
Abstract
We have followed up a 2002 population study of autism prevalence in 15–24-year olds in the Faroe Islands. The rate of ASD grew significantly from 0.56% in 2002 to 0.94% in 2009. Although these results are within the range of typical findings from other studies, there were some interesting details. There were—in addition to 43 originally diagnosed cases in 2002—24 newly discovered cases in 2009 and nearly half of them were females. It is possible that unfamiliarity with the clinical presentation of autism in females have played a significant role in this context. There was diagnostic stability for the overall category of ASD over time in the group diagnosed in childhood (7—16) years, but considerable variability as regards diagnostic sub-groupings.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Autism is much more common than previously believed (Gillberg and Wing 1999; Baron-Cohen et al. 2009). It is clear that the increase in reported prevalence is—to some extent—due to change in diagnostic criteria, and heightened awareness (Fernell and Gillberg 2010), but there is remaining uncertainty as to whether autism “in itself” is on the increase. There is a growing concern that girls with autism might be missed if screening is performed at young ages (Kopp et al. 2010).
Several years ago we performed a population study of autism spectrum disorder (ASD) in the Faroe Islands (Ellefsen et al. 2007). All children 7–16 years of age were screened for autism in the general population, in all schools and all relevant registers. Screen positive cases were examined in depth, including collateral interviews with the parents using the Diagnostic Interview for Social and COmmunication disorders (DISCO-10) (Wing et al. 2002). We found a prevalence of 0.56% of the whole age cohort meeting the ICD-10 clinical (and research) diagnostic criteria for childhood autism, atypical autism, or Asperger’s syndrome (according to Gillberg and Gillberg 1989, criteria). The same cohort has now been re-screened and re-examined in depth by a clinical researcher not involved in the original diagnostic study, with a view to establishing whether (a) cases might have been missed in the original study, and (b) prevalence rates might have changed significantly over the follow-up period of 7 years. Particularly, we wanted to test the hypothesis that (c) girls might have been missed in the previous screening, and that therefore (d) the prevalence rate of autism in females might have gone up drastically over the 7-year period.
Methods
The whole Faroese population comprised 47,962 individuals on December 31, 2009. Of these, 7,122 belonged to the (then 7–16-year-old) cohort of 7,689 individuals who had been screened by December 31, 2002. In addition to these, 6 individuals had migrated to the Faroe Islands from other countries in the period of 2003–2009. The target group for the new study consisted of those 7,122 from the original cohort plus the 6 “new” individuals.
The Faroe Islands population, in spite of being spread out over 18 different islands (several of which are now connected through tunnels), is a closely-knit community, and it is difficult to remain completely anonymous. Doctors, teachers and psychologists are a small group of professionals who, together, are in contact with virtually every single person in the 7–24-year-old age range resident on one of the islands. Reaching the vast majority of all individuals in this age group when screening for problems is therefore usually relatively easier than in most other population settings.
Target Screen Population
The screening population consisted of the 7,128 individuals (3,590 males, 3,538 females) aged 15–24 years on December 31, 2009. This should be contrasted with the screening population of 7,689 (3,895 males, 3,794 females) residing in the Faroe Islands on December 31, 2002, when the original screening had been performed. In this study, we have not been able to specifically document the reason for the drop in the number of males (8%) or females (7%) in the age-specific population, even though it is likely that quite a proportion of the reduction in numbers is accounted for by temporary migration for educational purposes. As it turned out, none of those in the out-migration group had been detected as having ASD at the time of the population study in 2002.
Screening Methods
In the original study performed in 2002, all children aged 7–16 years were screened after a process of systematically organised education (through TV and public lectures) and face-to-face contact with headmasters and teachers of all schools in the Faroe Islands (see Ellefsen et al. 2007 for details). The screening included the use of the Autism Spectrum Screening Questionnaire (ASSQ) (Ehlers and Gillberg 1993), which has been shown to be highly reliable and valid for screening autism across the range of intellectual functioning (Posserud et al. 2006, 2009). The screen positive children were examined in detail with a number of instruments including the DISCO-10 and the Wechsler Intelligence Scale for Children—Third edition (WISC) (1992) / Wechsler Adult Intelligence Scale—Revised (WAIS) (1981).
Recruitment Procedure at Study in 2009
Members of the research group appeared on TV, radio, and in the newspapers, sharing information about ASD during the period from 2003 through 2009. They also gave a series of widely attended public lectures about ASD during the same period. At the follow-up study, which was performed during the whole year of 2009, all previous participants were invited to take part. Hospital doctors, GPs, teachers and psychologists were encouraged to refer any cases, diagnosed with ASD or undiagnosed but raising some suspicion of suffering from ASD, to members of the team (RB in all cases, CG and RB jointly in many, see below).
Diagnostic Measures
The DISCO-11 (including all the measures of the DISCO-10 plus a number of additional items) was used. The DISCO-11 is a 2–4 h semi-structured interview about autism spectrum disorders and other developmental disorders affecting social interaction and communication. Its algorithm enables one to investigate whether the necessary criteria of different diagnostic system, such as ICD-10 (WHO 1993) and DSM-IV (APA 1994) are met. This interview was performed by the second author (RB), usually with the mother of the index person, or, much more rarely, with a father or sibling of the person suspected of suffering from ASD. The Autism Diagnostic Observation Schedule (ADOS) (Lord et al. 2000) was also used.
Neuropsychological Testing
In order to establish the cognitive level the Wechsler Adult Intelligence Scale Revised (WAIS) (1981) and—in a few (the youngest)—cases, the Wechsler Intelligence Scale for Children Third edition (WISC) (1992) were used.
Medical Examinations and Medical Record Data
Parents, or in a few cases siblings, were interviewed regarding their child’s pre-, and perinatal periods and early development in accordance with a structured pro-forma used in the PARIS project (Philippe et al. 1999). The individuals themselves were examined in accordance with the pro-forma. All psychiatric and medical records of ASD suspected cases were retrieved and any relevant risk factors, diseases, and disorders were noted down.
Final Diagnostic Assessment
All the clinical data (including the data from the DISCO-11 and the ADOS) was reviewed by the second author and clinical research comprehensive (CRC) diagnoses of childhood autism/autistic disorder, atypical autism/pervasive developmental disorder not otherwise specified (PDDNOS) and Asperger’s disorder were assigned. The same categories and diagnostic criteria that had been used in the original diagnostic study were applied, i.e., the ICD-10 and DSM-IV criteria for childhood autism/autistic disorder (APA 1994), ICD-10/DSM-IV-similar Billstedt et al. (2005) criteria for atypical autism, i.e., 5 or more childhood autism/autistic disorder symptom criteria met, at least two of which from the social interaction domain, and not meeting criteria for childhood autism/autistic disorder or Asperger’s disorder (Billstedt et al. 2005) and Gillberg (1991) criteria for Asperger’s syndrome. In case of any clinical doubt, individuals were seen also by the senior author (CG) (n = 12), and final diagnosis was then assigned by him. DISCO-11 diagnoses were separately assigned in accordance with the computer algorithm of this instrument. This included a new “proposed DSM-V diagnosis for ASD” (see http://www.dsm5.org) according to an algorithm suggested by Hallerbäck et al. (2011).
Statistical Methods Used
Poissson-distributed 95% confidence intervals (ci) were calculated for population absolute rates and overall prevalence rates. Chi-square-tests were applied when comparing group frequencies. Means were compared using Fischer’s permutation test.
Ethics
The study was approved by the Faroe Islands Board for Ethics in Medicine. All families provided informed consent (parents or, in the case of individuals 18 years or over, by the individuals with suspected autism spectrum problems themselves).
Results
Overall Number of Suspected and Definitive Cases Identified
In the original time 1 diagnostic study performed in 2002, 43 individuals with clear ASD diagnoses had been identified (two of whom had not been assessed by the research team). In the new study, all of these 43 minus the two who had not wanted to be part of the in-depth study at time 1 were again contacted and confirmed by telephone interview (one exception see below) to have diagnoses within the autism spectrum. They were all invited to take part in the in-depth clinical research follow-up study—10 declined participation and 31 underwent the in-depth clinical examination. There was one interesting exception—one male (22 years old) with a clear diagnosis of Asperger’s syndrome at time 1, who did not meet criteria for a clinical ASD diagnosis at time 2 even though he still demonstrated some ‘autistic traits’.
A further 30 individuals from the same age cohort were seen in the 2009 study given that some suspicion had arisen that they might be suffering from a previously undiagnosed ASD. Of these, 22 (13 males and 9 females) actually did meet the criteria for ASD: 2 cases of childhood autism (1 male, 1 female), 6 cases of atypical autism (4 males, 2 females), and 14 cases of Asperger’s syndrome (8 males, 6 females). In addition, two further females with Asperger’s syndrome, who had already received a clinical diagnosis of ASD elsewhere, were referred to the research team, leading to a total number of newly diagnosed ASD cases of 24, 16 of whom (8 males, 8 females) had Asperger’s syndrome (Table 1).
This means that at the follow-up study in 2009 there were altogether 55 examined/re-examined cases with a CRC diagnosis of ASD (plus the 12 non-participants in 2009 who had an ASD-diagnosis in 2002—of whom one no longer meet the criteria for an ASD-diagnosis). Out of these, 52 individuals participated in the in-depth study: 31 cases diagnosed in the original study in 2001 and 21 newly discovered and diagnosed only in the follow-up study in 2009. Three additional cases (1 male, 2 females) did not take part in the in-depth study but had been referred to the research team from the Faroe Islands main hospital, and diagnosed by other clinicians. When combined, altogether 43 cases from 2002 (36 males, 7 females), including those 12 who received their diagnosis in 2002 and declined participation in the follow-up study, and 24 newly diagnosed cases in 2009 (13 males, 11 females), the total number of cases of “ever” ASD was 67 (and the number of “current” ASD was 66). Among all 67 cases (49 males, 18 females) there were 15 cases with childhood autism (10 males and 5 females), 15 cases with atypical autism (13 males, 2 females), and 37 cases with Asperger’s disorder (26 males, 11 females). These diagnoses and the DISCO-11 diagnoses are outlined in Table 2 and Appendix 1.
Comparison of the ASD Cohorts in 2002
The newly discovered cases of ASD in the age cohort examined differed from the originally diagnosed cases in the following ways (Table 1).
The newly discovered cases, were, of course, significantly older at the time of receiving a diagnosis of ASD (mean age at diagnosis 18.2, SD 3.5 vs. 11.2, SD 3.6, p < 0.001). There were relatively more females among the “new” cases (16.3% of the original cohort versus 45.8% in the newly diagnosed, p < 0.001), as well as more cases of atypical autism (0% versus 22%, p < 0.001).
Prevalence of ASDs
The total prevalence of ASDs in 15–24-year-olds in the Faroe Islands on December 31, 2009 was estimated at 0.94% (ci: 0.73%, 1.19%) of the whole age specific population (1.37% males, 0.51% females). The relative contribution to this proportion of autistic disorder was 24%, Asperger’s disorder 54%, and atypical autism 22%. Among the males, the corresponding rates were 22.5, 51, and 26.5%, and among the females 27.8, 61.1, and 11.1%, respectively.
Gender Effects
In the 2002 study, 36 of the total number of 43 with ASD were male and 7 female. Among the new 24 cases identified in the 2009 study, there were 13 male and 11 female cases. The newly diagnosed males constituted 27% of the whole 2009 group of males with ASD, whereas the newly diagnosed females constituted 61% of the total female group (p < 0.05, Chi-square test with Yates’s correction).
CRC Diagnoses versus DISCO-11 Diagnoses in Diagnostic and Follow-up Studies
There was good correspondence between CRC and DISCO diagnoses both in the diagnostic and in the follow-up study (Appendix 1). In the original study, DISCO-10 was used. The minor changes from DISCO-10 to DISCO-11 did not affect the diagnostic algorithms used in the present study. The figures are therefore presented as “DISCO-11” findings.
DSM-IV and DSM-V Diagnoses Compared
There was an excellent correspondence between DSM-IV and DSM-V diagnoses as regards the collapsed group of DSM-IV autistic disorder, atypical autism and Gillberg’s Asperger’s disorder cohort on one hand, and the ASD category of the DSM-V on the other. All cases with DSM-IV autistic disorder, atypical autism and Gillberg’s Asperger’s disorder qualified for a DSM-V ASD diagnosis.
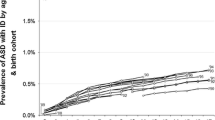
Year of Birth
There was a non-significant trend towards higher prevalence rates of ASD among participants born in the second half of the 10–year period between 1985 and 1994.
Discussion
The prevalence of ASDs (0.94% of the general population) in the Faroe Islands is within the range of “typical” findings in Europe and the rest of the western world (Fombonne 2008).
We found a significant number of “missed” cases in the follow-up study, individuals with unequivocal ASDs who had not been identified as having autistic disorder, Asperger’s disorder, or atypical autism when they were younger. Superficially, the findings, if treated as the results of two separate cross-sectional studies performed with a time gap of seven years, could have been interpreted as support for the notion that the prevalence of ASDs has gone up with time. This would be supported particularly in view of the generally held notion that it is easier to recognise autism in young (school age) children—and therefore more likely that the prevalence would be higher—than in young adults, producing a lower rather than a higher estimate at the older age. However, this was a longitudinal study following (almost exactly) the same cohort of individuals over time. This means that the “rising prevalence” was an artefact of insufficient coverage and diagnostic precision at the time of the original study. The group of ASD cases missed in the original screening had all shown autism symptoms in childhood, but these had not been recognized by the teachers as abnormal. If parents had also been included as informants in that screening, it is possible that many of the missed cases would have been detected. A number of studies have shown that there are large differences across informants (Posserud et al. 2006; Ronald et al. 2008), suggesting the need to gather information both from families and from schools when screening for ASD. There was virtually no migration to the Faroe Islands over the time period covered, in fact there were indications of some migration from the islands in the studied age cohort, and so the prevalence increase could not have been produced by influx of new cases. Conversely, the rather limited migration from the Faroe Islands in the original target population and none in the autism sample, meaning that the “base rate” contributed by cases identified in the first study remained stable over time. Instead, our findings indicate that insufficient knowledge about the phenotype of ASDs, particularly about the clinical presentation in females, is the main reason for the apparent rise in autism prevalence in the Faroe Islands between 2001 and 2009.
Females with autism are very often diagnosed as having other disorders, and the autism aspect of their impairment may be missed altogether (Kopp et al. 2010). The trend (statistically significant) in our study was for missed autism cases (i.e., missed at the time of the original diagnostic study) to be relatively much more often female than male. Almost two-thirds of all the females with ASD in the study were only recognised at or after age 15 years, whereas almost three quarters of all males with ASD had been diagnosed before that age. Also, there was a significant trend towards older (previously unrecognised) females with ASD having an “atypical” presentation, even though the majority of them actually met full Gillberg and Gillberg (1989) diagnostic criteria for Asperger’s disorder.
As in previous psychometric research on the DISCO (Wing et al. 2002; Nygren et al. 2009), agreement between interview and clinical diagnosis for the overall category of ASD was very good. Before drawing any conclusions in this respect one has to have born in mind that CRC diagnosis took findings at DISCO-interview into account. Nevertheless, the DISCO algorithm diagnoses were computer-generated, and the clinician making the final CRC diagnosis was not influenced by the specific DISCO ASD subgroup diagnosis. The study findings demonstrated that, even though the overall rate of ASDs was not greatly influenced by CRC or DISCO-11 ASD status, subgroup diagnosis was clearly affected by clinical judgement as compared with DISCO algorithm diagnosis. This is partly stemming from the fact that the DISCO generates at least ten possible diagnostic subgroups (many of which overlap), whereas the number of CRC diagnoses was limited to three. However, even when like was compared with like (clinical autistic disorder with DISCO autistic disorder, Gillberg’s Asperger’s disorder with Gillberg’s Asperger’s disorder, and atypical autism with atypical autism) and the clinical hierarchy method was applied to the DISCO as well as the CRC diagnoses (autistic disorder taking precedence over Asperger’s disorder etc.), very substantial discrepancies were identified. This, clearly, could be taken to support the stance of the DSM-V, in which only one major category of autism (“ASD”) is acknowledged with sub-grouping recommended only on the basis of non-autism measures, such as IQ and adaptive functioning.
Limitations
In spite of the fact that this was a total population study, and screening was achieved in the total group of young people in the Faroe Islands, the target population was, by default, relatively small, and the number of cases identified correspondingly limited. The confidence limits for the reported prevalence were therefore relatively wide, particularly for females who were represented by very small numbers indeed.
Strengths
The total population character of the sample and the very good coverage plus the comprehensive assessment including gold standard instruments (with well documented good–excellent psychometric properties) for the diagnosis of ASD were the major assets, counterbalancing the limitations to some extent. The follow-up over a period of many years from school age into late adolescence and early adult life, using the same instruments at both time points is a unique feature of the study. The use of both DSM-IV, Gillberg, and DSM-V criteria in one and the same study is a first, and clearly an additional strength. The fact that the original cohort was seen at time 1 by two clinicians and at time 2 by one other clinician adds to the validity of the findings obtained.
Conclusions
Autism is as common in the Faroe Islands—a genetic isolate—as in the rest of the western world. There was a diagnostic stability for the overall category of ASD over time in the group diagnosed in childhood (7–16 years), but considerable variability as regards diagnostic sub-grouping. The follow-up study in late adolescence-young adult age (15–24 years) revealed that about 36% of the total cohort of clinically clear ASD cases had been missed in the first screening study performed in childhood. The reasons for this failure to identify the whole autism population at an earlier age remain partly obscure but it is possible that the unfamiliarity with the clinical presentation of autism in females may have played a significant role in this context.
References
American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders (4th ed.). Washington: American Psychiatric Association.
Baron-Cohen, S., Scott, F. J., Allison, C., Williams, J., Bolton, P., Matthews, F. E., et al. (2009). Prevalence of autism-spectrum conditions: UK school-based population study. The British Journal of Psychiatry, 194, 500–509.
Billstedt, E., Gillberg, I. C., & Gillberg, C. (2005). Autism after adolescence: Population-based 13–22-year follow-up study of 120 individuals with autism diagnosed in childhood. Journal of Autism and Developmental Disorders, 35, 351–360.
Ehlers, S., & Gillberg, C. (1993). The epidemiology of Asperger’s syndrome. A total population study. Journal of Child Psychology and Psychiatry, 34, 1327–1350.
Ellefsen, A., Kampmann, H., Billstedt, E., Gillberg, I. C., & Gillberg, C. (2007). Autism in the Faroe Islands. An epidemiological study. Journal of Autism and Developmental Disorders, 37, 437–444.
Fernell, E., & Gillberg, C. (2010). ASD diagnoses in Stockholm preschoolers. Research in Developmental Disabilities, 31, 680–685.
Fombonne, E. (2008). Is autism getting commoner? The British Journal of Psychiatry, 193, 159.
Gillberg, C. (1991). Clinical and neurobiological aspects of Asperger syndrome in six family studies. In: U. Frith (Ed.), Autism and Asperger Syndrome (pp. 122–146). Cambridge: Cambridge University Press.
Gillberg, I. C., & Gillberg, C. (1989). Asperger’s syndrome: Some epidemiological considerations: A research note. Journal of Child Psychology and Psychiatry, 30, 631–638.
Gillberg, C., & Wing, L. (1999). Autism: Not an extremly rare disorder. Acta Psychiatrica Scandinavica, 99, 399–406.
Hallerbäck, M., Billstedt, E, Johansson, M, Gillberg, I. C., & Gillberg, C. (2011). Diagnostic Interview for Social and COmmunication Disorders—DISCO-11: The correspondence between the DISCO diagnosis and DSM-V. Unpublished manuscript.
Kopp, S., Kelly, K., & Gillberg, C. (2010). Girls with social and/or attention deficits: A descriptive study of 100 clinic attenders. Journal of Attention Disorders, 14, 167–181.
Lord, C., Risi, S., Lambrecht, L., Cook, E. H., Leventhal, B. L., & DiLavore, P. C. (2000). The autism diagnostic observation schedule-generic: A standard measure of social and communication deficits associated with the spectrum of autism. Journal of Attention Disorders, 30, 205–223.
Nygren, G., Hagberg, B., Billstedt, E., Skoglund, A., Gillberg, C., & Johansson, M. (2009). The Swedish version of the Diagnostic Interview for Social and COmmunication Disorders (DISCO-10). Psychometric properties. Journal of Autism and Developmental Disorders, 39, 730–741.
Philippe, A., Martinez, M., Guilloud-Bataille, M., Gillberg, C., Råstam, M., Sponheim, E., et al. (1999). Genome-wide scan for autism susceptibility genes. Paris Autism Research International Sibpair Study. Human Molecular Genetics, 8, 805–812.
Posserud, M.-B., Lundervold, A. J., & Gillberg, C. (2006). Autistic features in a total population of 7–9-year-old children assessed by the ASSQ (Autism Spectrum Screening Questionnaire). Journal of Child Psychology and Psychiatry, 47, 167–175.
Posserud, M.-B., Lundervold, A. J., & Gillberg, C. (2009). Validation of the autism spectrum screening questionnaire in a total population sample. Journal of Autism and Developmental Disorders, 39, 126–134.
Ronald, A., Happé, F., & Plomin, R. (2008). A twin study investigating the genetic and environmental aetiologies of parent, teacher and child ratings of autistic-like traits and their overlap. European Child and Adolescent Psychiatry, 17, 473–483.
Wechsler, D. (1981). Wechsler adult intelligence scale-revised. San Antonio: Psychological Corporation.
Wechsler, D. (1992). Wechsler intelligence scale for children (3rd ed.). London: Psychological Corporation.
Wing, L., Leekam, S. R., Libby, S. J., Gould, J., & Larcombe, M. (2002). The diagnostic interview for social and communication disorders: Background, inter-rater reliability and clinical use. Journal of Child Psychology and Psychiatry, 43, 307–325.
World Health Organization. (1993). The ICD-10 classification of mental and behavioural disorders. Diagnsotic criteria for research. Geneva: World Health Organisation.
Author information
Authors and Affiliations
Corresponding author
Appendix
Appendix
See Table 3.
Rights and permissions
About this article
Cite this article
Kočovská, E., Biskupstø, R., Carina Gillberg, I. et al. The Rising Prevalence of Autism: A Prospective Longitudinal Study in the Faroe Islands. J Autism Dev Disord 42, 1959–1966 (2012). https://doi.org/10.1007/s10803-012-1444-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-012-1444-9