
Abstract
The prevalence of autism spectrum disorders has been steadily rising. In most parts of the world, rates as high as 1 % are reported, including in the United States. In Israel, previously reported prevalence rates have been in the 0.2 % range, and were based on parental reporting of diagnosis. In this study, records from one of the largest Israeli Health Maintenance organizations were used to calculate both incidence and prevalence of autism spectrum disorder (ASD) in Israel. Israeli prevalence of ASD was calculated at 0.48 % for 1–12 years olds and 0.65 % for 8 year old children in 2010, higher than previous Israeli reports, but still lower than prevalence estimates for the US. Incidence calculations ranged from 0.65 to 0.84 per 1,000 children for children 1–12 year olds. Reasons for these differences are suggested and discussed.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The dramatic rise over the last several decades in the diagnosis of autism spectrum disorders (ASD) has been documented extensively around the world. Here, we use the term ASD to include autistic disorder, Asperger’s syndrome and cases of pervasive developmental disorder-not otherwise specified (PDD-NOS). A comprehensive review of 61 studies from 18 countries, published between 1966 and 2009 found from recent studies an overall prevalence of 0.7 %, or 1 child in 143 (Fombonne et al. 2011). Significant methodological differences across studies exist, and a 6 fold variation in prevalence proportions was found in studies published since 2000. Males were consistently overrepresented. Numerous factors were identified as potential contributors to the interpretation of increasing prevalence as evidence of increasing incidence, including use of inappropriate referral statistics, and the role of diagnostic substitution. Authors concluded “the recent upward trends in rates of prevalence cannot be directly attributed to an increase in the incidence of the disorder, or to an epidemic of autism.” However, it was also noted that current evidence does not eliminate the possibility that a true increase in the incidence of PDDs has contributed to rising overall prevalence (Fombonne et al. 2011). The most recent prevalence figures have continued to rise, with US and Canadian studies reporting prevalence estimates of approximately 1 % (ADDMNS 2009, 2012; Kogan et al. 2009; Lazoff et al. 2010). A 2011 study from a South Korean community estimated ASD prevalence at a surprising 2.6 % (Kim et al. 2011). Notably, the Korean study results reflected directed assessment of children with possible ASD, versus record review. The most recent global estimate of autism prevalence published in 2012 is 0.62 % (Elsabbagh et al. 2012).
In some cases, incidence rates for ASD have shown a similar trend to prevalence, with several studies documenting an increase in incidence from the late 1980s to the early 2000s (Powell et al. 2000; Smeeth et al. 2004). Another study, which examined autism incidence in China between 1990 and 2003 in children aged 0–4 years, showed a relatively stable annual incidence rate (0.5 per 1,000, Wong and Hui 2008). In the United Kingdom, the incidence rate remained steady through the first decade of 2,000, with annual incidence figures of approximately 1 per 1,000 (Jick et al. 2006).
In Israel, three epidemiological studies on ASD have been published. The first collected data from diagnostic and treatment facilities in a single city district and reported an incidence of 0.1 % for the years 1989–1993 amongst children aged 0–5 years (Davidovitch et al. 2001). The second study examined cases of ASD that were reported to the National Insurance Institute of Israel in 2004, and found a very low annual incidence of 0.019 % (Senecky et al. 2009). However, this low incidence rate was suggested to be the result of using an unsuitably large denominator (Gal and Gross 2009). The third study (Gal et al. 2012) analyzed data from the Israeli Ministry of Social Affairs for children born between 1986 and 2005, and reported a prevalence of 0.12 % for children born in 1986, which had increased to 0.36 % for children born in 2003. This result is significantly lower than reported global prevalence figures. It is important to note that the latter two studies based their work on data from government bodies. In these cases, parents reported the ASD diagnosis (made by an expert in child neurology and development or a child psychiatrist) in order to receive government support, such as medical treatments and other benefits.
Several studies have attempted to explain increases in ASD prevalence and incidence. Changes in diagnostic approach, such as the shift from the general diagnosis of developmental delays or language delays to autism (Jick and Kaye 2003; Bishop et al. 2008), have been implicated in the increase. In addition, diagnostic substitution from mental retardation to autism has been suggested to account for as much as 25 % of the increase (King and Bearman 2009). Other possible explanations for the increases include greater ASD awareness (Posserud et al. 2010), earlier age of diagnosis, changes in diagnostic criteria (Fombonne et al. 2011) and methodological differences (Wazana et al. 2007). Despite a general recognition that broader diagnostic criteria have influenced changes in prevalence, changes in diagnostic criteria and younger age at diagnosis were felt to explain only a fraction of the dramatic rise in autism diagnoses in California (Hertz-Picciotto and Delwiche 2009). Environmental factors, such as certain pesticides, were also suggested as possible explanation for the rising prevalence of autism (Shelton et al. 2012).
The objective of the present study was to calculate the prevalence and incidence of ASD over 7 years in the Israeli population. Previously reported prevalence figures in Israel have been unusually low as compared to global figures, and there have been no recent reported incidence figures in Israel. To obtain the most precise data, we examined physician records of ASD, rather than government reports or educational sources.
Methods
Case Identification
Israel has a socialized healthcare system in which all citizens are free to choose between four health maintenance organizations (HMOs). Patient fees are equivalent across all four HMOs, and all HMOs provide equivalent medical services that are based on national health regulations. For this review, we examined data on ASD diagnosis from the computer database of the second-largest HMO, Maccabi Healthcare Services, which provides services to 1.8 million people [The distribution in 2009 between the 4 HMO–Clalit 52.4 %, Maccabi 24.8 %, Meuhedet 13.6 %, and Leumit 9.2 %. The percentage of children up to 15 years old from the general population is 28.7 (Clalit 26.2 %, Maccabi 31.1 %, Meuhedet 35 %, Leumit 30.7 %)] (Israeli Central Bureau of Statistics 2010).
In Maccabi Healthcare Services, for children up to the age of 6 years, referrals for an ASD evaluation are usually initiated by parents, preschool teachers, nurses in Baby Health Centers, or the primary pediatrician. The primary pediatrician does not make the ASD diagnosis; rather, he refers the child to Maccabi’s Child Development Center (or a similar hospital-based center) for a thorough evaluation. There the child undergoes a multidisciplinary assessment, including assessments by an expert in pediatric neurology and development and a child psychologist, and in the majority of cases, and additional assessment by a speech language pathologist. The final diagnosis reflects the impression of the team and follows the criteria for ASD set forth in the DSM-IV (American Psychiatric Association 1994). An ASD diagnosis made at the Center is recorded directly into Maccabi’s computer registry by the specialist in pediatric neurology and development; this method of diagnosis represents the majority of ASD diagnoses in children younger than 6 years.
For children aged 6 and above, an ASD diagnosis is made outside of the Maccabi Child Development Center, usually by a Maccabi pediatric neurologist or child psychiatrist, who records the diagnosis on the individual’s electronic file on Maccabi’s computer registry. On rare occasions, a child psychologist within Maccabi will make and record the diagnosis. These methods of diagnosis represent the majority of ASD diagnoses in children aged 6 and above.
In the remainder of cases, the children’s primary pediatrician records the ASD diagnosis on the Maccabi computer registry, though the primary pediatrician never makes the actual diagnosis. In some instances, for example, children can be referred to a hospital-based clinic instead of a Maccabi Child Development Center. Parents then present the results of the hospital-based clinic’s evaluation to the child’s primary pediatrician, who records the diagnosis in the Maccabi computer registry. In other instances, parents may have their child evaluated privately by a pediatric neurologist or psychiatrist. Parents then present the results of the private evaluation to the child’s primary pediatrician, who records the diagnosis in the Maccabi computer registry. Finally, if a child switches from another HMO to Maccabi, the Maccabi primary pediatrician reviews existing medical records and takes an oral patient history; the pediatrician then records any prior ASD diagnosis into the Maccabi computer registry.
Case Ascertainment Procedures
When searching the Maccabi records for cases of ASD diagnoses, the first author checked each patient record to eliminate cases of technical errors (e.g., in some cases, the referral for ASD evaluation was erroneously recorded as an ASD diagnosis) and ensured that only those children with definitive ASD diagnoses were included in the study.
Case Definition
For both incidence and prevalence figures, a case of ASD was defined as any child in the target age group with a physician–recorded diagnosis. ASD criteria, based on the DSM-IV, included those diagnosed with autistic disorder, Asperger’s syndrome, and PDD-NOS. As in most other prevalence and incidence studies, children with the diagnosis of Rett syndrome and childhood disintegrative disorder were excluded from the survey.
Data Analysis
We calculated autism prevalence in two ways. In the first prevalence figure, we determined for the 2010 calendar year the total number of children aged 1–12 years of age who had ever received an autism diagnosis (period prevalence). We divided that figure by the total number of children in that age group who were registered with Maccabi in 2010. Children diagnosed under 1 year of age were excluded due to the negligible impact of this low number. For the second ASD prevalence figure, we measured the 2010 autism prevalence among 8-year-old children in order to obtain comparable data to the United States Developmental Disabilities Monitoring Network (ADDMNS 2009, 2012). We calculated the total number of 8-year-old children in 2010 (born from 1/1/2002 to12/31/2002) that had ever received an ASD diagnosis and divided by the total number of 8-year-old children registered in Maccabi during the same year.
Next, we calculated annual autism incidence as the total number of new cases of ASD diagnosis in children 1–12 years of age (in each year from 2004 to 2010) divided by the total membership in that age group in the same year. Only the records of all of the children enrolled in Maccabi from birth (with and without autism) were included in this calculation to ensure that first time diagnoses were accurately captured, and thus mitigate the effect of patients changing HMOs. For the same reason as indicated above, children who were diagnosed with autism in the first 12 months of their life were not included in this calculation. In addition, the cumulative annual incidence for children born from 2002 to 2006 was calculated up to 2010.
Data on Correlates
We explored if ASD prevalence varied by socioeconomic status (SES) or demographic group. Two separate measures of socioeconomic status were utilized. The first was based on a scale that divides geographic locations into different socioeconomic categories on a scale ranging from 1–10, where one is the lowest SES and ten is the highest (Israeli Central Bureau of Statistics, 2006). We assigned each individual a number based on his reported residence, and for the purposes of our analysis, we divided the figures into low SES (1–4 level), average SES (5–6), high average SES (7–8) and high SES (9–10) groups. The second, separate SES analysis was conducted by examining the differences in prevalence figures between those children who have supplemental insurance coverage (86.9 %) and those who do not (13.1 %). The price of the supplemental insurance coverage varies, but for a family of four, the cost is approximately $40 per month. This supplement provides benefits in addition to the medical services that are mandated by national health regulations. For example, if a parent purchased supplementary insurance, among other benefits, the child would receive additional sessions (at a discounted rate) with occupational therapists, speech and hearing pathologists, as well as optional extras like art therapy and hippotherapy. For the purposes of this paper, we assumed that more affluent citizens elect to purchase supplemental insurance, whereas less affluent citizens retain the basic coverage. As neither measure is highly specific for SES, both were used.
In order to characterize the prevalence of ASD by ethnic group, we examined individuals who resided in towns and villages that are populated exclusively by a specific demographic group (e.g., Umm el-Fahm is populated solely by Israeli Arabs, and Modi’in Illit is populated solely by ultra-orthodox Jews).
Statistical Analysis
We calculated cumulative incidence rate per 1,000 for birth cohorts born in years 2002–2006, with follow-up through 2010. We used the Cochran Armitage trend test to compare cumulative incidence between birth cohorts at each year of age during follow-up. We tested differences in ASD prevalence between demographic groups by Chi square for categorical variables. For all analysis P < 0.05 was considered statistically significant. All analysis was carried out using IBM SPSS Statistics version 19.0 for Windows, using the recommended correction for the Cochran Armitage test (Cochran-Armitage test 2012).
Results
For the first prevalence calculation, during the 2010 calendar year, 423,524 children between the ages of 1–12 years were registered in Maccabi Healthcare Services, and 2,187 had an ASD diagnosis. After searching each record for technical errors, 153 children were eliminated, leaving a total of 2,034 children who had a definitive diagnosis of ASD. Thus the prevalence was 4.8 per 1,000 (0.48 %). The prevalence for boys was 7.8 per 1,000 and for girls 1.6 per 1,000 (Table 1), corresponding to a male:female ratio of 5.2:1. For the second prevalence calculation, in children 8 years of age in 2010, we obtained a figure of 6.5 per 1,000 children (0.65 %, 95 % CI 0.569–0.731; Table 2).
With regard to the two measures of socioeconomic status, we found a significantly lower prevalence of ASD for the low SES group (1–4 level; Table 1) as compared to the other SES groups, and a significantly lower prevalence of ASD for the group without supplemental insurance (Table 1). In addition, prevalence was lower for both Israeli Arabs and ultra-Orthodox Jews as compared to the rest of the population (Table 3).
For the annual incidence calculation, a total of 2,272 children less than 12 years of age were registered in the Maccabi registry and received a diagnosis of ASD during the years 2004–2010. Technical errors were identified in 146 records, leaving a total of 2,126 children with definitive diagnosis of ASD. Three children received their diagnosis before their first birthday and were not included. Of the remaining 2,123 children, 54.2 % received their first diagnosis from a specialist in pediatric neurology and development at Maccabi’s Child Development Centers. Diagnoses made within Maccabi but outside of the Child Development Center accounted for 17 % of total diagnoses (10.7 % from a child psychiatrist, 3.5 % by pediatric neurologist, 2.4 % by clinical psychologist, and 0.4 % by other physician). The remaining 28.8 % of children received their first diagnosis outside of Maccabi; these diagnoses were recorded in the Maccabi computer registry by the child’s primary pediatrician. We found that 62.8 % of the children were first diagnosed with ASD from age 1 up until 4, another 20 % from age 4 up until 8, and the remaining 17.2 % from age 8 up until 12 (Table 4) with a mean age at diagnosis of 5.29 years (SD = 2.86) for the entire sample.
Table 5 details the autism spectrum annual incidence for the years 2004–2010. The average ASD annual incidence for all children aged 1–12 years was 0.76 per 1,000, and ranged from 0.65 per 1,000 (in 2004) and 0.84 per 1,000 (in 2010).
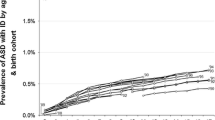
The cumulative incidence for children born in 2002 through 2010 was 5.94 per 1,000. This result is lower than the measured prevalence for 8-year-olds in 2010 (6.5 per 1,000), because only children who were enrolled in Maccabi from birth and received a diagnosis of ASD were utilized for incidence calculation A statistically significant increase in the annual incidence was observed for children born from 2002 through 2005 at the ages 3, 4, 5 and 6 years old (Fig. 1, Table 6), A decrease in annual incidence was noted for those born in 2006.

Cohorts of child’s birth year, cumulative incidence at successive ages
For 5 year olds born in 2002 through 2005, a statistically significant increase in annual cumulative incidence was seen for the general population, but not for the minority populations (Fig. 2).

Trend of cumulative incidence of ASD at 5 years old among Ethnic group
Discussion
We obtained a rate of ASD prevalence for the 2010 calendar year in Israel of 0.48 % for children 1–12 years, which is higher than previously reported Israeli prevalence figures (Gal et al. 2012). However, this figure is markedly lower than recent reported global figures, which generally fall in the range of 1 %. For our second measure, we found ASD prevalence for 8-year-olds in Israeli in the 2010 calendar year to be 0.65 %, which is notably lower than the previously reported CDC rates in the US of 0.9 % (ADDMNS 2009) and 1.1 % (Autism and Developmental Disabilities Monitoring Network Surveillance Year 2008 Principal Investigators 2012) amongst 8-year-olds (the calculated Odd Ratio is 0.55 (95 % CI 0.497–0.645). The results of this study are comparable to global average estimates of 0.62 % (Elsabbagh et al. 2012) and 0.7 % (Fombonne et al. 2011).
With regard to ASD incidence in children aged 1–12, we found an increase in both annual and cumulative incidence for the general population, but not for minority populations. Interestingly, this increase abated in the last birth cohort of children born in 2006. Whether or not this finding indicates a plateauing of the incidence in Israel cannot be tested from the available data but it calls for future monitoring of ASD incidence in more recent birth cohorts.
What factors could explain the discrepancy between Israeli and US prevalence figures? Since there is extensive screening for developmental problems in Israel, as well as widespread awareness of ASD and services, it is unlikely that this discrepancy is due to differences in these factors. It is also unlikely that the differences are due to lack of facilities, as there is a well-established system for monitoring and supporting children through Child Development Centers, which are separate from the primary pediatrician settings. Furthermore, it is unlikely that the discrepancy is due to lack of health benefits provided for children with ASD, as Israel provides a generous amount of therapy and special education services, starting at the age of 1 year, for those children diagnosed with ASD. These benefits are mandated by national health regulations and are similar across HMOs. It is possible that methodological differences in case ascertainment in this study versus CDC studies account for some of the discrepancy. A large number of records from a variety of sources (schools, health care providers) are abstracted in CDC studies. In this study prevalence is determined solely from the medical record.
It is possible that societal influences—such as socioeconomic status (SES) or ethnic group—played a role in the discrepancy, as we found lower prevalence rates in minority groups (Table 3) and in the population with a low SES (Table 1). However, these low prevalence rates are similar to those reported in other studies that include ethnic minorities (Mandell et al. 2009; ADDMNS 2009, 2012) and lower SES groups (Durkin et al. 2010), and it is therefore unlikely that they would be sufficient to explain the lower prevalence in Israel. In Israel specifically, lower rates of autism in certain ethnic groups could be accounted for by differences in autism awareness. In addition, in the experience of the first author, certain cultural groups may associate more stigma about a child receiving a label or diagnosis, as this can impact how the family is perceived within their cultural group.
The Maccabi database does not include an indicator of membership in a minority population, therefore we use place of residence as a proxy for this variable. Many members of ethnic groups live in a more mixed environment, and therefore have access to the same resources for diagnosis and treatment of ASD. Thus, ASD prevalence in these minority groups could be expected to more closely match the general population. However, our current data about ASD prevalence in minority ethnic groups seems to suggest that factors beyond SES influence rates of ASD diagnosis, particularly cultural differences in the ways that disabilities are viewed and understood.
We propose two possible explanations for the lower reported prevalence in Israel as compared to US figures. The first is related to more strict diagnostic practices: for children up until the age of 6, who are evaluated at the Child Development Center, the diagnosis reflects the impression of a varied team, which consists of at least two specialists with different backgrounds (e.g., a child psychologist and a specialist in pediatric neurology and development). Furthermore, these evaluations are not conducted at a single meeting, but rather at several different meetings. For children aged 6 and up, who are not referred to the Child Development Center, new health regulations (established in 2008) require that an ASD diagnosis be made only after two separate evaluations (one from a specialist in pediatric neurology and development, and the other from a clinical psychologist). Another important advantage in the Israeli system is the fact that the physician and psychologists are currently required to write out how each child’s symptoms match the criteria of the DSM-IV. In the US, similar mandates regarding establishing the diagnosis of ASD do not exist, and despite efforts towards a diagnostic standard of care through networks such as the Autism Treatment Network, there is still considerable variability regarding diagnostic practices. While diagnostic variability likely exists in both the US and Israel, it appears that there could be more variability in the US. There also exists the possibility that some children are diagnosed by private providers, and therefore the diagnosis is not recorded in the HMO database.
Second, it is theoretically possible that Israeli children are genetically different from other populations, and are therefore less susceptible to ASD. A recent report of lack of macrocephaly in this population could support this premise (Davidovitch et al. 2011). However, more research is needed to further elucidate the genetic role in predisposition to ASD. Arguing against a genetic explanation, is our finding of increasing incidence in successive birth cohorts which is similar to that found in other countries and inconsistent with a genetic etiology.
While the criteria for ASD diagnosis in Israel follow the DSM-IV, children diagnosed with ASD in Israel do not routinely undergo assessment with the Autism Diagnostic Observation Schedule (ADOS; Lord et al. 2008), which could be viewed as a weakness of this study. However, given recent reports of ADOS sensitivity and specificity in a clinical setting (Molloy et al. 2011), it is possible that not using ADOS for clinical diagnosis has played a role in the apparent lower prevalence. In the estimated 10 years that the ADOS has been used in a more widespread manner for clinical diagnosis in the US, including outside of academic centers and in communities, the increase in ASD diagnosis incidence and prevalence in the US has been dramatic.
In Israel, the incidence of ASDs appears to be rising, although it is possible with more recent statistics that this will level out. Minimally, this observed increase necessitates ongoing monitoring to determine if there is an ongoing true increase in ASD incidence in Israel, despite the above described efforts to standardize and regulate this diagnosis.
This report presents the ASD prevalence and incidence in one Israeli HMO, which covers one quarter of the Israeli population. Although every Israeli citizen can choose his HMO and monthly costs among HMOs are similar, it is possible that our results are not representative of the entire Israeli population. For example the average monthly income in Maccabi Healthcare Services is the highest among the four HMOs, and 31 % higher than in the largest Israeli HMO–Clalit. Since higher income reflects higher SES, and autism prevalence is higher in higher SES groups, it is possible that the national prevalence could be lower. A further limitation of this study relates to the first age of diagnosis: since some ASD evaluations were performed outside of Maccabi and later recorded by the child’s primary physician, it is possible that in some instances, diagnosis was made at an earlier age than reported in our data (Table 4).
This study contributes to the larger and growing body of work on ASD incidence and prevalence. Ongoing study is needed to fully understand global ASD incidence and prevalence, as well as the different variables that influence the observed increases in these figures. We strongly recommend that researchers and institutions adopt more standardized methods of calculating ASD incidence and prevalence; such standardization would lead to better consistency and an enhanced ability to make more precise comparisons across different groups. In addition, there is clear need for more standardization in diagnostic practices for ASD, for without this, efforts to understand prevalence and incidence of ASDs will be thwarted.
References
American Psychiatric Association. (1994). Diagnostic and statisticalmanual of mental disorders (DSM-IV). Washington, DC: American Psychiatric Press.
Autism and Developmental Disabilities Monitoring Network Surveillance Year 2006 Principal Investigators; Centers for Disease Control and Prevention (CDC). (2009). Prevalence of autism spectrum disorders—Autism and Developmental Disabilities Monitoring Network, United States, 2006. Morbidity and Mortality Weekly Report. Surveillance Summaries, 18(10), 1–20.
Autism and Developmental Disabilities Monitoring Network Surveillance Year 2008 Principal Investigators. (2012). Prevalence of autism spectrum disorders–autism and developmental disabilities monitoring network, 14 sites, United States, 2008. Morbidity and Mortality Weekly Report. Surveillance Summaries, 30(3), 1–19.
Bishop, D. V., Whitehouse, A. J., Watt, H. J., & Line, E. A. (2008). Autism and diagnostic substitution: Evidence from a study of adults with a history of developmental language disorder. Developmental Medicine and Child Neurology, 50(5), 341–345.
Davidovitch, M., Golan, D., Vardi, O., Lev, D., & Lerman-Sagie, T. (2011). Israeli children with autism spectrum disorder are not macrocephalic. Journal of Child Neurology, 26(5), 580–585.
Davidovitch, M., Holtzman, G., & Tirosh, E. (2001). Autism in the Haifa area—an epidemiological perspective. The Israel Medical Association Journal, 3(3), 188–189.
Durkin, M. S., Maenner, M. J., Meaney, F. J., Levy, S. E., DiGuiseppi, C., Nicholas, J. S., et al. (2010). Socioeconomic inequality in the prevalence of autism spectrum disorder: Evidence from a U.S. cross-sectional study. PLoS One, 12(5), e11551.
Elsabbagh, M., Divan, G., Koh, Y. J., Kim, Y. S., Kauchali, S., Marcín, C., et al. (2012). Global prevalence of autism and other pervasive developmental disorders. Autism Research, 5(3), 160–179.
Fombonne, E., Quirke, S., & Hagen, A. (2011). Epidemiology of pervasive developmental disorders. In D. G. Amaral, G. Dawson, & D. H. Geschwind (Eds.), Autism spectrum disorders (pp. 90–111). New York: Oxford University Press.
Gal, G., Abiri, L., Reichenberg, A., Gabis, L., & Gross, R. (2012). Time trends in reported autism spectrum disorders in Israel, 1986–2005. Journal of Autism and Developmental Disorder, 42(3), 428–431.
Gal, G., & Gross, R. (2009). Time trends and autism. The Israel Medical Association Journal, 11(9), 577.
Hertz-Picciotto, I., & Delwiche, L. (2009). The rise in autism and the role of age at diagnosis. Epidemiology, 20(1), 84–90.
IBM Reference #1480127. (2012). Cochran-Armitage test for trend for 2xI tables. http://www-01.ibm.com/support/docview.wss?uid=swg21480127. Modified 04.01.2012.
Israeli Central Bureau of Statistics. (2006). http://www.cbs.gov.il/publications/local_authorities2006/excel/p_libud.xls.
Israeli Central Bureau of Statistics–National Insurance Institute. (2010). http://www.cbs.gov.il/q153_heb.htm.
Jick, H., Beach, K. J., & Kaye, J. A. (2006). Incidence of autism over time. Epidemiology, 17(1), 120–121.
Jick, H., & Kaye, J. A. (2003). Epidemiology and possible causes of autism. Pharmacotherapy, 23(12), 1524–1530.
Kim, Y. S., Leventhal, B. L., Koh, Y. J., Fombonne, E., Laska, E., Lim, E. C., et al. (2011). Prevalence of autism spectrum disorders in a total population sample. American Journal of Psychiatry, 168(9), 904–912.
King, M., & Bearman, P. (2009). Diagnostic change and the increased prevalence of autism. International Journal of Epidemiology, 38(5), 1224–1234.
Kogan, M. D., Blumberg, S. J., Schieve, L. A., Boyle, C. A., Perrin, J. M., & Ghandour, R. M. (2009). Prevalence of parent-reported diagnosis of autism spectrum disorder among children in the US, 2007. Pediatrics, 124, 1395–1403.
Lazoff, T., Zhong, L., Piperni, T., & Fombonne, E. (2010). Prevalence of pervasive developmental disorders among children at the English Montreal School Board. Canadian Journal of Psychiatry, 55(11), 715–720.
Lord, C., Rutter, M., Dilavore, P., & Risi, S. (2008). Autism diagnostic observation schedule manual. Los Angeles, CA: Western Psychological Services.
Mandell, D. S., Wiggins, L. D., Carpenter, L. A., Daniels, J., DiGuiseppi, C., Durkin, M. S., et al. (2009). Racial/ethnic disparities in the identification of children with autism spectrum disorders. American Journal of Public Health, 99(3), 493–498.
Molloy, C. A., Murray, D. S., Akers, R., Mitchell, T., & Manning-Courtney, P. (2011). Use of the Autism Diagnostic Observation Schedule (ADOS) in a clinical setting. Autism, 15(2), 143–162.
Posserud, M., Lundervold, A. J., Lie, S. A., & Gillberg, C. (2010). The prevalence of autism spectrum disorders: Impact of diagnostic instrument and non-response bias. Social Psychiatry and Psychiatric Epidemiology, 45(3), 319–327.
Powell, J. E., Edwards, A., Edwards, M., Pandit, B. S., Sungum-Paliwal, S. R., & Whitehouse, W. (2000). Changes in the incidence of childhood autism and other autistic spectrum disorders in preschool children from two areas of the West Midlands, UK. Developmental Medicine and Child Neurology, 42(9), 624–628.
Senecky, Y., Chodick, G., Diamond, G., Lobel, D., Drachman, R., & Inbar, D. (2009). Time trends in reported autistic spectrum disorders in Israel, 1972–2004. The Israel Medical Association Journal, 11(1), 30–33.
Shelton, J. F., Hertz-Picciotto, I., Pessah, I. N. (2012). Tipping the balance of autism risk: Potential mechanisms linking pesticides and autism. Environ Health Perspect. Apr 11.
Smeeth, L., Cook, C., Fombonne, E., Heavey, L., Rodrigues, L. C., Smith, P. G., et al. (2004). MMR vaccination and pervasive developmental disorders: A case-control study. Lancet, 364, 963–969.
Wazana, A., Bresnahan, M., & Kline, J. (2007). The autism epidemic: Fact or artifact? Journal of the American Academy of Child and Adolescent Psychiatry, 46(6), 721–730.
Wong, V. C., & Hui, S. L. (2008). Epidemiological study of autism spectrum disorder in China. Journal of Child Neurology, 23, 67–72.
Acknowledgments
The authors thank Professor Emanuel Tirosh for his thoughtful review and comments and Ms. Anna Wexler for editing the manuscript.
Ethical standards
The study was approved by the Ethics Review Board of Maccabi Healthcare Services.
Conflict of interest
The authors declare that they have no conflict of interest. Authors M.D. and H.B. are employees of Maccabi Healthcare Services.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Davidovitch, M., Hemo, B., Manning-Courtney, P. et al. Prevalence and Incidence of Autism Spectrum Disorder in an Israeli Population. J Autism Dev Disord 43, 785–793 (2013). https://doi.org/10.1007/s10803-012-1611-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-012-1611-z