
Abstract
Purpose
The aim was to evaluate mtDNA content and its dynamics in euploid and aneuploid embryos from cleavage to blastocyst stage following consecutive biopsies. The effect of female age on mtDNA content was evaluated by comparing reproductively younger (≤ 37 years) with older (> 37 years) women.
Methods
A retrospective single-centre descriptive study was performed between August 2016 and January 2017. Forty patients, with 112 embryos, undergoing preimplantation genetic testing for aneuploidies (PGT-A) by next-generation sequencing (NGS) were included. Embryos that reached the blastocyst stage and were not selected for fresh embryo transfer were included following consecutive biopsies of a single blastomere on day 3 and trophectoderm biopsy of day 5 blastocysts.
Results
Cleavage-stage mtDNA was significantly lower in fast cleaving embryos (p = 0.016). Based on the concordance between day 3 and day 5 biopsies, a difference was identified in blastocyst mtDNA content between groups (p = 0.019); true euploid blastocysts presented a lower mtDNA content. No association was identified between cleavage-stage mtDNA content and ploidy status (OR 1.008 [0.981–1.036], p = 0.565) nor between blastocyst mtDNA content and ploidy outcome (OR 0.954 [0.898–1.014], p = 0.129). No difference was found when comparing mtDNA content and ploidy outcome between the two reproductive age groups (p = 0.505 (cleavage stage) and p = 0.774 (blastocyst)).
Conclusion
Mitochondrial DNA content of cleavage-stage embryos and blastocysts is unable to predict ploidy status. Subgroup analysis based on ploidy concordance between day 3 and day 5 revealed a significantly lower mtDNA content for true euploid blastocysts. Reproductive ageing does not affect mtDNA content.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Human reproduction is known to be a highly inefficient process with only a small proportion of fertilized oocytes resulting in a live birth [1]. For assisted reproductive techniques (ART), controlled ovarian stimulation has been used to increase the chance of a live birth per cycle by generating multiple oocytes. The generated cohort of oocytes is characterized by differences in developmental competence that has been attributed to variations in mitochondrial DNA (mtDNA) content [2]. It is well established that oocyte mitochondrial copy numbers show a high inter-patient variability as well as a variability among oocytes from the same patient.
During foetal development, mitochondria start to replicate leading to oogonial cells with around 200 mitochondrial organelles [3]. Mitochondria continue to replicate during oocyte maturation and the mature metaphase II oocyte contains around 100,000 mitochondria and between 50,000 and 550,000 mtDNA copies [4, 5]. The mtDNA is a 16.6-kb circular double-stranded molecule, located in the inner mitochondrial membrane and encodes 13 gene products required for electron transport and oxidative phosphorylation. This makes the mature human oocyte not only the biggest cell in the body but also the richest cell in terms of mtDNA content.
As mitochondrial replication will only occur around the time of implantation and mtDNA replication will only start after blastocyst formation, the initial oocytes’ mtDNA content is one of the most important determinants of the preimplantation developmental capacity [2, 6]. Presence of high mtDNA copy numbers in cumulus cells is a strong predictor of preimplantation development [7, 8]; hence, an increased fertilization potential has also been observed in oocytes with a higher mtDNA content [4, 9]. During the initial mitotic divisions, the mtDNA content is thought to remain stable as the oocyte’s mitochondria and mtDNA are equally distributed to the resulting blastomeres based on their volume [10, 11]. On the other hand, major differences in mtDNA content between the 8 blastomeres of a single embryo have also been observed [12]. Currently, cleavage-stage mtDNA is unable to predict the ploidy status of embryos [13, 14], while the implantation potential of euploid embryos decreases with increasing mtDNA levels [15].
Only 2 to 3 days after the embryonic genome activation and after the first differentiation into trophectoderm (TE) and inner cell mass (ICM), the mtDNA will start to replicate in the expanded blastocyst; first, in the TE cells and only later, in the ICM cells [16, 17]. At this juncture, it is unclear if blastocyst mtDNA is able to predict ploidy status, as conflicting results have been described [14, 18,19,20]. Deficiencies in the cellular bioenergetic capacity and suboptimal ATP production by the mitochondria have been suggested to adversely affect pregnancy rates despite transfer of euploid blastocysts [2]. In addition, studies have suggested that increased mtDNA levels are associated with implantation failure [15, 18, 21, 22] but not all studies concur [20, 23].
The observed inconsistencies in mtDNA content of cleavage-stage embryos and blastocysts can be attributed to multiple factors (age, diminished ovarian reserve, stimulation protocol, BMI and smoking) that are known to affect mtDNA content at different stages of development [2, 8, 18, 19, 24,25,26,27,28]. At present, the relationship between mtDNA content and ploidy status at cleavage and blastocyst stage of embryo development remains unclear. Therefore, we performed a retrospective descriptive study to evaluate mtDNA content and its dynamics in euploid and aneuploid embryos as determined by consecutive biopsies from cleavage-stage day 3 embryos and blastocysts on day 5.
Material and methods
Approval for this study was obtained from the local Ethics Committee of IVIRMA Middle East Fertility Clinic, Abu Dhabi, UAE (Research Ethics Committee IVI-MEREF010/2017/REFA009). All patients signed a consent form allowing additional trophectoderm biopsy of supernumerary euploid and aneuploid embryos not selected for transfer. This study is part of a validation study designed to ascertain the concordance rates of chromosomal status and mtDNA content between cleavage-stage biopsy on day 3 and trophectoderm biopsy on day 5. This study was permissible as the law of the United Arab Emirates (UAE) governing ART prohibits cryopreservation of supernumerary embryos.
Study design
This retrospective descriptive study was performed at IVI RMA Middle East Fertility Clinic, Abu Dhabi, between August 2016 and January 2017. A total of 112 embryos from 40 patients undergoing preimplantation genetic testing for aneuploidies (PGT-A) by next-generation sequencing (NGS) were included. Only information from embryos reaching the blastocyst stage and not selected for fresh embryo transfer was included following two consecutive biopsies: a single blastomere biopsy on day 3 cleavage-stage embryos and trophectoderm biopsy on day 5 blastocysts. After blastomere biopsy and extended culture to day 5, euploid blastocysts not selected for fresh embryo transfer and aneuploid blastocysts were subjected to an additional trophectoderm biopsy, to evaluate the dynamics in mtDNA content between cleavage stage and blastocyst biopsies and to validate the chromosomal status between day 3 and day 5 biopsies. The effect of female age on mtDNA content was evaluated by comparing reproductively younger (≤ 37 years) women with reproductively older (> 37 years) women [18]. Additionally, pregnancy outcomes after fresh euploid day 5 transfers were correlated to the cleavage-stage mtDNA content after single blastomere biopsy on day 3. Full implantation was defined as the presence of a gestational sac on ultrasound scan for all transferred embryos (one sac for a single embryo transfer (SET) and two sacs after double embryo transfer (DET)). Failed implantation was described as the absence of any gestational sac after SET or DET. In case only one gestational sac was observed after DET, we were unable to assign the correct mtDNA content to the implanted embryo and therefore, these pregnancies were excluded from the analysis.
Ovarian stimulation protocols
Ovarian stimulation was performed by standard protocols, either gonadotropin-releasing hormone (GnRH) agonist or GnRH antagonist protocols, using recFSH (recombinant follicle-stimulating hormone) or HMG (human menopausal gonadotropin) as stimulation medication. The dosage of the stimulation medication was chosen according to the ovarian reserve parameters [29]. Trigger for final oocyte maturation was achieved by administration of either 5000–10,000 IU of hCG, 0.3 mg of GnRH agonist (triptorelin) or dual trigger (hCG and GnRH-analogue), as soon as ≥ 3 follicles ≥ 17 mm were present. Oocyte retrieval was carried out 36 h after trigger for final oocyte maturation.
Embryo culture and embryo biopsy
Four hours after oocyte retrieval, mature oocytes were subjected to intracytoplasmic sperm injection (ICSI) [30]. Embryos were cultured in Quinn’s Advantage Sequential medium, (SAGE, Målov, Denmark), using trigas incubators (6% CO2, 5% O2, 89% N2). Fertilization was assessed 17–20 h post-ICSI, and embryo development was recorded every 24 h until the day of embryo transfer. On day 3, embryos with ≥ 5 nucleated blastomeres and < 25% fragmentation were biopsied. Cleavage-stage embryos were placed in a droplet containing Ca2+/Mg2+-free medium (G-PGD, Vitrolife, Göteborg, Sweden/LifeGlobal, Guilford, CT), the zona pellucida was perforated by laser pulses (OCTAX, Herborn, Germany) and a single blastomere was withdrawn from each embryo and placed in 0.2 mL of PCR tubes containing 2 μL PBS. For blastomere washing and handling, 1% polyvinylpyrrolidone (PVP) was used. For trophectoderm biopsy, expanded and hatching blastocysts were biopsied using Quinn’s Advantage Medium with HEPES, (SAGE, Målov, Denmark) supplemented with HSA, (Vitrolife, Göteborg, Sweden). Three to five laser pulses were used to cut the trophectoderm cells inside the aspiration pipette; trophectoderm biopsies were washed and placed in 0.2 mL of PCR tubes containing 2 μL PBS.
Ploidy status of cleavage-stage embryos and blastocysts by NGS
A whole genome amplification (WGA) protocol was performed on all individual samples (PicoPlex technology by Rubicon Genomics, Inc.; Ann Arbor, MI, USA). After WGA, library preparation consisted of the incorporation of individual barcodes for the amplified DNA of each embryo. After isothermal amplification and enrichment, sequencing was performed in a 316 or 318 chip using the Personal Genome Machine sequencing (Life-Thermo Fisher, USA). For sequencing analysis and data interpretation, Ion Reporter software was employed. Embryos were diagnosed as euploid or aneuploid. Mosaicism above 70% was classified as abnormal and mosaicism between 30 and 70% was considered as mosaic embryos. In the case of a result indicating mosaicism, the embryo was classified as “euploid” when the extent of mosaicism was below 30% and as “aneuploid” when the extent of mosaicism was above 30%, as mosaic embryos were never transferred. Chaotic embryos were defined as those showing a complex pattern of aneuploidies, involving more than six chromosomes. The herein used NGS platform has been validated in previous studies [31, 32] and is commercially available. Ploidy refers to the diagnosis of the embryos after NGS: euploid or aneuploid.
Mitochondrial DNA copy number analysis
Relative values of mitochondrial DNA were directly obtained from the software and were analyzed using the Igenomix algorithm for day 3 and day 5 biopsies. For the mtDNA content calculation, an optimized algorithm was applied using the output dataset obtained from the PGT-A analysis that comprises a mixture of mtDNA reads and nuclear DNA (nDNA) reads. To calculate the relative mtDNA copy number score or mtDNA content, the number of reads after filtering mapping to the mitochondrial genome is divided by the number of reads mapping to the nuclear DNA [33]. This allows normalization of each batch and therefore reduces variability during NGS experiments as it makes the calculation independent of the number of cells obtained in each biopsy. Crucially, using nDNA values for normalization assumes that the composition of nDNA is equal across samples. Only embryos with informative results for the PGT-A and mtDNA content below 1000 were analyzed in the study (mtDNA contents above that value were considered as outliers). This technique has been validated internally by Igenomix.
Statistical analysis
Data concerning categorical and continuous variables were expressed as proportions and means with 95% confidence intervals (95%CI), standard deviations (SD) or ranges, unless stated otherwise. Categorical data were compared using chi-square analysis and Fisher’s exact test, where appropriate. Continuous data were compared with the Student t test and Wilcoxon signed-rank test when appropriate. Pairing for the pre-post comparisons of non-independent data was applied. Categorical variables were compared using general linear model (Wilks’ lambda test). Non-parametric tests were employed when sample size was below 30 cases, based on the central limit theorem. A Kruskal-Wallis test was applied for the overall comparisons, and then Mann-Whitney’s U in one-to-one comparisons.
A p value less than 0.05 was considered statistically significant. All statistical analyses were performed using the Statistical Package for Social Sciences, version 23 (SPSS Inc., Chicago, IL, USA). Statistical analysis of the final mtDNA values utilized unpaired two-tailed t tests. Parameters which were compared during this study included female age, comparing reproductively younger (≤ 37 years) women with reproductively older (> 37 years) women and embryo chromosomal status (euploid versus aneuploid). For the day 3 mtDNA values, a correction was made for the number of mitotic divisions that had appeared from the time of syngamy onwards (slow cleaving embryos who underwent 3 mitotic divisions and fast cleaving embryos who underwent 4 mitotic divisions). As the smallest mononucleated blastomere was selected for biopsy, the number of mitotic divisions provides a good estimation of the size of the biopsied blastomere in case equal cytoplasmic divisions occurred. Also, to compensate for potential mtDNA loss induced by cytoplasmic depletion due to fragmentation, a correction was made for the degree of fragmentation (no fragmentation, 0–10% fragmentation, 10–25% fragmentation) present in the cleavage-stage embryo at the time of biopsy. For day 5 embryos, a correction was made for the blastocyst expansion stage (minor expansion, expanded, fully expanded or hatched).
Results
Forty patients had a total of 112 supernumerary euploid or aneuploid blastocysts available for rebiopsy on day 5. The indications for performing a PGT-A analysis are depicted in Table 1. The mean female age was 33.2 ± 6.5 years [range 24–46 years] and on average 2.8 ± 1.9 supernumerary blastocysts were rebiopsied on day 5 after initial biopsy on day 3.
Day 3 cleavage-stage biopsy resulted in 46 (41.1%) euploid embryos and 66 (58.9%) aneuploid embryos. The mean mtDNA contents of euploid (51.5 [47.6–55.4]) and aneuploid embryos (49.9 [46.4–53.5]) were not significantly different (p = 0.568) (Fig. 1). Logistic regression was unable to find an association between the cleavage-stage mtDNA content and ploidy status on day 3 (OR 1.008 [0.981–1.036], p = 0.565) and remained non-significant after adjusting for the degree of fragmentation as a potential predictive factor (OR 1.012 [0.983–1.042], p = 0.415). However, when testing the association between mitochondrial DNA and the number of mitotic divisions, a statistically significant difference was found (p = 0.016).

Box and whisker plot of mtDNA content between euploid and aneuploid embryos
Day 5 trophectoderm biopsies revealed 61 (54.6%) euploid and 51 (45.5%) aneuploid blastocysts. The mean mtDNA content of euploid (20.5 [18.9–22.2]) and aneuploid blastocysts (22.4 [20.6–24.2]) were not significantly different (p = 0.124) (Fig. 1). There was no relationship between blastocyst mtDNA content and ploidy outcome (OR 0.954 [0.898–1.014], p = 0.129), even after taking into consideration the expansion stage of the blastocyst (OR 0.962 [0.904–1.024], p = 0.221).
Discrepancies were observed in ploidy status between day 3 and day 5 biopsies: of the 46 euploid cleavage-stage embryos, 45 (97.8%) were also euploid after TE biopsy, while for the aneuploid embryos, only 50/66 (75.8%) were concordant between cleavage stage and TE biopsy. As blastocyst biopsy is well recognized to be preferable to cleavage-stage biopsy in terms of accuracy, blastocyst ploidy status was used when determining the relationship between ploidy status and cleavage-stage mtDNA content. Based on this allocation, day 3 mtDNA content was not significantly different between euploid and aneuploid embryos: 47.9 ± 10.8 and 52.8 ± 15.7 respectively (p = 0.062). mtDNA content of cleavage-stage embryos and blastocysts was compared based on the concordance of the ploidy status between day 3 and day 5 (Table 2 comparing the different groups, Fig. 2 for individual embryo dynamics). While there was no difference in the mtDNA content between all groups on day 3 (p = 0.597), a significant difference was found between groups on day 5 (p = 0.019). More specifically, “aneuploid day 3-aneuploid day 5” embryos had a significantly higher blastocyst mtDNA content compared with “aneuploid day 3-euploid day 5” embryos (p = 0.002) while “aneuploid day 3-euploid day 5” embryos had a significantly lower blastocyst mtDNA content compared with “euploid day 3-euploid day 5” embryos (p = 0.027). The mtDNA dynamics between cleavage-stage embryos and blastocysts, based on the ploidy concordance, is presented in Fig. 3.

Box and whisker plot of mtDNA content based on concordances between day 3 and day 5

mtDNA dynamics between cleavage-stage embryos and blastocysts. mtDNA content of day 3 and day 5 embryos based on the ploidy concordance between both days. Each line represents one embryo
When the young (30.0 ± 4.1 [20–37]) and older (41.3 ± 2.1 [39–46]) reproductive age groups were compared, no significant difference was found in mtDNA content, both at the cleavage stage (p = 0.505) and at the blastocyst stage (p = 0.774) (Table 3). Also, the mtDNA content at the cleavage stage was not different between euploid and aneuploid embryos for younger (p = 0.918) or older (p = 0.258) women and similar results were obtained for the blastocyst mtDNA content: p = 0.208 and p = 0.097, respectively.
Additional information regarding day 3 mtDNA content and full and failed implantations is presented in Supplementary Table 1. Of the 40 patients, five (43.4 ± 2.4 years) did not receive a fresh embryo transfer as no euploid embryos were available, while 35 (31.7 ± 5.4 years) received a single (n = 11) or double (n = 24) embryo transfer of which 7 (1 patient with unknown outcome) and 15, respectively, resulted in a pregnancy. Full implantations (number of gestational sacs equals number of embryos transferred) were obtained for 7/7 (SET) and 6/15 (DET) pregnant patients.
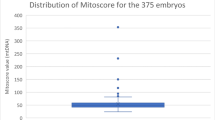
Discussion
Few studies have previously evaluated the effect of cleavage-stage mtDNA on the ploidy status of the corresponding embryo and all prior studies concur with our findings in that an association between both parameters was not identified [13, 14]. Moreover, mtDNA content is not a predictive factor in the identification of embryos which will progress to blastocyst stage or arrest during development [14]. Similar results were obtained in a recent study in our centre in which 375 day 3 embryos were stratified according to a low (≤ 49) and a high (> 49) mtDNA content (unpublished data) substantiating the results obtained in the current study. While the above studies all demonstrate no association between mtDNA content of cleavage-stage blastomeres and ploidy status, the evidence regarding mtDNA content and implantation potential of the embryo is inconsistent [15, 34]. When analyzing the mtDNA of cleavage-stage blastomeres, a decreasing implantation potential was observed with increasing mtDNA levels of 205 euploid embryos [15]. Contrarily, when a mtDNA/gDNA ratio was measured in spent culture media of cleavage-stage embryos, a significantly higher mtDNA/genomic DNA ratio was observed in embryos able to grow to blastocyst stage on day 5 and in blastocysts resulting in successful implantation [34]. The measured mtDNA value in the secretome would mirror the high mtDNA content present in a highly competent oocyte that is able to fuel fertilization and embryonic genome activation. When this is extended to cleavage-stage embryos however, a high mtDNA value is expected for embryos with a high implantation potential. Very much the opposite of the results obtained by Diez-Juan and colleagues [15] and not concurring with the obtained implantation results in this study. Thus, day 3 mtDNA content and spent culture media on day 3 show highly conflicting results with regard to their ability to predict embryo implantation potential.
Even though mtDNA will be evenly split between the blastomeres upon each cell division based on the blastomere volume [11], it has been shown that there is a high discrepancy in mtDNA load between the different blastomeres from the same embryo [12], indicating that blastomere volume could be directly proportional to mtDNA copy numbers [35, 36]. As blastomeres with a larger cytoplasmic volume, representing slower cleaving embryos, contain more mtDNA copies, a direct correlation between mtDNA and a day 3 blastomere could be possible by measuring the blastomere cytoplasmic diameter at the time of the biopsy. As this diameter was not measured in the present study, a correction was made for the number of mitotic divisions and the degree of fragmentation. As expected, the number of mitotic divisions affects mtDNA content at the cleavage stage (p = 0.016), which corresponds with the mitochondrial split between blastomeres based on their cell volume [11]. As only embryos with < 25% fragmentation were accepted for blastomere biopsy, the degree of fragmentation did not affect mtDNA content.
In contrast to the limited data available on day 3 cleavage-stage embryos, mtDNA content at the blastocyst stage has been more extensively studied, although generating inconsistent results. Even if increased mtDNA levels have been linked to aneuploidy [14, 18, 19], our study was consistent with that of Viktor and colleagues [20] in that it failed to discriminate euploid from aneuploid embryos based on the mtDNA content alone. Discrepant results were obtained when analyzing mtDNA content of implanting euploid blastocysts [15, 18, 20,21,22,23]. Unfortunately, implantation potential of the biopsied blastocysts could not be included as part of this study as the transferred blastocyst did not undergo a second biopsy at the blastocyst stage. Mitochondrial biogenesis induced by energetic stress has been proposed in an attempt to explain increased mtDNA content in blastocysts that fail to implant [15]. When compared with earlier biogenesis, higher mtDNA levels have been linked to poorer TE samples in which less cell divisions occurred, thus following a simple mathematical model [19]. However, as mtDNA replication is thought to start in the TE of the expanded blastocyst in order to respond to the high energy demand necessary for proliferation and implantation [6], higher mtDNA levels are expected in fully expanded blastocysts with grade A trophectoderm. This indicates that the mtDNA per cell probably remains constant from the expanded blastocyst onwards due to a balanced mtDNA replication. Though it should be used with caution, compared with cleavage-stage mtDNA content, blastocyst mtDNA content appears to be a stronger predictor of pregnancy [15, 21, 22, 37].
The behaviour of mtDNA content has been investigated in a very limited number (n = 50) of frozen-thawed zygotes that were further cultured to embryos undergoing consecutive biopsies on day 3 and day 6 of development [4]. While cleavage-stage mtDNA was also equal between euploid and aneuploid embryos, euploid blastocysts had a significantly lower mtDNA content. However, this study did not investigate the dynamics between discordant and concordant cleavage-stage and blastocyst mtDNA content. We identified that true euploid blastocysts (euploid-euploid or aneuploid-euploid) had a significantly lower mtDNA content compared with aneuploid-aneuploid embryos highlighting the importance of cautiously interpreting day 3 mtDNA content based on ploidy outcome. It is unclear how slow freezing of zygotes impacts mitochondria and mtDNA content of embryos and how these results can be extrapolated to embryos originating from fresh oocytes.
Female age has been proposed as one of the most important factors affecting embryonic mtDNA levels [18, 27, 28] with significant increases in mtDNA content occurring with advanced maternal age. Fragouli and colleagues [18] demonstrated that a significantly higher mtDNA content is associated with reproductively older women, a phenomenon that was also apparent when stratifying according to ploidy outcome. In contrast, significantly lower mtDNA content levels were obtained in blastomeres from reproductively younger women. When cleavage-stage or blastocyst mtDNA content was stratified according to these different age categories in our study, even after subgroup analysis for ploidy outcome, we did not observe any difference between both age groups. If the mtDNA content would be affected by age, it should be more pronounced in this study because of a higher age difference (30 versus 34 years and 41 versus 39 years). However, the low number of study participants may explain the absence of a difference in the study outcomes between the 2 age groups.
While the restrictions in cryopreservation of supernumerary embryos allowed us to perform rebiopsy of euploid blastocysts that were not selected for transfer, the second biopsy at the blastocyst stage was limited to those embryos with capability to develop into expanded blastocysts. As euploid embryos show a higher tendency to develop into blastocysts and not all aneuploidies are able to develop into blastocysts, cleavage-stage mtDNA content of aneuploid embryos may be biassed as only embryos that were able to develop into good-quality expanded blastocysts able to undergo additional TE biopsy were included. Inclusion of mtDNA content of aneuploid cleavage-stage embryos that fail to cavitate could therefore reveal different mtDNA content based on the ploidy status. Also, the best-quality euploid embryos were transferred on day 5 and therefore not included in the analysis. The two consecutive biopsies on cleavage-stage embryos and blastocysts are unique as they facilitate the evaluation of dynamics in ploidy status and mtDNA content between both preimplantation stages. The depletion of embryonic mass by performing a single blastomere biopsy on day 3 does not appear to be detrimental for further embryo development or implantation potential [38]. However, this single blastomere biopsy also coincides with a 5–20% reduction in mtDNA—depending on the cell stage and volume of the blastomere—which could lead to a reduced blastocyst mtDNA. We also acknowledge that the small sample size of this study may limit the validity of general interpretations.
The most accurate technique for the detection of the mtDNA content is RT-PCR using selected mtDNA regions and nuclear genes [15, 18]. Other recent studies obtained the mtDNA content by dividing the total number of reads of mtDNA and all nuclear DNA reads after low coverage NGS, as is the case in this study. Although it is not the optimal technique to estimate the mtDNA content (variability attributed to the biopsy quality and WGA amplification protocol), an internally validated correction model was applied to calculate the mtDNA content. These biases may explain differences with previous RT-PCR studies, implying that the mtDNA content obtained after NGS should be taken carefully, even if the same technique was used on both biopsies of the same embryo.
Embryonic mosaicism of day 3 biopsies is known to be high. This is an important barrier to the true ploidy status and the resulting mtDNA content [39], reflected in the high discordance rate of the 66 aneuploid day 3 embryos of which 16 (24.2%) were euploid at the blastocyst stage. However, even when the blastocyst ploidy status is set as the true ploidy status, day 3 mtDNA content was still unable to discriminate between euploid and aneuploid embryos. This mosaicism is not only present on day 3 since TE biopsies are also prone to a degree of mosaicism [40, 41], reflected in the variability of mtDNA content [39]. Although its incidence has been reported to range from 23 to 33% depending on the embryo stage at biopsy and the genetic platform [42,43,44], recent evidence points towards diminished rates of mosaicism (5–10%) in trophectoderm biopsies (PGDIS 2019, Geneva).
In conclusion, mtDNA content of cleavage-stage embryos and blastocysts is unable to predict ploidy status. Cleavage-stage mtDNA content is lower in fast-dividing embryos. Subgroup analysis based on ploidy concordance between day 3 and day 5 revealed a significantly lower mtDNA content for euploid blastocysts. Reproductive ageing seems not to affect mtDNA content.
References
Edwards RG. Causes of early pregnancy loss. Hum Reprod. 1986;1(3):185–98.
Van Blerkom J. Mitochondrial function in the human oocyte and embryo and their role in developmental competence. Mitochondrion. 2011;11:797–813.
Eichenlaub-Ritter U, Wieczorek M, Lüke S, Seidel T. Age related changes in mitochondrial function and new approaches to study redox regulation in mammalian oocytes in response to age or maturation conditions. Mitochondrion. 2011;11(5):783–96.
Reynier P, May-Panloup P, Chretien MF, Morgan CJ, Jean M, Savagner F, et al. Mitochondrial DNA content affects the fertilizability of human oocytes. Mol Hum Rep. 2001;7:425–9.
May-Panloup P, Chrétien MF, Jacques C, Vasseur C, Malthièry Y, Reynier P. Low oocyte mitochondrial DNA content in ovarian insufficiency. Hum Reprod. 2005;20(3):593–7.
Seli E. Mitochondrial DNA as a biomarker for in-vitro fertilization outcome. Curr Opin Obstet Gynecol. 2016;28(3):158–63.
Ogino M, Tsubamoto H, Sakata K, Oohama N, Hayakawa HM, Kojima T, et al. Mitochondrial DNA copy number in cumulus cells is a strong predictor of obtaining good-quality embryos after IVF. J Assist Reprod Genet. 2016;33(3):367–71.
Desquiret-Dumas Desquiret-Dumas V, Clément A, Seegers V, Boucret L, Ferré-L’Hotellier V, Bouet PE, et al. The mitochondrial DNA content of cumulus granulosa cells is linked to embryo quality. Hum Reprod. 2017;32(3):607–14.
Santos TA, El Shourbagy S, St John JC. Mitochondrial content reflects oocyte variability and fertilization outcome. Fertil Steril. 2006;85(3):584–91.
Cecchino GN, Garcia-Velasco JA. Mitochondrial DNA copy number as a predictor of embryo viability. Fertil Steril. 2018:0015–282.
Hashimoto S, Morimoto N, Yamanaka M, Matsumoto H, Yamochi T, Goto H, et al. Quantitative and qualitative changes of mitochondria in human preimplantation embryos. J Assist Reprod Genet. 2017;34(5):573–80.
Lin DP, Huang CC, Wu HM, Cheng TC, Chen CI, Lee MS. Comparison of mitochondrial DNA contents in human embryos with good or poor morphology at the 8-cell stage. Fertil Steril. 2004;81(1):73–9.
Shang W, Zhang Y, Shu M, Wang W, Ren L, Chen F, et al. Comprehensive chromosomal and mitochondrial copy number profiling in human IVF embryos. Reprod BioMed Online. 2018;36(1):67–74.
Ho JR, Arrach N, Rhodes-Long K, Salem W, McGinnis LK, Chung K, et al. Blastulation timing is associated with differential mitochondrial content in euploid embryos. J Assist Reprod Genet. 2018;35(4):711–20.
Diez-Juan A, Rubio C, Marin C, Martinez S, Al-Asmar N, Riboldi M, et al. Mitochondrial DNA content as a viability score in human euploid embryos: less is better. Fertil Steril. 2015;104(3):534–41.
Van Blerkom J. Mitochondria as regulatory forces in oocytes, preimplantation embryos and stem cells. Reprod BioMed Online. 2008;16(4):553–69.
St John JC, Facucho-Oliveira J, Jiang Y, et al. Mitochondrial DNA transmission, replication and inheritance: a journey from the gamete through the embryo and into offspring and embryonic stem cells. Hum Reprod Update. 2010;16:488–509.
Fragouli E, Spath K, Alfarawati S, Kaper F, Craig A, Michel CE, et al. Altered levels of mitochondrial DNA are associated with female age, aneuploidy, and provide an independent measure of embryonic implantation potential. PLoS Genet. 2015;11:e1005241.
de los Santos MJ, Diez-Juan A, Mifsud A, Mercader A, Meseguer M, Rubio C, et al. Variables associated with mitochondrial copy number in human blastocysts: what can we learn from trophectoderm biopsies? Fertil Steril. 2018;109(1):110–7.
Victor AR, Brake AJ, Tyndall JC, Griffin DK, Zouves CG, Barnes FL, et al. Accurate quantitation of mitochondrial DNA reveals uniform levels in human blastocysts irrespective of ploidy, age, or implantation potential. Fertil Steril. 2017;107(1):34–42.
Ravichandran K, McCaffrey C, Grifo J, Morales A, Perloe M, Munne S, et al. Mitochondrial DNA quantification as a tool for embryo viability assessment: retrospective analysis of data from single euploid blastocyst transfers. Hum Reprod. 2017;32(6):1282–92.
Fragouli E, McCaffrey C, Ravichandran K, Spath K, Grifo J, Munne S, et al. Clinical implications of mitochondrial DNA quantification on pregnancy outcomes: a blinded prospective non-selection study. Hum Reprod. 2017;32(11):2340–7.
Klimczak AM, Pacheco LE, Lewis KE, Massahi N, Richards JP, Kearns WG, et al. Embryonal mitochondrial DNA: relationship to embryo quality and transfer outcomes. J Assist Reprod Genet. 2018;35(5):871–7.
Fragouli E, Wells D. Mitochondrial DNA assessment to determine oocyte and embryo viability. Semin Reprod Med. 2015;33:401–9.
Cree LM, Hammond ER, Shelling AN, Berg MC, Peek JC, Green MP. Maternal age and ovarian stimulation independently affect oocyte mtDNA copy number and cumulus cell gene expression in bovine clones. Hum Reprod. 2015;30(6):1410–20.
Boucret L, de la Barca JM C, Morinière C, Desquiret V, Ferré-L’Hôttelier V, Descamps P, et al. Relationship between diminished ovarian reserve and mitochondrial biogenesis in cumulus cells. Hum Reprod. 2015;30(7):1653–64.
Babayev E, Seli E. Oocyte mitochondrial function and reproduction. Curr Opin Obstet Gynecol. 2015;27(3):175–81.
Treff NR, Zhan Y, Tao X, Olcha M, Han M, Rajchel J, et al. Levels of trophectoderm mitochondrial DNA do not predict the reproductive potential of sibling embryos. Hum Reprod. 2017;32(4):954–62.
La Marca A, Sunkara SK. Individualization of controlled ovarian stimulation in IVF using ovarian reserve markers: from theory to practice. Hum Reprod Update. 2014;20(1):124–40.
Steirteghem V, Nagy Z, Joris H, Liu J, Staessen C, Smitz J, et al. High fertilization and implantation rates after intracytoplasmic sperm injection. Hum Reprod. 1993;8(7):1061–6.
Wells D, Kaur K, Grifo J, Glassner M, Taylor JC, Fragouli E, et al. Clinical utilisation of a rapid low-pass whole genome sequencing technique for the diagnosis of aneuploidy in human embryos prior to implantation. J Med Genet. 2014;51(8):553–62.
Kung A, Munné S, Bankowski B, Coates A, Wells D. Validation of next-generation sequencing for comprehensive chromosome screening of embryos. Reprod BioMed Online. 2015;31(6):760–9.
Phillips NR, Sprouse ML, Roby RK. Simultaneous quantification of mitochondrial DNA copy number deletion ratio: a multiplex real-time PCR assay. SciRep. 2014;4:3887.
Stigliani S, Persico L, Lagazio C, Anserini P, Venturini PL, Scaruffi P. Mitochondrial DNA in day 3 embryo culture medium is a novel, non-invasive biomarker of blastocyst potential and implantation outcome. Mol Hum Reprod. 2014;20(12):1238–46.
Van Blerkom J, Davis P, Alexander S. Differential mitochondrial distribution in human pronuclear embryos leads to disproportionate inheritance between blastomeres: relationship to microtubular organisation, ATP content and competence. Hum Reprod. 2000;15(12):2621–33.
Murakoshi Y, Sueoka K, Takahashi K, Sato S, Sakurai T, Tajima H, et al. Embryo developmental capability and pregnancy outcome are related to the mitochondrial DNA copy number and ooplasmic volume. J Assist Reprod Genet. 2013;30(10):1367–75.
Wells D. Mitochondria DNA quantity as a biomarker for blastocyst implantation potential. Fertil Steril. 2017;108(5):742–7.
Cimadomo D, Capalbo A, Ubalid FM, Scarica C, Palagiano A, Cnaipari R, et al. The impact of biopsy on human embryo developmental potential during preimplantation genetic diagnosis. Biomed Res Int. 2016;2016:7193075.
Capalbo A, Rienzi L. Mosaicism between trophectoderm and inner cell mass. Fertil Steril. 2017;107(5):1098–106.
Munné S, Wells D. Detection of mosaicism at blastocyst stage with the use of high-resolution next-generation sequencing. Fertil Steril. 2017;107:1085–91.
Gleicher N, Metzger J, Croft G, Kushnir VA, Albertini DF, Barad DH. A single trophectoderm biopsy at blastocyst stage is mathematically unable to determine embryo ploidy accurately enough for clinical use. Reprod Biol Endocrinol. 2017;15(1):33.
Northrop LE, Treff NR, Levy B, Scott RT Jr. SNP microarray based 24 chromosome aneuploidy screening demonstrates that cleavage stage FISH poorly predicts aneuploidy in embryos that develop to morphologically normal blastocysts. Mol Hum Reprod. 2010;16:590–600.
Capalbo A, Wright G, Elliott T, Ubaldi FM, Rienzi L, Nagy ZP. FISH reanalysis of inner cell mass and trophectoderm samples of previously array-CGH screened blastocysts shows high accuracy of diagnosis and no major diagnostic impact of mosaicism at the blastocyst stage. Hum Reprod. 2013;28:2298–307.
Fragouli E, Munne S, Wells D. The cytogenetic constitution of human blastocysts: insights from comprehensive chromosome screening strategies. Hum Reprod Update. 2019;25(1):15–33.
Viotti M, Victor AR, Zouves CG, Barnes FL. Is mitochondrial DNA quantitation in blastocyst trophectoderm cells predictive of developmental competence and outcome in clinical IVF? J Assist Reprod Genet. 2017;34(12):1581–5.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Approval for this study was obtained from the local Ethics Committee of IVIRMA Middle East Fertility Clinic, Abu Dhabi, UAE (Research Ethics Committee IVI-MEREF010/2017/REFA009). All patients signed a consent form allowing additional trophectoderm biopsy of supernumerary euploid and aneuploid embryos not selected for transfer.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
ESM 1
(DOCX 12 kb)
Rights and permissions
About this article

Cite this article
De Munck, N., Liñán, A., Elkhatib, I. et al. mtDNA dynamics between cleavage-stage embryos and blastocysts. J Assist Reprod Genet 36, 1867–1875 (2019). https://doi.org/10.1007/s10815-019-01544-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10815-019-01544-4