
Abstract
Obstructive sleep apnea (OSA) is a disease with intermittent hypoxemia during sleep. It has been shown that OSA is related to several cardiovascular diseases including heart failure. Both OSA and heart failure have a close association bidirectionally. This study aimed to estimate the pooled prevalence of OSA in patients with heart failure as well as pooled prevalence of heart failure in patients with OSA. This was a systematic review with a meta-analysis. The inclusion criteria were observational or epidemiological studies conducted in adult patients with heart failure to evaluate the prevalence of OSA and patients with OSA to evaluate the prevalence of heart failure. The outcomes of this study were prevalence of OSA in patients with heart failure and prevalence of heart failure in patients with OSA. Four databases were used for systematic searching including PubMed, Science Direct, Scopus, and CINAHL Plus. Manual searches for related studies were also conducted. Proportion meta-analyses using a random-effects model were conducted to identify pooled proportion (prevalence) of heart failure in patients with OSA and vice versa. Among 3,941 articles from the four databases met the study criteria. Thirty-three studies showed the prevalence of OSA in patients with heart failure, while thirteen studies presented the prevalence of heart failure in patients with OSA. The prevalence of OSA in patients with heart failure was 38.4% (95% CI 31.9 to 45.2; I2 of 96.1%). Using a diagnostic criterion of OSA of more than 10 events/hr had the highest prevalence of OSA in patients with heart failure at 53.4% (95% CI 42.0 to 64.5). The highest prevalence of OSA in patients with heart failure was 60.1% (95% CI 51.4 to 68.3) in a report from India. The pooled prevalence of heart failure in patients with OSA was 12.8% (95% CI 8.1 to 19.5; I2 of 94.6%). The prevalence in Romania was highest at 22.6% (95% CI 20.4 to 24.9). The pooled prevalence of OSA in patients with heart failure was higher than the pooled prevalence of heart failure in patients with OSA. The pooled prevalence rates of these associations varied among the diagnostic criteria of OSA and countries.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Obstructive sleep apnea (OSA) is a common disease with a prevalence of 9–38% in the general population [1]. Its prevalence is slightly more in men than in women (22% vs. 17%), with extremely high figures in some populations such as the elderly (90% in men and 78% in women) [1, 2]. The mechanism of OSA is repeated hypoxemia during sleep, which may lead to several cardiovascular conditions including heart failure [3,4,5,6,7,8,9]. A Mendelian randomization study found that OSA increased the risk of heart failure by 1.13 times (95% CI 1.01 to 1.27) after adjusting for several variables [9]. Additionally, patients with OSA were related with diastolic dysfunction evidence by lower ratio of early to late mitral inflow velocities (E/A) by -0.62 compared with non-OSA patients (p-value = 0.001) [10].
Heart failure is a global health issue, which affects more than 25 million people worldwide, with new admissions of over one million per year in the US [11]. Hospital admissions for heart failure were 6.5 million hospital days annually with an annual cost of over 40 billion USD [11]. A recent study of 111 patients with heart failure found that OSA was highly prevalent at 63.5% [12]. To emphasize the correlation between OSA and heart failure, this study aimed to estimate the prevalence of OSA in patients with heart failure and the prevalence of heart failure in patients with OSA by a systematic review.
Methods
The inclusion criteria were survey or observational studies on the prevalence of OSA in patients with heart failure and the prevalence of heart failure in patients with OSA. We excluded studies with randomized controlled trials, case report/case series, commentaries, books, or reviews. Those studies without a prevalence or incidence of OSA or a diagnosis of OSA other than polysomnography were also excluded. Four databases were used for systematic searching, namely PubMed, Science Direct, Scopus, and CINAHL. In addition, manual searches for related studies were also performed. Search terms included obstructive sleep apnea, prevalence, incidence, epidemiological study, and observational study. The full list of search terms is shown in Appendix. The final search was performed on September 26, 2022.
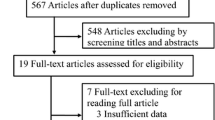
After duplication removal, initial screening was carried out for nonrelevant articles [13,14,15,16]. The initial screening process was performed by two authors (WP, SK) independently. Titles and abstracts were screened and included for any observational studies on OSA and heart failure. The full-text review and data extraction were performed by two independent authors (WP, SK). A PRISMA flow chart of article searching and included studies is shown in Fig. 1.

PRISMA flow for evaluating prevalence of obstructive sleep apnea in patients with heart failure
Data collection of each included study was retrieved for the following section publication characteristics, study characteristics, and outcomes. The publication characteristics comprised the first author, year of publication, and country of study origin, whereas study characteristics included study design, age of patients with heart failure or OSA, diagnosis of heart failure, and diagnosis of OSA. The primary outcome was the prevalence of OSA in patients with heart failure and the prevalence of heart failure in patients with OSA. Study quality of observational studies was evaluated by using the Newcastle–Ottawa Scale; but not the descriptive studies.
Statistical analysis
The I2 statistic and Cochran’s Q test were calculated to assess the heterogeneity of proportions among included studies. Subgroup analyses by diagnostic method, country, and region were used to investigate the heterogeneity between results of included studies. Proportion meta-analyses using a random-effects model were conducted to identify pooled proportion (prevalence) of heart failure in OSA patients and pooled proportion of OSA in heart failure patients. Publication bias was evaluated using Egger’s test. RStudio, R language, and the “meta” package in R were used to perform all data analyses [17,18,19].
Results
Prevalence of OSA in patients with heart failure
There were 3,941 articles eligible for the screening process. Of these, 46 articles entered the full-text review; 13 articles were excluded due to unavailability of polysomnography for OSA diagnosis (10 articles) or no OSA prevalence (3 articles). In total, 33 articles were included for the analysis (Fig. 1). All selected articles had been published between 1997 and 2022; they were mostly from the U.S. (8 articles); and most of them were prospective/cohort studies (18 articles) [20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52]. Diagnosis of OSA was made by evidence of an apnea–hypopnea index (AHI) of 5, 10, or 15 times/hr, while patients with heart failure had a low-left ventricular function of less than 35–55% (Table 1). One study conducted in patients with rheumatic valvular heart disease [25].
The studies contained data from 8,480 patients with heart failure. Of these, 3,079 patients (38.4%) had OSA (95% CI 31.9 to 45.2%), with an I2 of 96.1% (Fig. 2). A subgroup analysis by diagnostic criteria of OSA showed that AHI of more than 10 times/hr had the highest prevalence of OSA at 53.4% (95% CI 42.0 to 64.5%) (Fig. 2). Patients with heart failure in the Asia region had the highest prevalence of OSA with heart failure of 43.4% (95% CI 29.5 to 58.3) when compared with other regions (Fig. 3). Among the countries, India had the highest prevalence of OSA (2 studies, 60.1% with 95% CI 51.4 to 68.3) [36, 51], followed by Hong Kong (1 studies, 55.0% with 95% CI 31.5 to 76.9) [23], as shown in Fig. 4. Regarding study quality, five studies were observational studies; four cohort studies and one case-control study. Three out of four cohort studies had a good quality, while the case-control study had a poor quality (Table 2).

Meta-analysis of the prevalence of obstructive sleep apnea in patients with heart failure by diagnostic criteria

Meta-analysis of the prevalence of obstructive sleep apnea in patients with heart failure by region

Meta-analysis of the prevalence of obstructive sleep apnea in patients with heart failure by country
Prevalence of heart failure in patients with OSA
Among the 3,940 articles for screening, 22 articles met the criteria for full-text review (Fig. 5). Of these, 13 articles were included for the analysis that were published between 2003 and 2021, were mostly prospective/cohort studies (6 articles), and were conducted in the U.S. (4 articles) or China (3 articles) [53,54,55,56,57,58,59,60,61,62,63,64,65]. Diagnostic criteria for OSA varied from AHI of 5–15 times/hr, while most studies did not report the diagnostic criteria for heart failure (Table 3).

PRISMA flow for evaluating prevalence of heart failure in patients with obstructive sleep apnea
The pooled prevalence of heart failure in patients with OSA was 12.8% (95% CI 8.1 to 19.5; I2 of 94.6%) based on 5,250 patients with OSA (Fig. 6). In subgroup analysis by diagnostic criteria for OSA (Fig. 6), the pooled prevalence from five studies was 18.8% (95% CI 14.5 to 24.1) when using an AHI of 5 events/hr or more. Europe had the highest prevalence of heart failure at 15.8% (95% CI 10.5 to 23.1), as shown in Fig. 7. At the country level, the prevalence in Romania was highest at 22.6% (1 studies, 95% CI 20.4 to 24.9), as shown in Fig. 8. There were seven observational studies; five cohort and two cross-sectional studies (Table 4). One out of five cohort studies had a good quality, while both cross-sectional studies had a good quality. Based on Egger’s test, there was no evidence of significant publication bias among included studies that determined the prevalence of OSA in patients with heart failure (p-value = 0.6574) and the prevalence of heart failure in OSA patients (p-value = 0.0646) as shown in Figs. 9 and 10, respectively.

Meta-analysis of the prevalence of heart failure in patients with obstructive sleep apnea by diagnostic criteria of OSA.

Meta-analysis of the prevalence of heart failure in patients with obstructive sleep apnea by region

Meta-analysis of the prevalence of heart failure in patients with obstructive sleep apnea by country

Funnel of the prevalence of obstructive sleep apnea in patients with heart failure

Funnel of the prevalence of heart failure in patients with obstructive sleep apnea
Discussion
OSA is connected to heart failure through several mechanisms, including hemodynamic, neurohormonal, and oxidative/vascular effects [66,67,68]. Apnea induces an increase of intrathoracic pressure leading to a rise in left ventricular transmural pressure and afterload. Oxidative stress from apneic events also increases endothelial dysfunction and sympathetic activation. Cyclical hypoxemia activates endothelial cell inflammation and adhesion. These factors indicate how the underlying mechanism of OSA contributes to heart failure development.
The present review found more patients in the analysis of the prevalence of OSA in patients with heart failure than did the analysis of the prevalence of heart failure in patients with OSA (8,480 vs. 5,250), as shown in Figs. 2 and 6. The prevalence of OSA in patients with heart failure was also higher than the prevalence of heart failure in patients with OSA (38.4% vs. 12.8%), from 33 articles vs. 13 articles, respectively. These data may indicate that OSA may be the most common contributing factor in patients with heart failure. A previous review found that OSA had a prevalence of 53% in patients with heart failure with reduced ejection fraction, and 62% in patients with heart failure with preserved ejection fraction [28, 68]. The prevalence of OSA in patients with heart failure was high as these studies were conducted in those patients who already had consequences of OSA. Similarly, two previous studies found that the prevalence of OSA in patients with stroke or TIA was approximately 70% [69, 70]. On the other hand, the prevalence of heart failure in patients with OSA was low, as these studies enrolled those with and without consequences of OSA. These may result in a low prevalence of heart failure. However, patients with OSA may increase the risk of cardiovascular consequences of OSA if left untreated or undiagnosed.
This study found that prevalence rates of both diseases may be varied among countries. India had the highest prevalence of OSA in patients with heart failure at 60.1%. There are several explanations for these findings. First, the prevalence of moderate to severe OSA in Indian population by the type 1 polysomnography was high at 32.5% [71]. Second, the prevalence of OSA in South Asians was significantly higher than white Europeans who were severe obesity at 85% vs. 66%; p-value = 0.017 [72]. Third, the prevalence of metabolic syndrome in urban Indians was high at 43%; 32.4% were diagnosed as OSA. Fourth, the prevalence of coronary artery disease in Indians was 4.4 to 8.56 times higher than in the US; 11% in non-diabetic Indians and 21.4% in diabetic Indians vs. 2.5% in the US [73]. Additionally, major risk factors of coronary artery disease in Indian population were quite high including hypertension (36.9%), diabetes (21%), high cholesterol (54.1%), and smoking (42%). These data may imply that Indians are very high risk for both OSA and heart failure resulting in the highest prevalence of OSA in patients with heart failure. In another direction, prevalence of heart failure was highest in patients with OSA from Romania at 22.6% (Fig. 8). Other studies reported prevalence of heart failure in patients with OSA from 6.8 to 22.0% (Fig. 3). The different study population may explain varied prevalence rates among countries. The study from Romania enrolled patients with 34.2% of coronary artery disease. Additionally, only 76 patients (6%) had normal weight, while the others were overweight or obese. These two factors may result in high prevalence of heart failure in this study. Another implication is that it may take quite a long period of time to develop heart failure in patients with OSA. Note that not all countries evaluated the associations of OSA and heart failure. Further studies and possible explanations of different prevalence rates of both diseases are needed.
This meta-analysis reported on large sample sizes in both aspects. However, there are some limitations. First, the risk factors of heart failure in patients with OSA were not studied as well as the risk factors of OSA in patients with heart failure. This study did not evaluate the association between these two diseases. Second, no intervention or CPAP therapy was assessed [74,75,76,77]. Third, none of the prospective studies reported an annual incidence. Therefore, pooled incidence rates were not calculated. Finally, diagnostic criteria for OSA or heart failure were different among studies. In particular, only one study showed criteria for heart failure diagnosis in patients with OSA [78].
Conclusions
The pooled prevalence of OSA in patients with heart failure was higher than the pooled prevalence of heart failure in patients with OSA. The pooled prevalence rates of these associations varied among the diagnostic criteria of OSA and the different countries where the studies were undertaken.
Appendix
-
1.
Searching method for PubMed on 26 September 2022
Search
Number
Query
1
sleep apnea, obstructive[MeSH Terms] OR obstructive sleep apnea[Title/Abstract] OR OSA[Title/Abstract]
2
“Prevalence“[Mesh] OR “Incidence“[Mesh] OR “Epidemiology“[Mesh] OR Prevalence[Title/Abstract] OR Incidence[Title/Abstract] OR Epidemiolog*[Title/Abstract]
3
“Observational Study“[Publication Type] OR “Observational Studies as Topic“[Mesh] OR “Epidemiologic Studies“[Mesh]
4
(#1 AND #2) AND #3
-
2.
Searching method for ScienceDirect on 26 September 2022
Title, abstract, keywords: obstructive sleep apnea AND (prevalence OR incidence OR epidemiology), filter: Research articles
-
3.
Searching method for Scopus on 26 September 2022
((TITLE-ABS-KEY (obstructive AND sleep AND apnea) OR TITLE-ABS-KEY (osa))) AND ((TITLE-ABS-KEY (prevalence) OR TITLE-ABS-KEY (incidence) OR TITLE-ABS-KEY (epidemiolog*))) AND ((TITLE-ABS-KEY (observational AND study) OR TITLE-ABS-KEY (case-control AND study) OR TITLE-ABS-KEY (cross-sectional AND study) OR TITLE-ABS-KEY (cohort AND study))) AND (LIMIT-TO ( DOCTYPE, “ar”)) AND (LIMIT-TO (EXACTKEYWORD, “Sleep Apnea, Obstructive”) OR LIMIT-TO ( EXACTKEYWORD, “Prevalence”))
-
4.
Searching method for CINAHL on 26 September 2022
Search
Number
Query
1
TI obstructive sleep apnea OR AB obstructive sleep apnea OR TI osa OR AB osa
Expanders - Apply equivalent subjects
Search modes - Find all my search terms
2
TI ( prevalence or incidence or epidemiology ) OR AB ( prevalence or incidence or epidemiology )
Expanders - Apply equivalent subjects
Search modes - Find all my search terms
3
TI Observational Study OR AB Observational Study OR PT Observational Study
Expanders - Apply equivalent subjects
Search modes - Find all my search terms
4
#1 AND #2 AND #3
Expanders - Apply equivalent subjects
Search modes - Find all my search terms
Data availability
The authors confirm that the data supporting the findings of this study are available within the article and/or its supplementary materials.
References
Senaratna CV, Perret JL, Lodge CJ et al (2017) Prevalence of obstructive sleep apnea in the general population: a systematic review. Sleep Med Rev 34:70–81. https://doi.org/10.1016/j.smrv.2016.07.002
Franklin KA, Lindberg E (2015) Obstructive sleep apnea is a common disorder in the population-a review on the epidemiology of sleep apnea. J Thorac Dis 7:1311–1322. https://doi.org/10.3978/j.issn.2072-1439.2015.06.11
Khamsai S, Mahawarakorn P, Limpawattana P et al (2021) Prevalence and factors correlated with hypertension secondary from obstructive sleep apnea. Multidiscip Respir Med 16:777. https://doi.org/10.4081/mrm.2021.777
Soontornrungsun B, Khamsai S, Sawunyavisuth B et al (2020) Obstructive sleep apnea in patients with diabetes less than 40 years of age. Diabetes Metab Syndr Clin Res Rev 14:1859–1863. https://doi.org/10.1016/j.dsx.2020.09.008
Khamsai S, Chootrakool A, Limpawattana P et al (2021) Hypertensive crisis in patients with obstructive sleep apnea-induced hypertension. BMC Cardiovasc Disord 21:310. https://doi.org/10.1186/s12872-021-02119-x
Sanlung T, Sawanyawisuth K, Silaruks S et al (2020) Clinical characteristics and complications of obstructive sleep apnea in srinagarind hospital. J Med Assoc Thai 103:36–39
Khamsai S, Kachenchart S, Sawunyavisuth B et al (2021) Prevalence and risk factors of obstructive sleep apnea in hypertensive emergency. J Emerg Trauma Shock 14:104–107. https://doi.org/10.4103/JETS.JETS_47_20
Patel M, Yarlagadda H, Upadhyay S et al (2022) Disturbed sleep is not good for the heart: a narrative review. Curr Cardiol Rev. https://doi.org/10.2174/1573403X19666221130100141
Li Y, Miao Y, Zhang Q (2022) Causal associations of obstructive sleep apnea with cardiovascular disease: a mendelian randomization study. Sleep. https://doi.org/10.1093/sleep/zsac298
Al-Sadawi M, Theodoropoulos K, Saeidifard F et al (2022) Sleep apnea as a risk factor for diastolic dysfunction: a systematic review and meta-analysis. Respiration 101:1051–1068. https://doi.org/10.1159/000525782
Ambrosy AP, Gheorghiade M, Chioncel O et al (2014) Global perspectives in hospitalized heart failure: regional and ethnic variation in patient characteristics, management, and outcomes. Curr Heart Fail Rep 11:416–427. https://doi.org/10.1007/s11897-014-0221-9
Bekfani T, Schöbel C, Pietrock C et al (2020) Heart failure and sleep-disordered breathing: susceptibility to reduced muscle strength and preclinical congestion (SICA-HF cohort). ESC Heart Fail 7:2063–2070. https://doi.org/10.1002/ehf2.12798
Sawunyavisuth B, Ngamjarus C, Sawanyawisuth K (2023) Adherence to continuous positive airway pressure therapy in pediatric patients with obstructive sleep apnea: a meta-analysis. Ther Clin Risk Manag 19:143–162. https://doi.org/10.2147/TCRM.S358737
Sawunyavisuth B, Ngamjarus C, Sawanyawisuth K (2022) A meta-analysis to identify factors associated with CPAP machine purchasing in patients with obstructive sleep apnea. Biomed Rep. https://doi.org/10.3892/br.2022.1528
Sawunyavisuth B, Ngamjarus C, Sawanyawisuth K (2021) Any effective intervention to improve CPAP adherence in children with obstructive sleep apnea: a systematic review. Global Pediatr Health. https://doi.org/10.1177/2333794X211019884
Namwaing P, Ngamjarus C, Sakaew W et al (2021) Chest physical therapy and outcomes in primary spontaneous pneumothorax: a systematic review. J Med Assoc Thai 104:S165–S168. https://doi.org/10.35755/jmedassocthai.2021.S04.00059
RStudio T (2022) RStudio: integrated development environment for R. RStudio, PBC, Boston, MA. https://www.rstudio.com/
R Core Team (2022) R: A Language and Environment for Statistical Computing_. R Foundation for Statistical Computing, Vienna, Austria. https://www.r-project.org/
Balduzzi S, Rücker G, Schwarzer G (2019) How to perform a meta-analysis with R: a practical tutorial. Evid Based Ment Health 22:153–160
Alvi RM, Tariq N, Malhotra A et al (2018) Sleep apnea and heart failure with a reduced ejection fraction among persons living with human immunodeficiency virus. Clin Infect Dis 67:447–455. https://doi.org/10.1093/cid/ciy216
Arzt M, Oldenburg O, Graml A et al (2017) Phenotyping of sleep-disordered breathing in patients with chronic heart failure with reduced ejection fraction-the SchlaHF Registry. J Am Heart Assoc 6:e005899. https://doi.org/10.1161/JAHA.116.005899
Bitter T, Faber L, Hering D et al (2009) Sleep-disordered breathing in heart failure with normal left ventricular ejection fraction. Eur J Heart Fail 11:602–608. https://doi.org/10.1093/eurjhf/hfp057
Chan J, Sanderson J, Chan W et al (1997) Prevalence of sleep-disordered breathing in diastolic heart failure. Chest 111:1488–1493. https://doi.org/10.1378/chest.111.6.1488
Damy T, Margarit L, Noroc A et al (2012) Prognostic impact of sleep-disordered breathing and its treatment with nocturnal ventilation for chronic heart failure. Eur J Heart Fail 14:1009–1019. https://doi.org/10.1093/eurjhf/hfs085
Ding N, Ni B-Q, Zhang X-L et al (2013) Prevalence and risk factors of sleep disordered breathing in patients with rheumatic valvular heart disease. J Clin Sleep Med 9:781–787. https://doi.org/10.5664/jcsm.2920
Dolliner P, Brammen L, Graf S et al (2013) Portable recording for detecting sleep disorder breathing in patients under the care of a heart failure clinic. Clin Res Cardiol 102:535–542. https://doi.org/10.1007/s00392-013-0563-4
Donovan LM, Kapur VK (2016) Prevalence and characteristics of central compared to obstructive sleep apnea: analyses from the sleep heart health study cohort. Sleep 39:1353–1359. https://doi.org/10.5665/sleep.5962
Herrscher TE, Akre H, Øverland B et al (2011) High prevalence of sleep apnea in heart failure outpatients: even in patients with preserved systolic function. J Card Fail 17:420–425. https://doi.org/10.1016/j.cardfail.2011.01.013
Holtstrand Hjälm H, Fu M, Hansson P-O et al (2018) Association between left atrial enlargement and obstructive sleep apnea in a general population of 71-year-old men. J Sleep Res 27:252–258. https://doi.org/10.1111/jsr.12585
Huang Y, Wang Y, Huang Y et al (2020) Prognostic value of sleep apnea and nocturnal hypoxemia in patients with decompensated heart failure. Clin Cardiol 43:329–337. https://doi.org/10.1002/clc.23319
Javaheri S, Parker TJ, Liming JD et al (1998) Sleep apnea in 81 ambulatory male patients with stable heart failure. Types and their prevalences, consequences, and presentations. Circulation 97:2154–2159. https://doi.org/10.1161/01.cir.97.21.2154
Javaheri S (2006) Sleep disorders in systolic heart failure: a prospective study of 100 male patients. The final report. Int J Cardiol 106:21–28. https://doi.org/10.1016/j.ijcard.2004.12.068
Javaheri S, Sharma RK, Wang R et al (2016) Association between obstructive sleep apnea and left ventricular structure by age and gender: the multi-ethnic study of atherosclerosis. Sleep 39:523–529. https://doi.org/10.5665/sleep.5518
Ferrier K, Campbell A, Yee B et al (2005) Sleep-disordered breathing occurs frequently in stable outpatients with congestive heart failure. Chest 128:2116–2122. https://doi.org/10.1378/chest.128.4.2116
Khayat RN, Jarjoura D, Patt B et al (2009) In-hospital testing for sleep-disordered breathing in hospitalized patients with decompensated heart failure: report of prevalence and patient characteristics. J Card Fail 15:739–746. https://doi.org/10.1016/j.cardfail.2009.05.005
Kishan S, Rao MS, Ramachandran P et al (2021) Prevalence and patterns of sleep-disordered breathing in Indian heart failure population. Pulm Med 2021:9978906. https://doi.org/10.1155/2021/9978906
Lombardi C, Faini A, La Rovere M et al (2018) Heart failure and sleep related breathing disorders: data from PROMISES (Progetto Multicentrico Italiano Sonno E Scompenso Cardiaco) study. Int J Cardiol 271:140–145. https://doi.org/10.1016/j.ijcard.2018.05.001
MacDonald M, Fang J, Pittman SD et al (2008) The current prevalence of sleep disordered breathing in congestive heart failure patients treated with beta-blockers. J Clin Sleep Med 4:38–42.
Oldenburg O, Lamp B, Faber L et al (2007) Sleep-disordered breathing in patients with symptomatic heart failure: a contemporary study of prevalence in and characteristics of 700 patients. Eur J Heart Fail 9:251–257. https://doi.org/10.1016/j.ejheart.2006.08.003
Oldenburg O, Bitter T, Wiemer M et al (2009) Pulmonary capillary wedge pressure and pulmonary arterial pressure in heart failure patients with sleep-disordered breathing. Sleep Med 10:726–730. https://doi.org/10.1016/j.sleep.2008.08.004
Padeletti M, Green P, Mooney AM et al (2009) Sleep disordered breathing in patients with acutely decompensated heart failure. Sleep Med 10:353–360. https://doi.org/10.1016/j.sleep.2008.03.010
Paulino A, Damy T, Margarit L et al (2009) Prevalence of sleep-disordered breathing in a 316-patient French cohort of stable congestive heart failure. Arch Cardiovasc Dis 102:169–175. https://doi.org/10.1016/j.acvd.2008.12.006
Roebuck T, Solin P, Kaye DM et al (2004) Increased long-term mortality in heart failure due to sleep apnoea is not yet proven. Eur Respir J 23:735–740. https://doi.org/10.1183/09031936.04.00060404
Sin DD, Fitzgerald F, Parker JD et al (2003) Relationship of systolic BP to obstructive sleep apnea in patients with heart failure. Chest 123:1536–1543. https://doi.org/10.1378/chest.123.5.1536
Suda S, Kasai T, Matsumoto H et al (2018) Prevalence and clinical correlates of sleep-disordered breathing in patients hospitalized with acute decompensated heart failure. Can J Cardiol 34:784–790. https://doi.org/10.1016/j.cjca.2018.03.006
Tamisier R, Bocquillon V, Treptow E et al (2019) Prevalence and factors contributing to daytime and nocturnal hypoxemia in chronic heart failure patients. respiration 97:213–222. https://doi.org/10.1159/000490734
Tremel F, Pépin JL, Veale D et al (1999) High prevalence and persistence of sleep apnoea in patients referred for acute left ventricular failure and medically treated over 2 months. Eur Heart J 20:1201–1209. https://doi.org/10.1053/euhj.1999.1546
Vazir A, Hastings PC, Dayer M et al (2007) A high prevalence of sleep disordered breathing in men with mild symptomatic chronic heart failure due to left ventricular systolic dysfunction. Eur J Heart Fail 9:243–250. https://doi.org/10.1016/j.ejheart.2006.08.001
Wang H, Parker JD, Newton GE et al (2007) Influence of obstructive sleep apnea on mortality in patients with heart failure. J Am Coll Cardiol 49:1625–1631. https://doi.org/10.1016/j.jacc.2006.12.046
Yumino D, Wang H, Floras JS et al (2009) Prevalence and physiological predictors of sleep apnea in patients with heart failure and systolic dysfunction. J Card Fail 15:279–285. https://doi.org/10.1016/j.cardfail.2008.11.015
Gupta N, Agrawal S, Goel AD et al (2020) Profile of sleep disordered breathing in heart failure with preserved ejection fraction. Monaldi Arch Chest Dis. https://doi.org/10.4081/monaldi.2020.1329
Wang T, Yu F-C, Wei Q et al (2022) Sleep-disordered breathing in heart failure patients with different etiologies. Clin Cardiol 45:778–785. https://doi.org/10.1002/clc.23840
Bosanquet JP, Bade BC, Zia MF et al (2011) Patients with venous thromboembolism appear to have higher prevalence of obstructive sleep apnea than the general population. Clin Appl Thromb Hemost 17:E119–124. https://doi.org/10.1177/1076029610389023
Cai A, Zhang J, Wang R et al (2018) Joint effects of obstructive sleep apnea and resistant hypertension on chronic heart failure: a cross-sectional study. Int J Cardiol 257:125–130. https://doi.org/10.1016/j.ijcard.2017.10.089
Fan J, Wang X, Ma X et al (2019) Association of obstructive sleep apnea with cardiovascular outcomes in patients with acute coronary syndrome. J Am Heart Assoc 8:e010826. https://doi.org/10.1161/JAHA.118.010826
Frangopoulos F, Nicolaou I, Zannetos S et al (2020) Association between respiratory sleep indices and cardiovascular disease in sleep apnea-a community-based study in Cyprus. J Clin Med 9:2475. https://doi.org/10.3390/jcm9082475
Mazzotti DR, Keenan BT, Lim DC et al (2019) Symptom subtypes of obstructive sleep apnea predict incidence of cardiovascular outcomes. Am J Respir Crit Care Med 200:493–506. https://doi.org/10.1164/rccm.201808-1509OC
Platek AE, Szymanski FM, Filipiak KJ et al (2017) Stratification of cardiovascular risk in patients with atrial fibrillation and obstructive sleep apnea-validity of the 2MACE score. Sleep Breath 21:601–606. https://doi.org/10.1007/s11325-017-1469-6
Pleavă R, Gaiţă D, Ardeleanu C et al (2016) Obesity in association with sleep apnea syndrome as predictor for coronary-vascular comorbidities. Pneumologia 65:14–18.
Quintos A, Naranjo M, Kelly C et al (2019) Recognition and treatment of sleep-disordered breathing in obese African American hospitalized patients may improve outcome. J Natl Med Assoc 111:176–184. https://doi.org/10.1016/j.jnma.2018.09.003
Roche F, Xuong ANT, Court-Fortune I et al (2003) Relationship among the severity of sleep apnea syndrome, cardiac arrhythmias, and autonomic imbalance. Pacing Clin Electrophysiol 26:669–677. https://doi.org/10.1046/j.1460-9592.2003.00116.x
Sharma S, Mukhtar U, Kelly C et al (2017) Recognition and treatment of sleep-disordered breathing in obese hospitalized patients may improve survival. The HoSMed Database. Am J Med 130:1184–1191. https://doi.org/10.1016/j.amjmed.2017.03.055
Sweed RA, Hassan S, ElWahab NHA et al (2019) Comorbidities associated with obstructive sleep apnea: a retrospective Egyptian study on 244 patients. Sleep Breath 23:1079–1085. https://doi.org/10.1007/s11325-019-01783-w
Tafelmeier M, Luft L, Zistler E et al (2021) Central Sleep Apnea predicts pulmonary complications after cardiac surgery. Chest 159:798–809. https://doi.org/10.1016/j.chest.2020.07.080
Tang M, Wang Y, Wang M et al (2021) Risk for cardiovascular disease and one-year mortality in patients with chronic obstructive pulmonary disease and obstructive sleep apnea syndrome overlap syndrome. Front Pharmacol 12:767982. https://doi.org/10.3389/fphar.2021.767982
Wang Y, Schöbel C, Penzel T (2022) Management of obstructive sleep apnea in patients with heart failure. Front Med (Lausanne) 9:803388. https://doi.org/10.3389/fmed.2022.803388
Bradley TD, Floras JS (2003) Sleep apnea and heart failure: part I: obstructive sleep apnea. Circulation 107:1671–1678. https://doi.org/10.1161/01.CIR.0000061757.12581.15
Khattak HK, Hayat F, Pamboukian SV et al (2018) Obstructive sleep apnea in Heart failure: review of prevalence, treatment with continuous positive airway pressure, and prognosis. Tex Heart Inst J 45:151–161. https://doi.org/10.14503/THIJ-15-5678
Seiler A, Camilo M, Korostovtseva L et al (2019) Prevalence of sleep-disordered breathing after stroke and TIA: a meta-analysis. Neurology 92:e648–e654. https://doi.org/10.1212/WNL.0000000000006904
Johnson KG, Johnson DC (2010) Frequency of sleep apnea in stroke and TIA patients: a meta-analysis. J Clin Sleep Med 6:131–137.
Goyal A, Pakhare A, Joshi A (2023) Prevalence of OSA in Indian population and diagnostic accuracy of different tools for OSA. ERJ Open Res 9:58. https://doi.org/10.1183/23120541.sleepandbreathing-2023.58
Leong WB, Arora T, Jenkinson D et al (2013) The prevalence and severity of obstructive sleep apnea in severe obesity: the impact of ethnicity. J Clin Sleep Med 9:853–858. https://doi.org/10.5664/jcsm.2978
Ardeshna DR, Bob-Manuel T, Nanda A et al (2018) Asian-Indians: a review of coronary artery disease in this understudied cohort in the United States. Ann Transl Med 6:12–12. https://doi.org/10.21037/atm.2017.10.18
Sawunyavisuth B (2018) What are predictors for a continuous positive airway pressure machine purchasing in obstructive sleep apnea patients? Asia-Pacific J Sci Technol 23:APST-23-03-10
Sawunyavisuth B (2018) What personal experiences of CPAP use affect CPAP adherence and duration of CPAP use in OSA patients? J Med Assoc Thai 101:S245–S249
Kaewkes C, Sawanyawisuth K, Sawunyavisuth B (2020) Are symptoms of obstructive sleep apnoea related to good continuous positive airway pressure compliance? ERJ Open Res 6:1–4. https://doi.org/10.1183/23120541.00169-2019
Sawunyavisuth B, Sopapol N, Tseng C-H, Sawanyawisuth K (2023) Marketing factors associated with a continuous positive airway pressure machine purchasing in patients with obstructive sleep apnea. Future Sci OA. https://doi.org/10.2144/fsoa-2022-0073
Chan MTV, Wang C-Y, Seet E et al (2014) Postoperative vascular complications in unrecognised obstructive sleep apnoea (POSA) study protocol: an observational cohort study in moderate-to-high risk patients undergoing non-cardiac surgery. BMJ Open 4:e004097. https://doi.org/10.1136/bmjopen-2013-004097
Funding
This study was granted by Faculty of Medicine, Khon Kaen University, Thailand (Grant Number SY67002).
Author information
Authors and Affiliations
Contributions
Study concept and design: W.P., P.H., K.S., and S.K. Acquisition of data: all authors. Analysis and interpretation of data: all authors. Searching: C.N. Statistical analysis: C.N. and K.S. Drafting of the manuscript: W.P. and S.K. Critical revision of the manuscript for important intellectual content: all authors.
Corresponding authors
Ethics declarations
Ethical approval
This work required no ethical approval.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Prechaporn, W., Hantrakul, P., Ngamjarus, C. et al. Pooled prevalences of obstructive sleep apnea and heart failure: a systematic review and meta-analysis. Heart Fail Rev 29, 811–826 (2024). https://doi.org/10.1007/s10741-024-10399-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10741-024-10399-6