
Abstract
Spinal dural arteriovenous fistula (SDAVF) is also known as a type 1 spinal arteriovenous malformation, representing the most frequent vascular malformation of the spine. A high suspicion index is often required for the initial diagnosis of SDAVF because of subtle magnetic resonance imaging signs. We present the case of a patient with SDAVF associated with syringomyelia of the thoracic spinal cord and hypothesize that a fistula might induce intramedullary fluid accumulation due to venous hypertension, which leads to syrinx formation.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Main text
A 61-year-old male presented with progressive lower-limb weakness, numbness, and urinary retention for 10 months. Physical examination revealed that the muscle strength of both legs was grade 3/5. Symmetric paresthesia occurred below T6 sensory level. Spinal magnetic resonance imaging (MRI) revealed a large syrinx formation from T5 to T9 and multiple flow voids around the swollen spinal cord (Fig. 1A, B). Spinal digital subtraction angiography (DSA) showed a fistulous point at the T4 level with dilation of perimedullary vein drainage downward, confirming the presence of an arteriovenous fistula (Fig. 1C, D). The fistula was disconnected through a left T4 hemilaminectomy. Angiography showed successful obliteration of the serpiginous veins (Fig. 1E). The patient demonstrated motor and sensory improvement, recovering to near-normal walking 3 months after the procedure, with minimal urinary complaints. Follow-up MRI performed 6 months after the surgery showed resolution of the syrinx and reduction of the surrounding edema (Fig. 1F, G).

A Sagittal MRI shows T2-weighted hyperintensity throughout the thoracic spinal cord. A syrinx was noted (arrow) from T5-T9, with numerous serpiginous dorsal epidural flow voids (arrowheads) are apparent. B Axial T2-weighted MRI reveals the syrinx at the T7 level. Early C and late D angiography demonstrates the tortuous drainage vein (arrowheads). E Post-operation angiography reveals the disappearance of the drainage vein. Axial F and sagittal G views of MRI at the T7 level show the resolution of syrinx (arrow) after the procedure
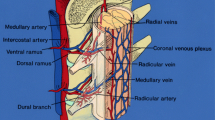
Spinal dural arteriovenous fistula (SDAVF) is a type one spinal arteriovenous malformation with an estimated incidence rate of 5~10/million/year [1]. They are typically located at the dural sleeve of the nerve root and are abnormal shunts between a segmental radiculomeningeal artery and a radicular vein. It can cause spinal cord congestion and lead to intramedullary edema, chronic hypoxia, and progressive myelopathy. Syringomyelia, a fluid-filled cavity in the spinal cord, can be associated with various disorders, most commonly the Chiari type I malformation, followed by intramedullary tumor, spinal cord trauma, and arachnoiditis. To our knowledge, case reports of syringomyelia associated with SDAVF are scarce in the literature. Singh et al. postulated that the fistula caused venous congestion, resulting in edema, and the syrinx began with obstruction of the CSF within the spinal subarachnoid space [2].
In our case, there was no evidence of Chiari malformation or obstruction at the occipital foramen magnum. During surgery, no arachnoid membrane adhesion was found, and both CSF waves from the rostral and caudal directions were regular. Thus, the absence of CSF blockage indicates that intrinsic medullary mechanisms may play a role in this process. The resolution of cavitation in parallel with the fistula and spatial co-occurrence of the syrinx and venous drainage revealed a causal connection between these two entities. We hypothesized that chronic venous congestion and vasogenic edema might contribute to syrinx development. Venous congestion inhibits drainage and contributes to the accumulation of extracellular fluid in the spinal cord, resulting in the extension of the edema. The syrinx formation occurs when circulation and absorption cannot compensate for this production [3]. This theory can be proven by the fact that the syrinx shrank after the venous pressure reduction following the disconnection of the fistula.
Since SDAVF is a rare and subtle MRI finding of flow voids, there is a potential for error or delay in diagnosis. A case of SDAVF associated with syrinx was reported for misdiagnosing as a spinal immunological disorder and treated with corticosteroids, which caused acute deterioration [4]. DSA should be considered to rule out fistula when encountering a syrinx without any readily identifiable cause.
In conclusion, our findings suggest that SDAVF can induce intraspinal fluid accumulation due to a change in intramedullary microvascular pressure resulting from venous hypertension. Consequently, syrinx formation occurs. Furthermore, SDAVF should be excluded if a syrinx is accompanied by spinal cord edema.
References
Krings T, Geibprasert S (2009) Spinal dural arteriovenous fistulas. AJNR Am J Neuroradiol 30(4):639–648
Singh R, Deshmukh N, Lalla R, Khadilkar S (2020) Syringomyelia associated with spinal dural arteriovenous fistula: clinical and radiological improvement after embolization. Neurointervention 15(3):140–143
Fischbein NJ, Dillon WP, Cobbs C, Weinstein PR (1999) The “presyrinx” state: a reversible myelopathic condition that may precede syringomyelia. AJNR Am J Neuroradiol 20(1):7–20
Finsterer J, Bavinzski G, Ungersböck K (2000) Spinal dural arteriovenous fistula associated with syringomyelia. J Neuroradiol 27(3):211–214
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical approval
Ethical approval is obtained from the local ethics committee.
Informed consent
Written informed consent is obtained from the patient.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Xu, W., Ye, M. & Sun, L. Syringomyelia secondary to thoracic spinal dural arteriovenous fistula presenting as paraparesis. Neurol Sci 44, 2985–2986 (2023). https://doi.org/10.1007/s10072-023-06809-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10072-023-06809-6