
Abstract
Background and Aims
Endoscopic ultrasound (EUS) guided choledochoduodenostomy using a lumen-apposing metal stent (LAMS) allows access to the biliary system with a sufficiently large diameter stent. However, an appropriate endoscope for this purpose is required. We evaluated the feasibility of per-oral cholangioscopy (POC) using a multibending ultra-slim endoscope through a LAMS for EUS-guided choledochoduodenostomy.
Methods
Twelve patients who underwent EUS-guided choledochoduodenostomy, followed by POC via a LAMS, were enrolled. POC was performed with an multibending ultra-slim endoscope. The primary outcome was technical success, defined as examination of both hepatic ducts and either the distal common bile duct or stricture site within 10 min. The types of intervention and adverse events were also assessed.
Results
Technical success was achieved in all cases with the multibending ultra-slim endoscope. Narrow-band imaging endoscopy was performed in five cases (41.7%) and POC-guided targeted biopsy was performed in three cases (25.0%). Stone extraction during POC was performed in two patients (16.7%) and foreign body removal from the intrahepatic duct was performed in one patient. One patient underwent additional metal stent insertion under direct visualization. After POC, no stent migration or severe adverse events were seen in any case.
Conclusions
POC using a multibending ultra-slim endoscope for diagnostic or therapeutic purposes can be performed effectively and safely through a LAMS after EUS-guided choledochoduodenostomy.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Endoscopic ultrasound (EUS)-guided biliary drainage could be an option in cases of failed or difficult biliary cannulation [1, 2]. EUS-guided choledochoduodenostomy (EUS-CDS) with a lumen-apposing metal stent (LAMS) can also be used to access the biliary system [3]. The feasibility of per-oral cholangioscopy (POC) through this novel route has not been well-evaluated. However, it is expected to be technically challenging due to the long, narrow tubular structure of the bile duct and acute angulation between the LAMS and bile duct. To overcome the structural difficulties, a suitable endoscope is required. Recently, a multibending ultra-slim endoscope (MB endoscope) with two bending parts was developed for direct POC and showed high technical success due to its unique specifications [4]. We believe that the MB endoscope is also suitable for POC through a LAMS. Hence, we evaluated the efficacy of POC using an MB endoscope through a LAMS for EUS-CDS in patients with distal malignant biliary strictures (MBS).
Methods
Study Design
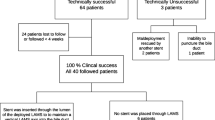
This is a feasibility study of MB endoscopes for POC through a LAMS for EUS-CDS. We retrospectively analyzed the prospectively collected data of patients who underwent POC via CDS using MB endoscope between October 2017 and September 2020 at a single tertiary care center (Fig. 1). The study was approved by the Institutional Review Board of SoonChunHyang University Bucheon Hospital.

Schematic of the study design
Patients
Patients who required diagnostic and therapeutic biliary procedures after EUS-CDS using a LAMS were included in this study. The indications for POC were evaluation of a bile duct lesion, endoscopic removal of bile duct stones, and the need for other advanced therapeutic procedures under direct visualization.
Instruments
Fully covered, self-expandable metal stents for lumen apposition with an electrocautery-enhanced (ECE) or non-ECE delivery system (Niti-S HOT SPAXUS or Niti-S SPAXUS; Taewoong Medical, Ilsan, South Korea) were used for EUS-CDS. The length of the stent was 20 mm, which was reduced to 7 mm by folding back both flanges. The diameter of the stent used in this study was 10 or 8 mm.
A third-generation prototype MB endoscope (CHF-Y0010; Olympus Medical Systems, Tokyo, Japan) was used for POC. The MB endoscope was described previously [4]. It is a reusable, forward-viewing endoscope with two bending sections and two working channels (2.2 and 1.0 mm). The characteristics of the MB and ultra-slim endoscope were compared in Table 1s (Fig. 1s).
Procedures
EUS-CDS Using a LAMS
All procedures were performed under conscious sedation. A linear echoendoscope (GF-UCT240; Olympus Medical Systems) was used. After advancement of the echoendoscope into the duodenal bulb, a 19-gauge needle (EZ Shot 3 Plus; Olympus Medical Systems) was used for puncture with color Doppler followed by placement of a 0.025-inch guidewire (VisiGlide; Olympus Medical Systems). After removing the needle and dilating the tract using a 6 Fr cystotome (Endo-Flex, GmbH, Voerde, Germany), a non-ECE-LAMS was inserted (Fig. 2s, Video 1s). An ECE-LAMS using pure cut current was inserted without tract dilatation.

Cholangiograms of a multibending ultra-slim endoscope being successfully advanced through the lumen-apposing metal stent for choledochoduodenostomy
Direct POC Using a MB Endoscope
Per-oral cholangioscopy through a LAMS was conducted 7–14 days after its placement. POC using a MB endoscopes was performed in all patients. After achieving technical success, the diagnostic and therapeutic procedures were performed as required. After the endoscope had been passed through the LAMS, insufflation of carbon dioxide was stopped. Irrigation with saline solution (sodium chloride 0.9%) and frequent suction were performed in the biliary tree. The endoscope was advanced under fluoroscopic and endoscopic control. After examination with white-light imaging, narrow-band imaging (NBI) was performed if there was a suspected lesion based on previous literatures from Mounzer et al. [5] and Robles-Medranda et al. [6]. Targeted biopsy was conducted under direct visualization using 5 Fr forceps (FB-39Q; Olympus Medical Systems). Stone extractions were performed using a 5 Fr lithotomy basket (MTW Endoskopie, Wesel, Germany).
Outcomes
The primary outcome was the technical success rate of POC. Technical success was defined as complete endoscopic examination of both hepatic ducts and either the distal common bile duct or obstructed site within 10 min (Fig. 2, Video 1). The secondary outcomes were successful endoscopic intervention under direct visualization, and the number and type of procedure-related adverse events (AEs). Patients were monitored for procedure-related AEs such as stent migration, perforation, cholangitis, and air embolism for 7 days after POC. AEs were graded using the criteria of the American Society for Gastrointestinal Endoscopy [7].
Statistical Analysis
All statistical analyses were performed using SPSS for Windows software (ver. 25.0; SPSS Inc., Chicago, IL, USA). Categorical variables are expressed as frequencies with percentages. Continuous data are expressed as median with interquartile range (IQR).
Results
Twelve patients underwent POC through a LAMS with an MB endoscope. The median (IQR) patient age was 60.5 (54.5–75.8) years and 6 (50%) patients were male. The two most common etiologies of distal MBS were cholangiocarcinoma (41.7%) and pancreatic cancer (41.7%). Five patients underwent EUS-CDS with an ECE-LAMS (Table 1).
The POCs were performed approximately 7.5 (4.0–33.8) days after EUS-CDS. All 12 of the POCs using the MB endoscope were technically successful. After successful intubation with the MB endoscope, diagnostic and therapeutic interventions were performed as required (Table 2, Fig. 3). Image-enhanced endoscopy using NBI and targeted biopsy was performed in five (41.7%) and three (25.0%) patients, respectively. On pathologic examination, two patients were diagnosed with adenocarcinoma (Fig. 3D). Four patients underwent advanced therapeutic procedures. Stone extraction using a 5 Fr lithotomy basket was performed in two patients (Fig. 3E, Fig. 4A). One patient showed repeated cholangitis due to food impaction within the LAMS, so an additional self-expandable metal stent was inserted into the duodenum under direct visualization (Fig. 4B, 4C, Video 2). In one patient with a broken PTBD catheter within the biliary tree, foreign body removal was performed under direct visualization. There were no cases of procedure-related stent migration. There were two cases of mild cholangitis after POC, which were treated conservatively (Table 2).

Diagnostic evaluation performed using per-oral cholangioscopy (POC). (A) Mass lesion on the bile duct. (B) The mucosal structures and tumor vessels on narrow-band imaging. (C) Cholangioscopic image of the targeted biopsy under direct visualization and (D) pathologic confirmation of adenocarcinoma (H&E, original magnification 200 ×). (E) Stones in bile duct

Therapeutic intervention using a lumen-apposing metal stent (LAMS). (A) Stone removal using 5 Fr basket. (B) Radiograph showing metal stent insertion through the LAMS. (C) Cholangioscopic view of the metal stent
Discussion
POC allows for intra-ductal evaluation of bile duct strictures or obstructions, and has also facilitated therapeutic interventions including lithotripsy, tumor ablation, and selective guidewire access [8]. POC was traditionally performed via the transpapillary route. EUS-CDS using LAMS offered another route to the biliary tree. LAMS can be used as a port for further interventions. This stent, designed specifically for EUS-guided drainage, can also serve as a bridge for direct endoscopic necrosectomy (DEN) in pancreatic fluid collection [9], and for cholecystoscopy after EUS-guided gallbladder drainage [10]. Regarding CDS, the only available case report described extraction of the IHD stone through the LAMS [3]. For EUS-CDS, LAMS with smaller diameters tend to be placed to prevent overdilation of the bile duct after stenting [1]. An acute angle between the bile duct and stent could prevent smooth advancement of the endoscope into the bile duct. Hence, a conventional endoscope for gastroscopy would not be suitable for POC via a fistulous tract created by the LAMS.
In the current study, we found that the MB endoscope, which is known to be effective for direct POC, was also useful in POC through a LAMS due to its delicate structure [4]. The MB endoscope had a high technical success rate in the POCs via LAMS in this study. During the POCs, diagnostic interventions and therapeutic procedures, such as stone extraction, insertion of an additional metal stent, and foreign body removal, were possible. Possible indications for POC through LAMS could be as follows: (1) diagnosis of combined neoplastic disease or stone in the gallbladder; (2) evaluation for the tumor extension; (3) endoscopic removal of a stone under direct visualization; (4) additional intervention for managing malignant stricture through LAMS. Using the specification of MB endoscope combined with future development of accessory for this endoscope, it is expected that various therapeutic procedures would be possible.
The MB endoscope has advantages for evaluation of narrowed and angled bile ducts. Since the MB endoscope is a modified version of the ultra-slim endoscope, it produces similarly high-resolution images quality. Two bending parts at the distal end of the insertion tube enable flexible intubation through the acute angle. A thick insertion tube and long total working length of 1,330 mm are favorable for preventing loop formation, and have made it possible to maintain the same position during cholangioscopy. In addition, two channels for instruments allow various procedures to be performed within the narrow and angular bile duct.
There were only a small number of cholangitis cases in our series, and all stents remained stable (without migration) after direct POC through a LAMS. The best time to perform interventions through the bypass after LAMS placement remains unclear. In previous reports of per-oral cholecystoscopy through a LAMS, the endoscope was typically passed through the LAMS after 1 to 3 months, but in some cases cholecystoscopy was performed within a few days after LAMS insertion [10]. In another study reporting placement of a LAMS in cases of walled off necrosis, DEN was performed at the time of initial stent deployment [11]. Determining the optimal interval between LAMS insertion and additional procedures through the stent should be a target for future studies.
Malignant biliary obstruction can be complicated by recurrent cholangitis, sepsis, and hepatic failure [4]. In patients with distal MBS, ERCP is often unavailable due to cancer progression [12]. Traditionally, PTBD has been used as salvage treatment [13, 14]. EUS-guided drainage could be used instead of PTBD for further procedures [3, 15, 16]. Some previous studies have reported POC assisted advanced procedures after EUS-guided hepaticogastrostomy (HGS) [17, 18]. Similar to EUS-HGS, EUS-CDS could also facilitate further interventions. There is no consensus regarding the use of an artificial fistula created by a stent for advanced interventions, but this may be an option when the ampulla is inaccessible due to MBS.
There were several strengths to this study. To the best of our knowledge, it was the first study to evaluate the feasibility of the POC through a LAMS. We also provided a clear definition of technical success for POC via a LAMS, and compared the MB and conventional endoscopes. In addition, we introduced a variety of therapeutic interventions meriting further study.
Our study also had several limitations. First, it used a retrospective design and included a small number of patients (as a feasibility study). Also, there was no POC protocol for EUS-CDS due to the study design, which made our results less reliable. To overcome these issues, every step of the procedure was carefully reviewed through images and videos. The time limit suggested in this study was set considering previous literature [4] regarding conventional POC using MB endoscope and should be clarified in the future study. Second, EUS-CDS using a LAMS is only available in a few centers. However, the use of the LAMS is expected to increase due to the availability of ECE delivery systems, which simplify the procedure. Third, this study only involved endoscopists highly experienced in the procedures of direct POC, and MB endoscopes that are not yet commercially available. Thus, the results may not be generalizable to other institutions. Further studies including endoscopists with varying skill levels are required.
In conclusion, POC using an MB endoscope, in which an anastomosis site was created by a LAMS, was safe and effective. This approach could facilitate the performance of various procedures in patients with MBS. Larger studies are required to validate our results.
References
Tsuchiya T, Teoh AYB, Itoi T et al. Long-term outcomes of EUS-guided choledochoduodenostomy using a lumen-apposing metal stent for malignant distal biliary obstruction: a prospective multicenter study. Gastrointest Endosc. 2018;87:1138–1146.
Isayama H, Nakai Y, Itoi T et al. Clinical practice guidelines for safe performance of endoscopic ultrasound/ultrasonography-guided biliary drainage: 2018. J Hepatobiliary Pancreat Sci. 2019;26:249–269.
Mukai S, Itoi T, Tsuchiya T, Tanaka R, Tonozuka R. EUS-guided intrahepatic bile duct stone extraction via choledochoduodenostomy created by a lumen-apposing metal stent. Gastrointest Endosc. 2016;83:832–833.
Lee YN, Moon JH, Lee TH et al. Prospective randomized trial of a new multibending versus conventional ultra-slim endoscope for peroral cholangioscopy without device or endoscope assistance (with video). Gastrointest Endosc. 2020;91:92–101.
Mounzer R, Austin GL, Wani S, Brauer BC, Fukami N, Shah RJ. Per-oral video cholangiopancreatoscopy with narrow-band imaging for the evaluation of indeterminate pancreaticobiliary disease. Gastrointest Endosc. 2017;85:509–517.
Robles-Medranda C, Valero M, Soria-Alcivar M et al. Reliability and accuracy of a novel classification system using peroral cholangioscopy for the diagnosis of bile duct lesions. Endoscopy. 2018;50:1059–1070.
Cotton PB, Eisen GM, Aabakken L et al. A lexicon for endoscopic adverse events: report of an ASGE workshop. Gastrointest Endosc. 2010;71:446–454.
Moon JH, Terheggen G, Choi HJ, Neuhaus H. Peroral cholangioscopy: diagnostic and therapeutic applications. Gastroenterology. 2013;144:276–282.
Chen YI, Barkun AN, Adam V et al. Cost-effectiveness analysis comparing lumen-apposing metal stents with plastic stents in the management of pancreatic walled-off necrosis. Gastrointest Endosc. 2018;88:267–276.
Chan SM, Teoh AYB, Yip HC, Wong VWY, Chiu PWY, Ng EKW. Feasibility of per-oral cholecystoscopy and advanced gallbladder interventions after EUS-guided gallbladder stenting (with video). Gastrointest Endosc. 2017;85:1225–1232.
Yan L, Dargan A, Nieto J et al. Direct endoscopic necrosectomy at the time of transmural stent placement results in earlier resolution of complex walled-off pancreatic necrosis: Results from a large multicenter United States trial. Endosc Ultrasound. 2019;8:172–179.
Hatamaru K, Kitano M. EUS-guided biliary drainage for difficult cannulation. Endosc Ultrasound. 2019;8:S67–S71.
Baars JE, Kaffes AJ, Saxena P. EUS-guided biliary drainage: A comprehensive review of the literature. Endosc Ultrasound. 2018;7:4–9.
Teoh AYB, Dhir V, Kida M et al. Consensus guidelines on the optimal management in interventional EUS procedures: results from the Asian EUS group RAND/UCLA expert panel. Gut. 2018;67:1209–1228.
Mandai K, Uno K, Yasuda K. A direct peroral cholangioscopy-assisted therapy for a choledochojejunostomy anastomotic stricture via EUS-guided hepaticogastrostomy. J Hepatobiliary Pancreat Sci. 2020;27:437–438.
Mukai S, Tsuchiya T, Itoi T. Endoscopic ultrasonography-guided hepaticogastrostomy with novel two-step puncture technique following peroral cholangioscopy-assisted stone removal. Dig Endosc. 2020;32:e32–e33.
Sanchez-Ocana R, Penas-Herrero I, de la Serna-Higuera C, Perez-Miranda M. Peroral transhepatic cholangioscopy and antegrade sphincterotomy via EUS-guided anastomosis. Gastrointest Endosc. 2016;83:466–467.
Mukai S, Tsuchiya T, Itoi T. Interventional endoscopic ultrasonography for benign biliary diseases in patients with surgically altered anatomy. Curr Opin Gastroenterol 2019;35:408–415.
Acknowledgments
We thank Olympus Medical Systems for providing the multibending ultra-slim endoscope unit. We also thank A Ri Song, RN, Song Ah Jeong, RN, Sun Yeong Moon, RN, Sun Hwa Cho, RN and all of the other nursing staff, for their support and assistance with the procedure.
Funding
None of the other authors have any financial relationships relevant to this publication. This work was supported, in part, by the SoonChunHyang University Research Fund.
Author information
Authors and Affiliations
Contributions
Conception and design: Jong Ho Moon, Yun Nah Lee, Analysis and interpretation of the data: Hae Won Yoo,. Drafting of the article: Hae Won Yoo, Critical revision of the article for important intellectual content: Jong Ho Moon, Yun Nah Lee, Il Sang Shin, Jae Kook Yang, Tae Hoon Lee, Sang-Woo Cha, Young Deok Cho, Sang-Heum Park, Final approval of the article: all of authors.
Corresponding author
Ethics declarations
Conflicts of interest
The authors disclose no conflicts.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Video 1. Per-oral cholangioscopy through a lumen-apposing metal stent (LAMS) with a conventional ultra-slim endoscope and multibending ultra-slim endoscope. (MP4 28490 KB)
Video 2. Metal stent insertion through the lumen-apposing metal stent (LAMS). (MP4 43596 KB)
Supplementary file4 (WMV 9197 KB)
Rights and permissions
About this article

Cite this article
Yoo, H.W., Moon, J.H., Lee, Y.N. et al. Feasibility of Cholangioscopy Using Multibending Ultra-Slim Endoscope Through a Lumen-Apposing Metal Stent for Choledochoduodenostomy. Dig Dis Sci 68, 268–273 (2023). https://doi.org/10.1007/s10620-022-07531-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-022-07531-7