
Abstract
Background
A novel lumen-apposing, self-expanding metal stent to perform EUS-guided drainage procedures has been recently developed. The aim of this study was to analyze the safety, technical and clinical effectiveness of this device for EUS-guided choledochoduodenostomy (EUS-CD) with palliative intent.
Methods
Retrospective analysis of all consecutive patients with unresectable malignant distal bile duct obstruction who, between March 2012 and September 2014, underwent EUS-CD using the study devices (AXIOS™ and Hot AXIOS™, Xlumena Inc., Mountain View, CA, USA) after unsuccessful ERCP in seven European centers was carried out.
Results
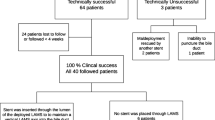
Fifty-seven patients (M/F 31/26; median age 73) underwent EUS-CD using the AXIOS™ stent or the Hot AXIOS™ delivery system. ERCP failure was due to duodenal obstruction in 41 patients (71.9 %) and to inability to cannulate the papilla in the remaining 16 patients (28.1 %). The procedure was technically successful in 56/57 patients (98.2 %), with a mean procedural time of 22.4 min (range 11–65). Clinical success was achieved in 54 of these 56 patients (96.4 %; 94.7 % of the entire cohort). Overall major procedural complication rate was 7 % (two duodenal perforations, one bleeding and one transient cholangitis). During follow-up, 5 out of 54 (9.3 %) patients with clinica success required re-intervention for stent migration in one case and a sump syndrome with transient increase in serum bilirubin concentrations with sludge in the distal duct reservoir in the remaining four patients.
Conclusions
Our study shows that EUS-CD using the AXIOS™ and the Hot AXIOS™ devices is a safe procedure, with high technical and clinical success rates.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Endoscopic retrograde cholangiopancreatography (ERCP) is the current standard of care for palliation of patients with unresectable malignant biliary obstruction. However, failure of ERCP due to malignant duodenal obstruction, inability to cannulate the papilla or traverse a common bile duct (CBD) stricture requires alternative methods of decompression [1, 2]. Options include percutaneous drainage, surgical bypass and more recently EUS-guided biliary drainage (EUS-BD) [3–5].
In an attempt to maintain internalized biliary drainage, EUS-guided methods are being used more and more frequently [6–8]. Technical and clinical success rates for EUS-BD have been reported to be high (91 and 88 %, respectively) [9]. However, the occurrence of complications has also been reported to be high (26 % with mortality of 0.4 %) [9], mostly reflecting the learning curve and the heterogeneity of the techniques used, but also the utilization of accessories not specifically designed for this procedure [10].
In the last few years, efforts to overcome this latter limitation by developing dedicated accessories to facilitate EUS-BD and decrease the risk of complications have been made. In particular, a lumen-apposing, fully covered self-expandable metal stent (LA–FCSEMS) specifically designed with the aim of creating anastomosis has become available and tested for drainage of pancreatic fluid collections and gallbladder, the latter in patients with acute cholecystitis unfit for surgery [11–17]. Moreover, case reports of successful EUS-guided choledochoduodenostomy (EUS-CD) by using this newly available stent have been recently published [18, 19].
The present study aimed to retrospectively analyze the safety and clinical effectiveness of EUS-CD using this newly available LA–FCSEMS in a large cohort of patients prospectively enrolled in seven European centers.
Materials and methods
All consecutive patients who, between March 2012 and September 2014, underwent EUS-BD using the study devices (AXIOS™ and Hot AXIOS™, Xlumena Inc., Mountain View, CA, USA) in seven tertiary care medical centers were retrospectively retrieved from each single-institution database. All included patients had malignant distal CBD obstruction that was inoperable, or they were unfit for surgery and all underwent attempted palliative ERCP, which failed.
The protocol to carry out retrospective revision of the cases performed was approved by all the local institutional ethics committees. All patients gave their informed consent prior to the use of the AXIOS™ and the Hot AXIOS™ devices.
The AXIOS™ stent and the Hot AXIOS™ system
The AXIOS™ stent is made up of braided nitinol that is fully covered with silicone, with wide flanges on both ends that provide anchoring within the bile duct (Fig. 1; Table 1). The stent is delivered through a 9- or a 10.8-French catheter, which is luer-locked to the inlet port of the echoendoscope’s working channel to provide deployment of the stent under full control by the endoscopist. Since the middle of 2013, the AXIOS™ stent was incorporated into a novel device, the Hot AXIOS™, in which an electrocautery wire was added to the distal tip of the delivery catheter to apply cutting current that allows the passage of the device through the gastrointestinal and the bile duct walls, without the need for prior dilation. The AXIOS™ and Hot AXIOS™ are CE-marked for CBD drainage.

The AXIOS™ stent made up of braided nitinol that is fully covered with silicone, with wide flanges on both ends to provide anchorage
EUS drainage procedure
All endoscopic procedures were performed under deep sedation or general anesthesia with endotracheal intubation. All, but one operator, were proficient in both ERCP and EUS procedures. Patients who were not undergoing antibiotic therapy prior to the procedure received prophylactic antibiotics, based on each center guidelines. Post-procedural continuation of antibiotics was upon endoscopist’s discretion.
A therapeutic linear echoendoscope was used in all cases. The echoendoscope was advanced into the duodenal bulb where by orienting the transducer medially, the dilated CBD or the common hepatic duct was visualized. Biliary access was achieved from the duodenal bulb using a 19-gauge EUS needle, which was followed by contrast injection and placement of a 0.035-in. guidewire. Dilation of the tract was done using a graduated dilation catheter, a 4-mm biliary dilation balloon or a 6-French cystotome (ENDO-FLEX GmbH, Voerde, Germany) based on endoscopist’s preference. When the Hot AXIOS™ was used, there was no need for tract dilation and insertion of the device was achieved by direct puncture with the device using pure cut without coagulation.
The choice of the size of the stent to be placed was independently taken by each individual endoscopist, without defined pre-procedural parameters. Once inside the CBD, the proximal flange of the stent was deployed under EUS guidance (Fig. 2), while the distal flange was deployed in the duodenum under EUS guidance or endoscopic view, with or without fluoroscopic assistance (Fig. 3). All procedures were performed using carbon dioxide insufflation.

EUS view of the distal flange of the AXIOS™ stent (arrow) opened inside a dilated common bile duct (CBD)

Endoscopic view of the proximal flange of the AXIOS™ stent placed in the duodenal bulb
Procedural time was calculated in all cases from echoendoscope insertion to complete release of the stent.
Outcome parameters
The primary outcome parameters were safety, technical and clinical success. Safety was defined by the frequency of occurrence of major procedure-related complications, such as bile leakage, bleeding or perforation.
Technical success was defined as satisfactory access and drainage of the CBD as determined by the successful placement of the AXIOS stent. Clinical success was defined as decline of serum bilirubin levels in patients with obstructive jaundice to <10 % of the initial levels and of the cholestatic parameters in those with cholestasis without jaundice.
Short- and long-term complications such as stent migration, stent occlusion with recurrent obstructive jaundice and/or cholangitis were assessed during follow-up on the basis of clinical need by biochemical and/or imaging studies.
Data analysis
Frequencies, percentages, means (±standard deviation) and medians (range) were used, as appropriate, for descriptive analysis.
Results
Study population
During the study period, 57 patients with inoperable malignant distal biliary obstruction who failed ERCP underwent EUS-CD using the study devices. Table 2 shows patient demographics and characteristics of the entire cohort.
The cause for ERCP failure was duodenal obstruction with inaccessible papilla in 41 patients (71.9 %) and inability to cannulate the papilla, despite the utilization of different advanced biliary cannulation techniques, in the remaining 16 patients (28.1 %). Fifty-three patients (93 %) had obstructive jaundice, while in 4 patients (7 %) there was cholestasis without increased bilirubin serum concentration. Additionally, 20 patients (35.1 %) were experiencing concomitant cholangitis or sepsis, while in 19 cases (33.3 %) ascites was present mostly detected during the EUS examination.
Drainage procedure and outcomes
Table 3 shows specifics of the drainage procedures. EUS-CD was performed during the same session following ERCP failure in all cases using the AXIOS™ or the Hot AXIOS™ devices in 27 and 30 patients, respectively. The median CBD diameter was 17.9 mm (range 8–35). Stent placement was technically successful in all but one case (98.2 %). In the failed case, duodenal perforation occurred while performing dilation of the tract needed to allow for subsequent insertion of the AXIOS™ stent delivery device. The perforation site was closed by placement of endoscopic clips, and EUS-guided hepaticogastrostomy was successfully performed instead, with uneventful recovery of the patient.
In patients with duodenal stenosis, duodenal stenting using different types of uncovered metal stents was performed, when clinically necessary, before, during the same session or the day after the EUS-CD procedure. When performed after EUS-CD, the duodenal stent overlapped the AXIOS™ stent.
In the 56 patients in whom LA–FCSEMS placement was technically successful, the median procedural time was 22.4 min (range 11–65) with no difference between the AXIOS™ and the Hot AXIOS™. A 6-mm internal diameter and 8-mm-long stent was used in 36 patients (64.2 %), an 8 mm × 8 mm in 2 patients (3.6 %), a 10 mm × 10 mm stent in 16 patients (28.6 %) and a 15 mm × 10 mm in 2 patients (3.6 %). Clinical success was achieved in 54 of these 56 patients (96.4 %; 94.7 % of the entire cohort). Two patients, who presented with sepsis and multi-organ failure prior to any intervention, died within 4 days of EUS-CD. In both patients, the EUS-CD was technically successful with effective biliary drainage as demonstrated by a substantial decrease in serum bilirubin concentration. This, however, was not enough to reverse their multi-organ failure, and they ultimately died.
Procedure-related complications
In addition to the duodenal perforation described above, another case of duodenal perforation occurred and was caused directly by the tip of the echoendoscope during evaluation of the most appropriate site where to perform the drainage. The perforation site was located at the apex of the duodenal bulb and was immediately closed using an over the scope clip (OTSC®, Ovesco Endoscopy GmbH, Tübingen, Germany). A window opportunity beside the OVESCO clip was found, which allowed the performance of EUS-CD with placement of a clinically effective AXIOS™ stent.
One patient with neoplastic infiltration of the duodenum experienced a severe acute arterial bleeding right after insertion of the Hot AXIOS™. He required coil embolization of the gastroduodenal artery and temporary placement alongside the LA–FCSEMS of a percutaneous biliary drainage catheter, which was removed 14 days afterward without any further adverse event.
One patient developed transient and self-limiting cholangitis after insertion of the AXIOS™ stent, without any evidence of stent occlusion or malfunction at the endoscopic examination.
Overall, complications occurred more frequently when the AXIOS™ stent was used, but without any significant difference as compared with the Hot AXIOS™.
Follow-up
The 54 patients with technical and clinical successful biliary drainage were followed up for a mean of 151 ± 145 days. At the end of follow-up, 15 patients were still alive.
One patient experienced spontaneous migration of the stent into the duodenum 7 days after insertion. This was incidentally detected at abdominal CT requested by the oncologist for routine check-up. The patient was completely asymptomatic, with normal liver function tests. Esophagogastroduodenoscopy revealed a mature CD tract with active bile flow. A new AXIOS™ stent of the same diameter and length (6 mm × 8 mm) was placed across the fistula, while the previously placed stent was removed, being wedged by the proximal end of the duodenal stent.
Four patients presented signs of intermittent malfunction of the LA–FCSEMS with transient increase in serum bilirubin concentrations. Control ERCP via CD revealed the presence of sludge in the distal duct reservoir in all patients, without any evidence of food impaction, consistent with a sump syndrome. All these cases were resolved by placement of a double-pigtail plastic stent through the CD, which was removed after 2 weeks without any further recurrence.
Overall at the end of follow-up, the stent was patent without any intervention in 49 patients (90.7 %).
Discussion
We retrospectively evaluated a large cohort of prospectively enrolled patients with malignant distal CBD obstruction who underwent EUS-CD, after failed attempted ERCP, using a newly available LA–FCSEMS specifically designed to create anastomosis. We found that stent placement was technically successful in all but one patient, with a very high clinical success rate of 94.7 % and low rates of procedure-related complications and re-interventions.
EUS-guided biliary drainage has become an attractive treatment alternative to the percutaneous route for effective biliary decompression in patients with unresectable malignant biliary obstruction after unsuccessful ERCP. Recent studies have reported EUS-BD to be as effective as percutaneous drainage [20, 21], with a lower rate of complications and with substantial reduction of costs, mostly due to reduced need for re-interventions [21].
Technically, EUS-BD can be performed with either a transgastric (intrahepatic) or transduodenal (extrahepatic) approach [7, 8, 22]. When a guidewire can be efficiently manipulated across the ampulla into the duodenum, the drainage can be completed by performing either a rendezvous procedure [23] or antegrade transpapillary biliary stent placement directly under EUS guidance [24, 25]. Alternatively, in all the other situations in which the guidewire cannot be passed through the ampulla, direct transluminal stenting can be done [7, 8].
Presently, the choice of the route of access and of the technique utilized to carry out the procedure is not standardized and usually depends on the endoscopist’ preference. Both rendezvous and direct transluminal stenting techniques as well as the use of the transhepatic route compared to the transduodenal route appear to be equally safe and effective [26, 27]. Importantly, the overall complications rate remains high (20.6 %), with a reported mortality of 4.4 % [22]. These high rates of complications may be in part related to a learning curve effect, but can also reflect the utilization of accessories not specifically dedicated to this procedure.
The most worrisome complication of EUS-BD using the transluminal stenting approach is bile leakage into the peritoneum or retroperitoneum, which would require surgery in most cases. This may theoretically be prevented by the use of FCSEMS, which can automatically seal the gap between the stent and the walls of the fistula through their expandability [28]. In previous studies, however, the rate of bile leakage with SEMSs ranged between 2.9 and 10 % [8, 22, 29], underlying the need for the development of dedicated SEMSs able to completely prevent the occurrence of this complication.
In our study, we used a novel LA–FCSEMS, the AXIOS™ stent, that has a peculiar design that makes possible to tightly hold together the walls of two hollow structures (in this case the bile duct and the duodenal lumen), thus potentially decreasing the risk of leakage and speeding up the process of a fistulous tract formation [11]. Indeed, no cases of bile leakage were observed in our series and in one patient in whom the stent spontaneously migrated 1 week after placement, the tract was fully developed and perfectly functional.
In the present study, we used both the AXIOS™ device and the Hot AXIOS™ delivery system to create a choledochoduodenostomy. The Hot AXIOS™ represents an evolution of the first device with the stent incorporated into a delivery system with an electrocautery wire mounted on the tip [14]. This allows the procedure to be performed in one step, from penetration in the CBD to delivery of the stent without the need for additional accessories exchange. Moreover, when using the Hot AXIOS™ device, most of the procedure can be done under complete EUS guidance with reduced need for fluoroscopic assistance, as previously shown for drainage of pancreatic fluid collections [16]. This new stent is indeed very visible by ultrasound (see Fig. 2) and represents the first accessory specifically designed for interventional EUS procedures.
In our study, EUS-BD was technically successful in all but one patient in whom a duodenal perforation occurred during balloon dilation of the tract needed to allow for insertion of the AXIOS stent device. Technical success was also obtained in three patients with a CBD diameter less than 1 cm. In these patients, the procedure was technically more challenging, because of the need to push the catheter toward the hilum to find an area of the biliary system with more space where to open the distal flange of the stent. Because of these difficulties, we highly recommend new users to start with patients with a more dilated CBD of at least 15 mm.
Clinical success with resolution of the jaundice and/or of the cholestatic parameters was achieved in 54 of the 56 patients (96.4 %; 94.7 % of the entire cohort) in whom the stent was successfully placed. These high success rates were obtained despite the multicenter nature of the study, involving seven tertiary care centers throughout Europe and the fact that this represented the first experience with this stent for EUS-BD. Most of the participants had previous experience in the use of this stent for drainage of pancreatic fluid collections [13, 16], which can be considered a sort of training opportunity before moving toward other more demanding targets/indications (i.e., the gallbladder and the CBD).
The failure cases were two patients with multi-organ failure prior to EUS-CD who died within 4 days, despite a clinically effective biliary drainage as demonstrated by a substantial decrease in serum bilirubin plasma concentration. Because of this finding, we strongly believe that in these patients death should not be considered as a complication of the EUS-CD procedure.
Procedural complications occurred in four patients (7 %), using both the AXIOS™ and the Hot AXIOS™ without any difference between them. This rate of complications is substantially lower than that reported in recent series and in a review of the published studies [8, 9, 22]. One of the complications was a duodenal perforation caused by the tip of the echoendoscope during evaluation of the most appropriate site where to perform the drainage. This complication should not be attributed to the stent placement procedure, which was indeed successfully achieved after closure of the duodenal defect by an OTSC device.
During follow-up, re-intervention was necessary in 5 of the 54 patients with follow-up (9.3 %). One patient had asymptomatic stent migration, while four patients experienced transient increase in serum bilirubin concentrations with sludge in the distal duct reservoir, consistent with a sump syndrome. All these cases were resolved by temporary placement of a double-pigtail plastic stent through the CD. The sump syndrome, first described in 1976, is a well-known phenomenon occurring after surgical side-to-side choledochoduodenostomy, with a reported prevalence ranging from 2.5 to 15.7 % [30–33], which as shown in our series can be easily treated without major drawbacks.
In conclusion, our study shows that EUS-CD using the AXIOS™ and the Hot AXIOS™ devices is a safe procedure with a high technical and clinical success rates. Future prospective multicenter studies with a standardization of the procedure are needed to fully assess the long-term patency of the stent and the re-intervention rates.
References
Halttunen J, Meisner S, Aabakken L, Arnelo U, Grönroos J, Hauge T, Kleveland PM, Nordblad Schmidt P, Saarela A, Swahn F, Toth E, Mustonen H, Löhr JM (2014) Difficult cannulation as defined by a prospective study of Scandinavian Association for Digestive Endoscopy (SADE) in 907 ERCPs. Scand J Gastroenterol 49:752–758
Bailey AA, Bourke MJ, Williams SJ, Walsh PR, Murray MA, Lee EY, Kwan V, Lynch PM (2008) A prospective randomized trial of cannulation technique in ERCP: effects on technical success and post-ERCP pancreatitis. Endoscopy 40:296–301
Ho CS, Warkentin AE (2012) Evidence-based decompression in malignant biliary obstruction. Korean J Radiol 13(Suppl 1):S56–S61
Glazer ES, Hornbrook MC, Krouse RS (2014) A meta-analysis of randomized trials: immediate stent placement vs. surgical bypass in the palliative management of malignant biliary obstruction. J Pain Symptom Manage 47:307–314
Rogart JN (2012) Endoscopic biliary access: endoscopic ultrasound joins the party. J Clin Gastroenterol 46:723–724
Khashab MA, Dewitt J (2013) EUS-guided biliary drainage: is it ready for prime time? Yes! Gastrointest Endosc 7:102–105
Kahaleh M, Artifon EL, Perez-Miranda M, Gupta K, Itoi T, Binmoeller KF, Giovannini M (2013) Endoscopic ultrasonography guided biliary drainage: summary of consortium meeting, May 7th, 2011, Chicago. World J Gastroenterol 19:1372–1379
Gupta K, Perez-Miranda M, Kahaleh M, Artifon EL, Itoi T, Freeman ML, de Serna C, Sauer B, Giovannini M, In EBD STUDY GROUP (2014) Endoscopic ultrasound-assisted bile duct access and drainage: multicenter, long-term analysis of approach, outcomes, and complications of a technique in evolution. J Clin Gastroenterol 48:80–87
Fabbri C, Luigiano C, Lisotti A, Cennamo V, Virgilio C, Caletti G, Fusaroli P (2014) Endoscopic ultrasound-guided treatments: are we getting evidence based. A systematic review. World J Gastroenterol 20:8424–8448
Fuccio L, Attili F, Vanella G, Larghi A (2014) Interventional endoscopic ultrasonography. Curr Treat Options Gastroenterol 12:183–210
Itoi T, Binmoeller KF, Shah J, Sofuni A, Itokawa F, Kurihara T, Tsuchiya T, Ishii K, Tsuji S, Ikeuchi N, Moriyasu F (2012) Clinical evaluation of a novel lumen-apposing metal stent for endosonography-guided pancreatic pseudocyst and gallbladder drainage (with videos). Gastrointest Endosc 75:870–876
Teoh AY, Binmoeller KF, Lau JY (2014) Single-step EUS-guided puncture and delivery of a lumen-apposing stent for gallbladder drainage using a novel cautery-tipped stent delivery system. Gastrointest Endosc 80:1171
Walter D, Will U, Sanchez-Yague A, Brenke D, Hampe J, Wollny H, López-Jamar JM, Jechart G, Vilmann P, Gornals JB, Ullrich S, Fähndrich M, de Tejada AH, Junquera F, Gonzalez-Huix F, Siersema PD, Vleggaar FP (2015) A novel lumen-apposing metal stent for endoscopic ultrasound-guided drainage of pancreatic fluid collections: a prospective cohort study. Endoscopy 47:63–67
Galasso D, Baron TH, Attili F, Zachariah K, Costamagna G, Larghi A (2015) Endoscopic ultrasound-guided drainage and necrosectomy of walled-off pancreatic necrosis using a metal stent with an electrocautery-enhanced delivery system. Endoscopy 47(Suppl 1):E68
Shah RJ, Shah JN, Waxman I, Kowalski TE, Sanchez-Yague A, Nieto J, Brauer BC, Gaidhane M, Kahaleh M (2015) Safety and efficacy of endoscopic ultrasound-guided drainage of pancreatic fluid collections with lumen-apposing covered self-expanding metal stents. Clin Gastroenterol Hepatol 13:747–752
Rinninella E, Kunda R, Dollhopf M, Sanchez-Yague A, Will U, Tarantino I, Gornals Soler J, Ullrich S, Meining A, Esteban JM, Enz T, Vanbiervliet G, Vleggaar F, Attili F, Larghi A (2015) EUS-guided drainage of pancreatic fluid collections using a novel lumen-apposing metal stent on an electrocautery enhanced delivery system: a large retrospective study. Gastrointest Endosc 82:1039–1046
Walter D, Teoh AY, Itoi T, Pérez-Miranda M, Larghi A, Sanchez-Yague A, Siersema PD, Vleggaar FP (2016) EUS-guided gallbladder drainage with a lumen-apposing metal stent: a prospective long-term evaluation. Gut 65:6–8
Tarantino I, Barresi L, Granata A, Ligresti D, Curcio G, Traina M (2015) Single-step EUS-guided choledocoduodenostomy and stenting. Gastrointest Endosc 81:1016–1017
Rimbas M, Attili F, Larghi A (2015) Single-session EUS-guided FNA and biliary drainage with use of a biflanged lumen-apposing stent on an electrocautery enhanced delivery system: 1-stop shop for unresectable pancreatic mass with duodenal obstruction. Gastrointest Endosc 2:405
Artifon EL, Aparicio D, Paione JB, Lo SK, Bordini A, Rabello C, Otoch JP, Gupta K (2012) Biliary drainage in patients with unresectable, malignant obstruction where ERCP fails: endoscopic ultrasonography-guided choledochoduodenostomy versus percutaneous drainage. J Clin Gastroenterol 46:768–774
Khashab MA, Valeshabad AK, Afghani E, Singh VK, Kumbhari V, Messallam A, Saxena P, El Zein M, Lennon AM, Canto MI, Kalloo AN (2015) A comparative evaluation of EUS-guided biliary drainage and percutaneous drainage in patients with distal malignant biliary obstruction and failed ERCP. Dig Dis Sci 60:557–565
Dhir V, Artifon EL, Gupta K, Vila JJ, Maselli R, Frazao M, Maydeo A (2014) Multicenter study on endoscopic ultrasound-guided expandable biliary metal stent placement: choice of access route, direction of stent insertion, and drainage route. Dig Endosc 26:430–435
Park do H, Jeong SU, Lee BU, Lee SS, Seo DW, Lee SK, Kim MH (2013) Prospective evaluation of a treatment algorithm with enhanced guidewire manipulation protocol for EUS-guided biliary drainage after failed ERCP (with video). Gastrointest Endosc 78:91–101
Nguyen-Tang T, Binmoeller KF, Sanchez-Yague A, Shah JN (2010) Endoscopic ultrasound (EUS)-guided transhepatic anterograde self-expandable metal stent (SEMS) placement across malignant biliary obstruction. Endoscopy 42:232–236
Artifon EL, Safatle-Ribeiro AV, Ferreira FC, Poli-de-Figueiredo L, Rasslan S, Carnevale F, Otoch JP, Sakai P, Kahaleh M (2011) EUS-guided antegrade transhepatic placement of a self-expandable metal stent in hepatico-jejunal anastomosis. JOP 12:610–613
Wang K, Zhu J, Xing L, Wang Y, Jin Z, Li Z (2015) Assessment of efficacy and safety of EUS-guided biliary drainage: a systematic review. Gastrointest Endosc. doi:10.1016/j.gie.2015.10.033 [Epub ahead of print]
Khashab MA, Valeshabad AK, Modayil R, Widmer J, Saxena P, Idrees M, Iqbal S, Kalloo AN, Stavropoulos SN (2013) EUS-guided biliary drainage by using a standardized approach for malignant biliary obstruction: rendezvous versus direct transluminal techniques (with videos). Gastrointest Endosc 78:734–741
Wang AY, Ellen K, Berg CL, Schmitt TM, Kahaleh M (2009) Fully covered self-expandable metallic stents in the management of complex biliary leaks: preliminary data—a case series. Endoscopy 41:781–786
Artifon EL, Marson FP, Gaidhane M, Kahaleh M, Otoch JP (2015) Hepaticogastrostomy or choledochoduodenostomy for distal malignant biliary obstruction after failed ERCP: is there any difference? Gastrointest Endosc 81:950–959
Leppard WM, Shary TM, Adams DB, Morgan KA (2011) Choledochoduodenostomy: is it really so bad? J Gastrointest Surg 15:754–757
Demirel BT, Kekilli M, Onal IK, Parlak E, Disibeyaz S, Kacar S, Kilic ZM, Sasmaz N, Sahin B (2011) ERCP experience in patients with choledochoduodenostomy: diagnostic findings and therapeutic management. Surg Endosc 25:1043–1047
Baker AR, Neoptolemos JP, Leese T, Fossard DP (1987) Choledochoduodenostomy, transduodenal sphincteroplasty and sphincterotomy for calculi of the common bile duct. Surg Gynecol Obstet 164:245–251
Baker AR, Neoptolemos JP, Carr-Locke DL, Fossard DP (1985) Sump syndrome following choledochoduodenostomy and its endoscopic treatment. Br J Surg 72:433–435
Disclosures
Dr. Rastislav Kunda is a consultant/speaker for Boston Scientific Corp. and for Olympus Medical. Dr. Manuel Pérez-Miranda is a consultant/speaker for Boston Scientific Corp., Xlumena and Gore. Dr. Alberto Larghi is a consultant/speaker for Cook Medical, Boston Scientific Corp., Covidien and Xlumena. Dr. Uwe Will, Dr. Sebastian Ullrich, Dr. Markus Dollhopf and Dr. Michelle Meier have no conflicts of interest or financial ties to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Kunda, R., Pérez-Miranda, M., Will, U. et al. EUS-guided choledochoduodenostomy for malignant distal biliary obstruction using a lumen-apposing fully covered metal stent after failed ERCP. Surg Endosc 30, 5002–5008 (2016). https://doi.org/10.1007/s00464-016-4845-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-016-4845-6