
Abstract
Objective
This study aimed to evaluate the long-term efficacy of peroral endoscopic myotomy (POEM) for patients with achalasia.
Methods
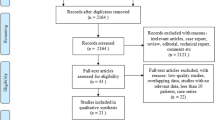
Prospective data collected from 115 patients (median age 45 years; interquartile range 34–57) with achalasia who underwent POEM at the First Affiliated Hospital of ZheJiang Chinese Medical University with a median follow-up of 36 months were retrospectively analyzed. The Eckardt score and lower esophageal sphincter pressure changes were analyzed, and the gastroesophageal reflux was observed.
Results
During the final follow-up, the mean Eckardt score reduced from 7.5 ± 1.9 preoperatively to 2.3 ± 1.4 after 1 month of surgery (P < 0.001). Treatment success was observed in 91.3% [confidence interval (CI) 86.2–96.4], 90.3% (CI 84.8–95.8), 89.0% (CI 83.1–94.9), 83.7% (CI 75.7–91.7), and 80.1% (CI 69.7–90.5) of patients after 12, 24, 36, 48, and 60 months, respectively. A total of 16 (13.9%) failures occurred. Four patients were nonresponders (failure within 3 months), eight had an early recurrence (between 3 months and 3 years), and four had a late recurrence (after 3 years). Further, 21 (20.6%) patients had symptoms of reflux during the two-year follow-up. Only one patient with symptomatic reflux was newly added during the subsequent three-year follow-up. Moreover, 71 (61.7%) patients underwent gastroscopy after POEM, and 13 (18.3%) patients were diagnosed with reflux esophagitis.
Conclusion
POEM is safe and effective in treating achalasia and has a favorable long-term efficacy.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Achalasia is a rare primary esophageal motility disorder characterized by the dysfunction of the lower esophageal sphincter (LES) and the absence of peristalsis in response to swallowing [1]. Hence, the treatment of achalasia involves mainly a reduction in the LES gradient pressure, thereby alleviating the symptoms [2]. Advances in endoscopic techniques, which are even less invasive, have led to a novel endoscopic procedure named peroral endoscopic myotomy (POEM). POEM was first described by Pasricha et al. [3]. in a porcine model based on submucosal endoscopy and endoscopic myotomy. However, it was not applied to treat patients successfully until 2009 [4]. Subsequently, the technique was modified by Inoue [5] and performed in patients with achalasia. The developmental history of POEM is relatively short compared with the traditional treatment of achalasia. Many studies [6,7,8,9,10] demonstrated that POEM was a safe and highly effective treatment for achalasia. A prior study [11, 12] by our center also demonstrated the excellent short-term safety and efficacy of POEM for treating achalasia. At present, the follow-up time of most studies on POEM is relatively short, and a recent systematic review [13] reported a median follow-up of 13 months (range 3–24). The present study aimed to assess the long-term efficacy of POEM in patients with achalasia using the Eckardt score [14], endoscopy, and high-resolution manometry (HRM). The aforementioned aspects provided an objective understanding of POEM and helped evaluate its long-term efficacy accurately.
Methods
Subjects
This study retrospectively analyzed the data collected prospectively from a single center. A total of 115 consecutive patients with achalasia treated using POEM in the First Affiliated Hospital of ZheJiang Chinese Medical University were recruited from January 2012 to May 2017. Achalasia was diagnosed on the basis of clinical symptoms, barium esophagogram examination, and esophageal HRM. The included patients agreed for POEM treatment and follow-up visits. The exclusion criteria were as follows: patients with diffuse esophageal spasm, jackhammer and nutcracker esophagus, and secondary achalasia. Patients who withdrew informed consent were also excluded. A previous treatment failure, including botulinum toxin injection, endoscopic balloon dilation, or laparoscopic Heller’s myotomy (LHM), was not considered a criterion for exclusion. Clinical data were extracted for all patients, including Eckardt scores, manometric data before or after therapy for achalasia, data related to POEM procedures, procedure-related adverse events, post-procedural reflux symptoms, and results of upper endoscopy. The study was approved by the Institutional Medical Ethics Committee at the First Affiliated Hospital of ZheJiang Chinese Medical University (approval number: 2012-x-003).
POEM Technique
POEM procedures were performed by Dr. B Lu as described by Inoue et al. [5]. In brief, the patients were administered intravenous anesthesia and CO2 insufflation. An upper gastrointestinal endoscope was attached with a transparent distal cap. First, indigo carmine with saline was injected to expand the submucosal space on the anterior or posterior wall of the mid-esophagus, about 12 cm above the esophagogastric junction (EGJ). Subsequently, a 1.5- to 2-cm mucosal incision was made to enter the submucosal space using a triangular-tip knife (KD-640L, Olympus, Tokyo, Japan). Second, the submucosal space was dissected to create a submucosal tunnel extending to the LES and across the EGJ, 2 or 3 cm into the proximal stomach. The myotomy of muscle fibers was started about 2 cm below the tunnel entry and extended 2–3 cm into the gastric cardia. Finally, the mucosal incision was closed using endoscopic clips (HX-610-090L, Olympus, Tokyo, Japan).
HRM
HRM was performed using a 36-channel solid-state catheter (ManoScan-360 HRM, Sierra Scientific Instruments Inc., CA, USA). Before the examination, all the patients were fasted for at least 8 h, and the prokinetic medications were disabled for more than 5 days. After administering local anesthesia, the catheter was advanced through the nasal canal and subsequently fixed in the correct position. The upper esophageal sphincter and LES resting pressure were recorded after adapting to the catheter for 5 min. All patients were investigated in a supine position with 10 swallows of water (10 × 5 mL). Manometric data were acquired and analyzed using the dedicated ManoView analysis software version 2.0.1 (Sierra Scientific Instruments Inc., CA, USA).
Eckardt Symptom Score
Achalasia-related symptoms were preoperatively and postoperatively assessed using the Eckardt score. The Eckardt score is the sum of the achalasia-related symptom scores for dysphagia, regurgitation, chest pain, and weight loss, which is used to assess achalasia symptom severity and treatment effectiveness. The higher the score, the greater the severity of the symptoms. The score also helps to determine the therapeutic effect [15] (Table 1).
Follow-Up and Outcome Measurements
After 1 month of the procedure, the patients were scheduled for HRM to re-examine esophageal motility and patency of the EGJ. Follow-up upper endoscopy was performed 2 months postoperatively to examine the healing of the wound and evaluate the reflux esophagitis. Data were obtained according to the actual situation of each patient thereafter. The Eckardt symptom scoring system was used to evaluate the therapeutic effects of POEM, which was repeated 1, 6, and 12 months after POEM and annually thereafter. A successful outcome was defined as a reduction in the Eckardt score to 3 or less [16]. Those with Eckardt score > 3 were grouped according to the time of the failure: within 3 months (nonresponders), between 3 months and 3 years (early recurrence), and after 3 years (late recurrence) [17]. Symptom relief was considered as the primary outcome. HRM was recommended to be done at least once preoperatively and postoperatively. Some HRM metrics, such as LES pressure, 4-s integrated relaxation pressure (IRP), symptom recurrence, and clinical reflux adverse events, were regarded as secondary outcomes. The gastroesophageal reflux disease questionnaires (GerdQ) were applied to evaluate the symptomatic reflux of the patients after POEM.
Statistical Analyses
SPSS statistical software (SPSS 19.0, IL, USA) was used to analyze experimental data. The measurement data were expressed as mean ± standard deviation and analyzed using the t test, and the count data were expressed as a ratio. The nonnormally distributed data were expressed as medians with interquartile ranges and analyzed using a nonparametric statistical test. Categorical data between proportions were compared using the Chi-square test. The long-term clinical success rate was estimated and graphed using the Kaplan–Meier survivor function. The logistic regression analysis was used to evaluate independent risk factors for clinical recurrence and reflux esophagitis. A P value < 0.05 indicated a statistically significant difference.
Results
General Information
A total of 115 patients [median age 45 years; interquartile range (IQR) 34–57 years; 51.3% males and 48.7% females)] were included in this study. The median duration of symptoms was 5 years (range 0.17–40 years). A total of 97 (84.3%) patients underwent HRM examination. The patients were classified as type I (16 patients, 16.5%), type II (71 patients, 73.2%), and type III (10 patients, 10.3%) according to the Chicago classification system [18]. Among 115 patients, 20 (17.4%) had received treatment before POEM; however, their clinical symptoms did not improve, or recurrence occurred after a short period of remission. Of these, 16 patients (13.9%) had received pneumatic dilation (PD) at least once, two patients (1.7%) had received a botulinum toxin injection, and two patients (1.7%) had undergone LHM (Table 2).
Procedure-Related Outcomes
All patients completed the POEM successfully. The mean length of myotomy was 11.1 ± 2.5 cm in type III achalasia and 11.0 ± 2.3 cm in types I and II achalasia. Posterior myotomy was performed in most patients (88.7%). Complications related to POEM were observed in nine patients (7.8%): two (1.7%) with pneumothorax or pneumomediastinum, three (2.6%) with pleural effusion, and four (3.5%) with fever. No intraoperative or delayed bleeding was observed in any of the patients during the follow-up. One patient underwent thoracic close drainage due to pleural effusion. The other complications were successfully managed conservatively (Table 3).
Clinical Outcomes After POEM
The median follow-up after POEM was 36 months (IQR 24–48). The overall success rate was achieved in 91.3% (CI 86.2–96.4), 90.3% (CI 84.8–95.8), 89.0% (CI 83.1–94.9), 83.7% (CI 75.7–91.7), and 80.1% (CI 69.7–90.5) of patients after 12, 24, 36, 48, and 60 months, respectively (Fig. 1). A significant reduction in symptoms was achieved, with the preoperative Eckardt score decreasing from 7.5 ± 1.9 preoperatively to 0.7 ± 1.1 after 1 month. A significant symptom reduction continued with a postoperative Eckardt score of 2.3 ± 1.4 (P < 0.001) during the last visit. Esophageal manometry data were available from 97 patients. The mean LES pressure and 4-s IRP decreased from 33.6 ± 15.5 to 16.4 ± 6.6 mm Hg (P < 0.001) and 27.4 ± 11.5 to 13.2 ± 6.6 mm Hg (P < 0.001), respectively, 1 month after POEM. The mean LES pressure and 4-s IRP pressure decreased during the 2-year follow-up from 33.6 ± 15.5 to 18.7 ± 6.3 mm Hg (P < 0.001) and 27.4 ± 11.5 to 14.4 ± 6.5 mm Hg (P < 0.001), respectively (Table 4).

Treatment success calculated using Kaplan–Meier analysis
POEM Failures
A total of 16 POEM failures, including one patient with type I achalasia, nine with type II achalasia, two with type III achalasia, and four unclassified, occurred during the study period. The success rate of treatment for types I, II, and III achalasia was 93.8, 87.3, and 80% (P = 0.568), respectively, during the five-year follow-up. One patient with type II achalasia was a nonresponder who had persistent symptoms after POEM with an Eckardt score of 7. Three patients (including one type II achalasia, one type III, and one unclassified) had improved symptoms after POEM, but the Eckardt score did not fall to 3 and less. Further, eight patients (including one type I achalasia, five type II, one type III, and one unclassified) experienced a symptomatic relapse between 3 and 36 months, and four patients (including two type II achalasia and two unclassified) experienced symptom recurrence after 3 years. The postoperative Eckardt scores of patients with POEM failure (Eckardt score > 3) decreased from 7.8 ± 2.2 preoperatively to 4.7 ± 0.9 (P < 0.001) after surgery. Of the patients with POEM failure, three patients did not receive any interventional treatment and chose an ongoing follow-up. The remaining 13 patients received one more treatment. PD was the first choice to treat the disease. Moreover, three of them experienced a symptomatic relapse after PD, and the re-POEM procedure was successful in two of three patients with complete symptom relief. The other one of the three patients received re-PD successfully. A myotomy length above EGJ ≤ 8 cm [odds ratio (OR) 0.279; 95% CI 0.081–0.962] and prior interventional treatments (OR 0.287; 95% CI 0.083–0.994) were independently related to a lower chance of nonrecurrence (Table 5).
Postoperative Reflux
Symptomatic reflux occurred in 11 patients (9.6%) after 1 month, in 19 patients (16.5%) after 12 months, and in 21 patients (20.6%) after 24 months of follow-up. Only one patient with symptomatic reflux was newly added during the subsequent 3-year follow-up. Of the 22 patients evaluated for symptomatic reflux, eight experienced reflux symptoms every day and 14 occasionally. Upper endoscopy was available in 71 patients (61.7%) 2 months after POEM. All patients were found to have a small scar at the mucosal incision without esophageal stenosis. Also, 13 of 71 patients (18.3%) had endoscopic findings of reflux esophagitis (eight with grade A and five with grade B according to the Los Angeles classification). Of the 22 (19.1%) patients who complained of gastroesophageal reflux disease (GERD) symptoms such as heartburn or regurgitation, 11 (50%) were confirmed to have reflux esophagitis using endoscopy. Combining both symptomatic reflux and reflux esophagitis, a clinical reflux occurred in 24 patients (20.9%).
Proton pump inhibitors (PPIs) are commonly used to treat postoperative reflux symptoms. The efficacy of PPIs was evaluated by asking patients for subjective symptoms at follow-up. Of the 22 patients evaluated for symptomatic reflux, 14 were easily controlled by intermittent medication with standard doses of PPIs. Four patients needed to take standard doses of PPIs daily. Two patients did not take PPIs and were further observed. No reflux-related post-POEM stricture requiring interventional treatments was confirmed. The logistic regression analysis did not reveal age, gender, achalasia subtypes, prior interventional treatments, baseline Eckardt score, full-thickness myotomy, and length of myotomy associated with the development of post-POEM esophagitis.
Learning Curve
Learning curve was defined as first 18 cases [19]. Days of hospitalization, length of muscle incision, and duration of surgery were chosen for comparing the first 18 patients and the last 18 patients. The length of the procedure was considered statistically different between the two groups (patients 1–18 and patients 19–36). In addition, three POEM failures occurred in the first 18 patients and one in the last 18 patients. No significant difference (P = 0.3) in the cumulative rates of clinical failure of the first 18 POEM procedures versus a small group of the last 18 POEM procedures was detected (Table 6).
Discussion
POEM has been reported as a novel and effective therapy for achalasia in the short term. Its long-term outcomes require further follow-up. After 5 years, the treatment success rate decreased to 80.1%, suggesting that the clinical efficacy might decrease with time. Similarly, Werner et al. [20] included 80 patients with achalasia and followed them up for at least 2 years. The initial clinical success rate was found to be 96.3%, but clinical recurrence was noted in further 14 patients (17.7%) during the long-term follow-up. Inoue et al. [8] reported a decrease in success rate from 91% after 2 months to 88.5% after 3 years of POEM in 500 consecutive patients. Another international multicenter study [21] analyzed data from 10 centers and reported a decrease in the success rate from 98% in 6 months to 91% after 2 years. Li et al. [17] demonstrated a decrease in the success rate from 94.2% in 12 months to 87.1% after 5 years. Further, the therapeutic success of POEM decreased over time. The long-term efficacy of Heller’s myotomy and PD also slightly decreased over time, similar to the POEM. The long-term efficacy of PD decreased from 86% after 2 years to 82% after 5 years, and the success rate of LHM decreased from 90% after 2 years to 84% after 5 years [16, 22]. In addition, the present study showed no difference in the POEM success rates (type I 93.8%, type II 87.3%, and type III 80.0%; P = 0.568) among different subtypes of achalasia during the 5-year follow-up. This could be in line with the findings of the study by Greene et al. [23], who observed no difference among the outcomes after myotomy in patients with these subtypes of achalasia. However, Guo et al. reported that POEM for type III achalasia might have more failures [9]. The number of type III achalasia was the least compared with types I and II achalasia. More cases are required to explore this issue.
Ngamruengphong et al. [21] reported that prior treatment with PD was associated with treatment failure. The present study also found that any type of prior interventional treatment (including botulinum toxin injection, balloon/bougie dilation, and Heller’s myotomy) was one of the risk factors for POEM failure. A previous study reported [24] that prior endoscopic or surgical interventions caused submucosal fibrosis, which changed the normal esophageal physiology, increased the difficulty, and affected the quality of POEM surgery. Further, a myotomy length above EGJ ≤ 8 cm was identified as another risk factor for POEM failures in the present study. Experts on Heller’s myotomy reported that incomplete myotomy was the most likely cause for treatment failure within 12 months [25, 26]. Similar to a study [17] conducted at another center in the country, a muscle incision length of EGJ > 8 cm was considered to be a more complete muscle incision length. Martinek Jan reported [19] that the endoscopist’s surgical skills reached a plateau after 18 clinical cases. In the present study, the cumulative rates of failures for the first 18 patients and the last 18 patients were not statistically significant. Only the procedure time was found to decrease with growing experience. The effect of the learning curve might not be responsible for POEM failures. In addition, the present study showed a significant decrease (preoperative 7.8 ± 2.2 vs postoperative 4.7 ± 0.9, P < 0.001) in the Eckardt score compared with their baseline even in patients considered to have failed POEM (Eckardt score > 3).
As POEM significantly reduced the 4-s IRP and LES pressure measurements 1 month after the surgery (13.2 ± 6.6 mm Hg vs 27.4 ± 11.5 mm Hg, P < 0.001; and 16.4 ± 6.6 mm Hg vs 33.6 ± 15.5 mm Hg, P < 0.001, respectively), Achalasia symptoms were alleviated in patients through the reduction of EGJ pressure accompanied by a significant reduction in the Eckardt score. In addition, the 4-s IRP and LES pressure scores did not increase significantly during the 2-year follow-up (14.4 ± 6.5 mm Hg vs 13.2 ± 6.6 mm Hg, P = 0.65; and 18.7 ± 6.3 mm Hg vs 16.4 ± 6.6 mm Hg, P = 0.09, respectively). However, a recent long-term study [27] on patients with type III achalasia showed an increase in IRP from a median of 10.3 mm Hg (3–18) 1 month after POEM to a median of 14.7 mm Hg (8–22) after 4 years. Unfortunately, a significant percentage of patients were unwilling to undergo HRM within the next 3 years of follow-up. Therefore, changes in HRM parameters could not be observed.
Previous studies reported that the post-POEM symptomatic reflux rate varied from 8.6 to 37%, and the endoscopic reflux esophagitis rate varied from 14.8 to 66% [7, 8, 20, 21, 28,29,30]. Therefore, it appeared that subjective symptoms were not a reliable indicator of postoperative reflux. In addition, most of these studies focused only on the short-term reflux symptoms in patients after POEM. In this study, the rate of reflux symptoms was approximately 20.6% during the 2-year follow-up. Only one patient with symptomatic reflux was newly added during the subsequent three-year follow-up. Reflux symptoms in most patients (19/22, 86.4%) appeared within 1 year after POEM. Reflux esophagitis was noted during the two-month follow-up after POEM in 18.3% of patients who underwent upper endoscopy. The results of gastroscopy examination did not fully correspond with the patient’s reflux symptoms. A recent meta-analysis [31] showed that reflux esophagitis caused by POEM was mostly of mild grade (LA-A and LA-B according to the LA classification). In the present study, esophagitis was classified to be of mild grade (11.3%, 8 of 71 findings in LA-A; 7.0%, 5 of 71 findings in LA-B). Although POEM caused reflux esophagitis, no severe esophagitis occurred in the present study. Some studies [32, 33] reported a clear association between GERD and higher body mass index (BMI). Different BMIs had an effect on the occurrence of postoperative gastroesophageal reflux. In the present study, the incidence of symptomatic reflux in patients after POEM was not high, which might be related to the low BMI of the patients. Symptomatic reflux was common after POEM, but most patients were easily controlled by intermittent medication using standard doses of PPIs.
The present study had several limitations. First, the study was carried out at a single center with a relatively small sample size. A larger sample is required for more accurate and meaningful data. Second, poor patient compliance during HRM examination and difficulties in accessing records from outside hospitals affected the results. Then, the 24-h pH measurement studies were not performed during the follow-up, which helped identify the actual rate of gastroesophageal reflux. In addition, more longitudinal endoscopy would be obligatory to make an accurate conclusion regarding the risks of reflux after POEM.
In the present study, some proportion of patients (15.7%) were diagnosed with achalasia through clinical symptoms and other ancillary examinations, although they did not receive esophageal manometry. These patients had typical symptoms such as dysphagia, weight loss, chest pain, and regurgitation with an Eckardt score > 3. Furthermore, their esophagography showed a typical bird’s beak aspect at the gastroesophageal junction and a large dilatation of the esophagus. Computed tomography scanning and endoscopy were used to exclude alternative pathology, principally pseudo-achalasia and/or other causes of obstruction. The Eckardt scores of these patients after POEM significantly declined (preoperative 6.0 ± 1.9 vs. postoperative 1.7 ± 1.8, P < 0.001).
In summary, the present study showed that POEM was an effective and safe endoscopic therapeutic method for patients with achalasia after a median follow-up of 36 months, relieving the symptoms and lowering the LES pressure. A significant improvement in symptoms compared with their baseline was observed even in patients considered to have POEM failure (Eckardt score > 3). A history of incomplete myotomy and interventional treatment was related to a lower chance of nonrecurrence of achalasia symptoms. The rate of reflux symptoms was approximately 20.6% during the two-year follow-up. Only one patient with symptomatic reflux was newly added during the subsequent three-year follow-up. Further, almost all patients with reflux symptoms after POEM were successfully treated with PPIs.
References
Boeckxstaens GE, Giovanni Z, Richter JE. Achalasia. Lancet. 2014;383:83–93.
Bello B, Herbella FA, Patti MG. Evolution of the minimally invasive treatment of esophageal achalasia. World J Surg. 2011;35:1442–1446.
Pasricha PJ, Hawari R, Ahmed I, et al. Submucosal endoscopic esophageal myotomy: a novel experimental approach for the treatment of achalasia. Endoscopy. 2007;39:761–764.
Perretta S, Dallemagne B, Allemann P, et al. Multimedia manuscript. Heller myotomy and intraluminal fundoplication: a NOTES technique. Surg Endosc. 2010;24:2904.
Inoue H, Minami H, Kobayashi Y, et al. Peroral endoscopic myotomy (POEM) for esophageal achalasia. Endoscopy. 2010;42:265–271.
Von Renteln D, Fuchs KH, Fockens P, et al. Peroral endoscopic myotomy for the treatment of achalasia: an international prospective multicenter study. Gastroenterology. 2013;145:309–311.
Ramchandani M, Nageshwar Reddy D, Darisetty S, et al. Peroral endoscopic myotomy for achalasia cardia: Treatment analysis and follow up of over 200 consecutive patients at a single center. Dig Endosc. 2016;28:19–26.
Inoue H, Sato H, Ikeda H, et al. Per-oral endoscopic myotomy: a series of 500 patients. J Am Coll Surg. 2015;221:256–264.
Guo H, Yang H, Zhang X, et al. Long-term outcomes of peroral endoscopic myotomy for patients with achalasia: a retrospective single-center study. Dis Esophagus. 2017;1:1–6.
Teitelbaum EN, Dunst CM, Reavis KM, et al. Clinical outcomes five years after POEM for treatment of primary esophageal motility disorders. Surg Endocr. 2018;32:421–427.
Bin L, Meng L, Yue H, et al. Effect of peroral esophageal myotomy for achalasia treatment: a Chinese study. World J Gastroenterol. 2015;21:5622–5629.
Hu Y, Li M, Lu B, et al. Esophageal motility after peroral endoscopic myotomy for achalasia. J Gastroenterol. 2016;51:458–464.
Crespin OM, Liu LWC, Parmar A, et al. Safety and efficacy of POEM for treatment of achalasia: a systematic review of the literature. Surg Endosc. 2017;31:2187–2201.
Eckardt VF. Clinical presentations and complications of achalasia. Gastrointest Endosc Clin N Am. 2001;11:281.
Eckardt VF, Aignherr C, Bernhard G. Predictors of outcome in patients with achalasia treated by pneumatic dilation. Gastroenterology. 1992;103:1732–1738.
Boeckxstaens GE, Annese V, des Varannes SB, et al. Pneumatic dilation versus laparoscopic Heller’s myotomy for idiopathic achalasia. N Engl J Med. 2011;364:1807–1816.
Li QL, Wu QN, Zhang XC, et al. Outcomes of per-oral endoscopic myotomy for treatment of esophageal achalasia with a median follow-up of 49 months. Gastrointest Endosc. 2018;87:1405–1412.
Herbella FA, Armijo PR, Patti MG. A pictorial presentation of 3.0 Chicago Classification for esophageal motility disorders. Einstein. 2016;14:439–442.
Jan M, Hana S, Zuzana V, et al. Per-oral endoscopic myotomy (POEM): mid-term efficacy and safety. Surg Endosc. 2018;32:1293–1302.
Werner YB, Costamagna G, Swanström LL, et al. Clinical response to peroral endoscopic myotomy in patients with idiopathic achalasia at a minimum follow-up of 2 years. Gut. 2015;65:899.
Ngamruengphong S, Inoue H, Chiu PW, et al. Long-term outcomes of per-oral endoscopic myotomy in patients with achalasia with a minimum follow-up of 2 years: an international multicenter study. Gastrointest Endosc. 2017;85:927.
Moonen A, Annese V, Belmans A, et al. Long-term results of the European achalasia trial: a multicentre randomised controlled trial comparing pneumatic dilation versus laparoscopic Heller myotomy. Gut. 2016;65:732.
Greene CL, Chang EJ, Oh DS, et al. High resolution manometry sub-classification of achalasia: does it really matter? Surg Endosc. 2015;29:1363.
Wu QN, Xu XY, Zhang XC, et al. Submucosal fibrosis in achalasia patients is a rare cause of aborted peroral endoscopic myotomy procedures. Endoscopy. 2017;49:736–744.
Zaninotto G, Costantini M, Rizzetto C, et al. Four hundred laparoscopic myotomies for esophageal achalasia. Ann Surg. 2008;248:986–993.
Patti MG, Molena D, Fisichella PM, et al. Laparoscopic Heller myotomy and Dor fundoplication for achalasia: analysis of successes and failures. Arch Surg. 2001;136:870–877.
Hernández OM, Martinez González MA, Blancas JV, et al. Long-term quality of life after peroral endoscopic myotomy remains compromised in patients with achalasia type III. Endoscopy. 2017;49:1209–1218.
Sharata AM, Dunst CM, Pescarus R, et al. Peroral endoscopic myotomy (POEM) for esophageal primary motility disorders: analysis of 100 consecutive patients. J Gastrointest Surg. 2015;19:161–170.
Shiwaku H, Inoue H, Yamashita K, et al. Peroral endoscopic myotomy for esophageal achalasia: outcomes of the first over 100 patients with short-term follow-up. Surg Endosc. 2016;30:4817–4826.
Ren Y, Tang X, Chen Y, et al. Pre-treatment Eckardt score is a simple factor for predicting one-year peroral endoscopic myotomy failure in patients with achalasia. Surg Endosc. 2017;31:3234–3241.
Repici A, Fuccio L, Maselli R, et al. Gastroesophageal reflux disease after per-oral endoscopic myotomy as compared with Heller’s myotomy with fundoplication: a systematic review with meta-analysis. Gastrointest Endosc. 2018;87:934–943.
Hajar N, Castell DO, Ghomrawi H, et al. Impedance pH confirms the relationship between GERD and BMI. Dig Dis Sci. 2012;57:1875–1879.
Viazis N, Karamanolis GP, Anastasiou J, et al. Refractory GERD: increased body mass index is associated with persisting acid exposure but not hypersensitive esophagus or functional heartburn. Eur J Gastroenterol Hepatol. 2013;25:1450–1455.
Acknowledgments
The authors thank Kejia Zhao and Xianjing Zhao for assisting in the preparation of this manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
The authors declare no conflicts of interest.
Rights and permissions
About this article

Cite this article
He, C., Li, M., Lu, B. et al. Long-Term Efficacy of Peroral Endoscopic Myotomy for Patients with Achalasia: Outcomes with a Median Follow-Up of 36 Months. Dig Dis Sci 64, 803–810 (2019). https://doi.org/10.1007/s10620-018-5373-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-018-5373-0