
Abstract
In Lebanon, no estimate for autism prevalence exists. This cross-sectional study examines the prevalence of Autism spectrum disorder (ASD) in toddlers in nurseries in Beirut and Mount-Lebanon. The final sample included 998 toddlers (16–48 months) from 177 nurseries. We sent parents the Modified Checklist for Autism in Toddlers (M-CHAT) for screening, and a self-administered questionnaire (associated factors). We imputed missing M-CHAT data with successful answers. Since there were no follow-up interviews for the M-CHAT, we used the positive predictive value (0.058) from a large study for prevalence estimates. ASD prevalence was 1 in 66 children (comparable to US). Ratios were: male/female: 1.05; Beirut/Mount-Lebanon: 1.2. Using a more representative sample and ascertaining results are needed for better prevalence estimates in Lebanon.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Autism spectrum disorder (ASD) is a neurodevelopmental disorder that is characterized by impaired social communication and interactions, repetitive behaviors, restricted interests and persistence on sameness (American Psychiatric Association 2013a). Once considered rare, ASD is now increasing in prevalence. For example, in 2010, The Center for Disease Control and Prevention (CDC) estimated the prevalence of autism to be 1 in 68 children, approximately two times higher than the estimate of 2000. These estimates come from data collected from health and special education records of 8 year-old children in 11 areas in the United States in 2010 through the Autism and Developmental Disabilities Monitoring (ADDM) network (CDC 2014a). Furthermore, CDC reported a mean ASD prevalence of 1 % based on studies conducted in Asia, Europe and North America, which is 19 times higher than the median prevalence estimate of autism of 5.2 per 10,000 found by Fombonne in a 1999 review of 23 studies (CDC 2014b; Fombonne 1999). In a recent review of 43 studies in 17 countries, Fombonne (2009) found a 20.6 per 10,000 average prevalence of autism, a fourfold increase from his 1999 review. This increase in the number of autism cases may be attributed to several factors including the growing awareness of the condition, the expanded definition of autism or a true increase in incidence of autism (NIMH 2012).
Despite the abundance of research on autism world-wide, there is a scarcity of studies on autism burden in the Eastern Mediterranean Region and a wide variation in reported prevalence among the few small scale studies conducted. For instance, the prevalence of ASD was estimated to be 29 per 10,000 in the United Arab Emirates when using a DSM-IV diagnosis of pervasive developmental disorder (PDD) (Eapen et al. 2007) compared to 4.3 per 10,000 in Bahrain (Al-Ansari and Ahmed 2013). The Sultanate of Oman had an even lower prevalence of 1.4 per 10,000 in children less than 14 years based on data retrieved from all hospitals and social institutions that offer targeted services to ASD patients (Al-Farsi et al. 2011). On the other hand, evidence from child psychiatry clinics in the Kingdom of Saudi Arabia (KSA) points to a higher rate of ASD, with 1250 per 10,000 in children younger than 18 years (Al-Habeeb et al. 2012). Further anecdotal evidence from KSA suggests that this number is even higher with a predicted prevalence of autism of 1 in 50 children (Saudi Gazette Report 2014).
In Lebanon and neighboring Arab countries (Syria, Jordan, Palestine), there are no estimates on the prevalence of autism. However, the prevalence of pervasive developmental disorders was found to be 1 % in adolescents in Beirut (F. Maalouf, personal communication, February 26, 2015). In addition, data collected at the American University of Beirut Medical Center (AUBMC) Special Kids Clinic indicate that the number of pediatric patients with ASD is increasing. The lack of data coupled with the increasing number in clinics underscore the necessity of studying the prevalence of ASD in Lebanon.
Identification of autism cases occurs at different ages, most commonly when kids are in school around the age of 8 years (Fombonne 2009). Evidence based research has shown that intensive behavioral intervention implemented at an early age stage improves learning and communication and enhances social and verbal skills (Autism Speaks 2012). Promising interventions can start as early as the first year of life and are beneficial in reducing the stress on parents and the cost of later treatment (Koegel et al. 2014). Treatment and care for autism are very costly and are estimated at ~3 million US dollars over the individual’s lifespan with a total of 35 billion US dollars for all autistic people annually (Moldin and Rubenstein 2006). This highlights the importance of early diagnosis and treatment.
The objective of this study was to assess the prevalence of autism spectrum disorder in toddlers aged between 18 and 30 months in nurseries in Lebanon using a screening instrument, and to calculate gender and governorate specific rates.
Methods
This was a cross-sectional study of children in nurseries located in two governorates in Lebanon.
Participants
The target population was children, from both genders and all ethnic groups, aged 18–30 months going to nurseries in the capital city, Beirut and Mount Lebanon (ML) the latter being the largest governorate in Lebanon with 41.06 % of the population. The two governorates represent 50 % of the Lebanese population (CAS 2009). Moreover, the choice of the two governorates lies in the fact that the percentage of Lebanese children 0–4 years attending registered nurseries in these areas is higher than in other governorates (12 % for Beirut and Mount Lebanon as compared to 1, 2 and 2.6 %, respectively, for the North, South and Bekaa governorates) (MOPH 2014; CAS 2009). Moreover, nurseries in the other governorates are more dispersed and fewer in number compared to those in the capital and ML. There are 36 nurseries in Beirut and 190 in Mount Lebanon versus 26 nurseries in the Bekaa, 30 nurseries in the North and 19 nurseries in the South (MOPH 2014). Excluded were children with both non-Lebanese parents and children in nurseries in Palestinian camps because this is part of a larger study examining the genetics of autism in the Lebanese population.
The sampling frame was a listing of registered nurseries in the syndicate of nurseries provided by the Ministry of Public Health. The frame was updated during field work by spot checking. Updating the frame has two main benefits: decreasing selection bias and reaching a larger population. A minimum sample size of 2610 was required, correcting for a finite population. Given the high expected non-response rate, we decided to include all eligible children.
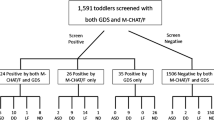
A total of 177 registered and unregistered nurseries in Beirut and Mount Lebanon were reached between February and September 2014 (Fig. 1). Of these, 32 nurseries were in Beirut with 27 registered and 5 unregistered. There were 145 nurseries in Mount Lebanon of which 126 are registered and 19 unregistered. From these nurseries, a total of 1216 children between 9 and 74 months, a wider age range than required, responded to the survey. Nine hundred nighty eight children between 16 and 48 months of age were included in the study. The age range was expanded from 18–30 to 16–48 months. The lowest bound was changed from 18 to 16 months since the screening instrument has been validated for toddlers aged 16–30 months (Robins et al. 2001).The upper bound was expanded from 30 to 48 since the screening instrument has been previously used in other studies for children that are up to 48 months old (Albores-Gallo et al. 2012; Glascoe et al. 2006).

Study participation flowchart
Screening Instrument and Other Data Collection Tools
Two instruments for data collection were used: the Modified Checklist for Autism in Toddlers (M-CHAT) as a screening tool for Autism Spectrum Disorder and a short structured questionnaire developed by researchers in this study.
The M-CHAT is an extension of the CHAT (Checklist for Autism in Toddlers). It comprises 23 yes/no questions answered by parents of children aged 16–30 months. The psychometric properties of M-CHAT with a follow-up questionnaire are very good, with a sensitivity of 0.87, a specificity of 0.99, a positive predictive value of 0.80, which is 0.36 without follow-up interview, and a negative predictive value of 0.99 (Robins et al. 2001). In a more recent study, Robins (2008) reported the positive predictive value to be 0.57 with follow-up interview and 0.058 when the follow-up interview is not conducted. The discrepancy between the positive predictive value in the initial study and the 2008 study could be explained by two major limitations of the 2001 study: results might have been inflated due to combining respondents from the early intervention group and the unselected population and lack of longitudinal data to obtain accurate measures (Robins and Dumont-Mathieu 2006). Previously the scoring system of the M-CHAT was based on either failing at least three items or failing at least two critical items (critical items being items number 2, 7, 9, 13, 14 and 15, see Table 3). The latest recommended scoring of the M-CHAT is based only on the total scoring system, with the child being at risk for ASD if he/she fails 3 items or more, disregarding whether items are critical or not (Robins 2013). The M-CHAT developed originally in English is now available in many languages (Arabic, Chinese, Czech, Dutch, and others), but has not been validated in all (Robins 2013). The Arabic version was validated in a study involving participants from nine Arab countries (Egypt, Kuwait, Jordan, Lebanon, Oman, Qatar, Saudi Arabia, Syria and Tunisia). The Arabic M-CHAT has a sensitivity of 0.86, a specificity of 0.80 and a positive predictive value of 0.88 (Seif Eldin et al. 2008). Permission to use the Arabic version of the M-CHAT was obtained from both the initial team who developed it and from the team who validated it in Arabic (Drs. Robins and Rashad).
A small structured questionnaire was also developed and administered. It included characteristics of the children (birth weight, vaccines, age at first word, frequency of visiting a pediatrician, history of being diagnosed with autism); factors related to pregnancy and delivery (maternal complications and moral support); and socio-demographic and behavioral characteristics of the parents (education level, occupation, and family history of mental health problems).
Procedures
After securing the approval of the Institutional Review Board (IRB) at the American University of Beirut (AUB), a support letter addressed to nursery directors and the list of nurseries were obtained from the Ministry of Public Health. Then, the investigators approached nursery directors (from registered and unregistered nurseries) and explained to them the aims of the study. If directors consented to participate in the study, field workers provided them with a number of envelopes equivalent to the number of children between 18 and 30 months of age in their nurseries. A closed box with a unique identifier for each nursery was placed at the nursery for parents to put back the envelopes once they completed filling the questionnaires. Each envelope contained a small memo prepared by the research team that explains the study in brief of which the director of the nursery was aware. It also contained a consent form comprising detailed explanation of the study and addressing risks and benefits of the study to the parents, a small questionnaire that was prepared and the M-CHAT. The questionnaire that could accommodate information for two children and two copies of the M-CHAT were provided to account for twins or two children in this age category. Since the study was anonymous and there were no means for researchers to contact parents whose child(ren) was/were potentially autistic, a fact sheet with information about signs and symptoms of ASD and names and telephones of some centers that deal with the diagnosis and treatment of ASD was also provided in the file. Nursery directors were asked to give the file to parents of eligible children at pick-up or drop-off from the nursery. Parents who consented to participate then filled the questionnaire and the M-CHAT form, placed them in a sealed envelope that was provided, and dropped it in the closed box at the nursery. Field workers made several visits to nurseries to collect the boxes which were then delivered to the university and opened by the research team.
Statistical Analysis
Data were entered using software EpiData version 3.1. The major statistical challenge in this study was related to the M-CHAT. One hundred sixty respondents (16 %) did not answer five or less items of the M-CHAT. Missing data on five or less items of the M-CHAT was imputed by replacing missing values with the most frequent answer by all respondents to each item (in this case the successful answer). Since no follow-up interview for the M-CHAT was conducted to ascertain results, the final prevalence estimate was obtained by multiplying results of the M-CHAT by the positive predictive value of M-CHAT without interview determined in a large scale study (0.058) (Robins 2008). For descriptive analysis, frequencies and percentages (for categorical variables) and means and standard deviations (for continuous variables) were generated. Prevalence of ASD was computed with a 95 % confidence interval. Gender and governorate specific rates were calculated.
Results
Population Profile
The characteristics of the sample are presented in Table 1. The average age of toddlers was 27.6 (±6.8) months with 54 % of the toddlers being males. Being the first born child represented more than half of the study population (58 %). The majority of mothers and fathers had at least a bachelor’s degree (83 and 64 % for mothers and fathers, respectively), and were employees or self-employed during the past 12 months (79 and 100 % for mothers and fathers, respectively). A higher proportion of the sample was from Mount Lebanon (78 %). A total of 15 toddlers had already been diagnosed with autism by a physician (1.5 %) as reported by parents in the questionnaire. Four were females, ten were males and one was of unknown gender.
Prevalence Rates of Autism Spectrum Disorders
Prevalence rates according to the M-CHAT without follow-up and corrected prevalence rates are presented in Table 2. Out of 998 toddlers, 263 (26 %) failed 3 or more items of the 23 items of the M-CHAT, and hence were labeled as possibly having ASD. Using a positive predictive value of 0.058, the final prevalence estimate of ASD was 1.53 % [95 % CI 0.77–2.29]. The male to female ratio was 1.05 (1 in 65 for males and 1 in 67 for females). The Beirut to Mount Lebanon ratio was 1.2 (1 in 57: Beirut and 1 in 68: Mount Lebanon). Out of the 15 children diagnosed by a physician as having ASD, 10 were captured by the M-CHAT.
The percentages of failures in each item of the M-CHAT are summarized in Table 3. Item 1 (does your child enjoy being swung, bounced on your knees?) was the most commonly failed item (22.7 %), followed by item 7 (does your child ever use his/her index finger to point, to indicate interest in something?) (16.7 %), followed by item 6 (does your child ever use his/her index finger to point, to ask for something?) (13.9 %). When segregated by gender, male toddlers’ top 3 failed items were 1, 7 and 6 (22.3, 17.1, and 15.3 %, respectively). While for females, the two most failed items were the same as for male toddlers (items 1 and 7: 23.3 and 16.3 %), however, the third most failed item for females was item 4 (does your child enjoy playing peek-a-boo/hide-and-seek?) (12.8 %). The least failed item for both genders was item 16 (does your child walk?) (0 and 0.9 % failed for males and females respectively).
Discussion
Results from this cross-sectional study estimated a prevalence of ASD of 153 per 10,000 which is similar to the prevalence of 147 per 10,000 reported by the CDC (CDC 2014a). Prevalence found in this study is higher than published figures from Arab nations such as the United Arab Emirates (29 per 10,000) (Eapen et al. 2007), Bahrain (4.3 per 10,000) (Al-Ansari and Ahmed 2013), the Sultanate of Oman (1.4 per 10,000) (Al-Farsi et al. 2011). Prevalence among Lebanese toddlers is also higher than among Israeli Arabs (12 per 10,000) (Davidovitch et al. 2013). The prevalence of 153 per 10,000 in this study is almost seven times higher than the average prevalence of 20.6 per 10,000 reported in a 2009 review by Fombonne.
Difference in prevalence might be due to different age groups selected. In our study, we chose to study toddlers (16–48 months old) attending nurseries, while most studies include a population of school children with a mean age of 8 years (Fombonne 2009). Additionally, data on autism estimates in the US coming from the CDC Autism and Developmental Disabilities Monitoring (ADDM) Network was collected from 8 year-old children (CDC 2014a). In Oman, the population studied was 0–14 years of age (Al-Farsi et al. 2011). Data collection methods might also affect prevalence estimates. Prevalence estimates based on a screening instrument such as the one used here are usually much higher than estimates which are based on medical records data such as the one of the Sultanate of Oman, especially that researchers in the latter study used DSM-IV criteria which might also explain the lower prevalence rates (Al-Farsi et al. 2011) (153 compared to 1.4 per 10,000). This is also supported by Fombonne (2009) who reported in a review of 43 studies related to pervasive developmental disorders that population-based surveys yielded higher estimates than studies that used passive data collection techniques.
Furthermore, changes in diagnostic criteria and in the availability of services have been linked to increased estimates (Fombonne 2009). A study conducted in Northern Finland found that the prevalence of autism changes in the same data with different diagnostic criteria (Kielinen et al. 2000). Even when using the same instrument, such as the M-CHAT, for screening, it is hard to compare between different studies since the categorization of those at risk of ASD has changed. Initially, a child was at risk of ASD if he/she failed any 3 items or two critical items of the M-CHAT, whereas now risk of ASD is defined by failing any 3 items (Robins 2013).
While, the male to female ratio in this study (1.05:1) is not consistent with data coming from the US (5:1), Bahrain (4:1), Oman (3:1) and 4.2:1 as a mean ratio derived from 43 studies worldwide (CDC 2014a; Al-Ansari and Ahmed 2013; Al-Farsi et al. 2011; Fombonne 2009), there is a growing literature that gender ratio differences in autism are exaggerated. In fact, a recent study using the Spanish version of the M-CHAT in the Canary Islands reported the male to female ratio to be 0.8:1 (Sevilla et al. 2013) which questions the accuracy of the existence of a gender gap. Furthermore, a prospective prevalence study in the Faroe Islands of 15–24 year olds found a male to female ratio of 1.2:1 in the 2009 follow-up as compared to 5:1 in the 2002 original study, which might be due to lack of understanding of the clinical presentation of autism in females (Kocovska et al. 2012). Another study comparing diagnosed ASD cases in Jordan, Egypt and Saudi Arabia established male to female ASD ratios of 1:1 and 1.3:1, respectively in Jordan and Egypt (Amr et al. 2012). The apparent gender gap is proving to be the result of a boy-centric aspect to the diagnosis. This is especially relevant to the type of restrictive behaviors affecting girls and boys. For example, girls tend to have more socially appropriate restricted interests than boys (Skuse and Mandy 2015). Females with ASD also have more developed social skills than boys with ASD. A recent study found that females with ASD had similar scores on the friendship questionnaire like typically developing males (Head et al. 2014). The fact that symptomatology and underlying neuroanatomy of the brain differs in autistic girls versus boys lends credence to this, particularly with regards to Magnetic Resonance Imaging (MRI)/Diffusion Tension Imaging (DTI) results pertaining to the corpus callossum and differing size of specific callossal-cortex projections (Nordahl et al. 2015). Additionally, it is well-known that IQ impacts sex ratios in autism. For lower IQ levels (<70), girls have more social communication impairment and less cognitive ability compared to boys. For those with higher levels of IQ (>70), girls have lower prevalence of restricted interests. Also, a higher non-verbal IQ than a verbal IQ is used as a clinical indication of ASD. This discrepancy is less apparent in girls rendering it harder to them to be diagnosed as having ASD. Furthermore, females with ASD and low IQ are often misdiagnosed as just being intellectually disabled (Frazier et al. 2014). Consequently, DSM-V criteria account more to this gender difference in diagnosis: “In clinic samples, females tend to be more likely to show accompanying intellectual disability, which suggests that girls without accompanying intellectual disability or language delays may go unrecognized, perhaps because of subtler manifestation of social and communication difficulties” (American Psychiatric Association 2013b).
Indeed, in the current study when asked if the child was previously diagnosed by a physician as having ASD, the male to female ratio was 2.5:1, a gender ratio that is different from the one based on the M-CHAT. The 2.5–1 male to female ratio as diagnosed by physicians is comparable to results found among the 55,266 children 7–12 years old in a study in South Korea in a general population sample. Additionally, the South Korean study found the male-to-female ratio to be 5.1:1 in the high probability group, suggesting that the gender gap in ASD is smaller in the general population as compared to a high-risk population or group (Kim et al. 2011).
The main strength of this study is that it is the first prevalence study to be conducted on a population-based sample in Lebanon. We also tried to reach out to all nurseries in the two selected governorates to participate in this study including nurseries certified by the syndicate of nurseries and the Ministry of Public Health and those uncertified. In Lebanon, there are no national surveillance systems or national registries from where we could extract information about prevalence or incidence of autism as was done in other studies (CDC 2014a; Fombonne 2009). Consequently, screening in nurseries of a restricted geographical area provides a sound choice for a first exploratory study to be followed by a larger, more inclusive study in the future. Though nurseries are not used commonly for data collection, a French study looking at sex differences in social development used a nursery school to conduct their study (Barbu et al. 2011). We believe that reaching out to parents through nurseries is a good alternative since it allowed inclusion of working parents. If the study is to be conducted on a national scale, it would be important to think of an alternative way of collecting data in rural areas where fewer children might attend nurseries.
The low response of parents does not necessarily lead to selection bias. We have been informed by the nursery directors and staff that parent participation rate in surveys is usually low and is not necessarily related to refusing to answer the questionnaire on autism, but simply could be due to lack of attention to the forms sent home with the toddlers by the nursery staff/directors.
One of the limitations of the current study was the completeness of data. Some parents missed filling some of the items of the M-CHAT. To remedy that, we checked that at least each item has 80 % completeness and that no specific items were left unanswered. We imputed data by replacing missing items by the most frequent answer (in this case: success in an item) for M-CHAT forms that were not missing more than 5 of the 23 items (20 %). Though 838 respondents (84 %) had answered all 23 items of the M-CHAT, data imputation for the rest of the study participants could have impacted the true prevalence figures. Replacing missing data with the most frequent answer by all respondents to each item which is in this case the successful answer (not failing the item) could have led to decrease the true prevalence of ASD in toddlers. Additionally, the M-CHAT has been validated for toddlers aged 16–30 months, both English and Arabic versions (Robins et al. 2001; Seif Eldin et al. 2008). We extended the upper age limit to 48 months to expand sample size as there are precedents for using the M-CHAT for children above 30 months (Albores-Gallo et al. 2012; Glascoe et al. 2006). Another limitation of this study is that we did not conduct the follow-up interview for the M-CHAT to ascertain results. This was not possible due to the fact that this was an anonymous study and we expected parents to be more reluctant to participate if their child(ren) and their identification had to be provided. Although it would have been ideal to conduct a follow-up interview or to have a PPV for the Arabic M-CHAT, to account for this issue, we used the positive predictive value of 0.058 as determined by Robins (2008) for the first stage M-CHAT. Another study conducted by Chlebowski et al. (2013) established a very similar PPV for stage one M-CHAT at 0.06. Although the M-CHAT is considered a good screening tool for ASD (Chlebowski et al. 2013), the cultural differences in its item responses render it tough for international comparison of results (Albores-Gallo et al. 2012). Moreover, although the Arabic M-CHAT has been validated, there is still room to improve the tool and its validation in Arab countries. The validation study was a pilot study that was not comprehensive of all Arab countries and most children that were at risk of ASD according to the M-CHAT were initially a high risk group (Seif Eldin et al. 2008).
Finally, the representativeness of the sample and the generalization to the whole Lebanese toddler population might be affected by the fact that 12 % of Lebanese children 0–4 years are attending registered nurseries Beirut and Mount Lebanon (MOPH 2014; CAS 2009). The socio-demographic characteristics of parents of children who answered the questionnaires might differ from those in the general population. In the sample, 83 and 64 % of mothers and fathers respectively have at least a university degree as compared to 23 and 17 % of Lebanese residents aged 30–34 years and 35–38 years, respectively (CAS 2009). This might be due to two things: parents with higher education being more prone to responding and/or parents with higher education tending to put their children more in nurseries versus parents with lower education. This could be explained by the fact that holders of university degrees are more likely to be in the workforce, thus needing to put their children in nurseries while they are at work. On another note, 11 % of mothers and 39 % of fathers in the study are self-employed. Given that the big majority of respondents hold a university degree, these results are comparable to the general Lebanese population as 21 % of people working with a university education in Lebanon are either employers or self-employed (CAS 2009).
Although the prevalence of ASD in this study is based on only two governorates, and does not reflect a national estimate, the magnitude should be of concern and a follow up on the issue by researchers and policy makers is warranted. It is worth noting that the areas not surveyed in this study, specifically the Bekaa and the North governorates, have high consanguinity rate, and therefore a higher incidence of autism is expected. Because of the stigma associated with autism, Arab parents in many neighboring Arab countries or in the US are not open about their children’s disability and are often hesitant to acknowledge autism symptoms and to seek care (Hijazi 2014). With the recent consensus that there has been an increase in the prevalence in autism globally and regionally, enhancing awareness of parents and more efforts for systematic assessment and early screening programs at the primary care levels conducted by pediatricians or family doctors is called for.
Further investigation is needed to understand the pattern of health services for children with ASD, the burden of care and coping of caregivers including extending observations to a wider geographical area and ascertainment of cases. Awareness should be increased in parents and physicians for early diagnosis and the implications of early intervention in ASD, as it results in better outcomes for children with ASD and stress reduction for parents (Autism Speaks 2012; Koegel et al. 2014).
References
Al-Ansari, A. M., & Ahmed, M. M. (2013). Epidemiology of autistic disorder in Bahrain: Prevalence and obstetric and familial characteristics. Eastern Mediterranean Health Journal, 19(9), 769–774.
Albores-Gallo, L., Roldan-Ceballos, O., Villarreal-Valdes, G., Betanzos-Cruz, B. X., Santos-Sanchez, C., Martinez-Jaime, M. M., et al. (2012). M-CHAT Mexican version validity and reliability and some cultural considerations. International scholarly research network. ISRN Neurology,. doi:10.5402/2012/408694.
Al-Farsi, Y. M., Al-Sharbati, M. M., Al-Farsi, O. A., Al-Shafaee, M. S., Brooks, D. R., & Waly, M. I. (2011). Brief report: Prevalence of autistic spectrum disorders in the sultanate of Oman. Journal of Autism and Developmental Disorders, 41, 821–825. doi:10.1007/s10803-010-1094-8.
Al-Habeeb, A. A., Qureshi, N. A., & Al-Maliki, T. A. (2012). Pattern of child and adolescent psychiatric disorders among patients consulting publicly-funded child psychiatric clinics in Saudi Arabia. Eastern Mediterranean Health Journal, 18, 112–119.
American Psychiatric Association. (2013a). Diagnostic and statistical manual of mental disorders-5 fact sheet. http://www.dsm5.org/Documents/Autism%20Spectrum%20Disorder%20Fact%20Sheet.pdf. Accessed May 8, 2015.
American Psychiatric Association. (2013b). Diagnostic and statistical manual of mental disorders (5th ed.). Arlington, VA: American Psychiatric Association.
Amr, M., Bu Ali, W., Hablas, H., Raddad, D., El-Mehesh, F., El-Gilany, A-H., & Al-Shamy, H. (2012). Sociodemographic factors in Arab children with Autism Spectrum Disorders. Pan African Medical Journal, 13, article 65.
Autism speaks. (2012). How is autism treated? http://www.autismspeaks.org/what-autism/treatment. Accessed September 18, 2012.
Barbu, S., Cabanes, G., & Le Maner-Idrissi, G. (2011). Boys and girls on the playground: Sex differences in social development are not stable across early childhood. PLoS one, 6, 1–7.
Centers for Disease Control and Prevention. (2014a). Prevalence of autism spectrum disorders among children aged 8 years—autism and developmental disabilities monitoring network, 11 sites, United States, 2010. Morbidity and Mortality Weekly Report, Surveillance Summaries, 63(SS02), 1–21.
Centers for Disease Control and Prevention. (2014b). Autism spectrum disorders. Data and statistics, http://www.cdc.gov/ncbddd/autism/data.html. Accessed August 28, 2014.
Central Administration of Statistics. (2009). Population statistics. http://www.cas.gov.lb/index.php/demographic-and-social-en/population-en. Accessed January 22, 2015.
Chlebowski, C., Robins, D. L., Barton, M. L., & Fein, D. (2013). Large scale use of the modified checklist for autism in low risk toddlers. Pediatrics, 131(4), e1121–e1127.
Davidovitch, M., Hemo, B., Manning-Courtney, P., & Fombonne, E. (2013). Prevalence and Incidence of autism spectrum disorder in an Israeli population. Journal of Autism and Developmental Disorders, 43, 785–793.
Eapen, V., Mabrouk, A. A., Zoubeidi, T., & Yunis, F. (2007). Prevalence of pervasive developmental disorders in preschool children in the UAE. Journal of Tropical Pediatrics, 53(3), 202–205. doi:10.1093/tropej/fml091.
Fombonne, E. (1999). The epidemiology of autism: A review. Psychological Medicine, 29, 769–786.
Fombonne, E. (2009). Epidemiology of pervasive developmental disorders. Pediatric Research, 65(6), 591–598.
Frazier, T. W., Georgiades, S., Bishop, S. L., & Hardan, A. Y. (2014). Behavioral and cognitive characteristics of females and males with autism in the simons simplex collection. Journal of the American Academy of Child and Adolescent Psychiatry, 53(3), 329–340.
Glascoe, F.P., Macias, M., & Wegner, L.M. (2006). Can parents’ concerns identify children likely to have autism-spectrum disorder? Presentation to the pediatric academic societies annual meeting, Spring, 2006.
Head, A.M., McGillivray, J.A. & Stokes, M.A. (2014). Gender differences in emotionality and sociability in children with autism spectrum disorders. Molecular Autism, 5, article19, 1–9.
Hijazi, S. (2014). Arab parents often hesitant in acknowledging children with autism. The Arab American News, February 20, 2014.
Kielinen, M., Linna, S. L., & Moilanen, I. (2000). Autism in Northern Finland. European Child and Adolescent Psychiatry, 9, 162–167.
Kim, Y. S., Leventhal, B. L., Koh, Y. J., Fombonne, E., Laska, E., Lim, E. C., et al. (2011). Prevalence of autism spectrum disorders in a total population sample. American Journal of Psychiatry,. doi:10.1176/appi.ajp.2011.10101532.
Kocovska, E., Biskupstø, R., Gillberg, I. C., Ellefsen, A., Kampmann, H., Stora, T., et al. (2012). The rising prevalence of autism: A prospective longitudinal study in the Faroe Islands. Journal of Autism and Developmental Disorders, 42, 1959–1966.
Koegel, L. K., Koegel, R. L., Ashbaugh, K., & Bradshaw, J. (2014). The importance of early identification and intervention for children with or at risk for autism spectrum disorders. International Journal of Speech-Language Pathology, 16(1), 50–56.
Ministry of Public Health. (2014). Nurseries. List of certified nurseries by the ministry of public health. http://www.moph.gov.lb/MedicalCare/HealthFacilities/Pages/Nurseries.aspx. Accessed January 22, 2015.
Moldin, S. O., & Rubenstein, J. L. R. (2006). Understanding autism: From basic neuroscience to treatment. Florida: CRC Press, Taylor and Francis Group.
National Institute of Mental Health. (2012). Autism: More affected or more detected. http://www.nimh.nih.gov/about/director/2012/autism-prevalence-more-affected-or-more-detected.shtml. Accessed August 28, 2014.
Nordahl, C.W., Iosif, A., Young, G.S, Perry, L.M., Dougherty, R., Lee, A. et al. (2015). Sex differences in the corpus callosum in preschool-aged children with autism spectrum disorder. Molecular Autism, 6, article 26, 1–11.
Robins, D. L. (2008). Screening for autism spectrum disorders in primary care settings. Autism, 12, 537–556. doi:10.1177/1362361308094502.
Robins, D.L. (2013). Official M-CHAT website. http://www.mchatscreen.com/Official_M-CHAT_Website.html. Accessed September 4, 2014.
Robins, D. L., & Dumont-Mathieu, T. M. (2006). Early screening for autism spectrum disorders: Update on the modified checklist for autism in toddlers and other measures. Journal of Developmental and Behavioral Pediatrics, 27(2), S111–S119.
Robins, D. L., Fein, D., Barton, M. L., & Green, J. A. (2001). The modified checklist for autism in toddlers: An initial study investigating the early detection of autism and pervasive developmental disorders. Journal of Autism and Developmental Disorders, 31(2), 131–144.
Saudi Gazette Report. (2014). A Saudi’s saga of suffering and confronting challenges. Saudi Gazette, September 20, 2014.
Seif Eldin, A., Habib, D., Noufal, A., Farrag, S., Bazaid, K., et al. (2008). Use of M-CHAT for a multinational screening of young children with autism in the Arab countries. International Review of Psychiatry, 20, 281–289.
Sevilla, F. M. S., Bermúdez, M. O. E., & Sánchez, J. J. C. (2013). Estimación de la prevalencia de los trastornos del espectro autista en Canarias. An Pediatr (Barc), 79(6), 352–359.
Skuse, D., & Mandy, W. (2015). The female autism conundrum. Webinar, March 11, 2015. Simons foundation autism research initiative. http://sfari.org/sfari-community/community-blog/webinar-series/2015/webinar-the-female-autism-conundrum?utm_source=Autism+research+news+from+SFARI.org&utm_campaign=1a863ae881-SFARI_WebinarSkuseMandy20150305&utm_medium=email&utm_term=0_0a60ccb345-1a863ae881-388776921#. Accessed March 13, 2015.
Acknowledgments
Supporting Grants are Program Projects in Biomedical Research (2013–2014) (amount: $80,000) and OpenMinds (private foundation/NGO) (amount: $125,360).
Author Contributions
MC contributed to conception and design, interpretation of data and write up; DS contributed to conception, design, data acquisition, analysis and interpretation of data and write up; FM contributed to interpretation of the data and critical revision of the manuscript; RB contributed to conception and design, interpretation of data, and critical revision of the manuscript. All authors read and approved the final manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Chaaya, M., Saab, D., Maalouf, F.T. et al. Prevalence of Autism Spectrum Disorder in Nurseries in Lebanon: A Cross Sectional Study. J Autism Dev Disord 46, 514–522 (2016). https://doi.org/10.1007/s10803-015-2590-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-015-2590-7