
Abstract
Background
Insulin resistance is one of the risks of chronic kidney disease (CKD). The triglyceride–glucose index (TyG index) has been suggested as a marker of moderate insulin resistance. We aimed to investigate the association between TyG index and incident CKD.
Methods
In this historical cohort study of 11,712 participants (6026 men and 5686 women), we investigated the impact of TyG index on incident CKD. CKD was defined as estimated GFR less than 60 mL/min/1.73 m2 and/or proteinuria detected by dipstick test in fasting morning urine. TyG index was calculated as ln [fasting triglycerides (mg/dL) × fasting plasma glucose (mg/dL)/2]. Cox proportional hazard models were performed to investigate the impact of TyG index on incident CKD, adjusting for age, BMI categories, waist circumference, smoking status, exercise, logarithm of alcohol consumption, systolic blood pressure, serum albumin, hemoglobin A1c, hyperuricemia, low HDL-cholesterol concentration, high LDL-cholesterol concentration, CRP, creatinine, and gamma-glutamyltransferase.
Results
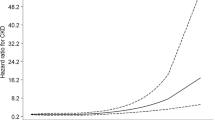
During the median 4.0-year follow-up duration for men and 3.7-year follow-up duration for women, 261 participants (120 men and 141 women) developed CKD. In Cox proportional hazard model, TyG index presented the significant risks for incident CKD in both men and women (men, hazard ratio 1.32, 95% confidence interval 1.02–1.70, p = 0.036, women, hazard ratio 1.50, 95% confidence interval 1.05–2.13, p = 0.024).
Conclusion
This study revealed that TyG index can be a predictor of incident CKD.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Chronic kidney disease (CKD) is a public health problem, which imposes health, social, and human burden on societies worldwide [1]. CKD remains asymptomatic until the stage of disease progresses. Moreover, CKD is reported to increase the risk of cardiovascular disease [2] and mortality [3]. Therefore, both prevention and treatment of CKD are important for prevention of end stage of renal dysfunction, cardiovascular disease, and mortality.
Insulin resistance is known to be a risk factor for the progression of CKD [4]. In addition, some previous studies reported that patients with CKD have insulin resistance from the early stage [5,6,7]. Therefore, detection of insulin resistance at an early stage of kidney disease is important in the prevention of CKD. Triglyceride–glucose index (TyG index), which is calculated with fasting plasma glucose and triglycerides, has been suggested as a marker of moderate insulin resistance [8, 9]. Moreover, TyG index was reported to predict the development of type 2 diabetes [10, 11] and cardiovascular disease [12]. However, no previous studies revealed the association between TyG index and the development of CKD. Thus, we aimed to investigate the association between TyG index and the development of CKD using NAfld in the Gifu Area, Longitudinal Analysis (NAGALA) cohort database.
Materials and methods
Study design and study participants
The NAGALA cohort study is an ongoing prospective cohort study that began in 1994 [13]. For this population-based longitudinal analysis, we extracted the participants from a medical examination program at Asahi University Hospital (Gifu, Japan). This medical examination program, which is called a human dock, is aimed to detect chronic diseases and their risk factors and promote public health. More than 8000 participants annually registered and 60% of them receive 1–2 exams per year [14]. In this study, we investigated the effect of TyG index on incident CKD, using the NAGALA database. We extracted the participants who received the medical examination program at Asahi University Hospital from 1994 to 2016. Some previous studies reported that mildly decreased estimated glomerular filtration rate (eGFR) (60–74 mL/min/1.73 m2) has a significantly higher risk of CKD. Therefore, we excluded the participants who had not only with CKD (eGFR < 60 mL/min/1.73 m2) but also mildly decreased eGFR (60–74 mL/min/1.73 m2) at the baseline examination [15, 16]. Moreover, we excluded the participants with medication at the baseline examination. Approval for the study was obtained from the research ethics committees of the Asahi University Hospital, and written informed consent for their data to be used was obtained from all participants.
Standardized questionnaire for lifestyle factors
To determine the lifestyle factors of participants, a standardized questionnaire was performed to all participants [14]. We divided the participants into nonsmokers, ex-smokers, and current smokers. Next, we asked about the type and amount of alcohol consumption per week during the prior month, then estimating the mean ethanol intake per week. Finally, we defined the participants who performed any kind of sport regularly at least once a week as regular exercisers.
Data collection
Body mass index (BMI) was defined as weight in kilograms divided by height in meters squared. We divided the participants into four groups according to their BMI values: lean, BMI < 18.5 kg/m2; normal, ≥ 18.5 to < 23 kg/m2; overweight, ≥ 23 to < 25 kg/m2; obesity, ≥ 25 kg/m2 [17]. The participants’ levels of several factors including fasting plasma glucose, triglycerides, high-density lipoprotein (HDL) cholesterol, and creatinine were measured using venous blood after an overnight fast. We used the Japanese Society of Nephrology equation for calculating each patient’s eGFR: eGFR (mL/min/1.73 m2) = 194 × serum creatinine−1.094 × age−0.287 (× 0.739 for women) [18]. Spot morning urine sample was measured. Participants with serum uric acid level ≥ 416 mmol/L (7.0 mg/dL) for men and ≥ 386 mmol/L (6.5 mg/dL) for women were defined as having hyperuricemia [19]. Moreover, participants with serum HDL-cholesterol level < 1 mmol/L (40 mg/dL) for men and < 1.3 mmol/L (50 mg/dL) for women were defined as having low HDL concentrations. In addition, TG/HDL ratio was calculated in the following formula: TG (mg/dL)/HDL-cholesterol (mg/dL) [20]. Finally, TyG index was calculated as ln[fasting triglycerides (mg/dL) × fasting plasma glucose (mg/dL)/2] [8].
Definition of CKD
CKD was defined as decreased estimated glomerular filtration rate (eGFR). GFR was estimated using the Japanese Society of Nephrology equation. When eGFR was less than 60 mL/min/1.73 m2, it was defined as having CKD [21].
Statistical analysis
Statistical analyses were preformed using JMP ver. 12.0 software (SAS Institute, Cary, NC) and a p value < 0.05 was considered significant. Means or frequencies of potential confounding variables were calculated, and continuous variables are presented as the mean (standard deviation, SD). We divided the participants into men and women, because the distribution of TyG index differed between sexes. The p values were analyzed by one-way analysis of variance for continuous variables and chi-squared test for categorical variables. In addition, we checked the characteristics of participants with mildly decreased eGFR or CKD without medication at baseline examination as a subgroup analysis.
Cox proportional hazard model was used to calculate unadjusted and adjusted hazard ratio (HR) and 95% confidence interval (CI) for incident CKD. We adjusted for age, BMI categories, waist circumference, smoking status, exercise, logarithm of alcohol consumption, systolic blood pressure, serum albumin, hemoglobin A1c, hyperuricemia, low HDL-cholesterol concentration, high LDL-cholesterol concentration, CRP, creatinine, and gamma-glutamyltransferase.
In addition, the area under the curve (AUC) of several factors, including TyG index, for the incident CKD was calculated by the receiver-operating characteristic (ROC) curve.
Results
We enrolled 27,944 participants without any medication. At first, we divided them into two groups according to sex, and there were 16,454 men and 11,490 women. Among them, we excluded 3617 participants (2565 men and 1052 women) with CKD, 9744 participants with mildly decreased eGFR (6010 men and 3734 women) and 2501 participants with medication (1811 men and 690 women) at baseline examination. In addition, we also excluded 372 participants whose data were missed. Finally, 6026 men and 5686 women were analyzed in this study (Fig. 1).

Study flow diagram for the registration of participants
The baseline characteristics of the participants are shown in Table 1. TyG index in men was significantly higher than that in women (8.25 (0.66) vs 7.66 (0.57), p <0.001). In addition, the characteristics of the participants with CKD or mildly decreased eGFR at baseline examination are shown in Supplementary Table 1. TyG index of participants with CKD or mildly decreased eGFR at baseline examination was significantly higher than that without both in men and women [men: 8.54 (0.63) vs 8.25 (0.66), p < 0.001; women: 8.05 (0.57) vs 7.66 (0.57), p < 0.001]. Next, we investigated unadjusted HRs and 95% CIs for the incidence of CKD (Table 2). In univariate analyses, TyG index was significant risk for incident CKD (men, HR 1.59, 95% CI 1.21–2.07, p = 0.001; women, HR 2.25, 95% CI 1.70–2.96, p < 0.001). In multivariate analyses, TyG index presented the significant risk for incident CKD in both men and women (men, HR 1.32, 95% CI 1.02–1.70, p = 0.036; women, HR 1.50, 95% CI 1.05–2.13, p = 0.024) (Table 3).
In addition, in ROC analyses, AUC of TyG index was 0.593, and that of BMI, serum creatinine, HbA1c, TG, TG/HDL ratio, or waist circumference was 0.512 (p = 0.007 vs. TyG index), 0.468 (p < 0.001 vs. TyG index), 0.564 (p = 0.494 vs. TyG index), 0.598 (p = 0.179 vs. TyG index), 0.587 (p = 0.573 vs. TyG index), or 0.528 (p = 0.021 vs. TyG index), in men, respectively. AUC of TyG index was 0.634, and that of BMI, serum creatinine, HbA1c, TG, TG/HDL ratio or waist circumference was 0.594 (p = 0.156 vs. TyG index), 0.455 (p < 0.001 vs. TyG index), 0.474 (p < 0.001 vs. TyG index), 0.633 (p = 0.886 vs. TyG index), 0.632 (p = 0.815 vs. TyG index), and 0.552 (p = 0.006 vs. TyG index), in women, respectively (Fig. 2).

Area under the receiver-operating characteristic (ROC)curve (AUC) [95% confidence interval (CI)] of several factors for incident CKD. a TyG index, b BMI, c serum creatinine, d HbA1c, e TG, f TG/HDL ratio, and g waist circumference. AUC of TyG index was 0.593, and that of BMI, serum creatinine, HbA1c, TG, TG/HDL ratio or waist circumference was 0.512 (p = 0.007 vs. TyG index), 0.468 (p < 0.001 vs. TyG index), 0.564 (p = 0.494 vs. TyG index), 0.598 (p = 0.179 vs. TyG index), 0.587 (p = 0.573 vs. TyG index), or 0.528 (p = 0.021 vs. TyG index), in men, respectively. AUC of TyG index was 0.634, and that of BMI, serum creatinine, HbA1c, TG, TG/HDL ratio or waist circumference was 0.594 (p = 0.156 vs. TyG index), 0.455 (p < 0.001 vs. TyG index), 0.474 (p < 0.001 vs. TyG index), 0.633 (p = 0.886 vs. TyG index), 0.632 (p = 0.815 vs. TyG index), and 0.552 (p = 0.006 vs. TyG index), in women, respectively
Discussion
In this cohort study of over 10,000 Japanese individuals, for the first time, we investigated the association between TyG index and incident CKD. CKD, which has become a public health problem [1], is the risk of cardiovascular disease [2] and mortality [3]. Hence, intervention at an early stage of the disease is desirable. Some previous reports revealed the association between TyG index and incident type 2 diabetes [10] and cardiovascular disease [12]. However, there is no report of the association between TyG index and incident CKD. We showed that high TyG index is associated with risk of incident CKD. In fact, we compared area under the curve (AUC) of TyG index with that of BMI, serum creatinine, HbA1c, TG, TG/HDL ratio [20], and waist circumference. Then, TyG index was equal or superior to other markers of insulin resistance, including TG, TG/HDL ratio, waist circumference, and HbA1c for predicting CKD. Among them, AUCs of TG both in men and women were almost the same as those of TyG index. Therefore, TG itself might also be a risk marker of incident CKD.
Several groups demonstrated the association between insulin resistance and CKD [5, 22, 23]. Some animal and human experimental studies demonstrated that hyperinsulinemia induces renal vasodilatation, increases sodium reabsorption, enhances the renin–angiotensin system, and induces glomerular hyperfiltration, which increases GFR [24,25,26]. Increased filtration per nephron causes nephron loss and results in glomerular hypertension, which induces glomerular sclerosis and subsequent renal dysfunction [27]. Moreover, in some clinical studies, insulin resistance is already present in patients with mild degrees of renal dysfunction [6, 7, 28]. The association between insulin resistance and CKD could be explained by some biological mechanisms such as inflammation, oxidative stress, and metabolic acidosis. First, inflammation and CKD are known to be related each other [29]. Recently, Shimobayashi et al. [30] demonstrated that insulin resistance induces inflammation in adipose tissue by inhibiting insulin-signaling pathway and increasing monocyte chemoattractant protein 1 production. M2 macrophage activated by inflammation in adipose tissue produces and releases proinflammatory cytokines such as interleukin (IL)-6 and tumor necrosis factor (TNF)-α [31]. IL-6 induces endothelial dysfunction and vascular hypertrophy in response to angiotensin II [32]. In addition, TNF-α was also reported to induce endothelial dysfunction [33]. Endothelial dysfunction is associated with incident CKD [34]. Therefore, Both IL-6 [32] and TNF-α [33] induces endothelial dysfunction, which has close association with incident CKD [34]. Second, insulin resistance induces oxidative stress [34]. Oxidative stress and inflammation impair the activation of nuclear factor erythroid-2-related factor-2 which protects against tissue injury of kidney [35]. In fact, TyG index showed a positive association with CRP in this study (men, r = 0.055, p < 0.001, women, r = 0.051, p = 0.045, by Pearson’s correlation coefficient). Third, metabolic acidosis, which is induced by hyperglycemia [36], also causes insulin resistance [37]. Metabolic acidosis causes change in function of kidney, including an increase in renal plasma flow and GFR, to excrete the excess acid load [38]. Glomerular hyperfiltration may facilitate the progression of CKD [27]. A previous study reported the association between metabolic acidosis and urine pH [39]. In this study, TyG index showed a negative association with urine pH (men, r = − 0.113, p < 0.001, women, r = − 0.086, p < 0.001, by Pearson’s correlation coefficient). Taken together, inflammation, oxidative stress, and metabolic acidosis induced by insulin resistance play key roles in pathogenesis of CKD.
The strengths of our study include using the standardized questionnaire for lifestyle factors, and the relatively large population-based longitudinal research. Our study has also several limitations. First, we assessed proteinuria with urine dipstick test and did not quantify proteinuria. A dipstick test is often used in general practice and < 1+ or less than trace has a high negative predictive value in the general community setting [40]. In addition, we confirmed urine experiments once. If we performed urine experiments multiple times, we could evaluate CKD more accurately. Second, the follow-up was medium term; therefore, the statistical power might be limited. Third, sodium and protein intake are associated with pathogenesis of CKD [41, 42]. However, we did not have the data of them. If we had the data, we could more accurately investigate the association between TyG index and incident CKD. Fourth, participants in this study received a health examination; therefore, part of them might have changed and improved their lifestyles, which prevent incident CKD. Finally, almost all participants were Japanese; therefore, it is uncertain whether our findings can be generalized to other ethnic groups.
In conclusion, we demonstrated, for the first time, that TyG index can be a predictor of incident CKD.
References
Levey AS, Atkins R, Coresh J, Cohen EP, Collins AJ, Eckardt K-U, et al. Chronic kidney disease as a global public health problem: approaches and initiatives—a position statement from kidney disease improving global outcomes. Kidney Int. 2007;72:247–59.
Holman RR, Paul SK, Bethel MA, Neil HAW, Matthews DR. Long-term follow-up after tight control of blood pressure in type 2 diabetes. N Engl J Med. 2008;359:1565–76.
Afkarian M, Sachs MC, Kestenbaum B, Hirsch IB, Tuttle KR, Himmelfarb J, et al. Kidney disease and increased mortality risk in type 2 diabetes. J Am Soc Nephrol. 2013;24:302–8.
de Boer IH, Mehrotra R. Insulin resistance in chronic kidney disease: a step closer to effective evaluation and treatment. Kidney Int. 2014;86:243–5.
Fliser D, Pacini G, Engelleiter R, Kautzky-Willer A, Prager R, Franek E, et al. Insulin resistance and hyperinsulinemia are already present in patients with incipient renal disease. Kidney Int. 1998;53:1343–7.
Eidemak I, Feldt-Rasmussen B, Kanstrup IL, Nielsen SL, Schmitz O, Strandgaard S. Insulin resistance and hyperinsulinaemia in mild to moderate progressive chronic renal failure and its association with aerobic work capacity. Diabetologia. 1995;38:565–72.
Kato Y, Hayashi M, Ohno Y, Suzawa T, Sasaki T, Saruta T. Mild renal dysfunction is associated with insulin resistance in chronic glomerulonephritis. Clin Nephrol. 2000;54:366–73.
Simental-Mendía LE, Rodríguez-Morán M, Guerrero-Romero F. The product of fasting glucose and triglycerides as surrogate for identifying insulin resistance in apparently healthy subjects. Metab Syndr Relat Disord. 2008;6:299–304.
Du T, Yuan G, Zhang M, Zhou X, Sun X, Yu X. Clinical usefulness of lipid ratios, visceral adiposity indicators, and the triglycerides and glucose index as risk markers of insulin resistance. Cardiovasc Diabetol. 2014;13:146.
Navarro-González D, Sánchez-Íñigo L, Pastrana-Delgado J, Fernández-Montero A, Martinez JA. Triglyceride–glucose index (TyG index) in comparison with fasting plasma glucose improved diabetes prediction in patients with normal fasting glucose: the vascular-metabolic CUN cohort. Prev Med (Baltim). 2016;86:99–105.
Low S, Khoo KCJ, Irwan B, Sum CF, Subramaniam T, Lim SC, et al. The role of triglyceride glucose index in development of type 2 diabetes mellitus. Diabetes Res Clin Pract. 2018;143:43–9.
Sánchez-Íñigo L, Navarro-González D, Fernández-Montero A, Pastrana-Delgado J, Martínez JA. The TyG index may predict the development of cardiovascular events. Eur J Clin Investig. 2016;46:189–97.
Hamaguchi M, Kojima T, Takeda N, Nakagawa T, Taniguchi H, Fujii K, et al. The metabolic syndrome as a predictor of nonalcoholic fatty liver disease. Ann Intern Med. 2005;143:722–8.
Okamura T, Hashimoto Y, Hamaguchi M, Obora A, Kojima T, Fukui M. Ectopic fat obesity presents the greatest risk for incident type 2 diabetes: a population-based longitudinal study. Int J Obes. 2019;43:139–48.
Wang Y, Katzmarzyk PT, Horswell R, Zhao W, Johnson J, Hu G. Kidney function and the risk of cardiovascular disease in patients with type 2 diabetes. Kidney Int. 2014;85:1192–9.
Tohidi M, Hasheminia M, Mohebi R, Khalili D, Hosseinpanah F, Yazdani B, et al. Incidence of chronic kidney disease and its risk factors, results of over 10 year follow up in an Iranian cohort. PLoS One. 2012;7:e45304.
Japan Society for the Study of Obesity. Diagnostic criteria for obesity. Nihon Himan Gakkai. 2011;17:i–vii.
Matsuo S, Imai E, Horio M, Yasuda Y, Tomita K, Nitta K, et al. Revised equations for estimated GFR from serum creatinine in Japan. Am J Kidney Dis. 2009;53:982–92.
Zoppini G, Targher G, Chonchol M, Ortalda V, Abaterusso C, Pichiri I, et al. Serum uric acid levels and incident chronic kidney disease in patients with type 2 diabetes and preserved kidney function. Diabetes Care. 2012;35:99–104.
Fukuda Y, Hashimoto Y, Hamaguchi M, Fukuda T, Nakamura N, Ohbora A, Kato T, Kojima T, Fukui M. Triglycerides to high-density lipoprotein cholesterol ratio is an independent predictor of incident fatty liver; a population-based cohort study. Liver Int. 2016;36:713–20.
Hashimoto Y, Tanaka M, Okada H, Senmaru T, Hamaguchi M, Asano M, et al. Metabolically Healthy Obesity and Risk of Incident CKD. Clin J Am Soc Nephrol. 2015;10:578–83.
Kobayashi H, Tokudome G, Hara Y, Sugano N, Endo S, Suetsugu Y, et al. Insulin resistance is a risk factor for the progression of chronic kidney disease. Clin Nephrol. 2009;71:643–51.
Kobayashi S, Maesato K, Moriya H, Ohtake T, Ikeda T. Insulin resistance in patients with chronic kidney disease. Am J Kidney Dis. 2005;45:275–80.
Esteghamati A, Ashraf H, Nakhjavani M, Najafian B, Hamidi S, Abbasi M. Insulin resistance is an independent correlate of increased urine albumin excretion: a cross-sectional study in Iranian type 2 diabetic patients. Diabet Med. 2009;26:177–81.
Tucker BJ, Anderson CM, Thies RS, Collins RC, Blantz RC. Glomerular hemodynamic alterations during acute hyperinsulinemia in normal and diabetic rats. Kidney Int. 1992;42:1160–8.
Dengel DR, Goldberg AP, Mayuga RS, Kairis GM, Weir MR. Insulin resistance, elevated glomerular filtration fraction, and renal injury. Hypertens (Dallas Tex 1979). 1996;28:127–32.
Helal I, Fick-Brosnahan GM, Reed-Gitomer B, Schrier RW. Glomerular hyperfiltration: definitions, mechanisms and clinical implications. Nat Rev Nephrol. 2012;8:293–300.
Chen J, Muntner P, Hamm LL, Fonseca V, Batuman V, Whelton PK, et al. Insulin resistance and risk of chronic kidney disease in nondiabetic US adults. J Am Soc Nephrol. 2003;14:469–77.
Gupta J, Mitra N, Kanetsky PA, Devaney J, Wing MR, Reilly M, et al. Association between albuminuria, kidney function, and inflammatory biomarker profile in CKD in CRIC. Clin J Am Soc Nephrol. 2012;7:1938–46.
Shimobayashi M, Albert V, Woelnerhanssen B, Frei IC, Weissenberger D, Meyer-Gerspach AC, et al. Insulin resistance causes inflammation in adipose tissue. J Clin Investig. 2018;128:1538–50.
Weisberg SP, McCann D, Desai M, Rosenbaum M, Leibel RL, Ferrante AW. Obesity is associated with macrophage accumulation in adipose tissue. J Clin Investig. 2003;112:1796–808.
Schrader LI, Kinzenbaw DA, Johnson AW, Faraci FM, Didion SP. IL-6 deficiency protects against angiotensin II induced endothelial dysfunction and hypertrophy. Arterioscler Thromb Vasc Biol. 2007;27:2576–81.
Picchi A, Gao X, Belmadani S, Potter BJ, Focardi M, Chilian WM, et al. Tumor necrosis factor-induces endothelial dysfunction in the prediabetic metabolic syndrome. Circ Res. 2006;99:69–77.
Bolton CH, Downs LG, Victory JGG, Dwight JF, Tomson CRV, Mackness MI, et al. Endothelial dysfunction in chronic renal failure: roles of lipoprotein oxidation and pro-inflammatory cytokines. Nephrol Dial Transplant. 2001;16:1189–97.
Kim HJ, Vaziri ND. Contribution of impaired Nrf2-Keap1 pathway to oxidative stress and inflammation in chronic renal failure. Am J Physiol Physiol. 2010;298:F662–71.
Avogaro A, Crepaldi C, Miola M, Maran A, Pengo V, Tiengo A, et al. High blood ketone body concentration in type 2 non-insulin dependent diabetic patients. J Endocrinol Investig. 1996;19:99–105.
Mak RH. Effect of metabolic acidosis on insulin action and secretion in uremia. Kidney Int. 1998;54:603–7.
Györke ZS, Sulyok E, Guignard JP. Ammonium chloride metabolic acidosis and the activity of renin-angiotensin-aldosterone system in children. Eur J Pediatr. 1991;150:547–9.
Marunaka Y. Roles of interstitial fluid pH in diabetes mellitus: glycolysis and mitochondrial function. World J Diabetes. 2015;6:125–35.
White SL, Yu R, Craig JC, Polkinghorne KR, Atkins RC, Chadban SJ. Diagnostic accuracy of urine dipsticks for detection of albuminuria in the general community. Am J Kidney Dis. 2011;58:19–28.
Vegter S, Perna A, Postma MJ, Navis G, Remuzzi G, Ruggenenti P. Sodium intake, ACE inhibition, and progression to ESRD. J Am Soc Nephrol. 2012;23:165–73.
Martin WF, Armstrong LE, Rodriguez NR. Dietary protein intake and renal function. Nutr Metab (Lond). 2005;2:25.
Acknowledgements
We thank all of the staff members in the medical health checkup center at Asahi University Hospital.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Yoshitaka Hashimoto received Grants from the Fuji Foundation for Protein Research, outside the submitted work. Michiaki Fukui reports Grants from AstraZeneca plc, Grants from Astellas Pharma Inc., Grants from Nippon Boehringer Ingelheim Co., Ltd., Grants from Daiichi Sankyo Co., Ltd., Grants from Eli Lilly Japan K.K., Grants from Kyowa Hakko Kirin Company Ltd., Grants from Kissei Pharmaceutical Co., Ltd., Grants from MSD K.K., Grants from Mitsubishi Tanabe Pharma Corporation, Grants from Novo Nordisk Pharma Ltd., Grants from Sanwa Kagaku Kenkyusho Co., Ltd., Grants from Sanofi K.K., Grants from Ono Pharmaceutical Co., Ltd., and Grants from Takeda Pharmaceutical Co., Ltd., outside the submitted work. The sponsors were not involved in the study design; in the collection, analysis, interpretation of data; in the writing of this manuscript; or in the decision to submit the article for publication. The authors, their immediate families, and any research foundations with which they are affiliated have not received any financial payments or other benefits from any commercial entity related to the subject of this article. The authors declare that although they are affiliated with a department that is supported financially by pharmaceutical company, the authors received no current funding for this study and this does not alter their adherence to all the journal policies on sharing data and materials. The other authors have nothing to disclose.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee at which the studies were conducted and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
About this article

Cite this article
Okamura, T., Hashimoto, Y., Hamaguchi, M. et al. Triglyceride–glucose index is a predictor of incident chronic kidney disease: a population-based longitudinal study. Clin Exp Nephrol 23, 948–955 (2019). https://doi.org/10.1007/s10157-019-01729-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10157-019-01729-2