
Abstract
Background
Global academic difficulties have often been reported in youth with anxiety disorders, however, little is known about the specific academic deficits in this population.
Objective
To (a) evaluate the prevalence of seven specific academic impairments in children and adolescents with anxiety disorders, (b) determine whether these impairments are associated with demographic (i.e., race, gender and age) and clinical characteristics (i.e., type of disorder, anxiety severity and global impairment) and (c) examine the impact of anxiety treatments on these impairments.
Methods
As part of the Child-Adolescent Anxiety Multimodal Study (a randomized controlled trial), academic impairments, anxiety severity and global impairment were measured in 488 youth (mean age = 10.7 years) with separation, social and/or generalized anxiety disorders.
Results
At baseline, 47 % of the sample was rated as impaired on 4 out of 7 items, and nearly 10 % of the sample was rated as academically impaired on 6 out of 7 items. Conversely, 28 % reported no impairment across the 7 items. There were no significant differences in parent-reported academic impairments by race, age or gender. Academic impairment was significantly, positively correlated with anxiety severity and negatively correlated with global functioning. Treatment responders were significantly more likely than non-responders to evidence improvement across all seven specific academic items.
Conclusions
Specific academic impairments are prevalent among youth with anxiety disorders. The benefits of evidence-based treatments (i.e., medication/sertraline; CBT/Coping cat) extend beyond symptom relief to include improved academic performance, as perceived by parents, in youth with anxiety disorders.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Anxiety disorders are one of the most prevalent mental health problems in youth (Rapee et al. 2009). Without treatment, anxiety disorders can confer considerable impairment in functioning across multiple domains, including familial (e.g., getting along with siblings), social (e.g., making friends), and academic (e.g., performing well in school) (Langley et al. 2004; see Muroff and Ross 2011 for a review). Despite evidence showing that youth with excessive anxiety often experience general difficulty in school (Mychailyszyn et al. 2010), studies examining the negative impacts of excessive anxiety on specific academic tasks, such as concentrating and completing assignments, are surprisingly limited. In the limited extant research on specific academic tasks affected by anxiety, test anxiety has been negatively correlated with academic performance, as measured by standardized test scores (Weems et al. 2013). However, other specific aspects of academic performance that are impaired in anxious youth are not well-understood.
Excessive anxiety, assessed dimensionally or categorically, has been associated with global academic underachievement (i.e., poor grades and poor academic performance as rated by parents and teachers), both cross-sectionally and longitudinally in clinical and community samples of youth. For instance, in a longitudinal, epidemiologic study of youth, Ialongo and colleagues found that youth scoring in the top third on a measure of anxious symptoms (using the Revised Children’s Manifest Anxiety Scale) in 1st grade were more likely to score in the bottom third of the sample in academic achievement (as measured by a standardized achievement battery) in the 5th grade (Ialongo et al. 1995). Similarly, using prospective, longitudinal data from a community sample (N = 1,003), Duchesne and colleagues found a significant association between parent-reported anxiety symptoms in kindergarten and parent-reported difficulty with overall academic performance in 9th grade (Duchesne et al. 2005). In another study, a sample of youth with anxiety disorders (N = 174; age = 7–14 years) were rated by parents and teachers as having significantly more difficulty with learning and academic performance on the Achenbach scales compared to youth (N = 53) with no mental health diagnoses (Mychailyszyn et al. 2010). Together, these studies show that youth with excessive anxiety exhibit global academic difficulties. More research in large samples of youth with anxiety disorders is needed to understand what specific areas of academic performance are impaired and contribute to academic underachievement in this population. Also, relatively little is known about whether these specific academic impairments differ by age, gender, and/or specific diagnosis. The current study addressed these issues.
The current study also examined whether anxiety treatment impacts specific academic impairments. Research suggests that youth who receive psychosocial interventions for anxiety show improvements in global academic functioning. For instance, compared to anxious youth who did not receive treatment, youth who received cognitive behavioral therapy (CBT) showed improvements in academic motivation (Keogh et al. 2006), standardized test scores (Keogh et al. 2006), Grade Point Average (GPA) (Weems et al. 2009), and teacher and parent ratings of general academic functioning (as measured by the Child Behavior Checklist academic functioning scale and the Child Anxiety Impact Scale (CAIS) school subscale, respectively; Suveg et al. 2009; Wood 2006). These results provide initial support for the benefit of treating anxiety to improve academic functioning. However, the research to date included youth in a narrow age range who received only psychological treatment for anxiety and measured global functioning, rather than specific academic impairments. Thus, data are needed on a broader age range and for youth receiving evidence-based pharmacological, psychological, and combined pharmacological and psychological treatments.
The current study examined four aims. The first aim was to report the frequency of parent-reported difficulties on seven specific aspects of academic functioning in a large sample of youth diagnosed with anxiety disorders. Given high rates of general academic difficulty among youth with anxiety disorders, we hypothesized that a large proportion of parents would report impairment across the specific academic items. The second aim was to determine whether academic impairments varied as a function of gender, race, age, and diagnosis (e.g., social, generalized and separation anxiety disorders). Previous research shows that there are no age differences in parent-rated academic difficulty, thus, we did not expect to find age differences in the current study. Data on gender differences in academic performance among anxious youth are mixed (Derdikman-Eiron et al. 2012; Langley et al. 2004) and research on racial differences is lacking, thus we made no directional hypotheses regarding gender or race. Given the broad range of impairments Generalized Anxiety Disorder (GAD) confers, we hypothesized that youth with GAD would have more parent-rated impairments than youth with other diagnoses. The third aim was to determine whether specific academic impairments were associated with anxiety severity and global impairment. We expected that academic impairment would be positively correlated with anxiety severity and negatively correlated with global impairment scores. The fourth aim examined the impact of three anxiety treatments on specific academic impairments. We expected that parents of youth receiving a combination of medication and CBT would report significant reductions in impairments across all seven academic items, consistent with findings showing that youth receiving combined psychological and pharmacological treatment show the greatest reductions in anxiety symptoms and improvement in overall functioning. Also, we expected that treatment responders would show improvements in more impairments than non-responders (Walkup et al. 2008). These hypotheses were tested using data from the Child/Adolescent Anxiety Multimodal Treatment Study (CAMS; Walkup et al. 2008). CAMS was a multi-center randomized controlled trial that evaluated the efficacy of cognitive-behavioral therapy (Coping cat; CBT), medication (sertraline; SRT), combination (SRT and CBT; COMB), and pill placebo (PBO) in 488 anxious youth between the ages of 7–17 years (mean age = 10.7 years; see Compton et al. 2010 and Walkup et al. 2008 and for additional information on the CAMS).
Method
Participants
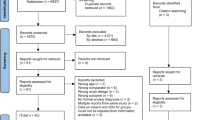
Demographic and diagnostic characteristics of the 488 youth who participated in the CAMS are displayed in Table 1. Participants were primarily Caucasian. Twenty-five percent of the sample were from low socioeconomic status (SES) backgrounds. At pre-treatment, all youth met diagnostic criteria for a primary diagnosis of an anxiety disorder (i.e., social phobia, generalized anxiety disorder and separation anxiety disorder) based on the Anxiety Disorder Interview Schedule for DSM-IV (Silverman and Albano 1996). The majority of youth (79 %) met criteria for 2 or more anxiety disorders. Additional details about the sample, including a CONSORT diagram, are available in other reports (Compton et al. 2010; Kendall et al. 2010).
Procedure
Approval for the current study was obtained from the Institutional Review Boards at all participating universities. Parents provided informed consent for their child’s participation; youth provided assent. The authors wrote the manuscript and are responsible for data gathering and/or analysis. Pfizer provided sertraline and placebo pills free of charge, but the company was not involved in study design, data analysis, manuscript preparation or publication of the study.
Design
Eligible participants were randomly assigned to receive 12 weeks of CBT, SRT, COMB or PBO treatment. Independent evaluators (IEs) who were blind to study condition conducted assessments at baseline and at weeks 4, 8, and 12. A CONSORT diagram describing details of participant recruitment, participant flow and randomization has been previously reported (Walkup et al. 2008). The current study used data from the baseline and week 12 time points.
Measures
The Anxiety Disorders Interview Schedule for DSM-IV, Parent and Child Versions, (ADIS-IV-C; Silverman and Albano 1996)
The ADIS-IV-C is the semi-structured diagnostic interview for childhood anxiety disorders used to determine primary diagnosis of the participants in the current study. It assesses anxiety, mood, and externalizing disorders, and screens for the presence of additional disorders (e.g., developmental, psychotic and somatoform). IEs generated severity and impairment ratings. Ratings range from 0 to 8 (a 4 is required to make a diagnosis). The ADIS has been extensively studied and has been found to have excellent interrater reliability, retest reliability, and concurrent validity (Kendall et al. 2010; Silverman et al. 2001; Wood et al. 2002). In the current study, interrater agreement (weighted k) for specific CAMS anxiety diagnoses were .87 for SAD, .78 for SOP, and .72 for GAD at week 12 (Piacentini et al. 2014).
Child Anxiety Impact Scale-Parent Version (CAIS-P; Langley et al. 2004)
A subset of items from the school subscale of the Child Anxiety Impact Scale-Parent version (CAIS-P; Langley et al. 2004) was used to measure the association between anxiety and academic impairments. The seven items used in the current study were: completing assignments, concentrating on work, doing homework, getting good grades, giving oral reports/reading in class, taking tests/exams and writing in class. Three items (getting to school on time, eating lunch with other kids, and doing fun things during recess) were not used in the current study because they are not specific academic tasks. Using a 4-point Likert-type scale, parents reported the degree to which their child’s anxiety impairs their performance on specific academic tasks, from “not at all” to “very much.” In the current study, ratings of “pretty much” or “very much” were used to indicate impairment; binary scores were created to compare impaired youth to non-impaired youth. For analyses using overall scores, a total score was calculated by summing ratings across the seven items. Descriptive statistics for item scores are presented in Table 2. In a psychometric evaluation of the CAIS-P, Cronbach’s alpha for the CAIS-P school subscale was .86 (Langley et al. 2004). Cronbach’s alpha for the seven items of the school subscale used in the present study was .83.
The Children’s Global Assessment Scale (CGAS; Shaffer et al. 1983)
The CGAS is a clinician rating of global functioning performed by IEs. The CGAS is a modification of the adult Global Assessment Scale that provides a measure of global impairment and functioning with scores ranging from 1 (lowest functioning/greatest impairment) to 100 (highest functioning/lowest impairment). The psychometric properties of the scale have been investigated extensively and are adequate (Bird et al. 1987; Dyrborg et al. 2000).
Clinical Global Impression-Severity Scale (CGI-S; Guy 1976)
The CGI-S is a clinician (IE) rating of anxiety severity using a 7-point scale, ranging from 0 (normal) to 7 (most severe anxiety). Inter-rater agreement was high for anxiety severity (r = .85; Walkup et al. 2008).
Clinical Global Impression-Improvement Scale (CGI-I; Guy 1976)
The CGI-I is an IE rating of the child’s improvement in anxiety symptoms as compared to their baseline evaluation, used to determine responder status. Scores range from 1 (Very much improved) to 7 (Very much worse). Treatment responders were defined by a CGI-I score of 1 (very much improved) or 2 (much improved). If the CGI-I rating was 3 or greater, the child was classified as a non-responder.
Demographic Information
Parents provided demographic information, including gender, race, living situation, family composition, income, education level and parental occupation at the initial study visit.
Statistical Analyses
For aim 1, frequencies of the seven academic items were calculated to determine how often parents endorsed that their child had impairments in specific areas of academic performance. To address aim 2, χ2 analyses of independence were conducted to compare the frequency of specific academic impairments across gender, race, age and diagnosis. For age, a binary variable was created (ages 7–11 or 12–17). For diagnosis, youth with a diagnosis were compared to youth without that diagnosis (e.g., youth with SAD in their diagnostic profile vs. youth without any SAD). For aim 3, Pearson’s correlations were calculated between the overall CAIS-P academic impairment score and anxiety severity (as measured by the CGI-S score at the 12-week time point) and between academic impairments and global impairment (as measured by the CGAS at the 12-week time point). For aim 4, McNemar’s tests were conducted to compare the frequency of specific academic impairments from pre- to post-treatment within treatment groups (COMB, SRT, CBT and PBO). Chi square analyses were conducted to compare the proportion of treatment responders (regardless of treatment group) to non-responders with impairment on each academic item. The SAS macro, COMBCHI, for imputed datasets was used to test the significance of χ2. This macro combines Chi square results and reports them as an F-statistic.
For all aims, the False Discovery Rate (FDR) procedure was used to address the problem of familywise error when conducting multiple comparisons (Benjamini and Hochberg 1995). The FDR determines the expected proportion of false discoveries among significant findings, yielding a q-value based on the p-values of the multiple comparisons. P-values below the set q-value are considered statistically significant.
Multiple imputation using IBM SPSS version 20 was used to create 20 imputed datasets under the assumption that data were missing at random (MAR) for all aims. Overall, there was a small amount of missing data. Approximately 4 % of the data pre-treatment data were missing overall. Missingness increased at the post-treatment evaluation, with 14 % of data missing overall. This is likely due to participants being lost to follow-up. Missingness was evenly distributed across treatment groups.
Results
Aim 1: Description of Academic Impairments
Table 3 shows frequencies of the seven specific academic impairments for the whole sample and by race (Caucasian; Non-Caucasian), gender, and age (7–11 years; 12–17 years). Rates of impairment ranged from 22 to 45 % on the items at baseline. The CAIS-P school items most frequently endorsed as problematic (i.e., rated as “pretty much” or “very much” a problem) for the whole sample were: concentrating on work (45.1 %) and giving oral reports/reading aloud (38.7 %). Concentrating on work was also the most frequently reported difficulty across racial, gender, and age groups.
Aim 2: Academic Impairments by Demographic and Diagnostic Characteristics
Demographic Characteristics
As shown in Table 3, there were no significant baseline differences between racial, gender, or age groups on any of the CAIS-P items.
Diagnosis
Frequencies of the academic impairments at baseline by diagnosis and differences in impairments among diagnostic groups are presented in Table 4. As predicted, youth with GAD had the highest number of parent-reported impairments.
Aim 3: Anxiety Severity and Global Functioning
Anxiety Severity
The summed total score on the 7 CAIS-P items was modestly but significantly and positively correlated with the baseline CGI-S score (r = .14, p < .01, 2-tailed). Independent samples t-tests compared baseline severity scores of youth with and without impairment on each academic item. As shown in Table 5, there were significant differences on CGI-S scores between impaired and non-impaired youth 6 out of 7 items (false discovery rate corrected at p < .04).
Global Functioning
The summed total score across the 7 CAIS-P items was modestly but significantly and negatively correlated with the baseline CGAS score (r = −.11, p < .05, 2-tailed). Results of an independent samples t test comparing the baseline global functioning scores of youth with and without impairment on each academic item are in Table 5. There were significant differences on CGAS scores between impaired and non-impaired youth on 4 of the 7 items (false discovery rate corrected at p < .02).
Aim 4: Changes in Academic Impairment from Pre- to Post-Treatment Within Treatment Groups and Between Treatment Responders and Non-responders
Table 6 displays changes in impairment from pre- to post-treatment on each academic item. In each of the active treatment groups (i.e., COMB, SRT, and CBT), McNemar’s test revealed significant decreases in parent-rated academic impairment from pre- to post-treatment on all 7 items (false discovery rate corrected at p < .05). In the placebo group, McNemar’s test revealed significant decreases in parent-rated academic impairment from pre- to post-treatment for 5 out of the 7 items (false discovery rate corrected at p < .04). Table 7 shows the frequency of academic impairments between treatment responders and non-responders. Significantly more non-responders than responders were rated as impaired on all 7 academic items at post-treatment.
Discussion
This study examined specific academic deficits, as reported by parents, in a large sample of clinically anxious youth. Study objectives were: (1) to report the frequency of specific academic impairments, (2) to examine associations between specific impairments and demographic and diagnostic characteristics, (3) to examine associations between anxiety severity, global functioning and impairments and (4) to report changes in academic impairments from pre- to post-treatment in the full sample and within treatment groups.
At baseline, nearly half the sample was reported as impaired on 4 out of 7 academic items; 28 % were not reported as impaired on any item. Impaired concentration on schoolwork was the most frequently reported academic difficulty across the whole sample and within racial, gender, age, and diagnostic subgroups, indicating that this is a key feature of the most commonly occurring anxiety disorders. These findings are consistent with studies showing that youth with anxiety often selectively attend to threat in the environment (e.g., attentional bias; Bar-Haim et al. 2007; Roy et al. 2008). Such an attentional bias may manifest as distraction (Eysenck et al. 2007), which can reduce cognitive efficiency and negatively affect academic performance (Derakshan and Eysenck 2009). Time accommodations may mitigate the effects of reduced efficiency and be empirically justified for some anxious children.
The negative impact of anxiety on concentration is an important finding given emerging evidence that impaired concentration due to anxiety may be misdiagnosed as attention deficit/hyperactivity disorder (ADHD) (Abramovitch et al. 2013). Although estimates of the comorbidity between ADHD and anxiety disorders range from 25 to 40 % in some clinical and community samples (Jarrett and Ollendick 2012; Tannock 2009), only 12 % of participants were identified as having ADHD on the ADIS-IV-C in CAMS (Kendall et al. 2008). Thus, for many participants in the present study, it is more likely that difficulty concentrating represents an anxiety-related academic impairment, not comorbid ADHD.
Approximately 39 % of the entire sample was reported to have difficulty giving oral reports/reading aloud. This finding is consistent with the symptom presentation of youth with anxiety and may be attributed to underlying concerns about negative evaluation, scrutiny, perfectionism, and performance. Given the frequency of reading aloud and presenting orally in the school setting, difficulty with these tasks could impact overall academic performance and could contribute to negative longer-term academic and vocational outcomes for anxious youth (Duchesne et al. 2008; Kessler et al. 1995).
Based on this study, it appears that the frequency and severity of academic impairments varies by diagnostic but not demographic characteristics. With regard to demographic differences, more research with larger samples of minority racial and ethnic groups is needed to improve generalizability of study findings. Youth with GAD exhibited the highest number of specific academic impairments, with parent-rated difficulty on 6 of the 7 CAIS-P items. This high number of impairments is consistent with the pervasive nature of the dread and worry associated with GAD, which affects functioning across many areas. Given the frequency of academic impairments in youth with GAD, identifying and treating these youth could have positive effects on academic performance and even long-term school and vocational outcomes. Youth with SOP were rated as having significant difficulty with giving oral reports/reading aloud, which is consistent with the performance fears associated with the diagnosis. This finding highlights how anxiety affects those with SOP differently from those with GAD, and has treatment implications. For example, youth with GAD may benefit from strategies to challenge cognitive distortions related to pervasive school-related dread and general worry, whereas youth with SOP may benefit from graduated exposure to performance activities, such as hand-raising, participating in class, and reading aloud. Only youth with SAD did not have significant academic impairments. In the case of SAD, the greatest school-related challenge may be getting the child to go to or stay in school, which was not assessed in the current study.
Is overall academic impairment related to overall anxiety severity and global impairment? Findings revealed a modest (.14) relation between academic impairment and anxiety severity and global impairment. Although causality cannot be established, it is likely that relations between anxiety, overall functioning and academic performance are reciprocal, such that excessive anxiety contributes to reduced overall functioning, which negatively affects academic performance. At the same time, academic problems, such as poor grades, increase anxiety and reduce overall functioning. This bidirectional conceptualization is consistent with a developmental psychopathology model of the etiology and maintenance of anxiety disorders, in which a child’s symptoms influence how he interacts with his environment, while anxious symptoms are simultaneously reinforced by contextual factors (i.e., peer, family, teacher, school interactions; McClure and Pine 2006).
Significant reductions in impairment on all 7 academic items were reported in each of the active treatments (CBT, SRT, and COMB) from pre- to post-treatment. The absence of clear differences between the three active treatment groups in reducing academic impairments was unexpected, given that the COMB response rate was significantly greater (81 % response) than the other two active groups (55 % response SRT; 60 % response CBT; Walkup et al. 2008). We speculate that parent detection of change in child academic function may require a longer period of observation than the 12-week acute treatment period reported herein.
Significant reductions in impairment were also reported in the PBO group, but for only 5 items, which likely reflects the modest (relative to active treatments), but measureable decreases in anxiety symptoms in this group (36 % reduction in anxiety severity from baseline to Week 12; 24 % responder rate). This symptom reduction, either as a result of a placebo effect or the normative fluctuation of anxiety symptom severity in youth, could have positively biased parent reports of academic impairment, and explain the significant reduction in impairments in this group. Notably, the 2 academic items that did not show significant change in the PBO group both relate to in-class task performance (taking tests/exams and writing in class), where the effects of reduced cognitive efficiency due to anxiety may be most evident.
Finally, treatment responders, compared to non-responders (regardless of treatment arm), showed fewer academic difficulties at post-treatment. These results suggest that academic task performance may be considered a surrogate response measure of treatment and that symptom reduction may be a sufficient intervention for most youth to experience improved academic performance. Conversely, treatment of pediatric anxiety without reductions in academic impairment may suggest a need for treatment intensification or re-evaluation of the treatment. What is left unanswered by virtue of our study design is whether targeting academic impairment as an additional component of anxiety treatment may yield even greater academic improvements.
Limitations
Results should be interpreted in light of several potential limitations. Only 7 specific academic impairments were assessed. It is possible that other areas, such as reading comprehension or rote memorization of math facts, are also negatively impacted by excessive anxiety. Only parent report was used to assess academic impairment; teacher reports, or more objective measures of academic functioning may have yielded differing results. As parents are not with their children during the school day, they may not be aware of the full extent of their child’s academic impairment. As noted, it is also possible that parent expectancies of positive treatment outcomes, particularly among treatment responders, could have positively biased parent reports of academic impairment. Future research would benefit from the use of multivariate techniques that would permit controlling for these expectancies. The CAMS sample included mostly Caucasian youth who met inclusion/exclusion criteria and had GAD, SOP and SAD diagnoses. Generalizability of the findings to minority youth or youth with other anxiety disorders and youth with other comorbid conditions (e.g., externalizing problems) may be limited.
Implications
Findings from the present study have several important implications for school-based mental health clinicians, teachers and students. First, results highlight several specific academic difficulties among youth with anxiety disorders. Given the frequency of these problems, schools might consider implementing an emotion-focused Response to Intervention (RtI) model to identify and support youth with excessive anxiety (Kearney and Graczyk 2014; Weems et al. 2014). Monitoring the relation between symptom reduction and academic deficits would be particularly helpful for youth in need of intensive, individualized intervention (i.e., Tier 3 of RTI model) and would inform future research on best practices for treating anxious youth in school settings (Kearney and Graczyk 2014; Weems et al. 2014). Second, because research indicates that targeting specific anxiety-related academic impairments can reduce other anxiety symptoms and promote academic performance (Weems et al. 2009), school mental health professionals would benefit from training in treatments that target the academic impairments identified in the current study as common among anxious youth (e.g., concentrating on work, reading aloud). Third, school mental health professionals should assess for excessive anxiety in students referred for evaluation for underachievement and/or neurocognitive problems. It is possible that some youth with academic problems, particularly those with difficulties exhibiting poor in-class performance, are struggling with anxiety-related academic problems rather than, or in addition to, another difficulty (e.g., a specific learning disorder or ADHD).
In sum, while a “glass half full” perspective suggests that nearly a third of parents of anxious youth do not report impairments in academic functioning, a significant proportion do. The empirically supported treatments tested in this study–CBT (Coping Cat), SSRI medications (sertraline) and a combination thereof–appear to significantly reduce academic difficulties, although additional research on mediators of this effect is warranted. School-based mental health professionals would benefit from continued training in the impact of anxiety on academic functioning and how empirically-supported psychosocial interventions can reduce barriers to learning for anxious youth (Ginsburg et al. 2012).
References
Abramovitch, A., Dar, R., Mittelman, A., & Schweiger, A. (2013). Don’t judge a book by its cover: ADHD-like symptoms in obsessive compulsive disorder. Journal of Obsessive Compulsive and Related Disorders, 2(1), 53–61. doi:10.1016/j.jocrd.2012.09.001.
Bar-Haim, Y., Lamy, D., Pergamin, L., Bakermans-Kranenburg, M. J., & Van Ijzendoorn, M. H. (2007). Threat-related attentional bias in anxious and nonanxious individuals: A meta-analytic study. Psychological Bulletin, 133, 1–24. doi:10.1037/0033-2909.133.1.1.
Benjamini, Y., & Hochberg, Y. (1995). Controlling the false discovery rate: A practical and powerful approach to multiple testing. Journal of the Royal Statistical Society. Series B (Methodological), 57, 289–300.
Bird, H. R., Canino, G., Rubio-Stipec, M., & Ribera, J. C. (1987). Further measures of the psychometric properties of the Children’s Global Assessment Scale. Archives of General Psychiatry, 44, 821–824. doi:10.1001/archpsych.1987.01800210069011.
Compton, S., Walkup, J., Albano, A., Piacentini, J., Birmaher, B., Sherrill, J., & March, J. (2010). Child/Adolescent Anxiety Multimodal Study (CAMS): Rationale, design, and methods. Child and Adolescent Psychiatry and Mental Health, 4, 1. doi:10.1186/1753-2000-4-1.
Derakshan, N., & Eysenck, M. W. (2009). Anxiety, processing efficiency, and cognitive performance: New developments from attentional control theory. European Psychologist, 14, 168–176. doi:10.1027/1016-9040.14.2.168.
Derdikman-Eiron, R., Indredavik, M. S., Bakken, I. J., Bratberg, G. H., Hjemdal, O., & Colton, M. (2012). Gender differences in psychosocial functioning of adolescents with symptoms of anxiety and depression: Longitudinal finding from the Nord-Trondelag Health Study. Social Psychiatry and Psychiatric Epidemiology, 47, 1855–1863. doi:10.1007/s00127-012-0492-y.
Duchesne, S., Larose, S., Guay, F., Tremblay, R. E., & Vitaro, F. (2005). The transition from elementary to high school: The pivotal role of family and child characteristics in explaining trajectories of academic functioning. International Journal of Behavioral Development, 29, 409–417. doi:10.1080/01650250500206067.
Duchesne, S., Vitaro, F., Larose, S., & Tremblay, R. E. (2008). Trajectories of anxiety during elementary school years and the prediction of high school noncompletion. Journal of Youth and Adolescence, 37, 1134–1146. doi:10.1007/s10964-007-9224-0.
Dyrborg, J., Larsen, F., Nielsen, S., Byman, J., Buhl-Nielsen, B., & Gautre-Delay, F. (2000). The Children’s Global Assessment Scale (CGAS) and Global Assessment of Psychosocial Disability (GAPD) in clinical practice-substance and reliability as judged by intraclass correlations. European Child and Adolescent Psychiatry, 9, 195–201. doi:10.1007/s007870070043.
Eysenck, M. W., Derakshan, N., Santos, R., & Calvo, M. G. (2007). Anxiety and cognitive performance: Attentional control theory. Emotion, 7, 336–353. doi:10.1037/1528-3542.7.2.336.
Ginsburg, G. S., Becker, K. D., Drazdowski, T. K., & Tein, J. Y. (2012). Treating anxiety disorders in inner city schools: Results from a pilot randomized controlled trial comparing CBT and usual care. Child & Youth Care Forum, 41, 1–19. doi:10.1007/s10566-011-9156-4.
Guy, W. (1976). The Clinical Global Impression Scale. In: ECDEU assessment manual for psychopharmacology-revised (pp. 218–222). Rockville, MD: US Department of Health, Education and Welfare, ADAMHA, MIMH Psychopharmacology Research Branch.
Ialongo, N., Edelsohn, G., Werthamer-Larsson, L., Crockett, L., & Kellam, S. (1995). The significance of self-reported anxious symptoms in first grade children: Prediction to anxious symptoms and adaptive functioning in fifth grade. Child Psychology & Psychiatry & Allied Disciplines, 36, 427–437. doi:10.1111/j.1469-7610.1995.tb01300.x.
Jarrett, M. A., & Ollendick, T. H. (2012). Treatment of comorbid attention-deficit/hyperactivity disorder and anxiety in children: A multiple baseline design analysis. Journal of Consulting and Clinical Psychology, 80, 239–244. doi:10.1037/a0027123.
Kearney, C. A., & Graczyk, P. (2014). A response to intervention model to promote school attendance and decrease school absenteeism. Child & Youth Care Forum, 43, 1–25.
Kendall, P., Compton, S., Walkup, J., Birmaher, B., Albano, A., Sherrill, J., & Piacentini, J. (2010). Clinical characteristics of anxiety disordered youth. Journal of Anxiety Disorders, 24, 360–365. doi:10.1016/j.janxdis.2010.01.009.
Kendall, P. C., Hudson, J., Gosch, E., Flannery-Schroeder, E., & Suveg, C. (2008). Cognitive-behavioral therapy for anxiety disordered youth: A randomized clinical trial evaluating child and family modalities. Journal of Consulting and Clinical Psychology, 76, 282–297. doi:10.1037/0022-006X.76.2.282.
Keogh, E., Bond, F. W., & Flaxman, P. E. (2006). Improving academic performance and mental health through a stress management intervention: Outcomes and mediators of change. Behavior Research and Therapy, 44, 339–357. doi:10.1016/j.brat.2005.03.002.
Kessler, R. C., Foster, C. L., Saunders, W. B., & Stang, P. E. (1995). Social consequences of psychiatric disorders I: Educational attainment. The American Journal of Psychiatry, 152, 1026–1032. http://ajp.psychiatryonline.org/article.aspx?articleID=171111.
Langley, A. K., Bergman, R., McCracken, J., & Piacentini, J. C. (2004). Impairment in childhood anxiety disorders: Preliminary examination of the Child Anxiety Impact Scale-Parent Version. Journal of Child and Adolescent Psychopharmacology, 14, 105–114. doi:10.1089/104454604773840544.
McClure & Pine. (2006). Social anxiety and emotion regulation: A model for developmental psychopathology perspectives on anxiety disorders. In D. Cicchetti & D. Cohen (Eds.), Developmental psychopathology (2nd Edn., Vol. 3, pp. 470–502). New York: Wiley.
Muroff, J., & Ross, A. (2011). Social disability and impairment in childhood anxiety. In D. McKay & E. A. Storch (Eds.), Handbook of child and adolescent anxiety disorders (pp. 457–478). New York, NY: Springer Science Business Media.
Mychailyszyn, M. P., Mendez, J. L., & Kendall, P. C. (2010). School functioning in youth with and without anxiety disorders: Comparisons by diagnosis and comorbidity. School Psychology Review, 39, 106–121. Retrieved from PsycINFO database.
Piacentini, J., Bennett, S., Compton, S. N., Kendall, P. C., Birmaher, B., Albano, A. M., & Walkup, J. (2014). 24- and 36-week outcomes for the Child/Adolescent Anxiety Multimodal Study (CAMS). Journal of the American Academy of Child and Adolescent Psychiatry, 53, 297–310. doi:10.1016/j.jaac.2013.11.010.
Rapee, R. M., Schniering, C. A., & Hudson, J. L. (2009). Anxiety disorders during childhood and adolescence: Origins and treatment. Annual Review of Clinical Psychology, 5311–5341. doi:10.1146/annurev.clinpsy.032408.153628.
Roy, A. K., Vasa, R. A., Bruck, M., Mogg, K., Bradley, B. P., & Sweeney, M. (2008). … and CAMS team. Journal of the American Academy of Child and Adolescent Psychiatry, 47, 1189–1196. doi:10.1097/CHI.0b013e3181825ace.
Shaffer, D., Gould, M. S., Brasic, J., Ambrosini, P., Fisher, P., Bird, H., & Aluwahlia, S. (1983). A children’s global assessment scale (CGAS). Archives of General Psychiatry, 40, 1228–1231.
Silverman, W. K., & Albano, A. M. (1996). Anxiety disorders interview schedule for DSM-IV: child and parent versions. New York, NY: Oxford University Press.
Silverman, W. K., Saavedra, L. M., & Pina, A. A. (2001). Test-retest reliability of anxiety symptoms and diagnoses with the Anxiety Disorders Interview Schedule for DSM-IV: Child and parent versions. Journal of the American Academy of Child and Adolescent Psychiatry, 40, 937–944. doi:10.1097/00004583-200108000-00016.
Suveg, C., Hudson, J. L., Brewer, G., Flannery-Schroeder, E., Gosch, E., & Kendall, P. C. (2009). Cognitive-behavioral therapy for anxiety-disordered youth: Secondary outcomes from a randomized clinical trial evaluating child and family modalities. Journal of Anxiety Disorders, 23, 341–349. doi:10.1016/j.janxdis.2009.01.003.
Tannock, R. (2009). ADHD with anxiety disorders. In T. E. Brown (Ed.), ADHD comorbidities: Handbook for ADHD complications in children and adults (pp. 131–155). Arlington, VA US: American Psychiatric Publishing Inc.
Walkup, J. T., Albano, A., Piacentini, J., Birmaher, B., Compton, S. N., Sherrill, J. T., & Kendall, P. C. (2008). Cognitive behavioral therapy, sertraline, or a combination in childhood anxiety. The New England Journal of Medicine, 359, 2753–2766. doi:10.1056/NEJMoa0804633.
Weems, C. F., Scott, B. G., Graham, R. A., Banks, D. M., Russell, J. D., Taylor, L. K., & Marino, R. C. (2014). Fitting anxious emotion focused intervention into the ecology of schools: Results from a test anxiety program evaluation. Prevention Science,. doi:10.1007/s11121-014-0491-1.
Weems, C. F., Scott, B. G., Taylor, L. K., Cannon, M. F., Romano, D. M., & Perry, A. M. (2013). A theoretical model of continuity in anxiety and links to academic achievement in disaster exposed school children. Development and Psychopathology, 25, 729–738. doi:10.1017/S0954579413000138.
Weems, C. F., Taylor, L. K., Costa, N. M., Marks, A. B., Romano, D. M., Verrett, S. L., et al. (2009). Effect of a school-based test anxiety intervention in ethnic minority youth exposed to Hurricane Katrina. Journal of Applied Developmental Psychology, 218–226. doi:10.1016/j.appdev.2008.11.005.
Wood, J. (2006). Effect of anxiety reduction on children’s school performance and social adjustment. Developmental Psychology, 42, 345–349. doi:10.1037/0012-1649.42.2.345.
Wood, J., Piacentini, J., Bergman, R., McCracken, J., & Barrios, V. (2002). Concurrent validity of the anxiety disorders section of the Anxiety Disorders Interview Schedule for DSM-IV: Child and parent versions. Journal of Clinical Child and Adolescent Psychology, 31, 335–342.
Acknowledgments
Funding for this research was supported by the following grants from the National Institute of Mental Health (NIMH): MH64089, MH64107, MH64003, MH63747, MH064092, and MH64088. Views expressed within this article represent those of the authors and are not intended to represent the position of the NIMH, National Institutes of Health, or Department of Health and Human Services. Phillip C. Kendall is an author of and receives royalties from publications of materials for treating childhood anxiety. James T. McCracken is a consultant for Roche, BioMarin, and PharmaNet and has research contracts with Roche, Seaside Therapeutics, and Otsuka. Boris Birmaher is an author of and receives royalties from publications by Random House and Lippincott Williams and Wilkins. John T. Walkup is a consultant for Shire and receives free medication and placebo from Eli Lilly, Pfizer, and Abbott for NIH-funded studies. He receives honoraria from the Tourette Syndrome Association and royalties from Guilford Press and Oxford University Press. Scott Compton has received research support from Shire Pharmaceuticals and the National Institutes of Health (NIH). Dara Sakolsky receives funding from NIH and the Brain and Behavior Research Foundation and honoraria from the American Academy of Child and Adolescent Psychiatry for teaching.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Nail, J.E., Christofferson, J., Ginsburg, G.S. et al. Academic Impairment and Impact of Treatments Among Youth with Anxiety Disorders. Child Youth Care Forum 44, 327–342 (2015). https://doi.org/10.1007/s10566-014-9290-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10566-014-9290-x