
Abstract
This study examined multiple determinants of discrepancies between mother and child reports of problem behavior. In 5,414 6-year-olds, child problem behavior was assessed by self-report using the Berkeley Puppet Interview and by maternal report using the Child Behavior Checklist. Patterns in mother–child reports were modeled using latent profile analysis. Four profiles, differing in problem level, and the direction and magnitude of mother–child discrepancies, were identified: one profile representing agreement (46 %), another representing slight discrepancies (30 %), and two representing higher problem levels and more discrepancies. In the latter two profiles either children (11 %) or mothers (13 %) reported more problems. Compared to the first profile, the second was predominantly characterized by a positive family environment, the third by child cognitive difficulties, and the fourth by harsh discipline and poor family functioning. Knowledge about specific child/family characteristics that contribute to mother–child discrepancies can help to interpret informants’ reports and to make diagnostic decisions.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The assessment of child emotional and behavioral problems often relies on the use of multiple informants. Information from several sources, such as parents, teachers, clinicians and the children themselves, provides a more accurate description of children’s problems [1]. Recently, instruments have become available to obtain structured self-reported information from children as young as 4 years old [2–4]. Hence, young children’s information can be included in studies that usually relied on adult information only, and multi-informant approaches can be applied from an early age onwards.
Although multi-informant approaches are a common practice, information obtained from multiple sources is often discrepant [5, 6]. A meta-analysis from Achenbach et al. [5] and more recent studies demonstrated that there is only little agreement across informants’ reports of problem behavior [6–8]. In addition, discrepancies between informants’ reports are found across the lifespan [9]. These discrepancies can influence how researchers and clinicians interpret information and may thus impact decision making in research and clinical practice [7, 10]. Consequently, discrepancies in informant reports have often been considered a nuisance and a problem of measurement error [10]. Yet, there can be useful information in the diverging reports of informants. Research has therefore aimed at identifying determinants of these discrepancies, as this may help to better value information of each individual informant.
Discrepancies can reflect the setting or context where information was obtained (e.g. home vs. non-home), as contextual fluctuations in the expression of children’s behavior may result in differing reports [5, 11]. In addition, discrepancies can reflect the underlying perspectives of informants about what is normal and abnormal behavior [5, 11, 12]. While both context and perspective may account for discrepancies, a recent review on the use of multi-informant reports encouraged researchers to focus on factors other than context when examining informant discrepancies [10]. Further, parents and young children are the focus of the present study, because parents (in particular mothers) are the most prominent informants about young children’s problem behavior. Parents and young children likely report largely about similar contexts.
Over the past decades research has identified several characteristics that may impact parents’ and children’s perspectives and that are associated with parent–child discrepancies. Among these are demographic and socioeconomic characteristics of families like children’s age, gender and family socioeconomic status [5, 13–16]; parental psychopathology, ranging from parental depression and anxiety to anger and hostility [15, 17–23]; and dysfunctional interactions between family members [24]. Specifically, problems in family functioning, parent–child conflict, or harsh discipline practices may influence family members’ perceptions of problem behavior [6, 13, 14, 25–27]. In contrast, child cognitive abilities have rarely been studied as determinants of informant discrepancies [28]. Differences in cognitive functioning may, however, determine the developing child’s ability to report on emotions and behavior.
A substantial number of characteristics have thus been studied in association with parent–child discrepancies, yet results remain inconclusive [11] and it is unclear which factors independently determine informant discrepancies. One reason for this gap is that most studies focused on single determinants of parent–child discrepancies, while only few tested the independent contribution of multiple determinants (e.g. [6, 20, 24, 25]). Further, studies that did test multiple determinants of parent–child discrepancies were generally conducted in relatively small samples or in samples of clinically referred children and their parents. Another gap in the existing literature is that most studies were performed in children from age 8 onwards. A number of recent studies did examine informant discrepancies in younger children [29–32]. However, given the paucity of methods to obtain young children’s self-reports, these studies focused on parent–teacher discrepancies. The studies showed that interrater agreement is also low when examining young (i.e. preschool) children’s problem behavior [29–31]. One study found that parent–teacher agreement appeared stronger when parents and teachers reported about the same context (e.g. school) [32]. In addition, family and parenting characteristics, such as parental stress level and family conflict, determined that parents reported more problems than teachers [29, 31]. Yet, none of these studies on informant discrepancies included the children’s own perspective of their problems. Kraemer et al. [1] were the first to include young children’s self-reports in a study related to the issue of informant discrepancies, but they used children’s information to illustrate a method on combining multi-informant reports. To the best of our knowledge, no study examined independent determinants explaining parent–child discrepancies in children younger than 8 years old.
The present study on informant discrepancies expands the age range of previous studies by focusing on children aged 5–7 years. Further, we examined the unique contribution of a wide range of determinants that may contribute to discrepancies between mother report and young child self-report.
Few validated instruments are available to systematically assess behavioral and emotional problems in children younger than 8 years, thus we could not obtain maternal information using different versions of the same instrument. Consequently, we examined patterns in the relative problem levels (z-scores) that mothers and children reported. Reporting patterns were obtained with latent profile analysis (LPA), which is a way to explore clusters of symptoms across informants. Previous studies have also used and recommended latent variable approaches in multi-informant studies [10, 25, 26, 33]. Our approach allowed us to examine the magnitude of discrepancies between a child’s and a mother’s relative problem level, the direction of discrepancies—i.e. whether the child or the mother reported more problems—[25], and the relative level of problems that mother and child reported. After obtaining these mother–child reporting profiles, we studied determinants of these profiles. Specific hypotheses regarding the associations could not be formed, given inconsistent results of prior research and the lack of studies examining determinants of discrepancies using young child self-reports. However, in general, we hypothesized that profiles with lager discrepancies and higher problem levels would be determined by problems in cognitive functioning of children, and by adverse socio-demographic and family related characteristics.
Methods
Design and Study Sample
This study was embedded in the Generation R Study, a population-based prospective cohort investigating growth, development and health from fetal life onward. The design and data collection procedures have previously been described in detail [34]. All children were born between April 2002 and January 2006 in Rotterdam, The Netherlands. Typically, enrolment took place in early pregnancy. The study was approved by the Medical Ethics Committee of Erasmus Medical Center, Rotterdam. Written informed consent was obtained from all caregivers.
Participants with consent for the study-phase from age 4 to 16 were eligible for the present study. Consent for this particular study phase was obtained from caregivers of 8,305 children that had all been followed since birth. Of the 8,305 children eligible for follow-up examinations, 6,690 children aged 5–7 years old (M = 6.1, SD = 0.04) visited, together with their caregiver, our research center at the Erasmus Medical Center–Sophia Children’s Hospital. During this visit child self-report of emotional and behavioral problems was obtained using the Berkeley Puppet Interview (BPI; n = 6,598). We excluded BPI data if coders had indicated that the child did not understand the interview, or if >25 % of the data was missing on all scales (n = 77). We also excluded data if only BPI and no parent reported Child Behavior Checklist (CBCL) data was available (n = 1,022) and if children were 8 years or older when either the BPI or the CBCL was completed (n = 85). This resulted in a sample for analysis of 5,414 (65 %) children.
Characteristics of participants that were included in the study (responders; n = 5,414), were compared with characteristic of participants with missing data on child or mother report (non-responders; n = 2,891). Among the non-responders, the average maternal age was lower (M1 = 28.80 and M2 = 31.07, t = −18.47 (5,254), p < .001). Non-responding mothers were more often of non-Western origin (51.8 vs. 32.2 %, χ 2 (1) = 280.6, p < .001) and lower educated (66.3 vs. 43.4 %, χ 2 (1) = 356.2, p < .001). No differences were detected in general maternal psychopathology scores (M1 = 3.70, M2 = 3.35, t = 1.59 (1,310), p = .113) or family income (26.1 vs. 23.1 %, χ2 (1) = 3.6, p = .059) between non-responders and responders.
Measures
Berkeley Puppet Interview—Child reported problem behavior was assessed with the Berkeley Puppet Interview, a semi-structured interactive interview to obtain self-reports from young children [35]. During the interview at the research center, two identical dog hand puppets, ‘Iggy’ and ‘Ziggy’, were introduced to the child and invited him or her to engage in conversation. The puppets made opposing statements about themselves and asked children to indicate which statement described him or her best. Afterwards, videotaped interviews were scored by trained coders on a 7-point scale ranging from 1 to 7. The exact score depended on which of the puppets’ statements the child chose and how much emphasis was put on the answer. Higher scores represented more problems. Items were summed to compute scale scores. We used the internalizing and externalizing scales. The internalizing scale (20 items) comprised the Depression, Separation Anxiety and Overanxious scales. The externalizing scale (21 items) comprised the Oppositional Defiant, Overt Hostility and Conduct Problems scales. A recent psychometric study of the BPI in the Generation R Study revealed that the interview has a multidimensional structure, acceptable internal consistencies, and that scores could be interpreted validly as shown by associations with socio-demographic factors [4].
Child Behavior Checklist 1½–5—Parent reported child emotional and behavioral problems were assessed with the Child Behavior Checklist for ages 1½–5 years (CBCL; 36). The primary caregiver completed the questionnaire at home, prior to the research center visit. As the majority (60 %) of the children were younger than 6 years old at the time of CBCL assessment (37 % were 6 years old and 3 % of the children were 7 years old), we used the CBCL 1½–5 version for all children during this assessment wave to enhance comparability across all children, as recommended in the ASEBA manual [36]. The primary caregiver rated the occurrence of their child’s behavior within the past 2 months on a scale from 0 (not true) to 2 (very true or often true). In 92 % of the sample the primary caregiver was the mother, therefore we refer to this report with the term ‘mother report’. A sensitivity analysis was performed using mother reported data only. Items were summed to compute scale scores, with higher scores representing more problems. We used the 36-item internalizing and 24-item externalizing scales. Good reliability and validity have been reported for the CBCL [36]. Internal consistencies of the internalizing and externalizing scales in the present study were α = .86 and α = .90, respectively. These internal consistencies were similar in children younger than 6 years and in children older than 6 years.
Determinants of informant discrepancies—The choice of potential determinants of discrepancies was based primarily on prior studies [11, 16, 24, 25]. Demographic and socioeconomic characteristics (maternal age at pregnancy, child age, child gender, siblings, maternal national origin, maternal education, marital status, and family income) were obtained from questionnaire data and medical records. Maternal age and child gender were obtained from medical records completed by midwives and gynecologists. Presence of siblings in the household, maternal national origin, maternal education, and family income were obtained by questionnaires filled out prior to the research center visit at the same time as the CBCL assessment. Maternal national origin was classified by the countries of birth of her parents, according to the Dutch standard classification criteria [37], and was categorized into “Dutch”, “other-Western” (i.e. other European, North-American and Oceania) and “non-Western” (i.e. Turkish, Moroccan, Indonesian, Cape Verdean, Surinamese and Antillean) national origin. Maternal education was defined as highest completed schooling and classified in three levels; “primary”, “secondary” or “higher” education. The mothers’ marital status was categorized as “married or cohabiting” and “single parenthood”. Family income, defined by the total net month income of the household, was categorized as “<1,200€ (social security level)”, “1,200–2,000€ (below modal)”, “2,000–4,000€ (above modal)” and “>4,000€ (two times above modal)” net income per month.
Parental psychopathology (depression, anxiety and hostility) was assessed using the Dutch version of the Brief Symptom Inventory (BSI); a validated self-report questionnaire which is widely used in clinical and research settings [38]. The BSI was completed by each parent when the child was 3 years old. The BSI originally consists of 53 items, in the present study we used the depression (6 items), anxiety (6 items) and hostility (5 items) subscales. Mothers and fathers rated the extent to which each item described their feelings in the past week according to a 5-point scale ranging from 0 (not at all) to 4 (extremely). We calculated a mean score on the subscales, with higher scores representing more problems (Cronbach’s alphas for mothers and fathers, respectively: depression α = .83 and α = .79; anxiety α = .75 and α = .63; hostility α = .62 and α = .60). Family and parenting factors that were considered were: family functioning and harsh discipline. Family functioning as perceived by the primary caregiver (in 92 % this was the mother) was measured at child age 6 years with the General Functioning scale of the McMasters Family Assessment Device (FAD: [39]), a validated 12-item self-report measure of family health and pathology. The primary caregiver rated how well each item described their family on a 4-point scale ranging from 1 (disagree strongly) to 4 (agree strongly). Sample items include “We cannot get along well with each other” and “There are a great many unpleasant, painful feelings in the family”. A mean score on the 12 items was calculated, with higher scores indicating more problems in family functioning (α = .89). Disciplinary styles of mothers and fathers were assessed using an adapted version of the Parent–Child Conflict Tactics Scale [40], when children were 3 years old. Parents rated their use of discipline during the past 2 weeks on a 6-point scale ranging from “never” to “five times or more”. The categories “twice”, “3 times”, “4 times”, and “5 times” were combined because of low prevalence rates. This resulted in a 3-point scale from 0 (never) to 2 (twice or more). In the Generation R Study, factor analysis of this adapted CTS-PC has identified a harsh discipline construct consisting of six items [41]. Items were included like “I shouted or screamed angrily at my child” and “I angrily pinched my child’s arm”. We calculated a harsh discipline sum score by summing the scores on the six ‘harsh discipline’ items (α = .57 for mothers and α = .55 for fathers). These modest Cronbach’s alphas reflect the small number of items in the scale, that in addition target a range of parental behaviors that do not necessarily co-occur [42].
Information on children’s cognitive abilities (IQ and verbal ability) was obtained during the research center visit. IQ was assessed using two subtests of a Dutch non-verbal IQ test: Snijders-Oomen Niet-verbale Intelligentie Test–Revisie (SON-R 2½–7: [43]). The two subsets used were ‘Mosaics’, which taps into spatial visualization abilities, and ‘Categories’, which assesses abstract reasoning abilities. The raw test scores were converted into non-verbal IQ using norms that were tailored to exact age [43]. The correlation of the IQ score derived by the mosaics and categories subsets and the IQ scores derived by the total test was high, r = .86 in an unrelated sample of 626 children aged 4½–7½ years (Tellegen, personal communication). To investigate language development in children, we assessed verbal ability with a receptive language subtest (syntax choice task) of a Dutch test battery [44]. A sum score on this subtest was calculated, with higher scores indicating better performance (α = .67).
Statistical Analysis
Baseline characteristics of the data were explored and Pearson’s correlation coefficients between BPI and CBCL internalizing and externalizing scale scores were calculated. Raw scores on the BPI and CBCL scales were transformed with inverse and square root transformations respectively, to achieve a more normal distribution of the data. The skewness of BPI and CBCL after the transformation was −0.16 and 0.23 for the internalizing scales, and 0.53 and −0.04 for the externalizing scales.
Next, z-scores of these transformed scale scores were computed. Z-scores have previously been used in multi-informant studies to compute a discrepancy measure, namely: ‘standardized difference scores’ (SDS’: subtracting the z-standardized scores of two informants [7]). While SDS’ provide a direct way to study discrepancies, results can be difficult to interpret. One single score represents the ratings from two different informants, thus information on the initial problem level that the informants reported is lost. Also, different problem levels can result in the same SDS. For example, if mother and child agreed that there were relatively many problems or if they agreed that there were none, this could both result in a SDS of 0, while these same SDS’ may well have different determinants. In the present study, we therefore used actual z-scores instead of a unidimensional discrepancy measure like SDS’.
To study determinants of informant discrepancies, data were analyzed in two steps. In the first step, patterns in mother and child report of problem behavior were modeled using latent profile analyses (LPA). Z-scores of the transformed internalizing and externalizing BPI and CBCL scale scores were used as indicators. LPA is a ‘person-centered’ method using continuous variables as indicators. The method attempts to identify profiles of individuals that show similar patterns across the indicators. A maximum likelihood estimator with robust standard errors was chosen to take into account any remaining skewness in the data. We started with a one profile model and increased the number of profiles until a parsimonious model with good model fit was reached. The best fitting model was determined by the sample size adjusted Bayesian Information Criterion (BIC), Akaikes Information Criteria (AIC), entropy, Vuong-Lo-Mendell-Rubin Likelihood Test (VLMRT) and the Bootstrapped Likelihood-Ratio Test (BLRT) [45]. Other relevant information such as interpretability and latent group size was also taken into account. Once the number of latent profiles was determined, each participant was assigned to the profile for which they had the highest assignment probability. LPA was conducted with Mplus version 6.2 [46].
In the second step, associations between potential determinants of discrepancies and the latent profiles were studied using multinomial regression analyses. We first examined univariate associations of demographic and socioeconomic characteristics, caregiver psychopathology, family and parenting factors, and cognitive abilities of the children with profile membership. Next, to study the independent contribution of each determinant, we added all determinants to a multinomial regression model. To facilitate the interpretation of the findings and to enhance comparability between the variables, the continuous measures of BSI, FAD, harsh discipline and language development were divided by their standard deviation (SD-scores). All regression analyses were performed in SPSS, version 20.0 (SPSS, Inc. Chicago, IL).
Missing values on the potential determinants of discrepancies were imputed using Multiple Imputation in SPSS 20.0. Missing values on these determinants ranged from < 0.01 % for gender, age and ethnicity to 14 % for verbal ability of the child (mean percentage missing data = 4.4 %). For logistical reasons, participants living in the south of Rotterdam were not approached for participation in the preschool period (0–4 years; n = 1,166). As a result, there was more missing data on information obtained by questionnaires in that period, i.e. parental psychopathology and harsh discipline: missing data ranged from 30 % for maternal harsh discipline to 43 % for paternal psychopathology. Imputed data were estimated using all predictors in the model, as well as mother, child and teacher reported problem behavior, and prenatal reports of psychopathology of both parents. Regression coefficients were averaged over twenty imputed datasets. To examine whether the imputation of missing data had influenced the results, analyses were repeated in the complete cases. In addition, analyses were repeated using only mother reports of child problem behavior, instead of primary caregiver reports.
In additional analyses, we examined whether discrepancies were not merely a result of potential biases in mothers’ reports, or of children’s inability to accurately report their problems. To address this issue, the discrepancy profiles were related to ratings of an external informant, in this case the teacher. Teacher reports of children’s problems were obtained using the validated Teacher Report Form [47]. This information was available in a subgroup of 3,102 participants, aged 6.8 years (SD = 2.7). The obtained profiles were associated with ratings of the teacher, using linear regression analysis. Demographic and socioeconomic characteristics, caregiver psychological problems, family and parenting factors, and cognitive abilities of the child were added as covariates.
Shared-method variance may have inflated results because the majority of the family and parenting measures were reported by mothers. We therefore performed additional analyses to examine whether an objective measure of parenting, namely observed maternal sensitivity, was associated with the discrepancy profiles. We used a maternal sensitivity measure obtained during a home visit when the child was 4 years old. This was the most recent assessment of maternal sensitivity. At the home visit, mother and child were asked to perform two interaction tasks that were too difficult for the child: building a tower and an etch-a-sketch task. The subsample and coding of the tasks was previously described in more detail [48]. Observed maternal sensitivity was available in a subgroup of 553 participants, aged 4.3 years (SD = 0.1) and was included as a determinant in nominal regression analyses, adjusted for demographic and socioeconomic covariates.
Results
Baseline characteristics of the children and their mothers are presented in Table 1. The majority of mothers were of Dutch national origin (60 %), their mean age was 31 years (SD = 4.9). About 43 % of the mothers had a medium or low education, and 23 % of the families had a household income below modal.
Pearson’s correlation coefficients between child self-report on the BPI and maternal report on the CBCL were low, but highly significant; internalizing r = .14, p < .001; externalizing r = .19, p < .001 (see also [4]).
The model fit for the LPA solutions for one to five profiles is shown in Table 2. Although BIC and AIC still decreased from a four to a five profile solution, the VLMRT pointed towards four profiles as best solution. Also, this four profile solution resulted in distinct and interpretable profiles.
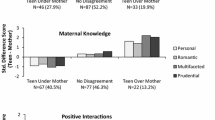
The four profile solution is graphically represented in Fig. 1. The profiles that we identified could be distinguished by three features: (1) the relative level of problems, (2) the magnitude of discrepancies and (3) the direction of the discrepancies, indicating whether the child or the mother reported more problems. The first and largest profile (n = 2,474; 46 %) was characterized by agreement. Children and mothers both reported an average relative problem level (both had z-scores of about 0), although mothers mostly reported a slightly higher problem level than their children. This profile was labeled ‘Child = Mother’. The second profile (n = 1,634; 30 %) was characterized by slight discrepancies, children represented in this profile reported an average relative problem level (z-scores of about 0), while mothers reported a lower relative problem level (negative z-scores). Overall, the lowest problem levels were reported in this second profile. We labeled this profile ‘Child > Mother’. The third and fourth profiles were characterized by higher relative problem levels and more discrepancies. The direction of discrepancies in these profiles differed. Characteristic for the third profile (n = 614; 11 %) was that children reported a higher relative problem level than mothers (child z-scores ≥1 SD; mother z-scores about 0). Children represented in this third profile reported particularly high levels of externalizing problems (≥1.5 SD), and lower, albeit still high, levels of internalizing problems (≈1 SD). This profile was labeled ‘Child ≫ Mother’. Characteristic for the fourth profile (n = 692; 13 %) was that children reported an average relative problem level, while mothers reported a higher relative problem level (child z-scores about 0, mother z-scores > 1), this profile was labeled ‘Child ≪ Mother’.

Reporting patterns within each latent profile
As discussed above, we considered the four profile solution to fit the data best. No distinct profile was found where mothers and children both reported a high level of problems. The mother–child dyads agreeing that relative problem levels were high (both ≥ 1 SD), were mostly found in the third and fourth profiles: 69 % of the mother–child dyads that agreed on a high level of internalizing problems were found in the fourth profile, 16 % in the third profile. Also, 57 % of the mother–child dyads that agreed on a high level of externalizing problems were in the fourth and 42 % in the third profile.
Next, the determinants of profile membership were examined. We studied unadjusted associations of potential determinants with profile membership and also the independent contribution of each of these determinants in a multivariate multinomial regression. The profile with most members (‘Child = Mother’) was chosen as reference group in the multinomial regressions, this was also the profile with most agreement between child and mother.
The results for the univariate multinomial regressions are presented in supplementary material (Table S1). Briefly, most determinants were associated with membership of one or more of the profiles. As compared to the reference group, more favorable determinants characterized the ‘Child > Mother’ profile. In contrast, more adverse determinants were associated with the ‘Child ≫ Mother’ and ‘Child ≪ Mother’ profiles.
In Table 3, results from the multivariate multinomial logistic regression are shown. All profiles were compared to the reference group ‘Child = Mother’. In the multivariate analysis many associations observed in the univariate analyses were attenuated and the pattern of associations for each profile became more distinct. First, we discuss determinants of the ‘Child > Mother’ profile. Mothers assigned to this profile were on average older at childbirth (OR = 1.02, p < .05), children were more likely to be a girl (OR boy = 0.86, p < .05) and to have siblings (OR no siblings = 0.78, p < .05). Parental psychopathology was not associated with membership of this profile, as was the case in most of the other profiles. Problems in family functioning and harsh discipline were less likely in members of this profile (OR FAD = 0.71, p < .001; OR HD-mother = 0.77, p < .001; OR HD-father = 0.89, p < .05). Further, cognitive abilities of children within this group were no different from those of children in the reference group.
Then, we examined determinants of the two profiles with larger mother–child reporting discrepancies: the ‘Child ≫ Mother’ and ‘Child ≪ Mother’ profiles. Children assigned to the ‘Child ≫ Mother’ profile were more often boys than girls (OR = 1.99, p < .001). Fathers of children assigned to this profile had reported higher levels of harsh discipline (OR = 1.15, p < .05). Most salient was that child cognitive abilities determined membership of this profile; children were more likely to have a lower IQ and poor performance on a receptive language task (OR IQ = 0.98, p < .001; OR language = 0.81, p < .001).
Finally, children assigned to the ‘Child ≪ Mother’ profile were more often boys than girls (OR = 1.50; p < .001). Mothers had more often a lower level of education (OR low = 1.63, p < .05) and they reported higher levels of anxiety (OR = 1.15; p < .05). In addition, problems in family functioning and harsh discipline were more likely in members of this profile (OR FAD = 1.38, p < .001; OR HD -mother = 1.16, p < .01; OR HD-father = 1.15, p < .05). We also found that children in this group were more likely to have a lower IQ than children in the reference group (OR = 0.99, p < .01).
Results from the multinomial logistic regressions with imputed data were compared to results obtained with the original, non-imputed, data. Results were essentially unchanged, with the exception that there was an effect of ethnicity in the original data that was not present in the imputed data. All analyses were also repeated using mother reported child problem behavior data only, instead of primary caregiver data. Results for these analyses were largely similar, with the difference that the effect of maternal anxiety in the ‘Child ≪ Mother’ profile disappeared.
Additional analyses using teacher reported child problems showed that children in the ‘Child > Mother’ profile had less internalizing and less externalizing problems according to teachers (B = −0.24, 95 % CI = −0.34;−0.15, p < .001 and B = −0.13, 95 % CI = −0.24;−0.03, p < .05) than in the reference profile (‘Child = Mother’). Conversely, children in the ‘Child ≪ Mother’ profile had more teacher reported internalizing and externalizing problems than children in the reference profile (B = 0.19, 95 % CI = 0.06; 0.33, p < .01 and B = 0.39, 95 % CI = 0.24; 0.53, p < .001), which is consistent with the high problem level mothers reported. According to teacher ratings, children classified in the ‘Child ≫ Mother’ profile had more externalizing problems (B = .41; 95 % CI = 0.26;0.56, p < .001), but not more internalizing problems than children in the reference profile. This specific association with externalizing problems was consistent with the children’s own report. Thus, if either mother or child reported a higher problem level, these problems were, on average, also apparent for teachers.
Additional analyses in a subgroup of 553 mothers and their children indicated that higher levels of observed maternal sensitivity were more common in the ‘Child > Mother’ profile (n = 184, mean sensitivity z-score = 0.19 versus mean sensitivity z-score = −0.08 in the ‘Child = Mother’ profile (n = 269), OR = 1.13, 95 % CI = 1.06; 1.58, p < .01). Observed maternal sensitivity was not associated with membership in any of the profiles (with fewer participants) representing more discrepancies, but associations were in the expected direction (‘Child ≫ Mother’, mean = −0.11, OR = 0.95, 95 % CI = 0.70; 1.28, n = 56; ‘Child ≪ Mother’, mean = −0.23, OR = 0.82, 95 % CI = 0.58; 1.15, n = 43).
Discussion
In this large population-based sample we examined independent determinants of discrepancies between maternal and young children’s self-report of problem behavior. To this aim we first identified patterns within the problem behavior reports of mothers and their children. Child-related characteristics, and in particular cognitive difficulties, predicted that children reported more problems than their mothers. In contrast, adverse family and parenting characteristics were the most salient correlates of a group in which mothers reported more problems than their children.
Determinants of mother–child reporting discrepancies
We examined mother–child reporting discrepancies by modeling patterns in mother and child reports of problem behavior using latent profile analysis and used actual informant scores instead of a unidimensional discrepancy measure. Four profiles, combining mothers’ and children’s reports, were identified that could be distinguished by the magnitude and the direction of discrepancies, and by the relative level of child problem behaviors.
Multiple factors were independently related to each of these profiles. Mothers with lower educational levels generally reported more problems than their children. Further, higher maternal age (which is a proxy for higher socio-economic status in the Netherlands) and the presence of a sibling in the household were associated with a group of mothers that reported less problems than their children. The presence of another child in the family may raise the threshold for mothers to consider her child’s behavior as problematic.
Also, the boy–girl ratio differed between each of the profiles. If the child was a girl, problem scores were generally lower and discrepancy between information from children and mothers was less common. In contrast, boys were more often found in the two groups characterized by more discrepancy. Interestingly, this association was independent of the direction of discrepancy. Previous studies yielded null or inconsistent findings regarding the effect of gender on informant discrepancies [5, 13, 14], which made De Los Reyes and Kazdin [11] suggest that child gender may not be related to informant discrepancies. The present findings suggest that gender determines the magnitude of discrepancy and the severity of problems reported, rather than the direction of discrepancy. Many previous studies were unable to distinguish between severity of problems, and the magnitude and direction of discrepancy in their analyses.
Parental psychopathology was—with the exception of a borderline significant effect of maternal anxiety—not related to mother–child reporting discrepancy in this study. This finding is not consistent with the view that parents with psychopathology overestimate their children’s problem behavior [14, 22, 49]. Only in univariate analyses did we observe that mothers with psychological problems consistently reported a higher level of problem behavior than their children. We discuss two explanations as to why we did not find a bias attributed to caregiver psychological problems. First, unlike most of the other determinants in this study, we measured parental psychological problems when the child was 3 years of age, instead of concurrent with the assessments of problem behavior. This time-lag may have influenced the effects we found for parental psychological problems as concurrent high levels of depressive symptoms may influence maternal reports of children’s problems more than depressive symptoms 3 years before. However, reporting tendencies of psychopathological symptoms—rather than specific disorders—are relatively stable across time. Also, previous research in the same cohort has shown that depressive symptoms in mothers were stable across 3 years’ time [50]. Nevertheless, the effects of depressive, anxiety and hostility symptoms on mother–child reporting discrepancies may have been underestimated in the present study as a consequence of the absence of concurrent measures of psychopathology. Second, we controlled the analyses for family functioning as it is strongly associated with parental psychopathology (e.g. [51–53]). Other studies that took the interdependency of depression and family functioning into account also reported no effect of parental psychological problems on informant discrepancies, or found that effects were greatly reduced [6, 25]. To some extent controlling for interdependent factors may be considered overadjustment. Family functioning and parental psychopathology are closely intertwined and may determine each other.
Family and parenting characteristics were independently associated with informant discrepancies. We found few mother–child reporting discrepancies in those families with less problems in family functioning, or low levels of harsh discipline. A stable family environment may support communication, mutual understanding [13], and a safe environment for children to disclose their feelings [26]. In contrast, more problems in family functioning and lower maternal education were associated with mothers reporting higher problem levels than their children. An unstable family environment may interfere with mothers’ ability to cope with a child’s behavior and may result in a low threshold for reporting problematic behavior [11]. Alternatively, children who grow up in a more problematic family environment, may not be used to expressing their feelings. Possibly, such children fear the consequences of disclosing emotional topics. Both processes may explain why more problems in family functioning were associated with a group of mothers that reported more problems than their children. Yet, alike parental psychopathology, parenting practices were assessed on average 3 years before the assessment of mother–child reporting discrepancies. Although parenting styles are moderately stable across time [54], effects may have been stronger if had assessment of parenting styles been concurrent.
When interpreting associations between parental psychopathology, family and parenting characteristics and informant discrepancies, it must be taken into account that (except for father reported variables) the mothers provided information on both the determinants and on one of the outcomes included in the discrepancy profiles. If one source provides information on both determinant and outcome, associations may be inflated due to shared-method variance [49]: some portion of the variance between the determinant and the outcome is likely to be shared as result of specific characteristics of the informant (e.g. the informants’ perspective on the world, test taking attitudes) rather than as a result of the specific determinant influencing the outcome [55]. However, the associations we found are unlikely to completely reflect such spurious inflations. First, maternal psychopathology was in general not associated with any of the discrepancy profiles. Second, harsh discipline reported by fathers and harsh discipline reported by the mother were similarly related to the discrepancy profiles. Third, associations between observed maternal sensitivity and mother–child reporting discrepancies further supported the validity of the analyses using maternal reported data: more observed maternal sensitivity was associated with a higher likelihood of being included in a profile in which mothers and children reported the lowest problem scores. Finally, more mother–child reporting discrepancies were related to higher teacher reported problem scores, indicating that if either mothers or children perceived problems, these were also apparent for an independent observer. These associations with teacher reported problems support the validity of our profiles.
Children with lower IQ and lower verbal ability were more likely to disagree with their mothers about problem behavior. Previous studies that have taken IQ into account did not find such a relation, however, these studies were all conducted in smaller clinical samples [15, 24, 28]. As a result of the smaller sample sizes, the power to detect an independent effect of IQ may have been limited. In addition, in the study by Penney and Skilling [28] there was little variance in the IQ range as most adolescents had a relatively low IQ. In the present study, child cognitive abilities were a determinant of membership in the two profiles with the largest mother–child reporting discrepancies. Interestingly, cognitive difficulties were one of many determinants of the group of mothers reporting more problems than their children. At the same time, cognitive difficulties were a more specific determinant of the group of children reporting more problems than their mothers. Several mechanisms may explain why lower child cognitive abilities determined discrepancies. First, in general, children with a lower IQ and verbal difficulties could, despite the age appropriate instrument used, have more trouble to report their emotions and behavior. This can result in either under or over reporting of problems. Indeed, a study on credibility of informants showed that clinicians judged children with lower cognitive abilities to be less credible informants [56]. Second, children with a lower IQ and verbal difficulties may really suffer from more problems, in particular in a cognitive environment like for example school. Some of the mother–child reporting discrepancies elucidated by this study may inform us about problems in a context that mothers cannot easily observe. Indeed, additional analyses with teacher reported data showed that teachers also reported more child problems if children reported more problems than their mothers.
Methodological considerations
Two methodological issues are important to discuss. First, discrepancies can only exist if problems are reported by at least one or the other informant. Thus, determinants of informant discrepancies and determinants of the level of problem behavior may be closely related. Indeed, we found that the profiles with larger discrepancies also had the highest average problem scores. Yet, the average level of problems could not fully explain our results as the two profiles with highest problem levels, but with a different direction of discrepancies in mother and child reports, had very distinct determinants. Second, we studied mother–child reporting discrepancies using non-parallel assessment methods: a puppet interview versus a questionnaire with a different scale structure and different items. This difference in instruments contributed per definition to the discrepancies. In other words, the study design introduced some random error by the choice of measurement tools [1]. Nevertheless, there were several specific determinants clearly associated with each profile. It is unlikely that these specific associations only explained random error. Rather, the findings of the present study are arguably ecologically valid, because different assessments tools reported by different informants are often used in research and clinical settings.
Strengths and Limitations
This study has considerable strengths, including the use of young children’s self-reports of their problems thereby expanding the age range of previous studies, the large sample size which allowed examining the unique contribution of multiple determinants, and the comprehensive set of characteristics that were jointly studied in association with informant discrepancies. Still, several limitations need to be discussed. First, we aimed at assessing determinants that influenced mother–child reporting discrepancies. However, we did not obtain concurrent measures of parental psychopathology and parental harsh discipline. Although previous studies indicated, as discussed before, that psychopathological symptoms and parenting styles are rather stable over time, the time-lag may have influenced our results. Yet, this time-lag may rather have led to underestimation of associations than to overestimation. Second, the entropy of the latent profile solution was .68, indicating that there was some insecurity in the estimation of the profiles. Consequently, the small effects of some of the determinants must be interpreted cautiously. Third, our non-response analysis demonstrated that participants included in the study had a higher socioeconomic status and were more often of Dutch national origin. Therefore, one should be careful when generalizing these findings. Yet, selective participation in cohort studies particularly constitutes a problem for estimating prevalence, but less likely biases the associations between variables [57].
Conclusions and Implications
The current study demonstrates that determinants of mother–child reporting discrepancies largely depend on the relative problem levels and, importantly, on which informant reports a higher level of problems. For instance, a positive family environment is associated with the absence of discrepancies, while an adverse family environment increases the likelihood that mothers report more problems than their children. Alternatively, child-related characteristics and cognitive difficulties in particular increase the likelihood that children report more problems than their mothers. These findings have an important implication for the way discrepancies in maternal and self-reports of young child problem behavior are perceived. If a mother reports more problems than her child, researchers or clinicians should be aware that family conflict, in addition to other environmental factors and child cognitive functioning, may underlie these discrepancies. In contrast, when a child reports much more problems than his or her mother, one should consider that this is mainly determined by child related characteristics such as a child’s cognitive functioning.
The clinical utility of our results should, however, be evaluated taking into account the following issues. We examined children below the age of 8, different processes may play a more or less important role in older children. In addition, even though we identified specific determinants of mother–child reporting discrepancies, effect estimates were small. Nevertheless, the associations observed in this large non-clinical sample may represent important mechanisms on an individual level, particularly in clinical settings.
Discrepancies between mothers’ and young children’s reports of problem behavior point to valuable information about underlying reporter characteristics. At the same time, knowledge of families and children can facilitate interpreting discrepancies in mother–child reports that are often difficult to conceptualize and can thereby facilitate diagnostic decisions.
Summary
Informant discrepancies are common when multiple informants rate child or adolescent problems. Discrepancies can influence how researchers and clinicians interpret information, and may thus impact decision making in research and clinical practice. In this study the unique contribution of multiple determinants to discrepancies in mothers’ and young children’s reports of problem behavior was examined. Discrepancies were examined by modeling patterns in maternal and children’s reports of child internalizing and externalizing problems using latent profile analysis. Mother reported child problems were obtained with the Child Behavior Checklist and children’s self-reported problems with the Berkeley Puppet Interview in 5,414 6-year-old children. Four profiles were identified that could be distinguished by problem level, and the direction and magnitude of mother–child reporting discrepancies: a first profile represented agreement (46 %), a second profile represented slight discrepancies (30 %), than there were two profiles with higher problem levels and more discrepancies. The latter two profiles were characterized either by the children (11 %) or the mothers (13 %) reporting more problems. Compared to the first profile, the second profile was predominantly characterized by a positive family environment, the third profile by child cognitive difficulties, and the fourth profile by harsh parenting and poor family functioning. This study demonstrated that determinants of discrepancy in mother and child reports of problem behavior largely depend on the level of problems and on which informant reports a higher level of problems. Knowledge of specific child and family related characteristics that may impact mother–child reporting discrepancies can help the interpretation of each informant’s report of child problems and can thereby facilitate diagnostic decisions.
References
Kraemer HC, Measelle JR, Ablow JC, Essex MJ, Boyce WT, Kupfer DJ (2003) A new approach to integrating data from multiple informants in psychiatric assessment and research: mixing and matching contexts and perspectives. Am J Psychiatry 160(9):1566–1577
Valla JP, Bergeron L, Smolla N (2000) The Dominic-R: a pictorial interview for 6- to 11-year-old children. J Am Acad Child Adolesc Psychiatry 39(1):85–93
Ablow JC, Measelle JR, Kraemer HC, Harrington R, Luby J, Smider N et al (1999) The MacArthur Three-City Outcome Study: evaluating multi-informant measures of young children’s symptomatology. J Am Acad Child Adolesc Psychiatry 38(12):1580–1590
Ringoot AP, Jansen PW, Steenweg-de Graaff J, Measelle JR, van der Ende J, Raat H et al (2013) Young children’s self-reported emotional, behavioral, and peer problems: the Berkeley Puppet Interview. Psychol Assess 25(4):1273
Achenbach TM, McConaughy SH, Howell CT (1987) Child/adolescent behavioral and emotional problems: Implications of cross-informant correlations for situational specificity. Psychol Bull 101(2):213–232
Youngstrom E, Loeber R, Stouthamer-Loeber M (2000) Patterns and correlates of agreement between parent, teacher, and male adolescent ratings of externalizing and internalizing problems. J Consult Clin Psychol 168:1038–1050
De Los Reyes A, Kazdin AE (2004) Measuring informant discrepancies in clinical child research. Psychol Assess 16(3):330–334
Grills AE, Ollendick TH (2002) Issues in parent-child agreement: the case of structured diagnostic interviews. Clin Child Fam Psychol 5(1):57–83
van der Ende J, Verhulst FC, Tiemeier H (2012) Agreement of informants on emotional and behavioral problems from childhood to adulthood. Psychol Assess 24(2):293–300
De Los Reyes A, Thomas SA, Goodman KL, Kundey SMA (2013) Principles underlying the use of multiple informants’ reports. Annu Rev Clin Psychol 9:123–149
De Los Reyes A, Kazdin AE (2005) Informant discrepancies in the assessment of childhood psychopathology: a critical review, theoretical framework, and recommendations for further study. Psychol Bull 131(4):483–509
Verhulst FC, van der Ende J (2008) Using Rating Scales in a clinical context. In: Rutter M, Bishop DVM, Pine DS, Scott S, Stevenson J, Taylor E et al (eds) Rutter’s child and adolescent psychiatry, 5th edn. Blackwell, Oxford
Grills AE, Ollendick TH (2003) Multiple informant agreement and the anxiety disorders interview schedule for parents and children. J Am Acad Child Adolesc Psychiatry 42(1):30–40
Kolko DJ, Kazdin AE (1993) Emotional/behavioral problems in clinic and nonclinic children: correspondence among child, parent and teacher reports. J Child Psychol Psychiatry 34(6):991–1006
Chi TC, Hinshaw SP (2002) Mother-child relationships of children with ADHD: the role of maternal depressive symptoms and depression-related distortions. J Abnorm Child Psychol 30(4):387–400
Duhig AM, Renk K, Epstein MK, Phares V (2000) Interparental agreement on internalizing, externalizing, and total behavior problems: a meta-analysis. Clin Psychol 7(4):435–453
Briggs-Gowan MJ, Carter AS, Schwab-Stone M (1996) Discrepancies among mother, child, and teacher reports: examining the contributions of maternal depression and anxiety. J Abnorm Child Psychol 24(6):749–765
Frick PJ, Silverthorn P, Evans C (1994) Assessment of childhood anxiety using structured interviews: patterns of agreement among informants and association with maternal anxiety. Psychol Assess 6(4):372–379
Krain AL, Kendall PC (2000) The role of parental emotional distress in parent report of child anxiety. J Clin Child Psychol 29(3):328–335
Treutler CM, Epkins CC (2003) Are discrepancies among child, mother, and father reports on children’s behavior related to parents’ psychological symptoms and aspects of parent–child relationships? J Abnorm Child Psychol 31(1):13–27
Youngstrom E, Izard C, Ackerman B (1999) Dysphoria-related bias in maternal ratings of children. J Consult Clin Psychol 67(6):905–916
Boyle MH, Pickles A (1997) Maternal depressive symptoms and ratings of emotional disorder symptoms in children and adolescents. J Child Psychol Psychiatry 38(8):981–992
Richters JE (1992) Depressed mothers as informants about their children: a critical review of the evidence for distortion. Psychol Bull 112(3):485–499
De Los Reyes A, Kazdin AE (2006) Informant discrepancies in assessing child dysfunction relate to dysfunction within mother–child interactions. J Child Fam Studies 15(5):643–661
De Los Reyes A, Youngstrom EA, Pabon SC, Youngstrom JK, Feeny NC, Findling RL (2011) Internal consistency and associated characteristics of informant discrepancies in clinic referred youths age 11 to 17 years. J Clin Child Adolesc Psychol 40(1):36–53
Goodman K, De Los Reyes A, Bradshaw C (2010) Understanding and using informants’ reporting discrepancies of youth victimization: a conceptual model and recommendations for research. Clin Child Fam Psychol 13(4):366–383
Reid JB, Kavanagh K, Baldwin DV (1987) Abusive parents’ perceptions of child problem behaviors: an example of parental bias. J Abnorm Child Psychol 15(3):457–466
Penney SR, Skilling TA (2012) Moderators of informant agreement in the assessment of adolescent psychopathology: extension to a forensic sample. Psychol Assess 24:386–401
Berg-Nielsen T, Solheim E, Belsky J, Wichstrom L (2012) Preschoolers’ psychosocial problems: in the eyes of the beholder? Adding teacher characteristics as determinants of discrepant parent–teacher reports. Child Psychiatry Hum Dev 43(3):393–413
Grietens H, Onghena P, Prinzie P, Gadeyne E, Van Assche V, Ghesquière P et al (2004) Comparison of mothers’, fathers’, and teachers’ reports on problem behavior in 5-to 6-year-old children. J Psychopathol Behav Assess 26(2):137–146
Lavigne JV, Dahl KP, Gouze KR, LeBailly SA, Hopkins J (2014) Multi-domain predictors of oppositional defiant disorder symptoms in preschool children: cross-informant differences. Child Psychiatry Hum Dev. doi:10.1007/s10578-014-0472-4
Strickland J, Hopkins J, Keenan K (2012) Mother–teacher agreement on preschoolers’ symptoms of ODD and CD: Does context matter? J Abnorm Child Psychol 40(6):933–943
Rubin DH, Althoff RR, Walkup JT, Hudziak JJ (2013) Cross-informant agreement on child and adolescent withdrawn behavior: a latent class approach. Child Psychiatry Hum Dev 44(3):361–369
Jaddoe VW, van Duijn CM, Franco OH, van der Heijden AJ, van Ilzendoorn MH, de Jongste JC et al (2012) The Generation R Study: design and cohort update 2012. Eur J Epidemiol 27(9):739–756
Arseneault L, Moffitt TE, Caspi A, Taylor A, Rijsdijk FV, Jaffee SR et al (2003) Strong genetic effects on cross-situational antisocial behaviour among 5-year-old children according to mothers, teachers, examiner-observers, and twins’ self-reports. J Child Psychol Psychiatry 44(6):832–848
Achenbach TM, Rescorla LA (2000) Manual for the ASEBA preschool forms and profiles. University of Vermont, Research Center for Children, Youth & Families, Burlington
Statistics Netherlands (2004) Allochtonen in Nederland 2004 [Foreigners in the Netherlands 2004]. Centraal Bureau voor de Statistiek, Voorburg/Heerlen. Retrieved from http://www.cbs.nl/nl-NL/menu/themas/bevolking/publicaties/publicaties/archief/2004/2004-b52-pub.htm
Derogatis LR (ed) (1993) The Brief Symptom Inventory (BSI): administration, scoring, and procedures. Manual, 3rd edn. National Computer System Inc., Minneapolis
Miller IW, Epstein NB, Bishop DS, Keitner GI (1985) The McMaster family assessment device: reliability and validity. J Marital Fam Ther 11(4):345–356
Straus MA, Hamby SL, Finkelhor D, Moore DW, Runyan D (1998) Identification of child maltreatment with the parent–child conflict tactics scales: development and psychometric data for a national sample of american parents. Child Abuse Negl 22:249–270
Jansen PW, Raat H, Mackenbach JP, Hofman A, Jaddoe VWV, Bakermans-Kranenburg MJ et al (2012) Early determinants of maternal and paternal harsh discipline: the Generation R Study. Fam Relat 61(2):253–270
Cortina JM (1993) What is coefficient alpha? An examination of theory and applications. J Appl Psychol 78(1):98–104
Tellegen PJ, Winkel M, Wijnberg-Williams BJ, Laros JA (2005) Snijders-Oomen Niet-Verbale Intelligentietest SON-R 2, 5-7. Handleiding [Snijders-Oomen Nonverbal Intelligence Test SON-R 2, 5-7. Manual]. Amsterdam: Boom Testuitgevers
Van Bon WHJ, Hoekstra JG (1982) Taaltests voor kinderen. Swets & Zeitlinger, Lisse
Nylund KL, Asparouhov T, Muthén BO (2007) Deciding on the number of classes in latent class analysis and growth mixture modeling: a Monte Carlo Simulation Study. Struct Equ Modeling Multidiscip J 14(4):535–569
Muthén LK, Muthén B (1998–2010) Mplus user’s guide, 6th edn. Muthén & Muthén, Los Angeles
Achenbach TM, Rescorla LA (2001) Manual for the ASEBA school-age forms and profiles. University of Vermont, Research Center for Children, Youth, & Families, Burlington
Kok R, Linting M, Bakermans-Kranenburg MJ, van Ijzendoorn MH, Jaddoe VWV, Hofman A et al (2013) Maternal sensitivity and internalizing problems: evidence from two longitudinal studies in early childhood. Child Psychiatry Hum Dev 44(6):751–765
Collishaw S, Goodman R, Ford T, Rabe-Hesketh S, Pickles A (2009) How far are associations between child, family and community factors and child psychopathology informant-specific and informant-general? J Child Psychol Psychiatry 50(5):571–580
Cents RAM, Diamantopoulou S, Hudziak JJ, Jaddoe VWV, Hofman A, Verhulst FC et al (2013) Trajectories of maternal depressive symptoms predict child problem behaviour: the Generation R Study. Psychol Med 43(01):13–25
Dickstein S, Seifer R, Hayden LC, Schiller M, Sameroff AJ, Keitner G et al (1998) Levels of family assessment: II. Impact of maternal psychopathology on family functioning. J Fam Psychol 12(1):23–40
Low SM, Stocker C (2005) Family functioning and children’s adjustment: associations among parents’ depressed mood, marital hostility, parent–child hostility, and children’s adjustment. J Fam Psychol 19(3):394–403
Velders FP, Dieleman G, Henrichs J, Jaddoe VW, Hofman A, Verhulst FC et al (2011) Prenatal and postnatal psychological symptoms of parents and family functioning: the impact on child emotional and behavioural problems. Eur Child Adolesc Psychiatry 20(7):341–350
Huang K-Y, O’Brien Caughy M, Lee L-C, Miller T, Genevro J (2009) Stability of maternal discipline practices and the quality of mother–child interaction during toddlerhood. J Appl Dev Psychol 30(4):431–441
LaGrange B, Cole DA (2008) An expansion of the trait-state-occasion model: accounting for shared method variance. Struct Equ Modeling 15(2):241–271
Youngstrom E, Youngstrom JK, Freeman AJ, De Los Reyes A, Feeny NC, Findling RL (2011) Informants are not all equal: predictors and correlates of clinician judgments about caregiver and youth credibility. J Child Adolesc Psychopharmacol 21(5):407–415
Wolke D, Waylen A, Samara M, Steer C, Goodman R, Ford T et al (2009) Selective drop-out in longitudinal studies and non-biased prediction of behaviour disorders. Br J Psychiatry 195(3):249–256
Acknowledgments
The Generation R Study is conducted by the Erasmus Medical Center in collaboration with the Erasmus University Rotterdam, School of Law and Faculty of Social Sciences; the Municipal Health Service Rotterdam area; the Rotterdam Homecare Foundation; and the Stichting Trombosedienst & Artsenlaboratorium Rijnmond (STAR), Rotterdam. We gratefully acknowledge the contribution of general practitioners, hospitals, midwives and pharmacies in Rotterdam. The present study was performed in close collaboration with the department of child and adolescent psychiatry of Riagg Rijnmond. The first phase of the Generation R Study was made possible by financial support from: Erasmus Medical Center, Rotterdam, Erasmus University Rotterdam and the Netherlands Organization for Health Research and Development (ZonMw). The work of Professor Tiemeier is supported by NWO-ZonMW VIDI (Grant No. 017.106.370).
Conflict of interest
Frank. C. Verhulst is a contributing author of the Achenbach System of Empirically based assessment, from which he receives remuneration. The remaining authors have no financial relationships relevant to this article to disclose.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Ringoot, A.P., van der Ende, J., Jansen, P.W. et al. Why Mothers and Young Children Agree or Disagree in Their Reports of the Child’s Problem Behavior. Child Psychiatry Hum Dev 46, 913–927 (2015). https://doi.org/10.1007/s10578-014-0531-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10578-014-0531-x