
Abstract
This study aimed to investigate the gap between adaptive functioning and cognitive functioning, especially verbal and nonverbal intelligence quotient (IQ) in Chinese children with ASD. We systematically explored cognitive functioning, ASD severity, early signs of developmental abnormalities, and socioeconomic factors as mediating factors of adaptive functioning. We enrolled 151 children (age: 2.5?6 years) with ASD and categorized them into one group with IQ ≥ 70 and another with IQ < 70. The two groups were calibrated for age, age at diagnosis, and IQ, and the relationship of adaptive skills with vocabulary acquisition index (VAI) and nonverbal index (NVI) were separately analyzed. Results show that the gap between IQ and adaptive functioning was significant in children with ASD having IQ ≥ 70, with both VAI and NVI showing statistically significant differences (all P < 0.001). VAI correlated positively with scores for overall adaptive skills and specific domains, whereas NVI had no significant correlations with adaptive skill scores. Age of first walking unaided had an independent positive correlation (all P < 0.05) with scores of adaptive skills and specific domains. IQ-adaptive functioning gap is significant in children with ASD having IQ ≥ 70, suggesting that defining “high-functioning autism” merely on the basis of IQ is not appropriate. Verbal IQ and early signs of motor development are specific and possible predictors of adaptive functioning in children with ASD, respectively.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Autism spectrum disorder (ASD) is a neurodevelopmental disorder characterized by deficiencies in communication and social interaction as well as stereotyped and repetitive behaviors, with symptoms appearing at an early age (APA, 2013; Lord, et al., 2018). Functional impairment is a prerequisite for the diagnosis of ASD, and individuals with ASD may exhibit a range of functional abilities, depending on their developmental stage and context (Chatham, et al., 2018). Adaptive functioning is a crucial factor considered in the evaluation of functional impairment in children with ASD. Both as children and as adults, individuals with ASD have been consistently shown to exhibit poorer adaptive abilities than typically developing individuals or individuals with other developmental disorders (Kenworthy, et al., 2010; Mouga, et al., 2015). Adaptive functioning comprises skills essential for everyday functioning, such as daily living skills, socialization, and communication. Lack of adaptive ability is an important indication for individual intervention (Bölte, et al., 2019). Assessing adaptive functioning complements the diagnostic evaluation in individuals suspected to have ASD and provides important information on requirements for functional support. Therefore, identifying the mediating factors that impact adaptive functioning can help develop strategies for early diagnosis and intervention in ASD.
The presence of intellectual impairment along with deficit in adaptive functioning is the foundational criterion for the diagnosis of intellectual disability (ID). Studies have shown that cognitive functioning is an important mediating factor of adaptive functioning in ASD, but the association between cognitive functioning and adaptive functioning has not been replicated in children with ID and without ID. Lower intelligence quotient (IQ) has been shown to be associated with poorer adaptive behaviors among individuals diagnosed with ASD and ID (Kanne, et al., 2011), suggesting low IQ is a major contributor to poor adaptive skills and prognosis. However, recent studies have shown that individuals without ID may still exhibit poorer adaptive skills than that expected from their intellectual potential (Bradshaw, et al., 2019). Adaptive functioning assessed using Vineland Adaptive Behavior Scales (VABS) have been found to be significantly lower than that expected for the corresponding IQ in children without ID (Alvares, et al., 2020). One possible explanation is that increased symptoms (e.g., attention deficit, hyperactivity, emotional disturbances) are closely related to poorer adaptive ability in children without ID. Further exploration of the relationship between adaptive ability and IQ in children with ASD is necessary. Previous studies on the correlation between IQ and adaptive behaviors have generally used Full-Scale Intelligence Quotient (FSIQ) to evaluate cognitive functioning (Kenworthy, et al., 2010; Liss, et al., 2001). In this study, we sought to determine how verbal IQ and nonverbal IQ impact adaptive behaviors.
Recently, researchers have begun to focus on the disparity between cognitive and adaptive functioning in ASD. Evidence has shown that the IQ-adaptive functioning gap in ASD without ID emerged in early toddlerhood (Klin, et al., 2007; Pugliese, et al., 2015) and continues through adolescence (Kraper, et al., 2017). Studies have shown that individuals with ASD without ID exhibit a disparity between IQ and adaptive behaviors, which exacerbates with age (Pugliese, et al., 2015). The disparity between IQ and VABS scores has been shown to increase with an increase in the age of diagnosis of ASD (Alvares, et al., 2020). Put together, these findings suggest that age and age at diagnosis of ASD are important factors influencing the IQ-adaptive functioning gap. Few studies have focused on the gap in preschool age population, and we sought to further explore the IQ-adaptive functioning gap in preschool age children with ASD after accounting for the two abovementioned factors.
A few studies have explored the correlation between ASD symptoms, diagnosis, and adaptive functioning, but the results are inconsistent. A small-scale study has shown that severe repetitive behaviors are closely related to less well-developed adaptive abilities and that autistic symptoms are negatively associated with overall adaptive skills (Troyb, et al., 2016). In contrast, a large-scale study (N = 2538) has shown that ASD severity is weakly associated with adaptive behaviors in school-aged children with ASD (Pathak, et al., 2019). In a recent study, ASD symptom severity has failed to predict variability in specific domains or global components of the adaptive behaviors included in VABS (Hodge, et al., 2021). The present study seeks to further explore the correlation between ASD symptoms and adaptive functioning in preschool age children with ASD. Early signs of developmental abnormalities, in both language and motor skills, are crucial to the diagnosis of ASD and for planning appropriate interventions; they may also be important predictors of adaptive behavior. Delay in early language development in children with ASD may affect verbal communication, thus resulting in a deficit of daily communication skills. To the best of our knowledge, few studies have investigated the relation between early signs of development and adaptive functioning in ASD.
Some studies have examined how socioeconomic factors, mainly family income, parental level of education, and community resources, impact behaviors in ASD. However, the findings of such studies are inconsistent. An earlier study on the impact of socioeconomic status (SES) on autistic symptoms found that lower SES is associated with increased emotional and behavioral challenges, which may aggravate adaptive behaviors in ASD (Mayes & Calhoun, 2011). However, a recent study on preschool-aged children has shown no significant relationship between SES and adaptive behaviors or ASD severity (Mathew, et al., 2019). Children with ASD are more likely to remain minimally verbal into adulthood in the context of lower parental income and education, suggesting the importance of socioeconomic factors in individual development (Maltman, et al., 2021). This study further examines how socioeconomic factors impact adaptive functioning.
The primary objective of our study is to examine the disparity between IQ and adaptive functioning in Chinese preschool-aged children with ASD. Additionally, we also explore how IQ, ASD severity, early signs of developmental abnormalities, and socioeconomic factors contribute to variability in adaptive functioning. Such an understanding would be conducive to early diagnosis and individualized planning of intervention and supportive services for children with ASD. On the basis of the findings of previous studies, we hypothesized the following: (1) There will be a significant disparity between IQ and adaptive functioning in children with ASD, especially in those having IQ ≥ 70. (2) IQ will be the most important factor that influences adaptive functioning, and verbal IQ may be a more specific predictor than nonverbal IQ. (3) ASD severity, early signs of developmental abnormalities, and socioeconomic factors will, at least to some extent, account for variability in specific domains of adaptive functioning.
Methods
Participants
This study was performed at the Child Developmental and Behavioral Center, a hospital in China. A total of 151 children aged 2.5–6 years who were clinically diagnosed with ASD were enrolled between September 2021 and May 2022. The criteria for inclusion in the study were as follows: (1) All the ASD diagnostic criteria defined by Diagnostic and Statistical Manual of Mental Disorders (DSM-V) (APA, 2013) are met. (2) The child has reached verbal developmental stage of single words and phrases. (3) The child has reached the developmental stage of independent walking. The exclusion criteria in this study were as follows: (1) diagnosis of fragile X syndrome, Rett syndrome, Prader-Willi syndrome, Angelman syndrome, or any other syndromes caused by known genetic abnormalities or hereditary metabolic disorders; (2) presence of hearing impairment or hearing disorder; (3) presence of physical disabilities; (4) history of epilepsy, epileptic seizure, or anti-epileptic medication; and (5) history of neonatal brain injury, hypoxic ischemic encephalopathy, or intrauterine hypoxia.
Measures
Adaptive Functioning
Adaptive functioning was measured using Adaptive Behavior Assessment System Version II (ABAS-II) (Oakland & Harrison, 2008). The infant/preschool form of the ABAS-II has been applied extensively to assess the adaptive ability of children aged 0–6 years (Ye, et al., 2021). The third edition of ABAS was not implemented in China when we designed the study, and the reliability and validity of the Chinese version was not verified, thereby we used the ABAS-II. The standardized Chinese version of ABAS-II is comparable to the US version in reliability and validity (Li & Qiu, 2016). Using ABAS-II adaptive functioning of children is evaluated at two levels. The first level contains three specific domains of adaptive skills, namely, conceptual skills, social skills, and practical skills. Conceptual skills include communication, preschool functioning, and self-management; social skills include leisure and social interaction; and practical skills include family life, community adaptability, self-care, and health and safety. The second level comprises overall adaptive skills, representing a composite of all three domains and motor skills. Consistent with previous studies, our study was conducted using composited standard scores of adaptive behaviors to evaluate adaptive skills. Standard scores were normalized for age and ranged from 40 to 160, with higher scores indicating better adaptive skills.
Cognitive Functioning
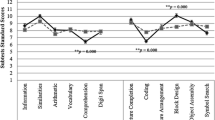
Cognitive functioning was assessed using Wechsler Preschool and Primary Scale of Intelligence IV (WPPSI-IV) (Wechsler, 2012). WPPSI-IV is a cognitive ability test with high reliability and validity, which has been confirmed by extensive use in children with ASD; its standard and index scores have been found to be stable over time (Watkins, et al., 2022). The standardized Chinese version of Wechsler intelligence scale has also been shown to have good reliability and validity (Zhang, 2009). Considering that the IQ of preschool-aged children is unbalanced, especially in verbal IQ and nonverbal IQ, cognitive functioning of children was evaluated at two levels in the present study. The first level of FSIQ evaluates the overall cognitive functioning. The second level contains two specific domains of cognitive ability: vocabulary acquisition index (VAI) and nonverbal index (NVI). VAI includes picture naming and receptive vocabulary and reflects verbal IQ. NVI includes block design, matrix reasoning, picture memory, and object assembly and reflects nonverbal IQ. As was the case with the ABAS-II scores, standard scores of WPPSI-IV were also normalized for age and ranged from 40 to 160, and higher scores estimate better cognitive ability.
Cognitive-adaptive Functioning Gap
Rather than directly using the difference in the FSIQ-adaptive functioning scores as a measure of the gap between cognitive functioning and adaptive functioning, we investigated the impact of VAI and NVI separately on the differences in IQ-adaptive functioning gap according to IQ level. A proportion score was used to analyze group differences according to IQ level, rather than a simple difference score. Similar to the methods used in recent studies (McQuaid, et al., 2021), the IQ-adaptive functioning gap was assessed using proportion scores of the differences between IQ and the scores for conceptual skills, social skills, and practical skills in ABAS-II that were calculated as follows: IQ-adaptive functioning gap proportion score = (IQ – Domain Score)/IQ *100. The proportion score was used to calibrate IQ, to account for the impact of lower IQ scores in the group with IQ < 70 and higher IQ scores in the group with IQ ≥ 70.
ASD Severity
ASD severity was evaluated using the Autism Diagnostic Observation Schedule (ADOS). The ADOS is a standardized assessment to evaluate the current severity of autistic symptoms for children with ASD (Lord, et al., 2002), which includes communication, social reciprocity, and restricted and repetitive behaviors. The validity of ADOS for the diagnosis of ASD in the Chinese population has been previously established (Sun, et al., 2015). Since the enrolled population included children with different levels of language skills and age, different modules (module 1, module 2, and module 3) were used for the evaluation of ASD symptoms. In order to reduce the differences in the language skill levels and age, we used standardized ADOS-Calibrated Severity Scores (ADOS-Css). First, the revised algorithms were used into total scores for the domains of social affect and restricted and repetitive behaviors, to improve predictive value (Gotham, et al., 2007). Next, the revised algorithms for all modules were transformed to calibrated severity scores (Gotham, et al., 2009), which range from 0 to 10. Higher ADOS-Css indicate more severe autism symptoms in children with ASD.
Early Signs of Developmental Abnormalities
Early signs of developmental abnormalities were assessed using Autism Diagnostic Interview-Revised (ADI-R). ADI-R is designed to evaluate autistic behaviors and quantify the developmental history in a semi-structured parent/caregiver interview (Rutter, et al., 2003). Early signs of developmental abnormalities included in ADI-R are age of first single words, age of first phrases, and age of first walking unaided. In our study, age of first single words and first phrases in ADI-R was used to assess early language development, while age of first walking unaided was used to evaluate motor development. Additionally, age at which parents first noticed developmental abnormalities was used to assess onset symptoms correlation with diagnosis of ASD. The above data are recorded in months according to ADI-R items.
Procedure
All clinical assessments were administered during hospitalization. Assessments using the ADOS and WPPSI-IV scales were performed by professional staff. Data on socioeconomic factors, including paternal/maternal level of education and family income, were collected from parent questionnaire. Data on age at diagnosis with ASD and age of first visit (to a doctor or hospital) were also obtained from parent questionnaire. The head circumference was measured according to standard methods. All enrolled children were classified into two groups based on FSIQ: children with ASD having IQ ≥ 70 and children with ASD having IQ < 70.
Quality Control
All children with ASD were diagnosed by two specialist and qualified clinicians to ensure diagnostic fidelity and consistency. ADOS and WPPSI-IV were administered with the standardized instructions by certified therapists and clinicians and in strict accordance with the operational process. Parents completed the ABAS-II form after receiving a uniform set of instructions from the professional staff. In addition, head circumference was measured using standard procedures, by specialist nurses who received uniform training.
Statistical Analyses
Continuous data were represented as means (M) and standard deviations (SD). In the first step, t-test was used to compare the normally distributed data in the two groups (children with IQ ≥ 70 vs. children with IQ < 70). Intergroup comparisons of continuous data that did not conform to normal distribution were made using t-test after conversion to normal distribution data. To preclude the confounding effect of age and age of diagnosis, in the second step, analysis of covariance (ANCOVA) was applied to compare data in IQ-adaptive skills gap between groups, with age and age at diagnosis as covariables. Discrete data were represented by frequency (%). Gender differences were compared using the Chi-square test, and ranked data were used to compare the two groups using the Mann-Whitney U test.
Rather than to automatically select the most important variable, a series of hierarchical regressions were performed in sequence to examine the unique contributions of socioeconomic factors, IQ, ASD severity, and early signs of developmental abnormalities to variation in adaptive skills. The sequence of hierarchical regression was similar to the statistical methods used in recent studies (Hodge, et al., 2021). To explore the contribution of the different predictors to overall and domain-specific components of adaptive functioning, hierarchical regressions on overall adaptive skills and the three domains were separately computed. P < 0.05 was considered as statistically significant. The value of Cohen’s d was determined to interpret the effect size for the t-test: 0.20, small; 0.50, moderate; and 0.80, large. η² was used to interpret effect size for ANCNOVA: 0.01, small; 0.06, moderate; and 0.14, large (Cohen, 1988). The SPSS version 20.0 software was used for all statistical analyses.
Results
Demographics
Table 1 displays the demographic data of the sample population, including head circumference. The average age of the enrolled children was 4.20 years, and the male to female sex ratio was 5.2:1, which is consistent with the sex bias reported for ASD in epidemiological surveys. Thus, the age and sex ratio of the sample population was representative of that in the general population of preschool-aged children with ASD. There were no statistically significant differences in the age and sex ratio in the group with IQ ≥ 70 and the group with IQ <70 (all P > 0.05). In terms of diagnosis, the age at diagnosis was significantly delayed in with the group with IQ ≥ 70 (t = 2.11, P = 0.037, Cohen’s d = 0.36). Similarly, the age at which parents first noticed developmental abnormalities was also later in the group with IQ ≥ 70 (t = 2.07, P = 0.041, Cohen’s d = 0.33). These findings suggest that higher IQ could lead to a delay in diagnosis of ASD.
Head circumference, as endophenotype of autism, was not found to correlate with global or domain-specific components of adaptive skills (all P > 0.05). No significant difference in head circumference was found between the two groups (Z = 0.56, P = 0.579). From the birth-related data, no statistically significant intergroup differences were found in birth weight, delivery method, or gestational age (all P > 0.05). Similarly, with respect to socioeconomic factors, no statistically significant differences were noted between the two groups with regard to the parents’ highest education level and family income (all P > 0.05).
Comparison of Adaptive Skills, IQ, Early Signs of Developmental Abnormalities, and Symptom Severity in Children with IQ ≥ 70 and IQ < 70
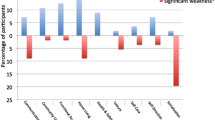
As shown in Table 2, significant differences were noted between children with IQ ≥ 70 and those with IQ < 70 in the scores of overall adaptive skills and the three domains of skills (all P > 0.05). In the assessment of cognition functioning, children having IQ ≥ 70 scored significantly higher in both VAI and NVI, when compared with children having IQ < 70 (t = 14.32, 15.40; P < 0.001; Cohen’s d = 2.56, 2.83). With respect to early signs of developmental abnormalities, age of first single words and first phrases for children with IQ ≥ 70 was significantly lower than that for children with IQ < 70 (t = 4.15, 4.24; P < 0.001; Cohen’s d = 0.61, 0.74); however, there were no significant differences between the two groups in the age of first walking unaided (t = 0.26, P = 0.799). In terms of symptoms, children with IQ ≥ 70 had less severe ASD symptoms when compared with children having IQ < 70 (t = 3.49, P = 0.001, Cohen’s d = 0.55).
Comparison of IQ-adaptive Skills Gap in Children with IQ ≥ 70 and those with IQ < 70
Next, we examined the gap between IQ and ABAS-II scores, for both the composite score and scores for each domain. We first examined the interaction between the group and age (group × age) and between group and age of diagnosis (group × age of diagnosis). The model comparisons showed no group × age and group × age of diagnosis interactions, except in the case of IQ-social skills gap (Table 3). At the first level, the proportion scores of children with IQ ≥ 70 had significantly higher FSIQ-Overall adaptive skills gap than those with IQ < 70 (F = 35.36, P < 0.001, η² = 0.19). Furthermore, this difference remained significant in the case of the proportion scores for VAI-Overall adaptive skills and NVI-Overall adaptive skills gap (F = 32.51, 22.61; P < 0.001; η² = 0.18, 0.13). At the second level of analysis, children with IQ ≥ 70 had significantly higher proportion scores for IQ-adaptive functioning gap in all the three domains (all P < 0.001). Moreover, significant differences between the two groups were also noted in the gap between VAI/NVI and specific domain scores (all P < 0.001).
Contribution of Socioeconomic Factors, IQ, ASD Severity, and Early Signs of Developmental Abnormalities to ABAS-II Overall Adaptive Skills
The hierarchical regression model was used to determine how socioeconomic factors, IQ, ASD severity, and early signs of developmental abnormalities impact overall adaptive skills in sequence (Table 4). The total model had good interpretation with 61.8% of variance (P < 0.001). Although gender was relevant to overall adaptive skills in the total model (β = 0.12, P = 0.038), age and gender did not show any significant variance in step 1 (F = 1.64, P = 0.198). Socioeconomic factors contributed to an additional 9.7% of variance in step 2 (ΔF = 5.31, P = 0.002), and maternal highest education was positively correlated with overall adaptive skills in the total model (β = 0.15, P = 0.022). FSIQ contributed an additional 36.9% variance in step 3 (ΔF = 103.14, P < 0.001), suggesting that IQ had the largest contribution to overall adaptive skills. VAI and NVI contributed to an additional 6.4% of the variance in step 4 (ΔF = 10.12, P < 0.001), and VAI emerged as a specific predictor in the total model (β = 0.34, P = 0.003), rather than NVI (β = -0.37, P = 0.087). ADOS-Css did not contribute any significant variance in step 5 (ΔF = 0.00, P = 0.964) and was found to have no significant correlation with overall adaptive skills in the total model (β = -0.07, P = 0.233). Early signs of developmental abnormalities accounted for an additional 6.6% of the variance in step 6 (ΔF = 7.84, P < 0.001), whereas age of first walking unaided was negatively correlated to overall adaptive skills in the total model (β = -0.21, P < 0.001).
Contribution of Socioeconomic Factors, IQ, ASD Severity, and Early Signs of Developmental Abnormalities to ABAS-II Conceptual Skills
Table 5 displays the model examining how socioeconomic factors, IQ, ASD severity, and early signs of developmental abnormalities impact ABAS-II conceptual skills. The total model still had good interpretability with 59.5% of variance (P = 0.002). Age and gender did not account for any significant variance in step 1 (F = 1.40, P = 0.251), and these factors did not predict conceptual skills in the total model (all P > 0.05). Socioeconomic factors contributed an additional 7.8% of variance in step 2 (ΔF = 4.16, P = 0.007), and the three socioeconomic factors were not significantly relevant to conceptual skills in the total model (all P > 0.05), which showed that socioeconomic factors were poorly associated with conceptual skills. FSIQ contributed an additional 34.6% variance in step 3 (ΔF = 88.88, P < 0.001), suggesting that IQ still had the largest contribution to conceptual skills. VAI and NVI contributed to an additional 10.0% of the variance in step 4 (ΔF = 15.40, P < 0.001). Rather than NVI (β = -0.36, P = 0.099), VAI still emerged as a specific predictor in the total model (β = 0.44, P < 0.001). ADOS-Css did not contribute to any significant variance in step 5 (ΔF = 1.33, P = 0.252) and did not predict overall adaptive skills in the total model (β = 0.00, P = 0.995). Early signs of developmental abnormalities accounted for an additional 4.8% of the variance in step 6 (ΔF = 5.39, P = 0.002), and age of first walking unaided was found to be negatively associated with conceptual skills in the total model (β = -0.15, P = 0.014).
Contribution of Socioeconomic Factors, IQ, ASD Severity, and Early Signs of Developmental Abnormalities to ABAS-II Social Skills
The hierarchical regression model was also used to examine the contribution of socioeconomic factors, IQ, ASD severity, and early signs of developmental abnormalities to social skills (Table 6). The total model had good interpretability with 49.2% of variance (P = 0.005). Age and gender did not account for any significant variance in step 1 (F = 1.69, P = 0.188). Although socioeconomic factors contributed an additional 9.5% of variance in step 2 (ΔF = 5.16, P = 0.002), they did not have any significant association with social skills in the total model (all P > 0.05). FSIQ contributed an additional 30.2% variance in step 3 (ΔF = 74.38, P < 0.001), which indicated that IQ was the largest contributor to social skills. Although ADOS-Css were negatively correlated with social skills in the total model (β = -0.15, P = 0.033), the scores did not account for any significant variance in step 5 (ΔF = 1.88, P = 0.173). Early signs of developmental abnormalities accounted for an additional 5.0% of the variance in step 6 (ΔF = 4.52, P = 0.005), and age of first phrases was negatively correlated with social skills (β = -0.21, P = 0.048), as well as age of first walking unaided (β = -0.16, P = 0.015).
Contribution of Socioeconomic Factors, IQ, ASD Severity, and Early Signs of Developmental Abnormalities to ABAS-II Practical Skills
Table 7 shows the hierarchical regression model examining how socioeconomic factors, IQ, ASD severity and early signs of developmental abnormalities impact ABAS-II practical skills. The total model also had good interpretation with 56.0% of variance (P < 0.001). Age and gender still did not account for any significant variance in step 1 (F = 1.46, P = 0.237). Socioeconomic factors contributed to an additional 8.1% of variance in step 2 (ΔF = 4.32, P = 0.006), and maternal highest education was positively associated with practical skills in the total model (β = 0.14, P = 0.043). FSIQ contributed an additional 31.2% variance in step 3 (ΔF = 75.94, P < 0.001), thereby indicating that IQ still had the largest contribution to practical skills, similar to the case with conceptual skills. VAI and NVI contributed an additional 7.2% of variance in step 4 (ΔF = 9.85, P < 0.001). VAI also emerged as a specific predictor to practical skills, as was the case with conceptual skills in the total model (β = 0.40, P = 0.001), rather than NVI (β = -0.32, P = 0.159). Although ADOS-Css was negatively correlated with practical skills in the total model (β = -0.14, P = 0.041), the scores did not account for any significant variance in step 5 (ΔF = 0.63, P = 0.428). In the final step, age of first walking unaided remained as a unique predictor of practical skills (β = -0.23, P < 0.001).
Discussion
Cognitive-adaptive Functioning Gap
Our results demonstrate a substantial discrepancy between IQ and each domain of adaptive skills in children with ASD having IQ ≥ 70. In this study, we included age and age at diagnosis as covariables to reduce influence of these factors on the results. The results show that IQ is an important factor for the gap of IQ-adaptive behavior in preschool children, as well as in verbal and nonverbal IQ domain. Cognitive functioning may be more important in preschool-aged children than in school-aged children or adolescents, possibly because of the coexistence of other psychiatric symptoms, such as emotional disorders, anxiety and depression, in older children, which may further compromise adaptive functioning. High-functioning autism (HFA) is a term widely used in both research and clinical practice to define children with ASD who have an IQ ≥ 70. Individuals classified with HFA are expected to have milder symptoms and better outcomes than their counterparts. However, recent studies have argued that HFA does not appropriately reflect the level of adaptive functioning in children with IQ evaluated of ≥ 70 (Alvares, et al., 2020). The results of our study are consistent with the contention that HFA is a misnomer when defined merely on the basis of IQ. The use of IQ cut-offs as a measure of adaptive functioning may be misleading regarding the functional ability of children with ASD, thereby resulting in biased assignment of supportive services and funds from government. Therefore, clinicians should fully analyze the differences in cognitive functioning and specific domains of adaptive functioning before planning individualized interventions.
IQ and Adaptive Functioning
The present study highlights that IQ is the most important factor influencing adaptive ability in preschool-aged children with ASD. In this study, adaptive skills in all domains were lower than IQ scores in the group with IQ ≥ 70, while the opposite pattern was existing in the group with IQ < 70 - adaptive skills in all domains were actually higher than IQ scores. The results suggest that adaptive impairment is more severe in ASD children with having IQ ≥ 70, while intellectual impairment is more severe in ASD children with having IQ < 70. Although the relationship between IQ and adaptive functioning has been reported in preschool children with ASD, the majority of the existing study reports do not clarify whether verbal or nonverbal IQ accounts for this relationship (Pathak, et al., 2019; Yang, et al., 2016). Considering that children with ASD show certain differences in the intelligence structure, we analyzed the influence of the verbal and nonverbal components separately, which may greatly alleviate the influence of the difference in cognitive structure. Though this study shows that there do not appear to be any differences in mean value between VAI and NVI both in the two groups, the reason may be mainly due to the highly heterogeneity in children with ASD. The hierarchical regression models indicate that verbal IQ has a significantly predictive effect on adaptive functioning for children with ASD, while nonverbal IQ has no significant association with adaptive functioning. Differences between verbal IQ and nonverbal IQ have been reported to be more frequent in children with ASD than in typical development (Ankenman, et al., 2014), thereby suggesting that differences in intelligence structure may be an important feature of ASD. The intelligence structure of children with ASD is often known to be unbalanced, with performance scores being greater than scores of verbal abilities and distinctive patterns seen in the subtests; children with ASD have been shown to have relatively good visuospatial ability, but poor verbal comprehension (Al-Mamari, et al., 2021; Cardillo, et al., 2018; Charman, et al., 2011). In fact, a recent study has shown that verbal IQ is most closely associated with low ASD symptom severity and that the correlations between performance IQ and IQ discrepancy were not significant enough to predict ASD symptoms; this suggests that verbal IQ may be a factor that can be used for subtyping ASD (Johnson, et al., 2021). Put together, these findings support our argument that verbal IQ can be a specific predictor of adaptive functioning in preschool children with ASD.
SES and Adaptive Functioning
Socioeconomic factors were found to have a significant impact on the adaptive functioning of children with ASD in the second step of hierarchical regression model, with maternal educational level being positively correlated to adaptive functioning. In fact, only maternal educational level was positively associated with overall adaptive skills and practical skills of children with ASD after taking into account IQ, ASD severity, and early signs of developmental abnormalities. The practical skills in ABAS-II include self-care, community adaptability, family life, and health and safety, which are closely related to the caregiver’s education level. The educational level of mothers may influence the manner in which individuals with ASD receive guidance for daily life skills and may therefore influence both practical skills and overall adaptive skills. Researchers focusing on the association between language development and SES in ASD; their findings have found that maternal education level is significantly associated with variability in expressive and receptive language in preschoolers with ASD, with lower SES indicating lower language skills (Olson, et al., 2021). A recent study argues that SES may be closely correlated with parental wellbeing index and competency, which are factors that further influence adaptive ability in preschoolers with ASD (Mathew, et al., 2019). In light of the results of previous studies on the relationship between SES and adaptive behaviors, we family income and parental background as important factors in our study, instead of simply using the total score of SES. The disadvantages of using total percentiles of SES as a measure of SES in individual with ASD has been shown previously (Hodge, et al., 2021). However, we were unable to evaluate other social support factors, such as family educational method and the degree of social support. Further systematic exploration is necessary to determine the impact of family ecosystem and social support factors on adaptive behavior in children with ASD.
ASD Severity and Adaptive Functioning
Some studies have reported an association between the severity of ASD and adaptive functioning (Golya & McIntyre, 2018; Kenworthy, et al., 2010), and evidence has shown that ASD children with greater severity and lower social interest exhibit more rapidly declining trajectories of adaptive abilities than their counterparts (Franchini, et al., 2018). In our study, Although ASD severity was negatively correlated with social and practical skills in the total models, it did not contribute any significant variance for overall and domain-specific adaptive skills. A possible explanation for this is that verbal IQ was mainly relevant to low symptom severity, as discussed above, and the variance in ASD severity to account for adaptive skills was not significant when including verbal IQ. Our results are consistent with those of previous studies that have shown no significant correlation between autistic symptomatology and adaptive ability (Ray-Subramanian, et al., 2011; Yang, et al., 2016), in the presence of strict calibration for differences in age and language level. A previous longitudinal study revealed only a small yoking of developmental trajectories in autistic severity and adaptive behavior during the preschool years in ASD (Szatmari, et al., 2015), thereby suggesting that the correlation between ASD severity and adaptive ability over time is complex. To rigorously explore the correlation between ASD severity and adaptive functioning, we used ADOS to evaluate symptom severity rather than ADI-R. ADI-R has two versions—one for children of 2–4 years and another for children above 4 years—and the diagnostic algorithms mainly contain the most abnormal conditions observed at 4–5 years of age. Therefore, ADI-R cannot accurately reflect the current symptom severity of ASD for children with ASD aged above 4 years. To sum up, the present study argues that the severity of ASD symptoms has no significant contribution to the prediction of adaptive functioning.
Early Signs of Developmental Abnormalities and Adaptive Functioning
Our study on the relationship between early signs of developmental abnormalities and adaptive functioning revealed that the age of first walking unaided had an independent negative correlation with adaptive skills of ASD, whereas age of first single words and phrases failed to predict adaptive functioning. Age of first walking unaided was found to be an independent indicator of children’s motor development, which implies that motor ability may have a significant impact on adaptive functioning. The discrepancy in the motor skills of individuals with ASD may explain the variability in adaptive behaviors. A recent study has shown that poorer motor skills (especially manual dexterity) were closely associated with lower adaptive behaviors in children with ASD (Fears, et al., 2022). Age of first single words and phrases is closely related to expressive language rather than receptive language and, therefore, only partly reflects early language ability. However, an individual with ASD may have typical development in early expressive language, but poor understanding and acceptance of language, which could contribute to impairment in adaptive functioning. Moreover, in this study, we did not account for the development of fine motor skills, and the potential role of motor skill difficulties in mediating impairment of adaptive functioning in children with ASD warrants further exploration.
Strengths and Limitations
The current study is the first to examine cognitive-adaptive functioning gap in Chinese children with ASD. This study is unique in the following respects: (1) The impact of verbal IQ and nonverbal IQ on adaptive functioning were separately analyzed to evaluate the IQ-adaptive functioning gap. (2) The study population was rigorously calibrated for age, age at diagnosis, and IQ. (3) The contributions of socioeconomic factors, IQ, early signs of developmental abnormalities, and ASD severity to adaptive functioning were further assessed to help develop strategies for clinical diagnosis and individualized intervention. However, only a few socioeconomic factors were included in this study. The family ecosystem and social support factors should be more systematically analyzed to interpret how socioeconomic factors impact adaptive functioning, in order to facilitate the development of strategies for better support systems to improve the prognosis of children with ASD. Furthermore, the value of using IQ scores for children as young as 2.5 years old is debatable. In future, longitudinal studies on the relationship between the development trajectory of adaptive functioning and IQ are warranted, while also accounting for the variation and heterogeneity of development in preschool-aged children with ASD.
To summarize, our findings show that IQ-adaptive functioning gap is significant in children with ASD having IQ ≥ 70, suggesting that defining HFA merely on the basis of IQ is not appropriate. We also found that verbal IQ and early signs of motor development are specific and possible predictors of adaptive functioning of children with ASD, respectively.
Data Availability
All relevant raw data, will be freely available to any researcher wishing to use them for non-commercial purposes, without breaching participant confidentiality. The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Al-Mamari, W., Idris, A. B., Gabr, A., Jalees, S., Al-Jabri, M., Abdulrahim, R., Al-Mujaini, A., Islam, M. M., Al-Alawi, M., & Al-Adawi, S. (2021). Intellectual Profile of Children with Autism Spectrum Disorder: Identification of verbal and nonverbal subscales predicting intelligence quotient. Sultan Qaboos Univ Med J, 21(3), 386–393. https://doi.org/10.18295/squmj.4.2021.001
Alvares, G. A., Bebbington, K., Cleary, D., Evans, K., Glasson, E. J., Maybery, M. T., Pillar, S., Uljarević, M., Varcin, K., Wray, J., & Whitehouse, A. J. (2020). The misnomer of ‘high functioning autism’: Intelligence is an imprecise predictor of functional abilities at diagnosis. Autism, 24(1), 221–232. https://doi.org/10.1177/1362361319852831
Ankenman, K., Elgin, J., Sullivan, K., Vincent, L., & Bernier, R. (2014). Nonverbal and verbal cognitive discrepancy profiles in autism spectrum disorders: Influence of age and gender. Am J Intellect Dev Disabil, 119(1), 84–99. https://doi.org/10.1352/1944-7558-119.1.84
APA (2013). Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-5). American Psychiatric Publishing. https://doi.org/10.1176/appi.books.9780890425596
Bölte, S., Mahdi, S., de Vries, P. J., Granlund, M., Robison, J. E., Shulman, C., Swedo, S., Tonge, B., Wong, V., Zwaigenbaum, L., Segerer, W., & Selb, M. (2019). The Gestalt of functioning in autism spectrum disorder: Results of the international conference to develop final consensus International Classification of Functioning, Disability and Health core sets. Autism, 23(2), 449–467. https://doi.org/10.1177/1362361318755522
Bradshaw, J., Gillespie, S., Klaiman, C., Klin, A., & Saulnier, C. (2019). Early emergence of discrepancy in adaptive behavior and cognitive skills in toddlers with autism spectrum disorder. Autism, 23(6), 1485–1496. https://doi.org/10.1177/1362361318815662
Cardillo, R., Menazza, C., & Mammarella, I. C. (2018). Visuoconstructive abilities and visuospatial memory in autism spectrum disorder without intellectual disability: Is the role of local bias specific to the cognitive domain tested? Neuropsychology, 32(7), 822–834. https://doi.org/10.1037/neu0000472
Charman, T., Pickles, A., Simonoff, E., Chandler, S., Loucas, T., & Baird, G. (2011). IQ in children with autism spectrum disorders: Data from the Special needs and Autism Project (SNAP). Psychological Medicine, 41(3), 619–627. https://doi.org/10.1017/s0033291710000991
Chatham, C. H., Taylor, K. I., Charman, T., Liogier, D., Eule, X., Fedele, E., Hardan, A., Loth, A. Y., Murtagh, E., Del Valle Rubido, L., Caceres, M. S. J., Sevigny, A., Sikich, J., Snyder, L., Tillmann, L., Ventola, J. E., Walton-Bowen, P. E., Wang, K. L., Willgoss, P. P., T., & Bolognani, F. (2018). Adaptive behavior in autism: Minimal clinically important differences on the Vineland-II. Autism Research, 11(2), 270–283. https://doi.org/10.1002/aur.1874
Cohen, J. (1988). Statistical power analysis for the behavioral sciences (2nd ed.).). Lawrence Erlbaum.
Fears, N. E., Palmer, S. A., & Miller, H. L. (2022). Motor skills predict adaptive behavior in autistic children and adolescents. Autism Research, 15(6), 1083–1089. https://doi.org/10.1002/aur.2708
Franchini, M., Zöller, D., Gentaz, E., Glaser, B., de Wood, H., Kojovic, N., Eliez, S., & Schaer, M. (2018). Early adaptive functioning Trajectories in Preschoolers with Autism Spectrum Disorders. Journal Of Pediatric Psychology, 43(7), 800–813. https://doi.org/10.1093/jpepsy/jsy024
Golya, N., & McIntyre, L. L. (2018). Variability in adaptive behaviour in young children with autism spectrum disorder. Journal Of Intellectual Developmental Disability, 43(1), 102–111. https://doi.org/10.3109/13668250.2017.1287886
Gotham, K., Risi, S., Pickles, A., & Lord, C. (2007). The Autism Diagnostic Observation schedule: Revised algorithms for improved diagnostic validity. Journal Of Autism And Developmental Disorders, 37(4), 613–627. https://doi.org/10.1007/s10803-006-0280-1
Gotham, K., Pickles, A., & Lord, C. (2009). Standardizing ADOS scores for a measure of severity in autism spectrum disorders. Journal Of Autism And Developmental Disorders, 39(5), 693–705. https://doi.org/10.1007/s10803-008-0674-3
Hodge, M. A., Boulton, K. A., Sutherland, R., Barnett, D., Bennett, B., Chan, E., Cramsie, J., Drevensek, S., Eapen, V., Ganesalingam, K., Masi, A., Ong, N., Williamsz, M., Guastella, A. J., & Silove, N. (2021). Predictors of adaptive functioning in preschool aged children with autism spectrum disorder. Autism Research, 14(7), 1444–1455. https://doi.org/10.1002/aur.2501
Johnson, C. N., Ramphal, B., Koe, E., Raudales, A., Goldsmith, J., & Margolis, A. E. (2021). Cognitive correlates of autism spectrum disorder symptoms. Autism Research, 14(11), 2405–2411. https://doi.org/10.1002/aur.2577
Kanne, S. M., Gerber, A. J., Quirmbach, L. M., Sparrow, S. S., Cicchetti, D. V., & Saulnier, C. A. (2011). The role of adaptive behavior in autism spectrum disorders: Implications for functional outcome. Journal Of Autism And Developmental Disorders, 41(8), 1007–1018. https://doi.org/10.1007/s10803-010-1126-4
Kenworthy, L., Case, L., Harms, M. B., Martin, A., & Wallace, G. L. (2010). Adaptive behavior ratings correlate with symptomatology and IQ among individuals with high-functioning autism spectrum disorders. Journal Of Autism And Developmental Disorders, 40(4), 416–423. https://doi.org/10.1007/s10803-009-0911-4
Klin, A., Saulnier, C. A., Sparrow, S. S., Cicchetti, D. V., Volkmar, F. R., & Lord, C. (2007). Social and communication abilities and disabilities in higher functioning individuals with autism spectrum disorders: The Vineland and the ADOS. Journal Of Autism And Developmental Disorders, 37(4), 748–759. https://doi.org/10.1007/s10803-006-0229-4
Kraper, C. K., Kenworthy, L., Popal, H., Martin, A., & Wallace, G. L. (2017). The gap between adaptive behavior and intelligence in Autism Persists into Young Adulthood and is linked to Psychiatric co-morbidities. Journal Of Autism And Developmental Disorders, 47(10), 3007–3017. https://doi.org/10.1007/s10803-017-3213-2
Li, Y., & Qiu, Z. (2016). Standardization of adaptive Behavior Assessment System-II Chinese version. Chinese Journal of Rehabilitation Theory and Practice, 22(04), 378–382. https://kns.cnki.net/kcms/detail/11.3759.R.20160623.1149.066.html
Liss, M., Harel, B., Fein, D., Allen, D., Dunn, M., Feinstein, C., Morris, R., Waterhouse, L., & Rapin, I. (2001). Predictors and correlates of adaptive functioning in children with developmental disorders. Journal Of Autism And Developmental Disorders, 31(2), 219–230. https://doi.org/10.1023/a:1010707417274
Lord, C., Rutter, M., DiLavore, P., & Risi, S. (2002). Autism Diagnostic Observation schedule: ADOS manual. Western Psychological Services.
Lord, C., Elsabbagh, M., Baird, G., & Veenstra-Vanderweele, J. (2018). Autism spectrum disorder. Lancet, 392(10146), 508–520. https://doi.org/10.1016/s0140-6736(18)31129-2
Maltman, N., DaWalt, L. S., Hong, J., & Mailick, M. (2021). Brief report: Socioeconomic factors Associated with minimally verbal status in individuals with ASD. Journal Of Autism And Developmental Disorders, 51(6), 2139–2145. https://doi.org/10.1007/s10803-020-04646-6
Mathew, N. E., Burton, K. L. O., Schierbeek, A., Črnčec, R., Walter, A., & Eapen, V. (2019). Parenting preschoolers with autism: Socioeconomic influences on wellbeing and sense of competence. World J Psychiatry, 9(2), 30–46. https://doi.org/10.5498/wjp.v9.i2.30
Mayes, S. D., & Calhoun, S. L. (2011). Impact of IQ, age, SES, gender, and race on autistic symptoms. Res autism spect dis, 5(2), 749–757.
McQuaid, G. A., Pelphrey, K. A., Bookheimer, S. Y., Dapretto, M., Webb, S. J., Bernier, R. A., McPartland, J. C., Van Horn, J. D., & Wallace, G. L. (2021). The gap between IQ and adaptive functioning in autism spectrum disorder: Disentangling diagnostic and sex differences. Autism, 25(6), 1565–1579. https://doi.org/10.1177/1362361321995620
Mouga, S., Almeida, J., Café, C., Duque, F., & Oliveira, G. (2015). Adaptive profiles in autism and other neurodevelopmental disorders. Journal Of Autism And Developmental Disorders, 45(4), 1001–1012. https://doi.org/10.1007/s10803-014-2256-x
Oakland, T., & Harrison, P. (2008). Adaptive Behavior Assessment System-II: Clinical use and interpretation. Elsevier.
Olson, L., Kinnear, M., Chen, B., Reynolds, S., Ibarra, C., Wang, T., Linke, A., & Fishman, I. (2021). Socioeconomic factors account for variability in Language Skills in Preschoolers with Autism Spectrum Disorders. Journal Of Developmental And Behavioral Pediatrics, 42(2), 101–108. https://doi.org/10.1097/dbp.0000000000000870
Pathak, M., Bennett, A., & Shui, A. M. (2019). Correlates of adaptive behavior profiles in a large cohort of children with autism: The autism speaks Autism Treatment Network registry data. Autism, 23(1), 87–99. https://doi.org/10.1177/1362361317733113
Pugliese, C. E., Anthony, L., Strang, J. F., Dudley, K., Wallace, G. L., & Kenworthy, L. (2015). Increasing adaptive behavior skill deficits from childhood to adolescence in autism spectrum disorder: Role of executive function. Journal Of Autism And Developmental Disorders, 45(6), 1579–1587. https://doi.org/10.1007/s10803-014-2309-1
Ray-Subramanian, C. E., Huai, N., & Ellis Weismer, S. (2011). Brief report: Adaptive behavior and cognitive skills for toddlers on the autism spectrum. Journal Of Autism And Developmental Disorders, 41(5), 679–684. https://doi.org/10.1007/s10803-010-1083-y
Rutter, M., Le Couteur, A., & Lord, C. (2003). Autism Diagnostic interview-revised. Western Psychological Services.
Sun, X., Allison, C., Auyeung, B., Zhang, Z., Matthews, F. E., Baron-Cohen, S., & Brayne, C. (2015). Validation of existing diagnosis of autism in mainland China using standardised diagnostic instruments. Autism, 19(8), 1010–1017. https://doi.org/10.1177/1362361314556785
Szatmari, P., Georgiades, S., Duku, E., Bennett, T. A., Bryson, S., Fombonne, E., Mirenda, P., Roberts, W., Smith, I. M., Vaillancourt, T., Volden, J., Waddell, C., Zwaigenbaum, L., Elsabbagh, M., & Thompson, A. (2015). Developmental trajectories of symptom severity and adaptive functioning in an inception cohort of preschool children with autism spectrum disorder. JAMA Psychiatry, 72(3), 276–283. https://doi.org/10.1001/jamapsychiatry.2014.2463
Troyb, E., Knoch, K., Herlihy, L., Stevens, M. C., Chen, C. M., Barton, M., Treadwell, K., & Fein, D. (2016). Restricted and repetitive behaviors as predictors of Outcome in Autism Spectrum Disorders. Journal Of Autism And Developmental Disorders, 46(4), 1282–1296. https://doi.org/10.1007/s10803-015-2668-2
Watkins, M. W., Canivez, G. L., Dombrowski, S. C., McGill, R. J., Pritchard, A. E., Holingue, C. B., & Jacobson, L. A. (2022). Long-term stability of Wechsler Intelligence Scale for Children-fifth edition scores in a clinical sample. Appl Neuropsychol Child, 11(3), 422–428. https://doi.org/10.1080/21622965.2021.1875827
Wechsler, D. (2012). Wechsler Preschool and primary scale of Intelligence-Fourth Edition (WPPSI-IV) Pearson. NCS Pearson.
Yang, S., Paynter, J. M., & Gilmore, L. (2016). Vineland Adaptive Behavior Scales: II Profile of Young Children with Autism Spectrum Disorder. Journal Of Autism And Developmental Disorders, 46(1), 64–73. https://doi.org/10.1007/s10803-015-2543-1
Ye, Q., Liu, L., Lv, S., Cheng, S., Zhu, H., Xu, Y., Zou, X., & Deng, H. (2021). The Gestures in 2-4-year-old children with Autism Spectrum Disorder. Frontiers In Psychology, 12, 604542. https://doi.org/10.3389/fpsyg.2021.604542
Zhang, H. (2009). The revision of WISC-IV chinese version. Psychological Science, 32(05), 1177–1179. https://doi.org/10.16719/j.cnki.1671-6981.2009.05.026
Acknowledgements
We are grateful to all children and their parents participating in the study. We wish to appreciate our colleagues who provide significant comments and professional support on data collection and methodology.
Funding
This study was supported by Medical Science and Technology Research Foundation of Guangdong Province (A2022039), National Natural Science Foundation of China (81471017), Science and Technology Program of Guangzhou in China (202007030011).
Author information
Authors and Affiliations
Contributions
SHW acquired, analyzed and interpreted the data. QZ designed statistical methodology. Data collection and professional evaluation were performed by KYC, CY, YX, YYZ, GDZ. CQC provided professional support on methodology. HZD revised it critically for important intellectual content. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The current study was approved by the Third Affiliated Hospital of Sun Yat-sen University Research Ethics Committee (Approve No: [2022]02-245-01). All parents have signed consent forms for the use of the clinical data, which might be used in future scientific research. This article does not contain any studies with animals performed by any of the authors.
Consent for publication
All authors agreed the possible publication of our article on Journal of Autism and Developmental Disorders.
Competing interests
The authors declare that they have no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Wang, Sh., Zhou, Q., Chen, Ky. et al. Cognitive-adaptive Functioning Gap and Mediating Factors that Impact Adaptive Functioning in Chinese Preschool-aged Children with Autism Spectrum Disorder. J Autism Dev Disord 54, 3107–3121 (2024). https://doi.org/10.1007/s10803-023-06029-z
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-023-06029-z