
Abstract
Behavioral interventions remain the preferred strategy for reducing HIV-related risk behavior among men who have sex with men (MSM), one of the populations most affected by HIV. To improve intervention efforts, research is needed to identify cognitive-motivational factors that may play a role in sexual risk behaviors among MSM. This study sought to replicate and extend previous work from a heterosexual population that identified a serial mediation effect of perceived intoxication and subjective sexual arousal in the relationship between alcohol consumption and determinants of sexual risk in a population of MSM. Exploratory moderated mediation analyses tested subjective sexual arousal as a moderator of the indirect effect of alcohol consumption on determinants of sexual risk via perceived intoxication. Participants (N = 117 MSM, ages 21–50) were randomly assigned to one of six experimental conditions based on two manipulations: beverage condition (alcohol, placebo, or control) and sexual arousal (low or high). Dependent measures were likelihood to engage in risky sex and condom negotiation skills. Results did not support the serial mediation effect but showed some support for the moderated mediation model in the prediction of behavioral skills. Implications for alcohol and arousal myopia theories of risky behavior and HIV prevention efforts are discussed.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Sexual Risk Among Men Who Have Sex with Men
While public health research has documented a decline in rates of new HIV diagnoses overall in recent years, rates of HIV diagnoses attributable to male-to-male sexual contact have remained steady, and in some age groups, have increased [1]. Men who have sex with men (MSM) continue to be the subgroup in the U.S. that is most affected by HIV. As there continues to be no medical cure or effective vaccine, behavioral prevention efforts to reduce high risk sexual behavior remain an important approach to reducing the incidence of HIV infections [2]. Specifically, the promotion of safer sex practices among those at risk for HIV is an often-employed behavioral intervention strategy [3]. In addition to being at elevated risk for HIV infection, MSM also tend to be heavier drinkers than matched heterosexual groups [4]. Therefore, research on the role of concurrent alcohol use and risky sexual behavior is necessary in order to optimize the efficacy of behavioral interventions.
Alcohol Consumption and Risky Sex
Findings from several meta-analyses of the literature on global associations between alcohol consumption and sexual risk have revealed that alcohol consumption, including problematic drinking, binge drinking, and alcohol use in sexual contexts, is significantly and positively associated with greater engagement in sexual risk behaviors (e.g., unprotected sex) and a greater risk for HIV infection [5, 6]. However, results from event level studies, in which data on alcohol consumption and risky sexual behavior are gathered at the level of the sexual event, have been inconsistent [for reviews, see 7, 8]. The literature also includes experimental alcohol administration studies that have helped considerably to clarify whether alcohol consumption and sexual risk are causally related.
Experimental designs are crucial to determining causality in the relationship between alcohol consumption and sexual risk behavior but are ethically limited to assessing determinants of sexual risk behavior (e.g., decreased risk perception, poorer condom negotiation skills, greater intentions to engage in risky sex) rather than sexual risk behavior. To date, most experimental studies investigating alcohol consumption and determinants of risky sexual behavior have been conducted in heterosexual populations. Results from these studies have demonstrated that alcohol consumption is associated with decreased risk perception, poorer condom negotiation skills, and greater intentions to engage in risky sex [9, 10]. In the first experimental alcohol administration study conducted among MSM, Maisto, Palfai, Vanable, Heath and Woolf-King [11] reported similar negative effects of alcohol administration on condom negotiation skills, although other determinants of sexual risk (e.g., intentions to engage in unprotected anal intercourse) were unaffected by alcohol consumption. Overall, results from this line of work suggest a causal relationship between acute alcohol consumption and at least some determinants of sexual risk behavior, such that alcohol consumption increases determinants of sexual risk behavior. As such, experimental research has more recently focused on identifying the mechanisms that underlie the relationship between alcohol and determinants of risky sex.
Sexual Arousal, Alcohol Consumption, and Risky Sex
Loewenstein [12] proposed a model to explain instances in which behavior appears to contradict long-term self-interest. The model proposes that visceral factors, which include emotion and sexual arousal, influence behavior by increasing the desirability of immediately reinforcing behaviors, often at the expense of long-term goals or values [12]. This interpretation has been applied specifically to risk perception; the “risk as feelings” model suggests that visceral factors can influence cognitive appraisal of a situation, and in some cases, override cognition altogether to have a direct effect on behavior [13]. Empirical research supports the influence of arousal on risk perception as demonstrated by less perceived risk [14], decreased likelihood of using a condom [15], and greater intentions to engage in risky sex [16] under conditions of heightened sexual arousal.
Sexual arousal may independently be related to risky sexual behavior, and its interaction with alcohol may also be of importance in attempting to explain the relationship between alcohol consumption and risky sexual behavior. The alcohol myopia model [17] is often cited in explanations of behavior under alcohol intoxication, particularly when the behavior appears to contradict an individual’s long-term interests. As in theories of sexual arousal and risky sexual behavior [12, 13], the alcohol myopia model proposes that alcohol’s pharmacological properties affect cognitive capacity such that an individual’s ability to process complex environmental stimuli is compromised. As a result, cues that are immediately reinforcing are more salient to individuals when they are under the influence of alcohol. Both sexual arousal and alcohol consumption are theorized to affect complex decision-making by biasing perception towards those stimuli that are immediately reinforcing. Therefore, the interaction between sexual arousal and alcohol consumption may explain the occurrence of risky sexual behavior in situations in which alcohol is present and sexual activity is a possibility.
Several studies investigating the combined effect of alcohol and sexual arousal lend empirical support to the combined alcohol/arousal myopia interpretation. Studies in heterosexual populations showed that participants in a sexual arousal condition who consumed alcohol reported greater intentions to engage in unprotected sex than participants in control conditions [18, 19]. Furthermore, the effect of alcohol consumption on intentions to engage in unprotected sex was mediated by subjective sexual arousal [20, 21] and attention to arousal cues [22]. Similarly, exploratory analyses in the first study of alcohol administration and sexual arousal in MSM reported an alcohol by subjective sexual arousal interaction on intentions to engage in risky sex, such that those who consumed alcohol and reported higher subjective sexual arousal also reported greater intentions to engage in risky sex [11]. In sum, both alcohol and subjective sexual arousal appear to affect determinants of risky sexual behavior, and their interaction may be particularly relevant in situations in which alcohol is present and sexual activity is a possibility.
Perceived Intoxication and Risky Sex
Research has long demonstrated the importance of perceived intoxication in determining drinking behavior, including craving for alcohol [23] and ad libitum alcohol consumption [24]. Additionally, research has established an association between perceived intoxication and both sexual arousal and determinants of sexual risk behavior. Results from one study suggest that males who believed they consumed alcohol reported significantly greater subjective sexual arousal than those who believed they had not consumed alcohol, regardless of the actual alcohol content consumed [25]. These results were not replicated in a sample of female participants [26]; however, more recent research found that perceived intoxication was negatively associated with condom negotiation skills in heterosexual women [27, 28]. Similarly, Davis and colleagues [29] reported a serial mediation effect of alcohol consumption on intentions to engage in risky sexual behavior via perceived intoxication and subjective sexual arousal in a heterosexual population, such that alcohol consumption led to increases in perceived intoxication and subjective sexual arousal, thereby increasing intentions to engage in risky sexual behavior. Overall, research supports relationships among alcohol consumption, perceived intoxication, sexual arousal, and determinants of risky sexual behavior. However, further research is needed to investigate these relationships in a population for whom alcohol consumption and risky sexual behavior are of particular importance, MSM.
Sex and Sexual Orientation Differences in Sexual Response
Research has consistently demonstrated differences in sexual response based on sex [30,31,32] and sexual orientation [31, 33]. Additionally, differences in cognitive processing based on both gender and sexual orientation [34,35,36] have a well-established history in the literature. Sex and sexual orientation differences are often explained via theories of both neurobiological [37] and psychosocial factors [38], although it remains unclear how biological and psychosocial factors interact to affect sex and sexual orientation differences in sexual response and cognition [39]. Sex and sexual orientation differences in sexual response and cognitive processing [31, 37,38,39] suggest that findings on the effect of alcohol administration on sexual risk behavior, including mediators of this relationship [e.g., 29] in heterosexual men and women may differ among MSM. In particular, Rupp and Wallen [32] specify that differences in the cognitive processing of sexual stimuli may ultimately account for observed differences in sexual response. As such, research on cognitive processes involved in alcohol intoxication, arousal, and sexual risk among MSM are warranted, as differences from previous studies based on either sex or sexual orientation are possible.
Aims and Hypotheses
The purpose of this study was to replicate Davis and colleagues’ [29] serial mediation model of the relationship between alcohol consumption and determinants of risky sexual behaviors via perceived intoxication and subjective sexual arousal from a heterosexual population and extend the findings to an MSM population. It was hypothesized that perceived intoxication and subjective sexual arousal would serially mediate the relationship between alcohol consumption and sexual risk behaviors, such that increases in perceived intoxication and subjective sexual arousal would be associated with a higher likelihood of engaging in unprotected anal intercourse (UAI) and poorer condom negotiation skills. The current analyses were completed using data from the study by [11], an experimental alcohol administration study that examined the effects of alcohol and subjective sexual arousal on determinants of sexual risk behavior in MSM.
Research primarily has been designed to test sexual arousal as a mediator [e.g., 20, 21, 29]. However, sexual arousal may also act as a moderator, such that the effects of alcohol consumption and/or perceived intoxication may be most prominent when sexual arousal is high [40]. In other words, subjective sexual arousal may not simply be a response to the pharmacological effects of alcohol and one’s perceived level of intoxication; rather, for those who are highly aroused, alcohol may increase sexual risk via perceived intoxication. Exploratory analyses were conducted to evaluate a second-stage moderated mediation model [41], in which subjective sexual arousal moderates the effect of alcohol consumption on determinants of risky sexual behavior via perceived intoxication. Given that research has not yet tested subjective sexual arousal as a moderator, the second-stage moderated mediation model was considered exploratory and no a priori hypothesis was determined.
Method
Participants and Procedures
Detailed information on the methods for this study is provided in [11]. Participants were 117 MSM recruited from Syracuse, NY (n = 31) and Boston, MA (n = 86). Inclusion criteria included being 21-50 years of age, having a history of sexual activity with other men, being sexually active in the past year, and being moderate to heavy alcohol drinkers based on the Quantity-Frequency-Variability Index [QFV; 42]. Exclusion criteria included being in a committed relationship in the past 3 months, current or history of alcohol use disorder or other psychiatric disorders, and medical problems that contraindicated the consumption of alcohol (e.g., HIV, liver disorders, diabetes). Informed consent was obtained from all individual participants included in the study.
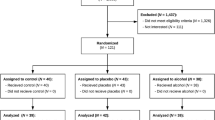
Of the 366 men screened for participation, 171 were considered eligible after an initial phone interview. Those eligible after the initial phone session were scheduled for an in-person screening session to determine final eligibility. Of the 171 men who participated in the in-person screening session, 53 did not complete the experimental session due to ineligibility (n = 44) or failure to return for follow-up (n = 9). Completers and non-completers were compared on a number of relevant variables (listed in Table 1). No significant differences were found except for age; completers were slightly younger than non-completers.
Eligible participants were randomly assigned to one of six experimental conditions formed by the combination of beverage (alcohol, placebo, control) and arousal (arousal, neutral) manipulations. During the experimental session a research assistant (research assistant 1) administered beverages according to each participant’s randomized beverage condition. Participants in the alcohol condition received 0.70 g alcohol/kg body weight in a mixture of 80-proof vodka, tonic water and lime juice in a 1:4 ratio. Participants in the placebo group received beverages containing tonic water and lime juice, with a vodka-soaked limes added and a minimal amount of vodka rubbed on the rim of the glass to enhance alcohol cues. The volume of the placebo and alcohol beverages were equivalent. Participants in the control condition were given water, in a comparable amount as the beverage given to participants in the alcohol or placebo conditions. Participants in the alcohol and placebo conditions were instructed that they would be consuming alcohol and participants in the control condition were told they would not be consuming alcohol. Drinks were divided into three doses, and participants were given 20 min to finish their beverages.
After the beverages had been administered, a second research assistant blind to beverage condition (research assistant 2) administered the arousal manipulation, per procedures established by Woolf-King and colleagues [43]. Erotic clips were designed to elicit a moderate level of arousal. Research assistant 2 left the room while participants watched the 6-min film clips. Research assistant 2 then asked participants to complete subjective effects ratings on subjective sexual arousal.
After ratings were completed, research assistant 2 left the room, and research assistant 1 returned to complete manipulation checks and provide feedback to participants about their BAC. Participants in the alcohol condition were told their actual BAC, participants in the placebo condition were told the BAC of a randomly selected participant in the alcohol condition, and participants in the control condition were told their actual BAC (zero). Research assistant 1 then asked participants to complete ratings of perceived intoxication.
Research assistant 2 administered the behavioral skills measures. Behavioral condom negotiation skills were measured via participants’ responses to two interactive videos that portrayed sexual situations (for more detail, refer to the measures section). Order of administration of the two videos was randomly determined for each participant, and participants’ responses were digitally recorded. After responses to both videos had been completed, participants completed a set of ratings of their likelihood of UAI. After completing the ratings, participants in the alcohol condition were breath tested every 15 min until their BAC was ≤ 0.02%, after which they were debriefed and permitted to leave the laboratory. Participants were paid $35 upon completion of session 2, and $15 for transportation.
Table I presents descriptive information for participants by experimental condition. All conditions had n = 19 except for the placebo/arousal (n = 20) and control/non-arousal (n = 21) conditions. Analyses of variance (ANOVAs; continuous variables) and χ2 tests (categorical variables) revealed no significant differences between groups on any of the Table 1 variables. Differences in descriptive variables were also tested based on site and found to differ only on age (t (114) = 2.17, p < .05), as participants recruited from Syracuse were older (M = 34.2 years, SD = 9.6) than those recruited from Boston (M = 30.5 years, SD = 9.0).
Measures
Predictor Variables
Perceived Intoxication
Perceived intoxication was assessed using a single-item measure administered after both the arousal and alcohol manipulations. Participants rated their perceived intoxication on a 10-point Likert scale, ranging from 1 (not at all) to 10 (more intoxicated than you’ve ever been). Manipulation checks performed in the parent study [11] support the validity of the perceived intoxication measure in this study as ratings of perceived intoxication in the alcohol (M = 5.00, SD = 1.79 and placebo (M = 2.56, SD = 1.14) conditions were higher than those in the control condition (M = 1.07, SD = 0.62).
Subjective Sexual Arousal
Subjective sexual arousal was assessed using a single-item measure administered after the arousal manipulation. Participants rated their subjective sexual arousal on a scale ranging from 0 (not at all) to 6 (extremely). Manipulation checks performed in the parent study [11] support the validity of the subjective sexual arousal measure in this study as ratings of arousal in the arousal condition (M = 2.86, SD = 1.43) were higher than those in the neutral condition (M = 0.29, SD = 0.67).
Dependent Variables
Behavioral Skills
Behavioral skills were measured using two interactive videos developed for this study according to the procedures detailed in [43]. The first interactive video showed two men who had recently met and were discussing the possibility of having sexual intercourse for the first time, without condoms. The second video portrayed two men who were friends deciding if they would use condoms during their first sexual encounter together. Professional actors played the parts of the two men according to a script, and professional videographers filmed the videos.
Behavioral skills were indicated by participants’ ability to successfully navigate the sexual encounters represented in the videos. Participants were asked to respond to prompts at certain decision points during the videos. Prompt 1 asked participants to respond to the video character (Jim) when he expressed a desire to have unprotected anal intercourse (UAI) and that there was no cause for concern because he was safe. Prompt 2 asked participants to respond to Jim’s second, more persistent statement that UAI would be safe and pleasurable, and that the participant could trust Jim. After each prompt, the video paused for 60 s to allow for the participant’s response. Participants spoke into a microphone next to the computer, and responses were digitally recorded.
Responses were scored on a 0–2 scale on five different dimensions: (1) use of an “I” statement of intention of safer sexual behavior or refusal of unsafe sexual behavior; (2) presence of a positive statement about the other person in the scenario; (3) provision of a statement of a reason for safer sexual behavior; (4) suggestion of a specific, safer, alternative behavior; (5) indications that the participant’s response was direct, serious, and clear. Higher scores on these dimensions indicated better communication and behavioral skills. Ratings for each dimension were summed to form a total behavioral skills score for each prompt. Criteria for scoring responses are specified in the rating manual developed through previous research by our team [27, 28]. Responses were scored independently by two raters, who were in agreement on 93% of the codes. Discrepancies were resolved through discussion.
Intentions
Intentions to engage in UAI were assessed using a single-item measure after each of the interactive videos. Following the interactive videos, participants were asked “How likely is it that you would have anal sex without a condom if you were actually in the situation depicted in the interactive video?” Participants rated the likelihood of their engaging in UAI on a 0 (not at all) to 6 (extremely likely) Likert-type scale. This rating is similar to ratings of “intention to have unprotected sex” [20], and similar single-item assessments of likelihood of engaging in unprotected sex have demonstrated their sensitivity to the effects of alcohol in previous research among heterosexual populations [22, 44].
Data Analysis Strategy
Descriptive statistics were computed to characterize sample demographics. Distributions of all continuous variables were examined, and transformations were computed and substituted for the original variables to increase normality as appropriate. Previous analyses of covariance [11] showed that placebo and control alcohol conditions did not differ on any of the dependent variables, therefore, in the current analyses the placebo and control conditions were combined. Following procedures established in previous research by our team [28], the likelihood of UAI ratings for each of the two videos were combined to form a single score for this measure.
Serial mediation models using path analysis were conducted in Mplus version 7 using the model indirect command. These models tested the serial mediation effect of perceived intoxication and subjective sexual arousal in the relationship between beverage condition and indicators of sexual risk (e.g., behavioral skills 1 and 2, and likelihood of UAI). Significance tests for the mediation effects were conducted via both Sobel first-order tests and 95% bootstrapped Confidence Intervals (CIs) based on 1,000 resamples. The effect of age was controlled for in the model. The model was specified such that the dependent variables were regressed on mediator 2 (subjective sexual arousal), mediator 1 (perceived intoxication), the independent variable (beverage condition) and the covariate (age). Additionally, mediator 2 (subjective sexual arousal) was regressed onto mediator 1 (perceived intoxication) and the independent variable (beverage condition), and mediator 1 (perceived intoxication) was regressed onto the independent variable (beverage) and covariate (age).
The exploratory second-stage moderated mediation models [41, 45] were tested using the PROCESS macro [45] in SPSS version 22. Significance tests for direct and indirect effects were conducted using 95% bootstrapped CIs based on 10,000 resamples. The conditional indirect effect (i.e., moderated mediation) was tested based on both normal theory tests of the indirect effect at different levels of the moderator (i.e., +1 SD above the mean, mean, and − 1 SD below the mean) and 95% bootstrapped CIs of the index of moderated mediation [46, 47]. Normal theory tests indicate if indirect effects at different levels of the moderator are significantly different from zero [46], and the index of moderated mediation indicates if the indirect effects at different levels of the moderator significantly differ from each other [47]. Evidence of moderated mediation is suggested by (1) a significant effect of the independent variable on the mediator (i.e., beverage condition on perceived intoxication), (2) a significant interaction between the mediator and moderator (i.e., perceived intoxication and subjective sexual arousal), and (3) a significant index of moderated mediation [47]. The effect of age was controlled for in the models, and perceived intoxication and subjective sexual arousal were mean-centered [48].
Results
Preliminary Analyses
Table I presents sample characteristics by alcohol and arousal condition. As in previous studies by our group [28], the behavioral skills prompts were significantly correlated (r = 0.68, p < 0.001). Neither behavioral skills measure was significantly correlated with the UAI measure (p’s > 0.05). The likelihood of UAI measure was log-transformed to reduce skewness, and the perceived intoxication and subjective sexual arousal variables were centered prior to performing analyses. All other variables were approximately normally distributed.
Manipulation Checks
The average peak BAC of participants in the alcohol/arousal condition was 0.068% (.016) and 0.061% (.019) in the alcohol/neutral condition, which did not differ statistically.
A one-way ANOVA was performed to test differences between alcohol groups on perceived intoxication ratings. Analyses revealed a significant main effect of beverage (F (2,114) = 95.30, p < .001) on perceived intoxication, such that alcohol consumption was associated with greater perceived intoxication. Means (standard deviations) for the control, placebo, and alcohol conditions were 1.07 (0.62), 2.56 (1.14), and 5.00 (1.79), respectively. Each group’s rating of perceived intoxication was statistically different (p’s < .01) from the other two groups in the expected direction.
An independent-samples t test was performed to test differences between arousal groups on subjective arousal ratings after viewing the film clip. Results showed significant differences (t (115) = 12.42, p < .001) in subjective arousal ratings between the arousal condition (M = 2.86, SD = 1.43) and neutral condition (M = 0.29, SD = 0.67) after viewing the film.
Serial Mediation Analyses
Figure 1 shows standardized coefficients from the path analysis of the serial mediation effect of perceived intoxication and subjective sexual arousal on the relationship between beverage condition and skills 2, with significant paths bolded. Similar patterns of results were found in the models predicting skills 1 and UAI. Age was controlled for in the model, but not included in the diagram for simplicity. For skills 2, the model accounted for 17% of the variance in skills 2, 8% of the variance in subjective sexual arousal, and 62% of the variance in perceived intoxication. For skills 1, the model accounted for 16% of the variance in skills 1, 8% of the variance in subjective sexual arousal, and 62% of the variance in perceived intoxication. For UAI, the model accounted for 20% of the variance in UAI, 10% of the variance in subjective sexual arousal, and 65% of the variance in perceived intoxication. Contrary to hypotheses, analysis of indirect effects revealed no significant serial mediation effects of perceived intoxication and subjective sexual arousal on skills 1(β = −.04, b = − 0.14, SE = 0.04, Sobel z = − 1.31, p = .30, 95% CI [− 0.12, 0.04]), skills 2 (β = − .06, b = − 0.21, SE = 0.16, Sobel z = − 1.33, p = .19, 95% CI [− 0.14, 0.03]), or UAI (β = − .001, b = − 0.002, SE = 0.03, Sobel z = − 0.08, p = .94, 95% CI [− 0.06, 0.06]).

Serial mediation effect of perceived intoxication and sexual arousal on skills 2. Coefficients are standardized (unstandardized). Model Fit: χ2 (1, n = 116) = 4.56, p = .03; AIC = 1468.58; BIC(adjusted) = 1462.88; RMSEA = .18 (0.04, 0.35); CFI = 0.97; TLI = 0.76; SRMR = .05. Significant paths/coefficients are bolded
Moderated Mediation Analyses
Figure 2 shows estimated regression coefficients from the moderated mediation analyses of the effect of subjective sexual arousal on the relationship between beverage condition and skills 2 via perceived intoxication, with significant paths bolded. Controlling for age, analysis of the second-stage moderated mediation model for skills 2 showed a significant effect of beverage condition on perceived intoxication (β = 1.97, SE = 0.15, p < .001, 95% CI [1.67, 2.25]) and a significant perceived intoxication x subjective sexual arousal interaction (β = − 0.18, SE = 0.08, p = .03, 95% CI [− 0.35, − 0.02]). The index of moderated mediation was also significant (index = − 0.36, SE = 0.17, 95% bootstrapped CI [− 0.68, − 0.02]). Together, this pattern of results suggests a significant second-stage moderated mediation effect of subjective sexual arousal on the relationship between beverage condition and skills 2 via perceived intoxication. In other words, the indirect effect of beverage condition on skills 2 via perceived intoxication depended upon the level of subjective sexual arousal. Specifically, the negative index of moderated mediation indicates a negative linear function, such that as subjective sexual arousal increases, the indirect effect of beverage condition on skills 2 via perceived intoxication becomes more negative. Probing of the conditional indirect effects at different levels of the moderator (see Fig. 3) revealed a positive indirect effect at low (β = 0.71, SE = 0.77, 95% CI [− 0.74, 2.26]) and mean (β = 0.13, SE = 0.64, 95% CI [− 1.11, 1.37]) levels of subjective sexual arousal, versus a negative indirect effect at high levels of subjective sexual arousal (β = − 0.49, SE = 0.60, 95% CI [− 1.65, 0.72]). Thus, at high levels of subjective sexual arousal, alcohol consumption had a negative effect on skills 2 via perceived intoxication. Although the conditional indirect effects were not significant at each level of subjective arousal, the relative change in the indirect effect at low and high levels of the moderator suggests that the overall moderated mediation effect is significant.

Second stage moderated mediation of sexual arousal on the relationship between beverage condition, perceived intoxication, and skills 2. Coefficients are unstandardized (standard error). Model Fit: R2 = .19; F(2, 112) = 5.12; p < .001. Significant index of moderated mediation: index = − 0.36, SE = 0.17, 95% CI (− 0.66, − 0.01). Significant paths/coefficients are bolded

Conditional indirect effects of perceived intoxication in the relationship between beverage condition and skills 2 at low, mean, and high levels of sexual arousal. The slope of the line (− 0.36) is the index of moderated mediation. Low = − 1 SD below the mean, High = + 1 SD above the mean. Coefficients are unstandardized
In the skills 1 model, there was a significant effect of beverage condition on perceived intoxication (β = 1.90, SE = 0.14, p < .001, 95% CI [1.63, 2.17]). Both the interaction of perceived intoxication and subjective sexual arousal (β = − 0.10, SE = 0.09, p = .29, 95% CI [− 0.28, 0.08]) and the index of moderated mediation (index = − 0.19, SE = 0.19, 95% CI [− 0.54, 0.19]) were nonsignificant, suggesting that there was no significant moderated mediation effect of subjective sexual arousal on the relationship between beverage condition and skills 1 via perceived intoxication.
Analysis of the second-stage moderated mediation model on UAI showed a significant effect of beverage condition on perceived intoxication (β = 1.93, SE = 0.15, p < .001, 95% CI [1.64, 2.23]). However, there was no significant perceived intoxication x subjective sexual arousal interaction (β = 0.01, SE = 0.01, p = .19, 95% CI [− 0.01, 0.03]). Along with a nonsignificant index of moderated mediation (index = 0.02, SE = 0.01, 95% CI [− 0.01, 0.05]), these results suggest there is no significant moderated mediation effect of subjective sexual arousal on the relationship between beverage condition and UAI via perceived intoxication.
Discussion
Contrary to previous research [29] and the primary hypothesis of the current analyses, there was not a significant serial mediation effect of perceived intoxication and subjective sexual arousal in the relationship between alcohol consumption and determinants of sexual risk. However, results did suggest a significant moderated mediation effect on behavioral skills 2, such that subjective sexual arousal moderated the effect of alcohol consumption on condom negotiation skills via perceived intoxication. There was no significant moderated mediation effect for behavioral skills 1 or likelihood of UAI, although the direction of the index of moderated mediation for behavioral skills 1 was consistent with the skills 2 index.
This study extends the findings of previous research on perceived intoxication and subjective sexual arousal to MSM, a population that has been disproportionately impacted by the HIV epidemic. The nonsignificant results from the current serial mediation models suggest that in MSM, unlike in heterosexual males and females [29], alcohol consumption does not affect determinants of sexual risk via the effects of perceived intoxication and subjective sexual arousal. Specifically, consistent results from models of all three determinants of sexual risk suggested that alcohol consumption is associated with greater perceived intoxication, and greater perceived intoxication is associated with greater subjective sexual arousal, but greater subjective sexual arousal is not predictive of greater determinants of sexual risk. Alternatively, the null findings may be in part due to a suppression effect, such that at low levels of subjective sexual arousal, the effect of alcohol on skills via perceived intoxication was slightly positive, while at high levels of subjective sexual arousal, the effect was slightly negative.
Exploratory analyses revealed a significant second-stage moderated mediation effect of subjective sexual arousal on the relationship between alcohol consumption and one of the determinants of sexual risk via perceived intoxication. Specifically, analysis of the indirect effects at different levels of the moderator revealed that at low levels of subjective sexual arousal, the effect of alcohol consumption on behavioral skills via perceived intoxication was positive; alcohol consumption was associated with greater perceived intoxication, which was associated with better behavioral skills. However, at high levels of subjective sexual arousal, the effect was negative; alcohol consumption was associated with greater perceived intoxication, which was related to poorer behavioral skills. Normal theory tests revealed that neither indirect effect itself was significantly different from zero, but examination of the index of moderated mediation suggested that the indirect effects were significantly different from each other, which is indicative of a moderated mediation effect [47]. The distribution of the effects (i.e., slightly positive at low levels of subjective sexual arousal and slightly negative at high levels of subjective sexual arousal) may explain why neither individual indirect effect was significant in normal theory tests. Additionally, floor effects on subjective sexual arousal ratings may have limited the variability in subjective sexual arousal, thus reducing the statistical power to detect significant effects. However, the change in the direction of the effect at different levels of subjective sexual arousal constitutes a statistically significant moderated mediation effect. This moderated mediation effect suggests that alcohol’s effect on behavioral skills via perceived intoxication depends on the level of subjective sexual arousal. It is possible that, at low levels of subjective sexual arousal, alcohol reduces any anxiety that may accompany condom negotiation scenarios, thus allowing for more effective condom negotiation. Research has demonstrated the anxiolytic effects of alcohol consumption, particularly in social situations [49, 50]. However, at high levels of subjective sexual arousal, alcohol and arousal’s myopic effects may combine to increase the saliency of sexual stimuli, thus impairing cognitive processing involved in behavioral skills to negotiate condom use.
The moderated mediation model was not significant for the other outcome measures (behavioral skills 1 and intentions for UAI). However, the direction of the index of moderated mediation for the nonsignificant behavioral skills measure was in the hypothesized direction and may therefore be attributable to low variability in the subjective sexual arousal measure. Additionally, the content of the prompts to which participants were required to respond differed, which may explain different findings for prompt 1 and prompt 2. Namely, prompt 2 consisted of a more insistent statement regarding the prospect of engaging in UAI. It is possible that it was more difficult for participants to effectively negotiate condom use in response to the more insistent statement regardless of intoxication and/or subjective arousal and that when in combination with high perceived intoxication and subjective sexual arousal, the detriment to behavioral skills was large enough to be detected by statistical tests. On the contrary, participants may have found it easier to negotiate condom use when the statement was less insistent (i.e., prompt 1), and therefore behavioral skills may have been less affected even when perceived intoxication and subjective sexual arousal were high. Either explanation of low variability in the subjective sexual arousal measure or the content of the prompts is consistent with the finding of a nonsignificant index of moderated mediation in the expected direction.
Although both can be considered determinants of sexual risk, the likelihood of UAI measure is a measure of intention to engage in a behavior, which may be distinct from the behavioral skills measures. The behavioral skills measures involve cognitive processing and condom negotiation skills; in contrast, intentions are the product of multiple components, such as attitudes and subjective norms [e.g., Theory of Planned Behavior; 51, Theory of Reasoned Action; 52, 53], that may involve different processes than condom negotiation skills. In all, differing findings across outcome measures highlight the importance of testing determinants of a particular outcome (i.e., sexual risk) using multiple methods (e.g., intentions and behavioral skills), as different measures may be differentially affected by alcohol and be differentially related to sexual risk behavior.
As discussed earlier, the overall pattern of findings from the serial mediation and moderated mediation models suggests that alcohol consumption alone does not increase subjective sexual arousal to a level that impairs condom negotiation skills. As such, there may be differences in the experience of subjective sexual arousal that influence sexual risk and such differences may be attributable to person-level or contextual factors. Further research is needed to investigate the influence of person-level (e.g., sex-related alcohol expectancies), contextual (e.g., characteristics of the stimulus), and sociocultural factors that may differentially affect the alcohol-sexual risk relationship in MSM compared to heterosexual populations. For example, sex-related alcohol expectancies, which are beliefs that individuals hold about the effects of alcohol on sexual behavior and sexual feelings [e.g., sexual disinhibition, enhancement; 54] have been found to interact with alcohol consumption to affect sexual arousal and predictors of sexual risk [e.g., 11, 55–57]. Additionally, research has shown that men and women show differences in sexual arousal based on characteristics of the stimulus [e.g., amount of contextual information included; 32]. Sociocultural factors may also influence the experience and subsequent reporting of sexual arousal, which differentially affect men and women [e.g., 58, 59]. Overall, the pattern of results from the current analyses suggests that the relationship among alcohol, sexual arousal, and determinants of sexual risk may differ by both sex and sexual orientation, and future research is needed to examine how person-level and contextual factors may differ among populations that differ in sex and sexual orientation.
Of note, the original study design included random assignment to experimental conditions and the experimentally manipulated alcohol variable was entered in the current model as a predictor. However, the mediators and moderators included in these analyses (subjective sexual arousal and perceived intoxication) were not directly manipulated, but rather were derived from participants’ ratings of their subjective experiences related to the two experimental manipulations. As such, the results of the current study may not be able to establish causality, but rather are meant to inform future experimental research on the relationship between alcohol and sexual risk among MSM.
As in all experimental studies, results from this study may have limited generalizability. Another potential limitation is that the data were collected from two different sites, and the sample was not large enough to directly test for site differences. However, results of this research are consistent with that of observational and correlational research on the relationship between alcohol and sexual risk [60]. This consistency allows for greater confidence in the study’s results, as it is less likely that results were due to site differences or other confounding variables.
The results may also be limited by the restricted demographic characteristics of the actors used in the videos for this study. The videos were chosen [43] in an attempt to be representative of likely participants in terms of demographic characteristics as well as situational relevance. It would have been preferable to develop a number of videos so that participants could be matched in terms of demographics to the video they viewed, although it is not clear that race in particular is an important consideration in this context [61]. Resources prevented the development of multiple videos, but it is possible that this may have affected the sensitivity of the design. Replication of these results with different stimuli is necessary to determine if the restricted nature of the stimuli impacted the results.
In conclusion, the current analyses extended the literature by testing a serial mediation model supported in a previous study with a heterosexual population [29] to a sample of MSM. The current analyses did not find support for the serial mediation model regarding effects of alcohol consumption on determinants of sexual risk via perceived intoxication and subjective sexual arousal. Rather, exploratory analyses found some support for a second-stage moderated mediation model. Future research should investigate the role of individual differences (e.g., sex-related alcohol expectancies) and contextual factors (i.e., characteristics of the stimulus) that may affect one’s experience of sexual arousal. Results from this study and future studies may expand an understanding of risky behavior as proposed by alcohol and arousal myopia models [12, 13, 17] and help to inform behavioral interventions for HIV transmission reduction by suggesting contextual and individual factors that may play a role in sexual risk-taking behavior.
References
Johnson AS, Hall HI, Hu X, Lansky A, Holtgrave DR, Mermin J. Trends in diagnoses of HIV infection in the United States, 2002-2011. J Am Med Assoc. 2014;312(4):432–4.
Johnson WD, Diaz RM, Flanders WD, Goodman M, Hill AN, Holtgrave D et al. Behavioral interventions to reduce risk for sexual transmission of HIV among men who have sex with men. Cochrane Database Syst Rev. 2008(3). https://doi.org/10.1002/14651858.cd001230.pub2.
Kalichman SC, Weinhardt L. Negative affect and sexual risk behavior: comment on Crepaz and Marks (2001). Health Psychol. 2001;20(4):300–1. https://doi.org/10.1037/0278-6133.20.4.300.
Patterson DA, Wolf S, Hall M, Golder S. Beliefs and behaviors regarding substance use and HIV risk among men who have sex with men (MSM) in a mid-sized U.S. community. J HIV AIDS Soc Serv. 2009;8(2):188–201. https://doi.org/10.1080/15381500903025605.
Baliunas D, Rehm J, Irving H, Shuper P. Alcohol consumption and risk of incident human immunodeficiency virus infection: a meta-analysis. Int J Public Health. 2010;55(3):159–66. https://doi.org/10.1007/s00038-009-0095-x.
Shuper PA, Joharchi N, Irving H, Rehm J. Alcohol as a correlate of unprotected sexual behavior among people living with HIV/AIDS: review and meta-analysis. AIDS Behav. 2009;13(6):1021–36. https://doi.org/10.1007/s10461-009-9589-z.
Cooper ML. Toward a person × situation model of sexual risk-taking behaviors: Illuminating the conditional effects of traits across sexual situations and relationship contexts. J Pers Soc Psychol. 2010;98(2):319–41. https://doi.org/10.1037/a0017785.
Weinhardt LS, Carey MP. Does alcohol lead to sexual risk behavior? Findings from event-level research. Annu Rev Sex Res. 2000;11:125–57.
Berry MS, Johnson MW. Does being drunk or high cause HIV sexual risk behavior? A systematic review of drug administration studies. Pharmacol Biochem Behav. 2017. https://doi.org/10.1016/j.pbb.2017.08.009.
Rehm J, Shield KD, Joharchi N, Shuper PA. Alcohol consumption and the intention to engage in unprotected sex: Systematic review and meta-analysis of experimental studies. Addiction. 2012;107(1):51–9. https://doi.org/10.1111/j.1360-0443.2011.03621.x.
Maisto SA, Palfai T, Vanable PA, Heath J, Woolf-King SE. The effects of alcohol and sexual arousal on determinants of sexual risk in men who have sex with men. Arch Sex Behav. 2012;41(4):971–86. https://doi.org/10.1007/s10508-011-9846-x.
Loewenstein G. Out of control: visceral influences on behavior. Organ Behav Hum Decis Process. 1996;65(3):272–92. https://doi.org/10.1006/obhd.1996.0028.
Loewenstein G, Weber EU, Hsee CK, Welch N. Risk as feelings. Psychol Bull. 2001;127(2):267–86. https://doi.org/10.1037/0033-2909.127.2.267.
Blanton H, Gerrard M. Effect of sexual motivation on men’s risk perception for sexually transmitted disease: there must be 50 ways to justify a lover. Health Psychol. 1997;16(4):374–9. https://doi.org/10.1037/0278-6133.16.4.374.
Ariely D, Loewenstein G. The heat of the moment: the effect of sexual arousal on sexual decision making. J Behav Decis Mak. 2006;19(2):87–98. https://doi.org/10.1002/bdm.501.
Wray TB, Simons JS, Maisto SA. Effects of alcohol intoxication and autonomic arousal on delay discounting and risky sex in young adult heterosexual men. Addict Behav. 2015;42:9–13.
Steele CM, Josephs RA. Alcohol myopia: Its prized and dangerous effects. Am Psychol. 1990;45(8):921–33. https://doi.org/10.1037/0003-066X.45.8.921.
Ebel-Lam AP, MacDonald TK, Zanna MP, Fong GT. An experimental investigation of the interactive effects of alcohol and sexual arousal on intentions to have unprotected sex. Basic Appl Soc Psych. 2009;31(3):226–33. https://doi.org/10.1080/01973530903058383.
MacDonald TK, MacDonald G, Zanna MP, Fong G. Alcohol, sexual arousal, and intentions to use condoms in young men: applying alcohol myopia theory to risky sexual behavior. Health Psychol. 2000;19(3):290–8. https://doi.org/10.1037/0278-6133.19.3.290.
George WH, Davis KC, Norris J, Heiman JR, Stoner SA, Schacht RL, et al. Indirect effects of acute alcohol intoxication on sexual risk-taking: the roles of subjective and physiological sexual arousal. Arch Sex Behav. 2009;38(4):498–513. https://doi.org/10.1007/s10508-008-9346-9.
Prause N, Staley C, Finn P. The effects of acute ethanol consumption on sexual response and sexual risk-taking intent. Arch Sex Behav. 2011;40(2):373–84.
Davis KC, Hendershot CS, George WH, Norris J, Heiman JR. Alcohol’s effects on sexual decision making: an integration of alcohol myopia and individual differences. J Stud Alcohol Drugs. 2007;68(6):843–51.
Engle KB, Williams TK. Effect of an ounce of vodka on alcoholics’ desire for alcohol. Q J Stud Alcohol. 1972;33(4-A):1099-105.
Marlatt GA, Demming B, Reid JB. Loss of control drinking in alcoholics: an experimental analogue. J Abnorm Psychol. 1973;81(3):233–41. https://doi.org/10.1037/h0034532.
Wilson GT, Lawson DM. Expectancies, alcohol, and sexual arousal in male social drinkers. J Abnorm Psychol. 1976;85(6):587–94. https://doi.org/10.1037/0021-843X.85.6.587.
Wilson GT, Lawson DM. Expectancies, alcohol, and sexual arousal in women. J Abnorm Psychol. 1978;87(3):358–67. https://doi.org/10.1037/0021-843X.87.8.358.
Maisto SA, Carey MP, Carey KB, Gordon CM. The effects of alcohol and expectancies on risk perception and behavioral skills relevant to safer sex among heterosexual young adult women. J Stud Alcohol. 2002;63(4):476–85.
Maisto SA, Carey MP, Carey KB, Gordon CM, Schum JL. Effects of alcohol and expectancies on HIV-related risk perception and behavioral skills in heterosexual women. Exp Clin Psychopharmacol. 2004;12(4):288–97. https://doi.org/10.1037/1064-1297.12.4.288.
Davis KC, George WH, Norris J, Schacht RL, Stoner SA, Hendershot CS, et al. Effects of alcohol and blood alcohol concentration limb on sexual risk-taking intentions. J Stud Alcohol Drugs. 2009;70(4):499–507.
Peplau LA. Human sexuality: how do men and women differ? Curr Dir Psychol Sci. 2003;12(2):37–40. https://doi.org/10.1111/1467-8721.01221.
Chivers ML, Seto MC, Blanchard R. Gender and sexual orientation differences in sexual response to sexual activities versus gender of actors in sexual films. J Pers Soc Psychol. 2007;93(6):1108–21. https://doi.org/10.1037/0022-3514.93.6.1108.
Rupp HA, Wallen K. Sex differences in response to visual sexual stimuli: a review. Arch Sex Behav. 2008;37(2):206–18.
Rieger G, Savin-Williams RC. The eyes have it: sex and sexual orientation differences in pupil dilation patterns. PLoS ONE. 2012;7(8):e40256.
Neave N, Menaged M, Weightman DR. Sex differences in cognition: the role of testosterone and sexual orientation. Brain Cognit. 1999;41(3):245–62.
Rahman Q, Wilson GD. Large sexual-orientation-related differences in performance on mental rotation and judgement of line orientation tasks. Neuropsychology. 2003;17(1):25–31.
Rahman Q, Abrahams S, Wilson GD. Sexual-orientation-related differences in verbal fluency. Neuropsychology. 2003;17(2):240–6.
Collaer ML, Hines M. Human behavioral sex differences: a role for gonadal hormones during early development? Psychol Bull. 1995;118(1):55–107.
Caplan PJ, Caplan JB. Thinking critically about research on sex and gender. New York: HarperCollins College Publishers; 1994.
Rahman Q, Wilson GD, Abrahams S. Biosocial factors, sexual orientation and neurocognitive functioning. Psychoneuroendocrinology. 2004;29(7):867–81.
Maisto SA, Simons JS. Research on the effects of alcohol and sexual arousal on sexual risk in men who have sex with men: Implications for HIV prevention interventions. AIDS Behav. 2016;20(1):158–72. https://doi.org/10.1007/s10461-015-1220-x.
Edwards JR, Lambert LS. Methods for integrating moderation and mediation: a general analytical framework using moderated path analysis. Psychol Methods. 2007;12(1):1–22.
Cahalan D, Cissin I, Crossley H. American drinking practices. New Brunswick: Rutgers Center for Alcohol Studies; 1969.
Woolf-King SE, Maisto S, Carey M, Vanable P. Selection of film clips and development of a video for the investigation of sexual decision making among men who have sex with men. J Sex Res. 2010;47(6):589–97. https://doi.org/10.1080/00224490903216748.
Abbey A, Saenz C, Buck PO. The cumulative effects of acute alcohol consumption, individual differences and situational perceptions on sexual decision making. J Stud Alcohol. 2005;66(1):82–90.
Hayes AF. Introduction to mediation, moderation, and conditional process analysis: a regression-based approach. New York: Guilford Press; 2013.
Preacher KJ, Rucker DD, Hayes AF. Addressing moderated mediation hypotheses: theory, methods, and prescriptions. Multivariate Behav Res. 2007;42(1):185–227.
Hayes AF. An index and test of linear moderated mediation. Multivariate Behav Res. 2015;50(1):1–22. https://doi.org/10.1080/00273171.2014.962683.
Aiken LS, West SG, Reno RR. Multiple regression: testing and interpreting interactions. Thousand Oaks: Sage; 1991.
Sher KJ, Walitzer KS. Individual differences in the stress-response-dampening effect of alcohol: a dose-response study. J Abnorm Psychol. 1986;95(2):159–67. https://doi.org/10.1037/0021-843X.95.2.159.
Moberg CA, Curtin JJ. Alcohol selectively reduces anxiety but not fear: startle response during unpredictable versus predictable threat. J Abnorm Psychol. 2009;118(2):335–47. https://doi.org/10.1037/a0015636.
Ajzen I. The theory of planned behavior. Organ Behav Hum Decis Process. 1991;50(2):179–211.
Ajzen I, Fishbein M. Understanding attitudes and predicting social behaviour. Englewood Cliffs: Prentice-Hall; 1980.
Fishbein M, Ajzen I. Belief, attitude, intention and behavior: an introduction to theory and research. Reading: Addison-Wesley; 1975.
Dermen KH, Cooper ML. Sex-related alcohol expectancies among adolescents: I. Scale development. Psychol Addict Behav. 1994;8(3):152–60. https://doi.org/10.1037/0893-164X.8.3.152.
Cooper ML, O’Hara RE, Martins J. Does drinking improve the quality of sexual experience?: Sex-specific alcohol expectancies and subjective experience on drinking versus sober sexual occasions. AIDS Behav. 2016;20(Suppl 1):40–51. https://doi.org/10.1007/s10461-015-1136-5.
Gilmore AK, George WH, Nguyen HV, Heiman JR, Davis KC, Norris J. Influences of situational factors and alcohol expectancies on sexual desire and arousal among heavy-episodic drinking women: acute alcohol intoxication and condom availability. Arch Sex Behav. 2013;42(6):949–59. https://doi.org/10.1007/s10508-013-0109-x.
George WH, Stoner SA, Norris J, Lopez PA, Lehman GL. Alcohol expectancies and sexuality: a self-fulfilling prophecy analysis of dyadic perceptions and behavior. J Stud Alcohol. 2000;61(1):168–76. https://doi.org/10.15288/jsa.2000.61.168.
Alexander MG, Fisher TD. Truth and consequences: using the bogus pipeline to examine sex differences in self-reported sexuality. J Sex Res. 2003;40(1):27–35. https://doi.org/10.1080/00224490309552164.
Fisher TD. Sex of experimenter and social norm effects on reports of sexual behavior in young men and women. Arch Sex Behav. 2007;36(1):89–100. https://doi.org/10.1007/s10508-006-9094-7.
Cooper ML. Alcohol use and risky sexual behavior among college students and youth: evaluating the evidence. J Stud Alcohol. 2002;supplement, (14):101–17.
Hughes KYR, Anderson VN. What turns women on? Black and White women’s sexual arousal. Int J Sex Health. 2007;19(2):17–31. https://doi.org/10.1300/J514v19n02_02.
Funding
This study was funded by the National Institute on Alcohol Abuse and Alcoholism (R01 AA14480 and 2K05 AA16928).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Buckheit, K.A., Mitzel, L.D., Maisto, S.A. et al. Moderated Mediation of Perceived Intoxication and Sexual Arousal on Determinants of Sexual Risk Behavior in Men Who Have Sex with Men. AIDS Behav 23, 1460–1470 (2019). https://doi.org/10.1007/s10461-018-2343-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10461-018-2343-7