
Abstract
Purpose
Mechanistic and observational data together support a role for prolactin in breast cancer development. Determinants of prolactin in Asian populations have not been meaningfully explored, despite the lower risk of breast cancer in Asian populations.
Methods
Determinants of plasma prolactin were evaluated in 442 postmenopausal women enrolled in the Singapore Chinese Health Study, a population-based prospective cohort study. At baseline all cohort members completed an in-person interview that elicited information on diet, menstrual and reproductive history, and lifestyle factors. One year after cohort initiation we began collecting blood samples. Quantified were plasma concentrations of prolactin, estrone, estradiol, testosterone, androstenedione, and sex hormone-binding globulin (SHBG). Analysis of covariance method was used for statistical analyses with age at blood draw, time since last meal, and time at blood draw as covariates.
Results
Mean prolactin levels were 25.1% lower with older age at menarche (p value = 0.001), and 27.6% higher with greater years between menarche and menopause (p value = 0.009). Prolactin levels were also positively associated with increased sleep duration (p value = 0.005). The independent determinants of prolactin were years from menarche to menopause, hours of sleep, and the plasma hormones estrone and SHBG (all p values < 0.01).
Conclusion
The role of prolactin in breast cancer development may involve reproductive and lifestyle factors, such as a longer duration of menstrual cycling and sleep patterns.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Prolactin is a hormone of pituitary origin that is expressed in a number of extrapituitary sites, including the breast. Prolactin contributes to the growth of normal breast tissue through activation of signaling pathways that promote cell growth and survival [1]. Higher expression of the prolactin receptor (PRLr) in tumor versus normal breast tissue suggests that prolactin may also play a role in mammary tumorigenesis [2]. It has been demonstrated that site-specific, persistent prolactin overexpression induces mammary tumor development in mice, and potential mechanisms are being investigated in cells [3,4,5,6]. Evidence from prospective epidemiological studies implicates prolactin as a risk factor for postmenopausal breast cancer [7, 8]. For example, higher prolactin levels measured in serum samples collected within 10 years prior to cancer diagnosis were associated with a statistically significant 37% increase in postmenopausal breast cancer risk [8]. These mechanistic and observational data together provide substantial evidence for a prolactin-breast cancer link, but the underlying mechanisms have not been delineated. Using epidemiologic studies to investigate the determinants of higher circulating prolactin levels may provide key information for generating hypotheses to be tested in mechanistic studies of prolactin and breast cancer development.
Relationships between factors associated with breast cancer risk and circulating prolactin levels have been observed. Prolactin levels have been consistently shown to be inversely associated with parity, number of births, and menopausal status [9,10,11,12]. Less consistent results have been shown for relationships between circulating prolactin and body size, where positive associations have been reported for body mass index (BMI) in some [13, 14], but not in other studies [15]. It is plausible that diet may influence prolactin levels, but too little information has been published to make a conclusion about the results [16,17,18]. In one study, prolactin was found to be lower during the follicular phase of the menstrual cycle in women eating a diet high in polyunsaturated fatty acids [16], while other studies show no influence of dietary pattern on prolactin levels [17, 18]. Nearly all of these previous studies have been conducted among U.S. or western European populations, with similarly high incidence of breast cancer. Asian populations have historically had among the lowest incidence of breast cancer worldwide, until recently [19, 20]. Given the different reproductive histories, environmental, and genetic backgrounds in Asians compared with western populations, it is of interest to evaluate whether the determinants of prolactin levels also differ.
In this study we investigated determinants of plasma prolactin in a well-characterized cohort of 442 postmenopausal women enrolled in the Singapore Chinese Health Study, a population-based prospective cohort study. This cohort consists of > 60,000 residents of Singapore, and includes middle-aged and older Chinese men and women [21]. Specifically, we evaluated the relationship between plasma prolactin levels and factors with established or suggestive associations with breast cancer risk, including menstrual and reproductive characteristics, hormone levels, as well as diet and lifestyle factors.
Materials and methods
Study population
The design of the Singapore Chinese Health Study has been previously described [21]. Eligible subjects were permanent residents or citizens of Singapore aged 45–74 years and belonging to one of the two major Chinese dialect groups (Cantonese and Hokkien). At baseline between 1993 and 1998, all cohort members completed an in-person interview that included a validated 165-item food frequency questionnaire [22]. The questionnaire also elicited information on demographics, menstrual and reproductive history, hormone use, sleep, and medical history.
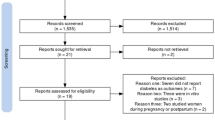
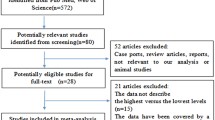
Between April 1994 and April 2005, biospecimens, including a blood sample, were obtained from 32,543 subjects, representing a 60% consent rate. Due to this study design, there was great variation in time between baseline interview and sample collection. We attempted to account for this by looking at our important findings after stratifying by years between sample collection and baseline interview (Supplemental Table S1). Most blood samples were collected in the morning with no requirement that the subjects fast. However, we asked and recorded the time of each subject’s last meal. We also attempted to account for this by looking at our important findings after stratifying by fasting status (Supplemental Table S2). All blood components were separated immediately and stored at − 80 °C until analyzed. Written, informed consent was obtained from study participants. The present investigation on determinants of blood hormone levels included the first 450 women enrolled who were at least 50 years of age, without a history of cancer, who had experienced a natural or a surgical menopause, and never used hormone replacement therapy. We excluded eight subjects who drank both green and black tea regularly (daily/weekly) because we hypothesized that the two types of tea might have opposing effects on blood hormone levels and our analysis was conducted on the remaining 442 women [23]. The Singapore Chinese Health Study was approved by the Institutional Review Boards at the National University of Singapore and the University of Pittsburgh.
Hormone measurements
Plasma aliquots from subjects under study were shipped in sealed containers on dry ice to the University of Southern California. Plasma prolactin concentrations (ng/mL) were quantified by a chemiluminescent immunometric assay using the Immulite analyzer (Siemens Healthcare Corporation, Deerfield, IL) at the Reproductive Endocrine Research Laboratory (University of Southern California). The interassay coefficients of variation (CV) for prolactin were 6.9, 5.8, and 3.9% at 6.7, 15.8, and 32.4 ng/mL, respectively [24]. We did not identify any outliers or values ± 2 standard deviations of the mean.
Plasma levels of estrone, estradiol, and androstenedione were measured using a validated radioimmunoassay [25, 26]. Prior to quantification, the hormones were first extracted with hexane:ethyl acetate (3:2) and then separated from interfering metabolites by the use of Celite column partition chromatography. The interassay CV at three (low, medium, and high) concentrations of estrone, estradiol, and androstenedione were between 7 and 16% [27]. Free estradiol was calculated on the basis of measured total estradiol concentration; sex hormone-binding globulin (SHBG) concentrations; and an assumed constant for albumin [28]. This method has been found to have high validity (r = 0.97) compared with direct measurements [29]. Other analytes were measured in plasma by highly specific direct immunoassays. SHBG was also measured by chemiluminescent immunometric assay on the Immulite analyzer. The SHBG intra-assay and interassay CVs were 7 and 10%, respectively. Hormone levels below the limit of detection were identified for estrone (n = 2), estradiol (n = 11), and free estradiol (n = 7), and indicated as missing values.
Statistical analysis
The distributions of the plasma hormone levels were skewed, which were largely corrected by transformation to logarithmic values that showed a more normalized distribution. Study subjects were also grouped into tertile categories based on the distributions of plasma hormones among all subjects. To examine differences in the distributions of reproductive factors across tertile of plasma prolactin either the Chi-square test (categorical variables) or the analysis of variance (ANOVA) (continuous variables) was used. We used the analysis of covariance method (ANCOVA) to compare mean plasma levels of estrone, estradiol, testosterone, SHBG, and androstenedione indices by tertiles of prolactin with adjustments for age at blood draw, time since last meal, and time at blood draw were included as covariates in all analyses. The same model was also used to compare mean plasma levels of prolactin by reproductive factors (i.e., age at menarche, menopause type, age at menopause, number of births, age at first birth, years between menarche and menopause, years between menarche and age at first birth, and years between first birth and blood draw), dietary factors (i.e., soy food, soy isoflavones, green tea, and black tea), and other factors (e.g., hours of sleep per day, height, weight, and body mass index). The percent difference of mean prolactin levels for the highest versus lowest category of hormone tertiles and the other exposures was calculated as (eb − 1) × 100. Difference of mean prolactin levels among exposure categories was assessed by F statistics obtained from linear regression models. Linear trends between prolactin levels and exposure categories were tested by fitting linear regression models with ordinal exposure variables. The multivariable linear regression analysis was used to determine the set of factors independently related to plasma prolactin. Calculations were performed using the SAS statistical software version 9.3 (SAS Institute, Cary, NC). All p values < 0.05 were considered statistically significant.
Results
In this study of 442 postmenopausal women all of whom were never hormone users, the average age at blood draw was 64.5 years (SD 4.8) and ranged from 54 to 81 years (Table 1). The average time from baseline interview to blood collection was 6.6 years (SD 1.7) and ranged from 4.4 months to 11.5 years. Cigarette smoking and alcohol use were rare. Nearly all women had at least one birth and achieved menopause naturally.
Mean age at blood draw increased with increasing tertiles of plasma prolactin (Table 1). The mean hours since last meal did not vary by prolactin tertile levels (Table 1). Although nonfasting blood samples were collected, 26% of the women provided blood at least 8 h since their last meal. Prolactin geometric mean levels, while not significantly different, varied slightly by time of day of blood draw, ranging from 7.08 ng/mL for blood draws between 8:00 and 9:45 am to 6.70 ng/mL between 1:00 and 2:45 pm (p value = 0.9) (Supplemental Table S3). Women in the highest tertile of plasma prolactin were more educated, had younger age at menarche and later age at first birth, compared with women in the first tertile (Table 1). Overall, adjusted geometric mean prolactin was 7.00 ng/mL.
Adjusted mean prolactin levels were evaluated by reproductive characteristics (Table 2). Statistically significant trends with prolactin were observed for age at menarche and years between menarche and age at first birth, where lower prolactin levels were observed with older age at menarche and with fewer years between menarche and age at first birth. There were also statistically significant differences in mean prolactin between the lowest and highest categories of years from menarche to menopause, with lower prolactin levels in women with fewer years from menarche to menopause. We also ran the analysis adjusting additionally for plasma-free estradiol, testosterone, SHGB, and androstenedione, which yielded a similar result (Supplemental Table S4).
In Table 3, mean prolactin levels are shown by level of selected diet and lifestyle factors. There was a significant positive relationship between prolactin and hours of sleep per day (p value = 0.005), with a 25.3% difference between mean prolactin in women who slept five or fewer hours per night and those who slept nine or more hours. No associations were observed with soy intake or tea (green or black) drinking in relation to mean prolactin levels. Similarly, no relationship was observed with dietary soy isoflavones (total isoflavones, genistein, daisein, or glycitein) (data not shown). BMI was not related to prolactin levels (Table 3), nor was weight or height (data not shown).
The relationship between plasma prolactin and other measured hormones is shown in Table 4. Prolactin levels decreased with increasing estrone (p value = 0.016). There was a statistically significant 14.8% decrease in adjusted mean prolactin comparing levels among women in the third versus first tertile of estrone. Similar trends were observed for estradiol and free estradiol, but the differences in mean prolactin between the highest and lowest tertiles were smaller than with estrone, and did not reach statistical significance. There was a positive relationship between prolactin and SHBG, with statistically significant increase in mean prolactin levels with increasing tertiles of SHBG (p value = 0.023). There was no relationship between prolactin and the androgens testosterone and androstenedione.
A linear regression modeling approach was used to evaluate the independent effects of reproductive, lifestyle, and plasma hormones on plasma prolactin levels. The initial model included all of the variables that had statistically significant individual relationships with plasma prolactin based on results shown in Tables 2, 3, and 4. This initial model (Model A) included terms for age at menarche, years from menarche to first birth, years from menarche to menopause, hours of sleep, plasma estrone, and plasma SHBG, as well as covariates for age at blood draw and time since last meal (Table 5). Age at menarche and years from menarche to first birth were not statistically significant predictors of prolactin in the initial model (Model A), and thus removed from further consideration. The remaining variables years from menarche to menopause (beta = 0.28 for ≥ 40.5 vs. < 34.5 years), hours of sleep (beta = 0.21 for ≥ 9 vs. ≤ 5 h), plasma estrone (beta = − 0.08 per ln pg/mL), and plasma SHBG (beta = 0.08 per lm nmol/mL) were retained in the final model (Model B) as independent, statistically significant predictors of prolactin (all p values < 0.01), and together explained 10.9% of the variation in plasma prolactin levels.
Discussion
Plasma prolactin levels among postmenopausal Chinese women in Singapore were associated with reproductive and lifestyle factors, as well as blood hormone levels. We reported statistically significant inverse associations for prolactin with older age at menarche and plasma estrone levels. In contrast, statistically significant positive associations for prolactin were observed with more years between menarche and first birth or menopause, and more hours of sleep per day. In summary, the statistically significant independent predictors of plasma prolactin were years between menarche and menopause, hours of sleep, and plasma estrone and SHBG. Together these factors explained 10.9% of the variation in plasma prolactin.
A novel finding from our study was a positive relationship between plasma prolactin and longer duration of sleep. A relationship between systemic prolactin and sleep has been documented in sleep-monitoring studies investigating sleep deprivation. In the context of short-term total sleep deprivation (24 or 36 h) [30,31,32], or partial sleep deprivation [33], prolactin levels decrease, while one study found no change in prolactin levels following sleep deprivation [34], although a follow-up study found a decrease in prolactin levels at 7 am after measuring at 2 h intervals [35]. Although long sleep duration was not directly tested in these sleep-monitoring studies, these findings align with those of the present study which show that longer sleep duration is associated with higher plasma prolactin.
Circadian disruptions are not limited to sleep deprivation but are also due to night shift work, sleep deficiency, and exposure to light at night. These circadian disruptions have been shown to increase breast cancer risk [36,37,38,39]; however the potential effect of sleep duration on breast cancer risk is not clear. In a prospective cohort of California teachers, sleeping more than 9 h a night was associated with an increased risk of estrogen-mediated cancers, including breast cancer (HR = 1.22; 95% CI 0.97–1.54, p for trend = 0.04) [38]. A large U.S. population-based case–control study found a significant 6% increase in relative breast cancer risk for every additional hour of sleep [39]. Although other prospective studies utilizing the Nurses Health Study, the Women’s Health Initiative, the Finnish Twin Cohort, the Breast Cancer Detection Demonstration Project, and the Breast Cancer Environment and Employment Study (Australia) reported no overall association between longer sleep duration and breast cancer risk [40,41,42,43,44], these studies found interesting findings or significant trends in subgroup analysis. In subsets of the Nurses Health Study, and the Women’s Health Initiative, a positive trend between increased sleep and breast cancer risk was found in women who consistently sleep more than 7 h (p trend = 0.05) [40], were diagnosed with ER-positive breast cancer (p trend = 0.0238), and have a normal BMI (p trend = 0.0764) [41]. The Breast Cancer Detection Demonstration Project found lower risk for ER-positive breast cancer in women who sleep for a short duration (p trend = 0.001 − ER+, p trend = 0.003 − ER/PR+) [43]. In contrast, in a subset of women from the Finnish Twin cohort who reported consistent sleep duration over time, an inverse association was reported between long sleep duration and breast cancer risk [44]. The full story is complex but these data together indicate that long sleep duration may have an impact on hormone responsive breast cancer.
Sleep duration and breast cancer risk has been interrogated in the Singapore Chinese Health Study, which was utilized for the current analysis. Initially, Wu et al. found a significantly lower breast cancer risk in postmenopausal women sleeping longer than 9 h (RR = 0.67, p trend = 0.047), however a more recent evaluation found no association between sleep duration and breast cancer risk [45, 46]. One limitation of this study was that questions on sleep were only administered at baseline and did not include information on sleep quality or consistency of sleep duration throughout follow-up [45, 46]. If longer sleep duration is related to breast cancer development, then prolactin may be a relevant contributing factor. Prolactin secretion is controlled by the circadian rhythm, which increase during nighttime sleeping and peaks in the early morning [47], and lower prolactin levels were reported among those who were sleep deprived [33, 48]. Thus, it is plausible that consistently sleeping for long periods (e.g., > 9 h) may lead to a longer cumulative exposure to higher circulating prolactin. Our finding should be interpreted cautiously, as it was based on one question about the average number of hours of sleep per day, and thus not able to capture potentially important distinctions between sleep duration and exposure to light at night and/or sleep quality, in addition to sleep duration as determinants of prolactin.
The greater the number of years between menarche and menopause, the longer a women is exposed to higher circulating levels of reproductive hormones [49, 50]. The positive association between the cumulative number of menstrual cycles and breast cancer risk has been observed in Whites [51, 52], and Asian Americans [53]. We observed that women in the highest quartile, with 40.5 or more years between menarche and menopause had statistically significant higher prolactin levels, compared with women in the lowest quartile with fewer than 34.5 years. Although age at menarche was related to prolactin levels in our data, the relationship weakened and lost statistical significance after including years between menarche and menopause in the linear regression model. The lack of an independent relationship between age at menarche and prolactin is consistent with previous studies in postmenopausal women [9, 13, 54]. Higher circulating estrogens are considered the primary factors responsible for the positive association between a longer reproductive window and breast cancer risk [51]. In consideration of our finding, it is plausible to also consider prolactin as part of the underlying mechanism. Replication of our finding in studies with available information on the potential relationship between prolactin and years between menarche and menopause is needed.
Prolactin levels are particularly influenced by the timing of pregnancy and lactation events, as is expected given the major involvement of prolactin in milk let down and lactation [55]. It was unexpected that we did not observe a relationship between parity and prolactin, given that lower prolactin levels have been consistently reported among postmenopausal women who had at least one birth, compared with no births [9,10,11]. There exists the possibility that with only 25 nulliparous women, or 5.7% of our study population, the study lacked the statistical power to observe statistically significant differences in mean prolactin levels by parity. Two other studies using a cross-sectional design included 131 nulliparous women (12% of their study population) in Nurses Health Study and 136 (13% of their study population) nulliparous women in the European Prospective into Cancer [9, 11]. One case–control study in an Australian cohort used a similar number of nulliparous women but specifically collected biospecimens during the 21 or 22 day of the menstrual cycle which may have been critical to observe a difference in their population [10]. For the other pregnancy characteristics, such as number of births and age at first birth, results from larger studies among postmenopausal women also report no relationship with prolactin [9, 11, 13]. Our findings are consistent with these previous studies for no association with number of births, age at first birth, or years since first birth (data not shown). Lactation information was not available in our dataset, but duration of breastfeeding does not appear to influence prolactin levels [11]. In Singapore, breastfeeding is prevalent with 99% of women enrolled in the National Breastfeeding Survey (n = 1,962) attempting nursing in the hospital and 42% still breastfeeding to some degree 6 months postpartum [56]. A longer time period between menarche and menopause was not associated with prolactin in the only study in which this has been evaluated [54]. Although we reported a positive relationship with prolactin for more years between menarche and first birth, the association was not independent of other reproductive characteristics including age at menarche and years between menarche and menopause.
In our data, prolactin was inversely associated with estrone, positively associated with SHBG, and positively associated with the breast cancer risk factors: younger age at menarche, longer time between menarche and first birth, and longer time between menarche and menopause. In postmenopausal women in the Nurses’ Health Study, doubling levels of prolactin and estrone sulfate, the major circulating form of estrogen in postmenopausal women [57], as well as testosterone remained in the final stepwise regression model for breast cancer risk [58]. In the same analysis, including prolactin with estrone, SHBG and testosterone improved the fit of the risk prediction model for invasive breast cancer (p value = 0.01), compared with a model based on the Gail score alone (i.e., without hormone measurements). Our findings for statistically significant, independent associations between prolactin and both estrone and SHBG are consistent with the recently reported associations between these hormones and breast cancer risk [58]. Several studies have identified SHBG to be inversely associated with breast cancer risk [59,60,61,62,63], and it is well known that estrogens increase breast cancer risk [64]. Interestingly, these two hormones interplay at the cellular level. Estrogens elicit cell growth in breast cancer cells and SHBG dampens the effect of estrogen in breast cancer cells. SHBG binds estrogen directly and inhibits its ability to bind the estrogen receptor and can instead bind its own receptor on the cell surface to elicit inhibitory functions [65]. It is therefore very interesting that SHBG is associated with prolactin levels. The molecular interplay between SHBG and prolactin has not been investigated but could represent a novel mechanism of prolactin’s ability to influence estrogen action.
No associations were observed between prolactin and soy or tea intake. Our finding for soy supports previously reported findings among Japanese premenopausal women [18]. Our rationale for evaluating possible prolactin–tea associations was based on our prior findings for lower estrogen and green tea in the Singapore cohort [23]. There are no published reports evaluating whether tea intake is related to prolactin.
Higher levels of prolactin have been observed with higher BMI among postmenopausal women in a Polish case–control study and the American Women’s Health Initiative Dietary Modification study [13, 14]. Body size characteristics including BMI, height, or weight, were not determinants of prolactin levels in our study population, or among another similarly thin Asian (Japanese) study population [15]. It is possible that the distribution of BMI in Asian population is shifted too far toward lower values to observe a relationship between high BMI and prolactin. In the current study as well as in the Japanese population, the majority of participants had a BMI < 24 or 25 (283 or 64% of the current study population, 384 or 88% of the Japanese population) [15], while in the American and Polish populations a third or less of the population had a BMI under 25 (66 or 25% in the WHI and 165 or 30% in the Polish cohort) [13, 14]. To further investigate this, we stratified our main findings by BMI (Supplemental Table S5).
A notable strength of our study is that it is the first evaluation of determinants of prolactin in a postmenopausal Asian population with historically low breast cancer risk. Limitations include the few number of nulliparous women and no lactation information. The study size was also relatively small, limiting the statistical power for some comparisons (e.g., too few women to evaluate combined effects of age at first birth with number of births). Biospecimens were not obtained at the time of the baseline interview. This could be a limitation since lifestyle factors can change drastically over that time. Given the circadian rhythm of prolactin secretion, a limitation was that prolactin was measured in blood specimens that were collected within a 7-h window (i.e., from 8 am to 2:45 pm). Ideally, specimens would have been collected at the same early morning time among all participants. Instead, we attempted to take into account the variation by time of collection by calculating adjusted geometric means (Supplementary Table S3).
In summary, we report that more years from menarche to menopause, more hours of sleep, lower estrone, and higher SHBG are independently associated with higher prolactin levels in a population-based sample of postmenopausal Chinese women in Singapore. Prolactin is associated with higher breast cancer risk in postmenopausal women. The role of prolactin in breast cancer development may involve predictors such as more years of menstrual cycling and longer duration of sleep. The observed relationship between duration of sleep and prolactin, while novel, was based on responses to a single question about average hours of sleep per day, and thus should be interpreted cautiously.
References
Perks CM, Keith AJ, Goodhew KL, Savage PB, Winters ZE, Holly JM (2004) Prolactin acts as a potent survival factor for human breast cancer cell lines. Br J Cancer 91(2):305–311. https://doi.org/10.1038/sj.bjc.6601947
Touraine P, Martini JF, Zafrani B, Durand JC, Labaille F, Malet C, Nicolas A, Trivin C, Postel-Vinay MC, Kuttenn F, Kelly PA (1998) Increased expression of prolactin receptor gene assessed by quantitative polymerase chain reaction in human breast tumors versus normal breast tissues. J Clin Endocrinol Metab 83(2):667–674. https://doi.org/10.1210/jcem.83.2.4564
Rose-Hellekant TA, Arendt LM, Schroeder MD, Gilchrist K, Sandgren EP, Schuler LA (2003) Prolactin induces ERalpha-positive and ERalpha-negative mammary cancer in transgenic mice. Oncogene 22(30):4664–4674. https://doi.org/10.1038/sj.onc.1206619
Wennbo H, Gebre-Medhin M, Gritli-Linde A, Ohlsson C, Isaksson OG, Tornell J (1997) Activation of the prolactin receptor but not the growth hormone receptor is important for induction of mammary tumors in transgenic mice. J Clin Invest 100(11):2744–2751. https://doi.org/10.1172/JCI119820
Arendt LM, Rugowski DE, Grafwallner-Huseth TA, Garcia-Barchino MJ, Rui H, Schuler LA (2011) Prolactin-induced mouse mammary carcinomas model estrogen resistant luminal breast cancer. Breast Cancer Res 13(1):R11. https://doi.org/10.1186/bcr2819
Yang N, Liu C, Peck AR, Girondo MA, Yanac AF, Tran TH, Utama FE, Tanaka T, Freydin B, Chervoneva I, Hyslop T, Kovatich AJ, Hooke JA, Shriver CD, Rui H (2013) Prolactin-Stat5 signaling in breast cancer is potently disrupted by acidosis within the tumor microenvironment. Breast Cancer Res 15(5):R73. https://doi.org/10.1186/bcr3467
Tikk K, Sookthai D, Johnson T, Rinaldi S, Romieu I, Tjonneland A, Olsen A, Overvad K, Clavel-Chapelon F, Baglietto L, Boeing H, Trichopoulou A, Lagiou P, Trichopoulos D, Palli D, Pala V, Tumino R, Rosso S, Panico S, Agudo A, Menendez V, Sanchez MJ, Amiano P, Huerta Castano JM, Ardanaz E, Bueno-de-Mesquita HB, Monninkhof E, Onland-Moret C, Andersson A, Sund M, Weiderpass E, Khaw KT, Key TJ, Travis RC, Gunter MJ, Riboli E, Dossus L, Kaaks R (2014) Circulating prolactin and breast cancer risk among pre- and postmenopausal women in the EPIC cohort. Annals of oncology: official journal of the European Society for Medical Oncology. ESMO 25(7):1422–1428. https://doi.org/10.1093/annonc/mdu150
Tworoger SS, Eliassen AH, Zhang X, Qian J, Sluss PM, Rosner BA, Hankinson SE (2013) A 20-year prospective study of plasma prolactin as a risk marker of breast cancer development. Cancer Res 73(15):4810–4819. https://doi.org/10.1158/0008-5472.CAN-13-0665
Eliassen AH, Tworoger SS, Hankinson SE (2007) Reproductive factors and family history of breast cancer in relation to plasma prolactin levels in premenopausal and postmenopausal women. Int J Cancer 120(7):1536–1541. https://doi.org/10.1002/ijc.22482
Ingram DM, Nottage EM, Roberts AN (1990) Prolactin and breast cancer risk. Med J Aust 153(8):469–473
Tikk K, Sookthai D, Johnson T, Dossus L, Clavel-Chapelon F, Tjonneland A, Olsen A, Overvad K, Baglietto L, Rinaldi S, Romieu I, Boeing H, Trichopoulou A, Lagiou P, Trichopoulos D, Masala G, Agnoli C, Tumino R, Sacerdote C, Mattiello A, Buckland G, Sanchez S, Molina-Montes E, Amiano P, Castano JM, Barricarte A, Bueno-de-Mesquita HB, Monninkhof EM, Onland-Moret NC, Idahl A, Lundin E, Weiderpass E, Lund E, Waaseth M, Khaw KT, Key TJ, Travis RC, Gunter MJ, Riboli E, Kaaks R (2014) Prolactin determinants in healthy women: A large cross-sectional study within the EPIC cohort. Cancer Epidemiol Biomark Prev 23(11):2532–2542. https://doi.org/10.1158/1055-9965.EPI-14-0613
Tworoger SS, Rice MS, Rosner BA, Feeney YB, Clevenger CV, Hankinson SE (2015) Bioactive prolactin levels and risk of breast cancer: a nested case-control study. Cancer Epidemiol Biomark Prev 24(1):73–80. https://doi.org/10.1158/1055-9965.EPI-14-0896
Faupel-Badger JM, Sherman ME, Garcia-Closas M, Gaudet MM, Falk RT, Andaya A, Pfeiffer RM, Yang XR, Lissowska J, Brinton LA, Peplonska B, Vonderhaar BK, Figueroa JD (2010) Prolactin serum levels and breast cancer: relationships with risk factors and tumour characteristics among pre- and postmenopausal women in a population-based case-control study from Poland. Br J Cancer 103(7):1097–1102. https://doi.org/10.1038/sj.bjc.6605844
McTiernan A, Wu L, Chen C, Chlebowski R, Mossavar-Rahmani Y, Modugno F, Perri MG, Stanczyk FZ, Van Horn L, Wang CY, Women’s Health Initiative I (2006) Relation of BMI and physical activity to sex hormones in postmenopausal women. Obesity 14(9):1662–1677. https://doi.org/10.1038/oby.2006.191
Nagata C, Wada K, Nakamura K, Hayashi M, Takeda N, Yasuda K (2011) Associations of body size and reproductive factors with circulating levels of sex hormones and prolactin in premenopausal Japanese women. Cancer Causes Control 22(4):581–588. https://doi.org/10.1007/s10552-011-9731-x
Brown BD, Thomas W, Hutchins A, Martini MC, Slavin JL (2002) Types of dietary fat and soy minimally affect hormones and biomarkers associated with breast cancer risk in premenopausal women. Nutr Cancer 43(1):22–30. https://doi.org/10.1207/S15327914NC431_2
Hirko KA, Spiegelman D, Barnett JB, Cho E, Willett WC, Hankinson SE, Eliassen AH (2016) Dietary patterns and plasma sex hormones, prolactin and sex hormone-binding globulin in premenopausal women. Cancer Epidemiol Biomark Prev. https://doi.org/10.1158/1055-9965.EPI-15-1019
Tsuji M, Tamai Y, Wada K, Nakamura K, Hayashi M, Takeda N, Yasuda K, Nagata C (2012) Associations of intakes of fat, dietary fiber, soy isoflavones, and alcohol with levels of sex hormones and prolactin in premenopausal Japanese women. Cancer Causes Control 23(5):683–689. https://doi.org/10.1007/s10552-012-9935-8
Bray F, McCarron P, Parkin DM (2004) The changing global patterns of female breast cancer incidence and mortality. Breast Cancer Res 6(6):229–239. https://doi.org/10.1186/bcr932
Global Burden of Disease Cancer C, Fitzmaurice C, Dicker D, Pain A, Hamavid H, Moradi-Lakeh M, MacIntyre MF, Allen C, Hansen G, Woodbrook R, Wolfe C, Hamadeh RR, Moore A, Werdecker A, Gessner BD, Te Ao B, McMahon B, Karimkhani C, Yu C, Cooke GS, Schwebel DC, Carpenter DO, Pereira DM, Nash D, Kazi DS, De Leo D, Plass D, Ukwaja KN, Thurston GD, Yun Jin K, Simard EP, Mills E, Park EK, Catala-Lopez F, deVeber G, Gotay C, Khan G, Hosgood HD, 3rd, Santos IS, Leasher JL, Singh J, Leigh J, Jonas JB, Sanabria J, Beardsley J, Jacobsen KH, Takahashi K, Franklin RC, Ronfani L, Montico M, Naldi L, Tonelli M, Geleijnse J, Petzold M, Shrime MG, Younis M, Yonemoto N, Breitborde N, Yip P, Pourmalek F, Lotufo PA, Esteghamati A, Hankey GJ, Ali R, Lunevicius R, Malekzadeh R, Dellavalle R, Weintraub R, Lucas R, Hay R, Rojas-Rueda D, Westerman R, Sepanlou SG, Nolte S, Patten S, Weichenthal S, Abera SF, Fereshtehnejad SM, Shiue I, Driscoll T, Vasankari T, Alsharif U, Rahimi-Movaghar V, Vlassov VV, Marcenes WS, Mekonnen W, Melaku YA, Yano Y, Artaman A, Campos I, MacLachlan J, Mueller U, Kim D, Trillini M, Eshrati B, Williams HC, Shibuya K, Dandona R, Murthy K, Cowie B, Amare AT, Antonio CA, Castaneda-Orjuela C, van Gool CH, Violante F, Oh IH, Deribe K, Soreide K, Knibbs L, Kereselidze M, Green M, Cardenas R, Roy N, Tillmann T, Li Y, Krueger H, Monasta L, Dey S, Sheikhbahaei S, Hafezi-Nejad N, Kumar GA, Sreeramareddy CT, Dandona L, Wang H, Vollset SE, Mokdad A, Salomon JA, Lozano R, Vos T, Forouzanfar M, Lopez A, Murray C, Naghavi M (2015) The Global Burden of Cancer 2013. JAMA Oncol 1(4):505–527. https://doi.org/10.1001/jamaoncol.2015.0735
Yuan JM, Stram DO, Arakawa K, Lee HP, Yu MC (2003) Dietary cryptoxanthin and reduced risk of lung cancer: the Singapore Chinese Health Study. Cancer Epidemiol Biomark Prev 12(9):890–898
Hankin JH, Stram DO, Arakawa K, Park S, Low SH, Lee HP, Yu MC (2001) Singapore Chinese Health Study: development, validation, and calibration of the quantitative food frequency questionnaire. Nutr Cancer 39(2):187–195
Wu AH, Arakawa K, Stanczyk FZ, Van Den Berg D, Koh WP, Yu MC (2005) Tea and circulating estrogen levels in postmenopausal Chinese women in Singapore. Carcinogenesis 26(5):976–980. https://doi.org/10.1093/carcin/bgi028
Reding KW, Lampe JW, Wang CY, Stanczyk FZ, Ulrich CM, Xiao L, Duggan CR, McTiernan A (2011) A 12-month moderate-intensity exercise intervention does not alter serum prolactin concentrations. Cancer Epidemiol 35(6):569–573. https://doi.org/10.1016/j.canep.2011.01.006
Goebelsmann U, Horton R, Mestman JH, Arce JJ, Nagata Y, Nakamura RM, Thorneycroft IH, Mishell DR Jr (1973) Male pseudohermaphroditism due to testicular 17-hydroxysteroid dehydrogenase deficiency. J Clin Endocrinol Metab 36(5):867–879
Stanczyk FZ, Shoupe D, Nunez V, Macias-Gonzales P, Vijod MA, Lobo RA (1988) A randomized comparison of nonoral estradiol delivery in postmenopausal women. Am J Obstet Gynecol 159(6):1540–1546
Wu AH, Stanczyk FZ, Seow A, Lee HP, Yu MC (2002) Soy intake and other lifestyle determinants of serum estrogen levels among postmenopausal Chinese women in Singapore. Cancer Epidemiol Biomark Prev 11 (9):844–851
Sodergard R, Backstrom T, Shanbhag V, Carstensen H (1982) Calculation of free and bound fractions of testosterone and estradiol-17 beta to human plasma proteins at body temperature. J Steroid Biochem 16(6):801–810
Rinaldi S, Dechaud H, Toniolo P, Kaaks R (2002) Reliability and validity of direct radioimmunoassays for measurement of postmenopausal serum androgens and estrogens. IARC Sci Publ 156:323–325
Arnal PJ, Drogou C, Sauvet F, Regnauld J, Dispersyn G, Faraut B, Millet GY, Leger D, Gomez-Merino D, Chennaoui M (2016) Effect of sleep extension on the subsequent testosterone, cortisol and prolactin responses to total sleep deprivation and recovery. J Neuroendocrinol 28(2):12346. https://doi.org/10.1111/jne.12346
Baumgartner A, Graf KJ, Kurten I, Meinhold H, Scholz P (1990) Neuroendocrinological investigations during sleep deprivation in depression. I. Early morning levels of thyrotropin, TH, cortisol, prolactin, LH, FSH, estradiol, and testosterone. Biol Psychiatry 28(7):556–568
Ebert D, Kaschka W, Stegbauer P, Schrell U (1993) Prolactin response to sulpiride before and after sleep deprivation in depression. Biol Psychiatry 33(8–9):666–669
Parry BL, Hauger R, LeVeau B, Mostofi N, Cover H, Clopton P, Gillin JC (1996) Circadian rhythms of prolactin and thyroid-stimulating hormone during the menstrual cycle and early versus late sleep deprivation in premenstrual dysphoric disorder. Psychiatry Res 62(2):147–160
Kuhs H, Farber D, Tolle R (1996) Serum prolactin, growth hormone, total corticoids, thyroid hormones and thyrotropine during serial therapeutic sleep deprivation. Biol Psychiatry 39(10):857–864. https://doi.org/10.1016/0006-3223(95)00240-5
Baumgartner A, Riemann D, Berger M (1990) Neuroendocrinological investigations during sleep deprivation in depression. II. Longitudinal measurement of thyrotropin, TH, cortisol, prolactin, GH, and LH during sleep and sleep deprivation. Biol Psychiatry 28(7):569–587
He C, Anand ST, Ebell MH, Vena JE, Robb SW (2015) Circadian disrupting exposures and breast cancer risk: a meta-analysis. Int Arch Occup Environ Health 88(5):533–547. https://doi.org/10.1007/s00420-014-0986-x
Lin X, Chen W, Wei F, Ying M, Wei W, Xie X (2015) Night-shift work increases morbidity of breast cancer and all-cause mortality: a meta-analysis of 16 prospective cohort studies. Sleep Med 16(11):1381–1387. https://doi.org/10.1016/j.sleep.2015.02.543
Hurley S, Goldberg D, Bernstein L, Reynolds P (2015) Sleep duration and cancer risk in women. Cancer Causes Control 26(7):1037–1045. https://doi.org/10.1007/s10552-015-0579-3
McElroy JA, Newcomb PA, Titus-Ernstoff L, Trentham-Dietz A, Hampton JM, Egan KM (2006) Duration of sleep and breast cancer risk in a large population-based case-control study. J Sleep Res 15(3):241–249. https://doi.org/10.1111/j.1365-2869.2006.00523.x
Pinheiro SP, Schernhammer ES, Tworoger SS, Michels KB (2006) A prospective study on habitual duration of sleep and incidence of breast cancer in a large cohort of women. Cancer Res 66(10):5521–5525. https://doi.org/10.1158/0008-5472.CAN-05-4652
Vogtmann E, Levitan EB, Hale L, Shikany JM, Shah NA, Endeshaw Y, Lewis CE, Manson JE, Chlebowski RT (2013) Association between sleep and breast cancer incidence among postmenopausal women in the Women’s Health Initiative. Sleep 36(10):1437–1444. https://doi.org/10.5665/sleep.3032
Girschik J, Heyworth J, Fritschi L (2013) Self-reported sleep duration, sleep quality, and breast cancer risk in a population-based case-control study. Am J Epidemiol 177(4):316–327. https://doi.org/10.1093/aje/kws422
Qian X, Brinton LA, Schairer C, Matthews CE (2015) Sleep duration and breast cancer risk in the Breast Cancer Detection Demonstration Project follow-up cohort. Br J Cancer 112(3):567–571. https://doi.org/10.1038/bjc.2014.600
Verkasalo PK, Lillberg K, Stevens RG, Hublin C, Partinen M, Koskenvuo M, Kaprio J (2005) Sleep duration and breast cancer: a prospective cohort study. Cancer Res 65(20):9595–9600. https://doi.org/10.1158/0008-5472.CAN-05-2138
Wu AH, Stanczyk FZ, Wang R, Koh WP, Yuan JM, Yu MC (2013) Sleep duration, spot urinary 6-sulfatoxymelatonin levels and risk of breast cancer among Chinese women in Singapore. Int J Cancer 132(4):891–896. https://doi.org/10.1002/ijc.27653
Wu AH, Wang R, Koh WP, Stanczyk FZ, Lee HP, Yu MC (2008) Sleep duration, melatonin and breast cancer among Chinese women in Singapore. Carcinogenesis 29(6):1244–1248. https://doi.org/10.1093/carcin/bgn100
Roelfsema F, Pijl H, Keenan DM, Veldhuis JD (2012) Prolactin secretion in healthy adults is determined by gender, age and body mass index. PLoS ONE 7(2):e31305. https://doi.org/10.1371/journal.pone.0031305
von Treuer K, Norman TR, Armstrong SM (1996) Overnight human plasma melatonin, cortisol, prolactin, TSH, under conditions of normal sleep, sleep deprivation, and sleep recovery. J Pineal Res 20(1):7–14
Chavez-MacGregor M, van Gils CH, van der Schouw YT, Monninkhof E, van Noord PA, Peeters PH (2008) Lifetime cumulative number of menstrual cycles and serum sex hormone levels in postmenopausal women. Breast Cancer Res Treat 108(1):101–112. https://doi.org/10.1007/s10549-007-9574-z
Endogenous H, Breast Cancer Collaborative G, Key TJ, Appleby PN, Reeves GK, Roddam AW, Helzlsouer KJ, Alberg AJ, Rollison DE, Dorgan JF, Brinton LA, Overvad K, Kaaks R, Trichopoulou A, Clavel-Chapelon F, Panico S, Duell EJ, Peeters PH, Rinaldi S, Fentiman IS, Dowsett M, Manjer J, Lenner P, Hallmans G, Baglietto L, English DR, Giles GG, Hopper JL, Severi G, Morris HA, Hankinson SE, Tworoger SS, Koenig K, Zeleniuch-Jacquotte A, Arslan AA, Toniolo P, Shore RE, Krogh V, Micheli A, Berrino F, Barrett-Connor E, Laughlin GA, Kabuto M, Akiba S, Stevens RG, Neriishi K, Land CE, Cauley JA, Lui LY, Cummings SR, Gunter MJ, Rohan TE, Strickler HD (2011) Circulating sex hormones and breast cancer risk factors in postmenopausal women: reanalysis of 13 studies. Br J Cancer 105(5):709–722. https://doi.org/10.1038/bjc.2011.254
Chavez-MacGregor M, Elias SG, Onland-Moret NC, van der Schouw YT, Van Gils CH, Monninkhof E, Grobbee DE, Peeters PH (2005) Postmenopausal breast cancer risk and cumulative number of menstrual cycles. Cancer Epidemiol Biomark Prev 14(4):799–804. https://doi.org/10.1158/1055-9965.EPI-04-0465
Clavel-Chapelon F, Group EN (2002) Cumulative number of menstrual cycles and breast cancer risk: results from the E3N cohort study of French women. Cancer Causes Control 13(9):831–838
Wu AH, Vigen C, Lee E, Tseng CC, Butler LM (2016) Traditional Breast Cancer Risk Factors in Filipina Americans Compared with Chinese and Japanese Americans in Los Angeles County. Cancer Epidemiol Biomark Prev 25(12):1572–1586. https://doi.org/10.1158/1055-9965.EPI-16-0203
Wang DY, de Stavola BL, Bulbrook RD, Allen DS, Kwa HG, Verstraeten AA, Moore JW, Fentiman IS, Hayward JL, Gravelle IH (1988) The permanent effect of reproductive events on blood prolactin levels and its relation to breast cancer risk: a population study of postmenopausal women. Eur J Cancer Clin Oncol 24(7):1225–1231
Crowley WR (2015) Neuroendocrine regulation of lactation and milk production. Compr Physiol 5(1):255–291. https://doi.org/10.1002/cphy.c140029
Chua L, Win AM (2013) Prevalence of breastfeeding in Singapore. Stat Singap Newsl. https://www.singstat.gov.sg/docs/default-source/default-documentlibrary/publications/newsletter/archive/ssnsep2013.pdf
Pasqualini JR (2004) The selective estrogen enzyme modulators in breast cancer: a review. Biochim Biophys Acta 1654(2):123–143. https://doi.org/10.1016/j.bbcan.2004.03.001
Tworoger SS, Zhang X, Eliassen AH, Qian J, Colditz GA, Willett WC, Rosner BA, Kraft P, Hankinson SE (2014) Inclusion of endogenous hormone levels in risk prediction models of postmenopausal breast cancer. J Clin Oncol 32(28):3111–3117. https://doi.org/10.1200/JCO.2014.56.1068
Duggan C, Stanczyk F, Campbell K, Neuhouser ML, Baumgartner RN, Baumgartner KB, Bernstein L, Ballard R, McTiernan A (2016) Associations of sex steroid hormones with mortality in women with breast cancer. Breast Cancer Res Treat 155(3):559–567. https://doi.org/10.1007/s10549-016-3704-4
Fourkala EO, Blyuss O, Field H, Gunu R, Ryan A, Barth J, Jacobs I, Zaikin A, Dawnay A, Menon U (2016) Sex hormone measurements using mass spectrometry and sensitive extraction radioimmunoassay and risk of estrogen receptor negative and positive breast cancer: case control study in UK Collaborative Cancer Trial of Ovarian Cancer Screening (UKCTOCS). Steroids 110:62–69. https://doi.org/10.1016/j.steroids.2016.04.003
Husing A, Fortner RT, Kuhn T, Overvad K, Tjonneland A, Olsen A, Boutron-Ruault MC, Severi G, Fournier A, Boeing H, Trichopoulou A, Benetou V, Orfanos P, Masala G, Pala V, Tumino R, Fasanelli F, Panico S, Bueno de Mesquita HB, Peeters PH, van Gills CH, Quiros JR, Agudo A, Sanchez MJ, Chirlaque MD, Barricarte A, Amiano P, Khaw KT, Travis RC, Dossus L, Li K, Ferrari P, Merritt MA, Tzoulaki I, Riboli E, Kaaks R (2017) Added value of serum hormone measurements in risk prediction models for breast cancer for women not using exogenous hormones: results from the EPIC cohort. Clin Cancer Res 23(15):4181–4189. https://doi.org/10.1158/1078-0432.CCR-16-3011
Key T, Appleby P, Barnes I, Reeves G, Endogenous H, Breast Cancer Collaborative G (2002) Endogenous sex hormones and breast cancer in postmenopausal women: reanalysis of nine prospective studies. J Natl Cancer Inst 94(8):606–616
Thaler MA, Seifert-Klauss V, Luppa PB (2015) The biomarker sex hormone-binding globulin—from established applications to emerging trends in clinical medicine. Best Pract Res Clin Endocrinol Metab 29(5):749–760. https://doi.org/10.1016/j.beem.2015.06.005
Hankinson SE, Willett WC, Manson JE, Colditz GA, Hunter DJ, Spiegelman D, Barbieri RL, Speizer FE (1998) Plasma sex steroid hormone levels and risk of breast cancer in postmenopausal women. J Natl Cancer Inst 90(17):1292–1299
Fortunati N, Catalano MG, Boccuzzi G, Frairia R (2010) Sex hormone-binding globulin (SHBG), estradiol and breast cancer. Mol Cell Endocrinol 316(1):86–92. https://doi.org/10.1016/j.mce.2009.09.012
Acknowledgments
We thank Ms. Siew Hong Low of the National University of Singapore for supervising the field work of the Singapore Chinese Health Study. Dr. Katz was a post-doctoral fellow in the Translational Research Training in Cancer Etiology and Prevention Program funded by National Cancer Institute (T32 CA186873).
Funding
This study was funded through grants from the US National Institutes of Health: T32 CA186873, R01 CA144034, UM1 CA182876, and R01 CA160746.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Katz, T.A., Wu, A.H., Stanczyk, F.Z. et al. Determinants of prolactin in postmenopausal Chinese women in Singapore. Cancer Causes Control 29, 51–62 (2018). https://doi.org/10.1007/s10552-017-0978-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10552-017-0978-8