
Abstract
Purpose
Preimplantation genetic screening (PGS) and diagnosis (PGD) with euploid embryo transfer is associated with improved implantation and live birth rates as compared to routine in vitro fertilization. However, misdiagnosis of the embryo is a potential risk. The purpose of this study was to investigate the clinical discrepant diagnosis rate associated with transfer of trophectoderm-biopsied blastocysts deemed to be euploid via array comparative genomic hybridization (aCGH).
Methods
This is a retrospective cohort study including cycles utilizing PGS or PGD with trophectoderm biopsy, aCGH, and euploid embryo transfer at a large university-based fertility center with known birth outcomes from November 2010 through July 2014 (n = 520).
Results
There were 520 embryo transfers of 579 euploid embryos as designated by aCGH. Five discrepant diagnoses were identified. Error rate per embryo transfer cycle was 1.0 %, 0.9 % per embryo transferred, and 1.5 % per pregnancy with a sac. The live birth (LB) error rate was 0.7 % (both sex chromosome errors), and the spontaneous abortion (SAB) error rate was 17.6 % (3/17 products of conception tested, but could range from 3/42 to 7/42). No single gene disorders were mistakenly selected for in any known cases.
Conclusions
Although aCGH has been shown to be a highly sensitive method of comprehensive chromosome screening, several possible sources of error still exist. While the overall error rate is low, these findings have implications for counseling couples that are contemplating PGS and PGD with aCGH.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Couples at increased risk of aneuploidy may benefit from in vitro fertilization (IVF) with preimplantation genetic screening (PGS) [1]. This technology has led to higher implantation and live birth rates with lower miscarriage rates [2–5]. In addition, identification of euploid embryos allows for single embryo transfer, effectively decreasing multiple gestation rates and associated maternal and neonatal morbidity [6].
Prior to 2010, PGS was predominantly performed using fluorescence in situ hybridization (FISH) of only a limited number of chromosomes. In 2010, the European Society for Human Reproduction (ESHRE) recommended the replacement of FISH by comprehensive chromosome screening of all 24 chromosomes [7]. The various methods of comprehensive chromosome screening (CCS) include single nucleotide polymorphism (SNP) array, array comparative genomic hybridization (aCGH), and quantitative polymerase chain reaction (qPCR) [8]. There are also several ways to obtain genetic material for testing, including polar body biopsy, cleavage-stage embryo biopsy, and blastocyst biopsy. Multiple studies have shown that blastocyst trophectoderm biopsy with CCS is associated with higher implantation and delivery rates as compared to cleavage-stage biopsy [9–11]. Furthermore, Yang et al demonstrated that aCGH screening of blastocysts prior to cryopreservation with subsequent thawed embryo transfer resulted in improved implantation rates with low miscarriage rates [12]. Other studies have corroborated the benefit of thawed embryo transfer after trophectoderm biopsy. In fact, the use of thawed embryo transfer alone has been associated with improved pregnancy outcomes, including decreased risk of ectopic pregnancy, preterm birth, antepartum hemorrhage, low birth weight, and perinatal mortality [13–15].
Although PGS confers many advantages, misdiagnosis of the embryo is a potential risk that has been associated with all forms of CCS. The aim of this study was to evaluate clinically relevant outcomes of aCGH CCS on biopsied blastocysts with subsequent thawed embryo transfer (FET) to provide an estimate of aCGH misdiagnosis. Our findings are intended to inform the counseling conversation between physician and patient prior to initiating the PGS process with aCGH.
Materials and methods
All cycles utilizing PGS or PGD at a large university-based fertility center with known outcomes from November 2010 through July 2014 were included (n = 520). Patients underwent controlled ovarian stimulation followed by trophectoderm (TE) blastocyst biopsy and CCS using aCGH. This study was approved by New York University’s School of Medicine Institutional Review Board (NYU IRB#13-00389).
Ovarian stimulation protocols were individualized. Gonadotropins were administered to achieve adequate amount of mature oocytes. When at least two lead follicles measured 17–19 mm in diameter, human chorionic gonadotropin (hCG), gonadotropin-releasing hormone (GnRH), or a combination of both were used to trigger ovulation. Approximately 35 hours later, oocytes were retrieved via ultrasound-guided transvaginal aspiration. Oocytes were immediately isolated from follicular fluid, and fertilization was achieved as previously described by Grifo et al. [6] Intracytoplasmic sperm injection (ICSI) was performed for cases of single gene testing, severe male factor, or history of impaired fertilization in a prior cycle. On day 3 of development, the zona pellucida was incised using a Cronus laser (Research Instruments, Falmouth, UK), which allowed a portion of the blastocyst to protrude through the small incision during blastocyst expansion. Embryos were then cultured to day 5, day 6, or rarely, day 7. When a portion of the trophectoderm protruded through the incision, biopsy was performed by removing a sample comprising a small subset of the trophectoderm cells (5–10 cells) using a laser to detach points of adhesion between the biopsied cells and the remaining trophectoderm. The biopsied cells were immediately placed in reaction tubes containing medium provided by the genetics lab. Tubes were stored in dry ice and transported in to Reprogenetics (Livingston, NJ) for aneuploidy screening using aCGH. Analysis was performed as described by Gutirrez-Mateo et al without alteration [16]. Vitrification was then employed to preserve the blastocysts while still collapsed from the biopsy. The vitrification process was performed as previously described by Grifo et al. [6].
Patients preparing for embryo transfer underwent uterine preparation using oral estradiol therapy supplemented by progesterone. Estradiol was administered daily until the endometrial stripe was trilaminar in appearance and measured greater than 7 mm. At that point, progesterone (intramuscular or vaginal) was started. Embryos were thawed and transferred with ultrasound-confirmed placement of the catheter in the uterine lumen on the sixth day of progesterone administration.
Cycles were included if the outcome could confirm the aCGH-predicted diagnosis, such as live birth after single embryo transfer, or in the case of spontaneous abortion where dilation and curettage was performed and chromosomes were sent for cytogenetic analysis. Cycles without available outcome data were excluded.
A retrospective chart review was performed using a secure electronic medical record of patients with embryos that underwent PGS or PGD with subsequent transfer at NYU Fertility Center. The number of embryos transferred, gestational sacs, clinical pregnancies with a fetal heartbeat (FH), and cycle outcomes (specifically, live birth (LB) or spontaneous abortion (SAB)) were recorded. Implantation rate was defined as number of gestational sacs per embryo transferred. Clinical pregnancy rate was defined as fetal pole with visible fetal heart rate per embryo transfer cycle. Products of conception (POCs) that were collected from dilation and curettage (D&C) of a SAB were reviewed. SAB rate was then calculated as number of pregnancies lost divided by the number of pregnancies with a gestational sac.
PGS or PGD report of the embryo(s) transferred was compared with either clinical outcome of live birth or cytogenetic analysis of products of conception, depending on whether pregnancy or miscarriage occurred. Clinical live birth outcomes were recorded according to documentation of a normal male or female neonatal phenotype. Rarely, amniocentesis results during the pregnancy were available to confirm the PGS or PGD report. If a discrepant diagnosis was identified from the LB outcome or POCs, the trophectoderm biopsy samples were retested with aCGH at Reprogenetics.
Results
There were 520 embryo transfers of 579 euploid embryos as designated by aCGH. Baseline patient characteristics are presented in Table 1. The implantation rate of this population was 61.5 % (356/579), clinical pregnancy rate was 59.4 % (309/520), and the first trimester SAB rate was 12.6 % (41/326). During this period, there was one intrauterine fetal demise and one periviable loss. Five clinical misdiagnoses were identified during this time (Table 2). All but one live births were apparently euploid and of the correct gender. Of SABs requiring D&C, all POCs were analyzed, and all but two agreed with the original PGS diagnosis.
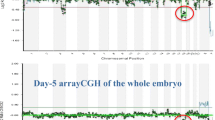
Specimens were re-analyzed by Reprogenetics using aCGH if a discrepancy was suspected between the PGD-predicted diagnosis and either the cytogenetic analysis of POCs or the live birth phenotypic outcome (Table 2). The original sample consisting of whole-genome-amplified DNA from a few (five to ten) trophectoderm cells was identified, and the amplified sample was reanalyzed with control DNA for comparison. In three of the five cases, the discrepancy reanalysis of the hybridization plot confirmed the initial PGS diagnosis and therefore was different than the karyotype obtained from POCs or live birth. In the remaining two cases, the reanalyzed result was assigned the same diagnosis as the karyotype obtained from POCs or the live-born infant, and therefore, the reanalysis was inconsistent with the initial PGS diagnosis.
After reanalysis, discordant diagnosis in four of five embryos was likely secondary to either mosaicism or technical error of the method. The final discrepant diagnosis was speculated to have occurred secondary to contamination of extraneous genetic material with the biopsied specimen. The predicted diagnosis was normal 46,XX; however, DNA fingerprinting of the infant via buccal swab confirmed a normal 46,XY karyotype (Table 1). A cell from a female embryologist handling the specimen was thought to have contaminated the assay, and therefore, a female biopsy diagnosis was obtained. DNA fingerprinting of the embryologist confirmed this suspicion.
Error rate per embryo transfer cycle was 1.0 %, 0.9 % per embryo transferred, and 1.5 % per pregnancy with a sac (Table 3). The LB error rate was 0.7 % (both sex chromosome errors), and the SAB POCs error rate was 17.6 %. The latter error rate derives from three errors of 17 POCs tested, but could potentially range from 3/42 to 7/42, as this number does not account for the error rate of embryos resulting in SABs lacking POCs available for analysis.
Comment
As prior studies suggest, PGS confers many advantages, especially when trophectoderm (TE) biopsy is used in combination with single thawed euploid embryo transfer [1, 3, 6]. However, couples must also understand potential risks of the process. Concerns have been raised regarding whether embryo biopsy and/or freezing with subsequent thaw is harmful for the embryo. Data suggests that TE biopsy does not injure the embryo, and cryopreserved transfer cycles have equivalent to improved outcomes as compared with fresh IVF cycles [10, 13, 14]. Alternatively, misdiagnosis of the embryo has been identified as a rare but potential risk occurring with all forms of chromosome screening. There are several opportunities for introduction of error throughout the process of preimplantation genetic screening; the most obvious of which is sampling error. Although TE biopsy has been shown to be superior to cleavage-stage biopsy [9], it remains unclear whether this small sampling of TE cells is representative of the entire trophectoderm, or more importantly, of the inner cell mass. Additionally, all samples are subject to contamination error (by parental or extraneous DNA), which may be impossible to completely eliminate despite implementation of optimal quality improvement measures.
The first PGS technique utilized cleavage-stage biopsy with FISH analysis, which has fallen out of favor due to lack of proven benefit [16]. Misdiagnosis rates of qPCR-based PGS have been reported at 0.27 % [17] and 0.32 % [18] per transfer for single gene disorders and aneuploidy screening, respectively. The misdiagnosis rate of aCGH is currently reported as 1.9 % (1/54) when reanalyzing specimens with fluorescence in situ hybridization (FISH) [17] and 7.0 % with SNP microarray reanalysis [19]. However, data regarding misdiagnosis remains limited regarding aCGH technology.
With the expanding population utilizing PGS technologies, continued assessment of test validity for each technique is necessary. Although aCGH has been shown to be a highly sensitive method of CCS [1, 5–7], both technical and biologic errors still exist. aCGH utilizes PCR technology, which lends specimens susceptible to several known sources of error including failure of amplification of one of the parental alleles and obscured diagnosis by the presence of haploid cells. Additionally, unprotected intercourse during the PGS or PGD cycle can result in implantation of an undiagnosed embryo, confounding the rate of misdiagnosis. De novo chromosomal errors can also take place secondary to post-zygotic mitotic changes [17, 20, 21]. Finally, it is known that aCGH technology is incapable of detecting mosaic embryos, which is a plausible cause of two cases of discrepant diagnoses in our study population. The rate of mosaicism between the trophectoderm and the inner cell mass has been reported as at least 3.9 % [22], which has unclear clinical implications at this point. Although CCS technology continues to improve, mosaicism cannot be fully diagnosed or excluded. The result is that a biopsied embryo can have a discrepant diagnosis if the abnormal cells become predominant after biopsying normal cells.
During our study period, many embryos were transferred that did not have a confirmed outcome diagnosis, such as biochemical and ectopic pregnancies and non-implanted blastocysts. Additionally, euploid embryos that were incorrectly diagnosed as aneuploid would have been discarded; therefore, the false positive rate in our population is unknown. Alternatively, the recognizable false negative test errors that were identified generate a negative predictive value of PGS with aCGH that is clinically relevant. This information is an essential component to PGS counseling, as all patients utilizing this technology have a chance of being affected.
Limitations of this study include lack of antepartum testing to confirm PGS or PGD results and the previously mentioned lack of confirmatory testing on embryos not transferred. PGS-predicted diagnosis of embryos resulting in miscarriage was confirmed with cytogenetic analysis after a suction D&C procedure; however, this occurred in only 40 % (17/42) of SABs. An additional limitation is the lack of confirmatory testing with a second CCS technology. The cells from the discrepant samples were whole-genome amplified for the initial analysis, and therefore, any error that occurred prior to this step would be undetectable. The discrepant samples were then reanalyzed with the same aCGH technology that produced the initial diagnosis; however, in a few cases, different results were obtained, likely secondary to improvements in the analysis software over time. Additionally, DNA degradation may have obscured the quality of the profiles as samples were reanalyzed several months after the initial analysis.
Our data from PGS and PGD cycles over the past several years reveals a low error rate that is consistent with rates reported in previous studies [17]. However, comparison of error rates between studies should be made with caution, as PCR-based misdiagnosis has been reported in a number of ways. In the ESHRE PGD Consortium of data collected from 1997 to 2007, misdiagnoses were identified as adverse or benign [17, 20]. Misdiagnoses are considered adverse if they result in the birth of an affected child or termination of an affected pregnancy. Alternatively, benign discrepant diagnoses are less serious, and result in offspring that is either a carrier of an autosomal recessive condition or alternatively occurs secondary to contamination and result in normal live birth. Only adverse misdiagnoses were reported in the ESHRE PGD Consortium, totaling 12 cases [17]. Rate of misdiagnosis was also categorized by indication for preimplantation genetic testing. Ten of these cases were undergoing PGD for single gene disorders, with a misdiagnosis rate of 0.27 % (10/3727). The two remaining misdiagnoses were following PCR testing for X-linked disorders. Additionally, two misdiagnoses were identified out of a total of 65 PGD cycles to determine sex for X-linked disorders, resulting in a misdiagnosis rate of 3.6 % [17]. In the present study, adverse false negative rate of aCGH was 0.5 % (3/584) per embryo transferred, and benign misdiagnosis rate was 0.3 % (2/584) per embryo transferred. Of note, no single gene disorders were misdiagnosed in any known cases.
As this study does not account for the error rate in embryos that were discarded, did not progress to a clinical stage, or result in POCs available for analysis, our findings should be used to counsel patients on the negative predictive value of aCGH in evaluable pregnancies. Although rare, the possibility of PGS or PGD error is important to discuss with patients, as misdiagnosis of embryos can have significant clinical consequences, especially in the event of a live birth outcome [23]. The etiologies of the identified discrepancies cannot be known for certain, as there are several steps in CCS (i.e., biopsy, whole-genome amplification, hybridization, analysis) and therefore several opportunities for error. Similarly, mosaicism of the embryo resulting in preimplantation diagnostic error cannot be definitively excluded or confirmed when using aCGH. As a result, patients utilizing PGS or PGD with aCGH should be offered antenatal diagnostic testing to confirm preimplantation diagnosis. It is important for clinicians to be aware of the specific PGS/PGD clinical error rate for their respective modality of preimplantation genetic testing in order to best counsel patients when considering this costly, yet rewarding, endeavor.
References
Chang J, Boulet SL, Jeng G, Flowers L, Kissin DM. Outcomes of in vitro fertilization with preimplantation genetic diagnosis: an analysis of the United States Assisted Reproductive Technology Surveillance Data, 2011–2012. Fertil Steril. 2016;105(2):394–400.
Scott Jr RT, Upham KM, Forman EJ, Hong KH, Scott KL, Taylor D, et al. Blastocyst biopsy with comprehensive chromosome screening and fresh embryo transfer significantly increases in vitro fertilization implantation and delivery rates: a randomized controlled trial. Fertil Steril. 2013;100:697–703.
Forman EJ, Hong KH, Ferry KM, Tao X, Taylor D, Levy B, et al. In vitro fertilization with single euploid blastocyst transfer: a randomized controlled trial. Fertil Steril. 2013;100:100–7.
Keltz MD, Vega M, Sirota I, et al. Preimplantation genetic screening (PGS) with comparative genomic hybridization (CGH) following day 3 single cell blastomere biopsy markedly improves IVF outcomes while lowering multiple pregnancies and miscarriages. J Assist Reprod Genet. 2013;30(10):1333–9.
Harton GL, Munne S, Surrey M, Grifo J, Kaplan B, McCulloh DH, et al. Diminished effect of maternal age on implantation after preimplantation genetic diagnosis with array comparative genomic hybridization. Fertil Steril. 2013;100(6):1695–703.
Grifo JA, Hodes-Wertz B, Lee HL, Amperloquio A, Clarke-Williams M, Adler A. Single thawed euploid embryo transfer improves IVF pregnancy, miscarriage, and multiple gestation outcomes and has similar implantation rates as egg donation. J Assist Reprod Genet. 2013;30:259–64.
Harper J, Coonen E, De Rycke M, et al. What next for preimplantation genetic screening (PGS)? A position statement from the ESHRE PGD Consortium Steering Committee. Hum Reprod. 2010;25(4):821–3.
Dahdouh EM, Balayla J, Aduibert F, et al. Technical update: preimplantation genetic diagnosis and screening. J Obstet Gynecol Can. 2015;37(5):451–63.
Scott Jr RT, Upham KM, Forman EJ, Zhao T, Treff NR. Cleavage-stage biopsy significantly impairs human embryonic implantation potential while blastocyst biopsy does not: a randomized and paired clinical trial. Fertil Steril. 2013;100:624–30.
Scott RT, Tao X, Taylor D, Ferry K, Treff N. A prospective randomized controlled trial demonstrating significantly increased clinical pregnancy rates following 24 chromosome aneuploidy screening: biopsy and analysis on day 5 with fresh transfer. Fertil Steril. 2010;94:S2.
Moutou C, Goossens V, Coonen E, et al. ESHRE PGD Consortium data collection XII: cycles from January to December 2009 with pregnancy follow-up to October 2010. Hum Reprod. 2014;29(5):880–903.
Yang Z, Salem SA, Liu X, Kuang Y, Salem RD, Liu J. Selection of euploid blastocysts for cryopreservation with array comparative genomic hybridization (aCGH) results in increased implantation rates in subsequent frozen and thawed embryo transfer cycles. Mol Cytogenet. 2013;6(1):32.
Shapiro BS, Daneshmand ST, Garner FC, Aguirre M, Hudson C, Thomas S. Evidence of impaired endometrial receptivity after ovarian stimulation for in vitro fertilization: a prospective randomized trial comparing fresh frozen-thawed embryo transfer in normal responders. Fertil Steril. 2011;96(2):344–8.
Maheshwari A, Pandey S, Shetty A, Hamilton M, Bhattacharya S. Obstetric and perinatal outcomes in singleton pregnancies resulting from the transfer of frozen thawed versus fresh embryos generated through in vitro fertilization treatment: a systematic review and meta-analysis. Fertil Steril. 2012;98(2):368–77.
Schoolcraft WB, Treff NR, Stevens JM, Ferry K, Katz-Jaffe M, Scott RT. Live birth outcome with trophectoderm biopsy, blastocyst vitrification, and single-nucleotide polymorphism microarray-based comprehensive chromosome screening in infertile patients. Fertil Steril. 2011;96:638–40.
Gutiérrez-Mateo C, Colls P, Sánchez-Garcia J, et al. Validation of microarray comparative genomic hybridization for comprehensive chromosome analysis of embryos. Fertil Steril. 2011;95:953–8.
Harper JC, Wilton L, Traeger-Synodinos J, Goossens V, Moutou C, SenGupta SB, et al. The ESHRE PGD Consortium: 10 years of data collection. Hum Reprod Update. 2012;18:234–47.
Werner MD, Leondires MP, Schoolcraft WB, Miller BT, Copperman AB, Robins ED, et al. Clinically recognizable error rate after the transfer of comprehensive chromosomal screened euploid embryos is low. Fertil Steril. 2014;102(6):1613–8.
Capalbo A, Ubaldi FM, Rienzi L, Tao X, Treff NR, Scott RT. Comparison of quantitative real-time (q)PCR and array comparative genomic hybridization (aCGH) based 24 chromosome aneuploidy screening in human blastocysts. Fertil Steril. 2013;100:S2.
Wilton L, Thornhill A, Traeger-Synodinos J, Sermon K, Harper J. The causes of misdiagnosis and adverse outcomes in PGD. Hum Reprod. 2009;24:1221–8.
Frumkin T, Malcov M, Yaron Y, Ben-Yosef D. Elucidating the origin of chromosomal aberrations in IVF embryos by preimplantation genetic analysis. Mol Cell Endocrinol. 2008;282(1–2):112–9.
Johnson DS, Cinnioglu C, Ross R, et al. Comprehensive analysis of karyotypic mosaicism between trophectoderm and inner cell mass. Mol Hum Reprod. 2010;16(12):944–9.
Klitzman R, Zolovska B, Folberth W, Sauer MV, Chung W, Appelbaum P. Preimplantation genetic diagnosis on in vitro fertilization clinic websites: presentations of risks, benefits and other information. Fertil Steril. 2009;92:1276–83.
Author information
Authors and Affiliations
Corresponding author
Additional information
CapsuleThis retrospective study identified a discrepant diagnosis rate of 1.0 % per embryo transfer cycle and 0.9 % per embryo transferred when utilizing array comparative genomic hybridization for PGS in trophectodermbiopsiedthawed blastocysts.
Rights and permissions
About this article

Cite this article
Tiegs, A.W., Hodes-Wertz, B., McCulloh, D.H. et al. Discrepant diagnosis rate of array comparative genomic hybridization in thawed euploid blastocysts. J Assist Reprod Genet 33, 893–897 (2016). https://doi.org/10.1007/s10815-016-0695-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10815-016-0695-3