing anterior tibial and rotational loads. J Bone Joint Surg Am. 2002;84(6):907–14.
Briard JL, Witoolkollachit P, Lin G. Weichteilmanagement in der Knieendoprothetik. Orthopade. 2007;36:635–42.
Bell CJ, Haider H, Blunn GW. Wear of fixed versus mobile bearing knees under normal and enhanced walking cycles. In: Transactions of the sixth World Biomaterials Congress (6), 6th World Biomaterials Congress, Kamuela (Big Island), Hawaii, USA, 2000:873.
Haider H, Alberts LR, Johnson TS, Yao JQ. Comparison between force-controlled and displacement-controlled in -vitro wear testing on a widely used TKR implant. In: Transactions of the Orthopaedic Research Society (48), 48 th Annual Meeting of the Orthopaedic Research Society, Dallas, TX, USA, 2002: Poster No. 1007.
Ngai V, Schwenke T, Wimmer MA. In-vivo kinematics of knee prostheses patients during level walking compared with the ISO force-controlled simulator standard. Proc Inst Mech Eng H. 2009;223(7):889–96.
Schwiesau J, Schilling C, Kaddick C, Utzschneider S, Jansson V, Fritz B, Blomer W, Grupp TM. Definition and evaluation of testing scenarios for knee wear simulation under conditions of highly demanding daily activities. Med Eng Phys. 2013;35(5):591–600.
Bergmann G, Bender A, Graichen F, Dymke J, Rohlmann A, Trepczynski A, Heller MO. Kutzner I1. Standardized loads acting in knee implants. PLoS One. 2014;9(1):e86035.
Wang A, Sun DC, Yau SS, Edwards B, Sokol M, Essner A, Polineni VK, Stark C, Dumbleton JH. Orientation softening in the deformation and wear of ultra-high molecular weight polyethylene. Wear. 1997;203–204:230–41.
Kang L, Galvin AL, Brown TD, Jin Z, Fisher J. Quantification of the effect of cross-shear on the wear of conventional and highly cross-linked UHMWPE. J Biomech. 2008;41(2):340–6.
Schwenke T, Wimmer MA. Cross-shear in metal-on-polyethylene articulation of orthopaedic implants and its relationship to wear. Wear. 2013;301(1–2):168–74.
Barnett PI, Fisher J, Auger DD, Stone MH, Ingham E. Comparison of wear in a total knee replacement under different kinematic conditions. J Mater Sci Mater Med. 2001;12(10–12):1039–42.
Knight LA, McEwen HM, Farrar R, Stone MH, Fisher J, Taylor M. The influence of the wear path on the rates on total knee replacement. Summer Bioengineering Conference, Key Biscayne, FL, USA, 2003:1179–80.
McEwen HM, Barnett PI, Bell CJ, Farrar R, Auger DD, Stone MH, Fisher J. The influence of design, materials and kinematics on the in vitro wear of total knee replacements. J Biomech. 2005;38(2):357–65.
Benson LC, DesJardins JD, Harman MK, LaBerge M. Effect of stair descent loading on ultra-high molecular weight polyethylene wear in a force-controlled knee simulator. Proc Inst Mech Eng H. 2002;216(6):409–18.
Cottrell JM, Babalola O, Furman BS, Wright TM. Stair ascent kinematics affect UHMWPE wear and damage in total knee replacements. J Biomed Mater Res B Appl Biomater. 2006;78(1):15–9.
Schaerer C, Mimnaugh K, Popoola OO, Seebeck J. Wear of UHMWPE tibial inserts under simulated obsese patient conditions. In: Transactions of the Orthopaedic Research Society (56), 56th Annual Meeting of the Orthopaedic Research Society, New Orleans, LA, USA, 2010: Poster No. 2329.
Essner A, Herrera L, Hughes P, Kester M. The influence of material and design on total knee replacement wear. J Knee Surg. 2011;24(1):9–17.
Johnson TS, Yao JQ, Laurent MP, Blanchard CR, Crowninshield RD. Implementation of multiple activities of daily living for knee wear testing. In: Transactions of the Seventh World Biomaterials Congress (7), Sydney, Australia, 2004:83.
Popoola OO, Yao JQ, Johnson TS, Blanchard CR. Wear, delamination, and fatigue resistance of melt-annealed highly crosslinked UHMWPE cruciate-retaining knee inserts under activities of daily living. J Orthop Res. 2010;28(9):1120–6.
Orozco DA, Wimmer MA. The impact of daily physical activities on TKR wear. Biomaterialien. 2010;11(S1):107.
Franta L, Kronek J, Suchánek J. TKA wear testing input after kinematic and dynamic meta-analysis: technique and proof of concept. Wear. 2011;271(9–10):2687–92.
Jennings LM, Bell CI, Ingham E, Komistek RD, Stone MH, Fisher J. The influence of femoral condylar lift-off on the wear of artificial knee joints. Proc Inst Mech Eng H. 2007;221(3):305–14.
Burton A, Williams S, Brockett CL, Fisher J. In vitro comparison of fixed- and mobile meniscal-bearing unicondylar knee arthroplasties: effect of design, kinematics, and condylar liftoff. J Arthroplasty. 2012;27(8):1452–9.
Bell CJ, Walker PS, Abeysundera MR, Simmons JM, King PM, Blunn GW. Effect of oxidation on delamination of ultrahigh-molecular-weight polyethylene tibial components. J Arthroplasty. 1998;13(3):280–90.
Blunn GW, Walker PS, Joshi A, Hardinge K. The dominance of cyclic sliding in producing wear on total knee replacements. Clin Orthop Relat Res. 1991;273:253–60.
Deluzio KJ, Connor DO, Bragdon CR, Muratoglu OK, Flynn H, Rubash H, Jasty M, Wyss UP, Harris WH. Development of an in vitro knee delamination model in a knee simulator with physiologic load and motion. In: Transactions of the Orthopaedic Research Society (46), 46th Annual Meeting of the Orthopaedic Research Society, Orlando, FL, USA, 2000: Poster No. 0490.
Muratoglu OK, Bragdon CR, Connor DO, Perinchief RS, Travers JT, Jasty M, Rubash H, Harris WH. Markedly improved adhesive wear and delamination resistance with a highly crosslinked UHMWPE for use in total knee arthroplasty. In: Transactions of the Orthopaedic Research Society (47), 47th Annual Meeting of the Orthopaedic Research Society, San Fransisco, CA, USA, 2001: Poster No. 1009.
Schwiesau J, Schilling C, Utzschneider S, Jansson V, Fritz B, Blomer W, Grupp TM. Knee wear simulation under conditions of highly demanding daily activities–influence on an unicompartmental fixed bearing knee design. Med Eng Phys. 2013;35(8):1204–11.
Walker PS, Haider H. Characterizing the motion of total knee replacements in laboratory tests. Clin Orthop Relat Res. 2003;410:54–68.
Walker PS, Blunn GW, Broome DR, Perry J, Watkins A, Sathasivam S, Dewar ME, Paul JP. A knee simulating machine for performance evaluation of total knee replacements. J Biomech. 1997;30(1):83–9.
DesJardins JD, Walker PS, Haider H, Perry J. The use of a force-controlled dynamic knee simulator to quantify the mechanical performance of total knee replacement designs during functional activity. J Biomech. 2000;33(10):1231–42.
Haider H, Walker PS. Measurements of constraint of total knee replacement. J Biomech. 2005;38(2):341–8.
Ezzet KA, Hermida JC, Colwell CW, D’Lima DD. Oxidized zirconium femoral components reduce polyethylene wear in a knee wear simulator. Clin Orthop Relat Res. 2004;428:120–4.
Johnson TS, Laurent MP, Yao JQ, Blanchard CR. Comparison of wear of mobile and fixed bearing knees tested in a knee simulator. Wear. 2003;255(7–12):1107–12.
Mueller-Rath R, Kleffner B, Andereya S, Mumme T, Wirtz DC. Measures for reducing ultra-high-molecular-weight polyethylene wear in total knee replacement: a simulator study. Biomed Tech (Berl). 2007;52(4):295–300.
Nassutt R, Wimmer MA, Schneider E, Morlock M. The influence of resting periods on friction in the artificial hip. Clin Orthop Relat Res. 2003;407:127–38.
Kretzer JP, Jakubowitz E, Hofmann K, Heisel C, Lietz E. Influence of resting periods on polyethylene wear in a knee simulator study. Med Sci Monit. 2009;15(11):MT143–6.
Shorez JP, Harding TS, Atkinson PJ, Walter N. Alteration of the amount and morphology of wear particles by the addition of loading profile transitions during artificial hip wear testing. Proc Inst Mech Eng H. 2008;222:865–75.
Reinders J, Sonntag R, Kretzer JP. How do gait frequency and serum-replacement interval affect polyethylene wear in knee-wear simulator tests? J Mater Sci Mater Med. 2014;25(11):2463–9.
Grupp TM, Saleh KJ, Mihalko WM, Hintner M, Fritz B, Schilling C, Schwiesau J, Kaddick C. Effect of anterior-posterior and internal-external motion restraint during knee wear simulation on a posterior stabilised knee design. J Biomech. 2013;46(3):491–7.
Grupp TM, Schroeder C, Kyun KT, Miehlke RK, Fritz B, Jansson V, Utzschneider S. Biotribology of a mobile bearing posterior stabilised knee design—effect of motion restraint on wear, tibio-femoral kinematics and particles. J Biomech. 2014;47(10):2415–23.
Kretzer JP, Jakubowitz E, Sonntag R, Hofmann K, Heisel C, Thomsen M. Effect of joint laxity on polyethylene wear in total knee replacement. J Biomech. 2010;43(6):1092–6.
Reinders J, Sonntag R, Kretzer JP. Wear behavior of an unstable knee: stabilization via implant design? Biomed Res Int. 2014;2014:7.
Chua KH, Chen Y, Lingaraj K. Navigated total knee arthroplasty: is it error-free? Knee Surg Sports Traumatol Arthrosc. 2014;22(3):643–9.
Perlick L, Luring C, Tingart M, Grifka J, Bathis H. Revision prosthetic of the knee joint. The influence of a navigation system on the alignment and reconstruction of the joint line. Orthopade. 2006;35(10):10806.
Fang DM, Ritter MA, Davis KE. Coronal alignment in total knee arthroplasty: just how important is it? J Arthroplasty. 2009;24(6 Suppl):39–43.
Kim YH, Park JW, Kim JS, Park SD. The relationship between the survival of total knee arthroplasty and postoperative coronal, sagittal and rotational alignment of knee prosthesis. Int Orthop. 2014;38(2):379–85.
Ritter MA, Faris PM, Keating EM, Meding JB. Postoperative alignment of total knee replacement. Its effect on survival. Clin Orthop Relat Res. 1994;299:153–6.
Srivastava A, Lee GY, Steklov N, Colwell CW, Ezzet KA, D’Lima DD. Effect of tibial component varus on wear in total knee arthroplasty. Knee. 2012;19(5):560–3.
Werner FW, Ayers DC, Maletsky LP, Rullkoetter PJ. The effect of valgus/varus malalignment on load distribution in total knee replacements. J Biomech. 2005;38(2):349–55.
Cheng CK, Huang CH, Liau JJ, Huang CH. The influence of surgical malalignment on the contact pressures of fixed and mobile bearing knee prostheses–a biomechanical study. Clin Biomech (Bristol, Avon). 2003;18(3):231–6.
Liau JJ, Cheng CK, Huang CH, Lo WH. The effect of malalignment on stresses in polyethylene component of total knee prostheses–a finite element analysis. Clin Biomech (Bristol, Avon). 2002;17(2):140–6.
Schubert R, Zietz C, Bergschmidt P, Fabry C, Bader R. Wear simulator study of malaligned TiN-coated vs. uncoated metallic femoral components of a bicondylar knee endoprosthesis. 15th EFORT Congress, London, UK, 2014: EFORT14-1388.
D’Lima DD, Hermida JC, Chen PC, Colwell CW. Polyethylene wear and variations in knee kinematics. Clin Orthop Relat Res. 2001;392:124–30.
Weber P, Schröder C, Utzschneider S, Schmidutz F, Jansson V, Müller PE. Does increased tibial slope reduce the wear rate of unicompartmental knee prostheses? An in vitro investigation. Orthopade. 2012;41(4):298–302.
Davidson JA, Poggie RA, Mishra AK. Abrasive wear of ceramic, metal, and UHMWPE bearing surfaces from third-body bone, PMMA bone cement, and titanium debris. Biomed Mater Eng. 1994;4(3):213–29.
Wang A, Schmidig G. Ceramic femoral heads prevent runaway wear for highly crosslinked polyethylene acetabular cups by third-body bone cement particles. Wear. 2003;255(7–12):1057–63.
Jones VC, Williams IR, Auger DD, Walsh W, Barton DC, Stone MH, Fisher J. Quantification of third body damage to the tibial counterface in mobile bearing knees. Proc Inst Mech Eng H. 2001;215(2):171–9.
Morscher EW, Hefti A, Aebi U. Severe osteolysis after third-body wear due to hydroxyapatite particles from acetabular cup coating. J Bone Joint Surg Br. 1998;80(2):267–72.
Minakawa H, Stone MH, Wroblewski BM, Lancaster JG, Ingham E, Fisher J. Quantification of third-body damage and its effect on UHMWPE wear with different types of femoral head. J Bone Joint Surg Br. 1998;80(5):894–9.
DeBaets T, Waelput W, Bellemans J. Analysis of third body particles generated during total knee arthroplasty: is metal debris an issue? Knee. 2008;15:95–7.
Niki Y, Matsumoto H, Otani T, Tomatsu T, Toyama Y. How much sterile saline should be used for efficient lavage during total knee arthroplasty? Effects of pulse lavage irrigation on removal of bone and cement debris. J Arthroplasty. 2007;22:95–9.
Gotterson PR, Nusem I, Pearcy MJ, Crawford RW. Metal debris from bony resection in knee arthroplasty–is it an issue? Acta Orthop. 2005;76(4):475–80.
Hauptmann SM, Weber P, Glaser C, Birkenmaier C, Jansson V, Muller PE. Free bone cement fragments after minimally invasive unicompartmental knee arthroplasty: an underappreciated problem. Knee Surg Sports Traumatol Arthrosc. 2008;16(8):770–5.
Muratoglu OK, Burroughs BR, Bragdon CR, Christensen S, Lozynsky A, Harris WH. Knee simulator wear of polyethylene tibias articulating against explanted rough femoral components. Clin Orthop Relat Res. 2004;428:108–13.
Zietz C, Bergschmidt P, Lange R, Mittelmeier W, Bader R. Third-body abrasive wear of tibial polyethylene inserts combined with metallic and ceramic femoral components in a knee simulator study. Int J Artif Organs. 2013;36(1):47–55.
Schroeder C, Grupp TM, Fritz B, Schilling C, Chevalier Y, Utzschneider S, Jansson V. The influence of third-body particles on wear rate in unicondylar knee arthroplasty: a wear simulator study with bone and cement debris. J Mater Sci Mater Med. 2013;24(5):1319–25.
Acknowledgments
We kindly thank Mrs. Regina Lange from the Institute of Electronic Appliances and Circuits, University of Rostock for preparation of the FESEM image (Fig. 10).
Conflict of interest
The authors declare that there is no conflict of interests regarding the publication of this paper.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Zietz, C., Reinders, J., Schwiesau, J. et al. Experimental testing of total knee replacements with UHMW-PE inserts: impact of severe wear test conditions. J Mater Sci: Mater Med 26, 134 (2015). https://doi.org/10.1007/s10856-015-5470-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10856-015-5470-y