
Abstract
Synoviocytes are located in the synovium lining layer, which is composed of macrophage-like synoviocytes (MLS) and fibroblast-like synoviocytes (FLS) with different characteristics. Mitochondria, which exist in most cells, are two membrane-covered organelles. In addition to providing the necessary ATP for synoviocytes, mitochondria are involved in the regulation of redox homeostasis and the integration of synoviocytes death signals. In recent years, mitochondrial dysfunction has been found in rheumatoid arthritis (RA) and osteoarthritis (OA). Interestingly, recent studies have started uncovering that mitochondria that were previously reported to play a role in chondrocytes or immune cells, but not known to have pronounced roles in synoviocytes, can actually play crucial roles in the regulation of the pathological properties of the synoviocytes. The purpose of this review is to summarize our current understanding of the key role of mitochondria in synoviocytes, including mitochondrial dysfunction in synoviocytes can induce and aggravate inflammatory responses and changes in mitochondrial structure and function with the involvement of multiple cytokines, signal pathway, and hypoxic state of synovial tissue alter the response of synoviocytes to apoptotic stimulation. Also, mitochondrial abnormalities in synoviocytes promote the synoviocytes invasion and proliferation.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The synovium is a special loose connective tissue that attaches to the edge of articular cartilage and inwardly to the non-articular area of the capsule, covering the surface of the capsule, internal ligaments, bones, and tendons. Its main function is to produce synovial hormone and hyaluronic acid, thus through the synovial fluid to help cartilage obtain nutrition. Normally, the synovial membrane has two layers: the intimal lining layer and the sublining layer. Synoviocytes are located in the synovium lining layer, which is composed of macrophage-like synoviocytes (MLS) and fibroblast-like synoviocytes (FLS) with different characteristics [1].
The detailed ontogeny of FLS is unclear, although it has been reported that FLS are mesenchymal stem cells and display typical properties of fibroblasts, including expression of CD90 (Thy-1), type IV, and V collagens, and vimentin [2]. Fibroblast-like synoviocytes are more abundant than MLS and are mainly characterized by the production of lubricin and hyaluronan, the main constituent of synovial fluid and extracellular matrix [3]. In addition, FLS also express cadherin-11, vascular adhesion molecule 1(VCAM-1), and are involved in the synthesis and degradation of cartilage and bone [2]. Macrophage-like synoviocytes most certainly are derived from embryonic precursor cells, but the detailed ontogeny is still cramped. Immunohistochemical studies have shown that MLS has characteristic surface receptors of macrophages, with the function of phagocytic intracellular debris, foreign bodies, and cell delivery [4]. In vitro, macrophage-like synoviocytes express DR antigens, Fc receptors, and monocyte/macrophage markers CD14 and CD68. MLS has a limited life span, rarely surviving more than a few weeks in vitro. After three or four generations, proliferating FLS are the dominant cell type [2].
In response to environmental stimuli (include infection and/or tissue injuries), synoviocytes are activated. Activated FLS secrete some cytokines to start or exacerbate inflammation like interleukin (IL)-6, a main proinflammatory factor [5]. In certain disease stimuli, such as rheumatoid arthritis (RA), activated FLS have characteristics of excessive proliferation and resistance to apoptosis, which lead to an increase in the number of FLS [4]. The hyper survival character of FLS in RA is regarded as tumor-like behavior. In addition, activated FLS secrete mediators, such as matrix metalloproteinase (MMP) and VCAM-1, to invade the articular cartilage [2, 6]. Compared with FLS, activated MLS produce mainly proinflammatory cytokines, such as IL-1 and tumor necrosis factor α (TNFα), to accelerate inflammation by recruiting other immune cells and activating FLS [4].
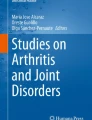
Mitochondria are two membrane-covered organelles that exist in most cells. Mitochondria are composed of four functional areas: mitochondrial outer membrane (OMM), mitochondrial intermembrane space, mitochondrial inner membrane (IMM), and mitochondrial matrix. OMM contains membrane pore proteins and Bcl-2 family proteins which control the substances in and out of mitochondria and regulate mitochondrial apoptosis [7]. Complexes I, II, III, and IV in the electron transport chain (ETC) of mitochondria and ATP synthase are mainly located in IMM, where it is the main site of synthesis of ATP. Mitochondrial intermembrane space mainly contains cytochrome c (Cyto c), apoptosis-inducing factor (AIF), second mitochondria-derived activator of caspases (Smac), and procaspases 3 and 9. These substances play an important role in mitochondria-mediated apoptosis [8]. Mitochondrial matrix contains genetic material such as mitochondrial DNA (mtDNA), as well as many proteins related to energy metabolism.
In the process of consuming oxygen to synthesize ATP, mitochondria produce reactive oxygen species (mtROS) due to proton leakage in ETC. ROS provokes oxidation of biological molecules including mitochondrial DNA, lipids, and proteins. Oxidative mtDNA damage causes the formation of pro-mutagenic DNA adducts such as 8-oxo-7, 8-dihydro-2′-deoxyguanine (8-oxo-dG). Oxidation of polyunsaturated fatty acids in mitochondrial membranes results in the production of 4-hydroxynonenal (4-HNE), which can impair structure and biological properties of DNA, phospholipids, and nucleophilic amino acids of mitochondria [9,10,11]. In general, mtROS increases the risk of mtDNA mutation and impairment of ATP synthesis, which contributes to overall mitochondrial dysfunction [12].
In addition to providing the necessary ATP for synoviocytes, mitochondria are involved in the regulation of redox homeostasis and the integration of synoviocytes death signals [13]. In recent years, mitochondrial dysfunction has been found in RA and osteoarthritis (OA) [14, 15]. Interestingly, studies have started uncovering that mitochondria that were previously reported to play a role in chondrocytes or immune cells, but not known to have pronounced roles in synoviocytes, can actually play crucial roles in the regulation of the pathological properties of the synoviocytes. The purpose of this review is to summarize our current understanding of the key role of mitochondria in synoviocytes (Fig. 1).

Structure and function of mitochondria. Mitochondria are composed of four functional areas: OMM, mitochondrial intermembrane space, IMM, and mitochondrial matrix. OMM contains membrane pore proteins which control the flow of material in and out of mitochondria and regulate mitochondrial apoptosis. Complexes I, II, III, and IV in the ETC of mitochondria and ATP synthase are mainly located in IMM, where it is the main site of synthesis of ATP. Mitochondrial intermembrane space mainly contains Cyto c and other proapoptotic factors. Mitochondrial matrix contains genetic material such as mtDNA, as well as many proteins related to energy metabolism. In the process of consuming oxygen to synthesize ATP, mitochondria mtROS due to proton leakage in ETC. ROS provokes oxidation of biological molecules including mitochondrial DNA, lipids, and proteins. OMM, mitochondrial outer membrane; IMM, mitochondrial inner membrane; ETC, electron transport chain; Cyto c, cytochrome c; mtDNA, mitochondrial DNA; and mtROS, mitochondria produce reactive oxygen species
The role of mitochondria in synoviocytes
Mitochondria are the key organelles in synoviocytes for the synthesis of ATP by aerobic respiration and the regulation of apoptosis. Many studies have shown that the abnormality of synoviocytes is related to the changes of mitochondrial morphology, increased mtROS, and the damage of mitochondrial function. However, whether these changes in mitochondrial function and structure can directly cause synoviocytes abnormalities, or whether changes in related cytokines and signal pathways caused by mitochondrial abnormalities can directly promote changes of synoviocytes and cause the occurrence of related diseases, is still a new field to be studied.
The physiological function of mitochondria in synoviocytes
Mitochondria, indispensable organelles in mammalian cells, synthetize ATP to provide energy for cells by performing the Krebs cycle and oxidative phosphorylation. In addition to ATP production, mitochondria in synovial cells are also involved in many other important cellular functions. For example, mitochondria produce superoxide radicals to synthesize hydrogen peroxide during electron transport in the respiratory chain. Hydrogen peroxide is a relatively stable ROS that has been postulated to play an important role in controlling energy metabolism, the cell cycle, and the expression of numerous redox-sensitive genes [16,17,18]. Moreover, mitochondria play a crucial role in the regulation of programmed apoptosis of dysfunctional synoviocytes by regulating the membrane potential, which is vital to maintain the homeostasis.
Mitochondrial dysfunction promotes the inflammation of synoviocytes
Inflammation of synoviocytes is a cellular and molecular response to certain stimuli such as trauma, infection, and other damage factors. Some studies confirm that the severity of inflammation in synoviocytes is closely related not only to the degree of pain, but also to a loss of articular cartilage and bone destruction [19, 20]. The mechanism of inflammation in synoviocytes is complicated and plays an important role in the pathogenesis of inflammatory joint disease.
Recent studies suggest that mitochondria have powerful immune activities. Because they share a common ancestor, the main components of mitochondria have many similarities with bacteria. Therefore, when mitochondrial components are released into the cytoplasm, they may act as damage-associated molecular patterns (DAMPs), which will be recognized by innate immune receptors [21]. Like bacterial DNA, endogenously oxidized mtDNA instead of nuclear DNA stimulate nuclear factor kappa-B (NF-κB), an important signaling pathway associated with inflammation and decreased apoptosis, and resulted in the production of TNFα as a result of its content of unmethylated CpG motifs [22]. Because mtDNA is close to electron transport chain reaction and mtDNA damage repair efficiency is low, it is easy to become the target of oxidative damage. Oxidative mtDNA results in the formation of 8-oxo-dG, a pro-mutagenic DNA adducts. Studies have shown that the number of mutations of MT-ND1 gene for mitochondrially encoded NADH dehydrogenase 1 of FLS mitochondria from RA patients is approximately twice that of the OA group, which may influence cellular function, contributing to the acquisition of transformed properties of FLS. In addition, some mtDNA mutation of FLS has resulted in potential non-self major histocompatibility complex (MHC) peptide epitopes, which will be recognized by the immune system, aiding in the recruitment of T cells and inflammatory factors [23,24,25].
Mitochondria-derived ROS, which is known as mtROS, is produced as a byproduct of the mitochondrial electron transport chain. mtROS has an established role in inflammation, as it has been shown to activate the NLRP3 inflammasome, one pathway for the secretion of IL-1β and generation of active caspase-1 [26]. Studies indicate that ROS can mediate IL-1β-induced cyclooxygenase-2(COX-2) expression in human synovial fibroblasts [27]. In addition, mtROS are strongly implicated in TNF-α and may mediate the activation of NF-κB [28]. Marta et al. reported that mitochondrial dysfunction induced by oligomycin (OLI), an inhibitor of mitochondrial ATP synthase, significantly stimulated mtROS production as well as low-grade expression of inflammatory cytokines such as COX-2, prostaglandin E2 (PGE2), and IL-8 in cultured synoviocytes. This phenomenon seems to depend on the production of mtROS and the activation of NF-κB. Furthermore, resveratrol, a natural antioxidant, significantly reduced the inflammatory response by decreasing mtROS production and NF-κB activation [29]. The experiment confirmed that mitochondrial dysfunction could induce a low-grade inflammatory response and synergistically intensify the expression of cytokine-induced inflammatory mediators in normal human synoviocytes. Additionally, animal studies have shown that OLI-induced mitochondrial dysfunction can increase mtROS, 4-hydroxy-2-nonenal(4-HNE), as well as the expression of nuclear factor erythroid 2-related factor 2 (Nrf2), an oxidative stress-related transcription factor, which induces an inflammatory response in the rat knee joint [30]. Studies suggest that mitochondrial dysfunction of FLS mediated by tumor necrosis factor like cytokine 1A/tumor necrosis factor receptor 2(TL1A/TNFR2) axis may amplify the expression of IL-1β, IL-6, and IL-8 by regulating mtROS production [31]. In addition, tumor necrosis factor receptor 1(TNFR1) mutant mouse fibroblasts show evidences of altered mitochondrial function, with increased mtROS generation and sustained mitogen-activated protein kinases (MAPK) activity, which enhances innate immune responses [32].
Hypoxia is a basic metabolic environment common in many inflammatory diseases. In this environment, the functional state of synoviocytes is highly susceptible. Hypoxia increases mitochondrial membrane potential by activating mitochondrial ATP-sensitive potassium channels, thus inducing ROS overproduction. Hypoxia-induced mitochondrial dysfunction drives mitochondrial genome mutagenesis in rheumatoid arthritis fibroblast-like synoviocytes (RAFLS) [25, 33, 34]. Studies indicate that some mitochondrial mutation of synoviocytes has resulted in potential non-self MHC peptide epitopes, which may be recognized by the immune system [23, 35]. In addition, synovial tissue mtDNA mutation frequency correlated with synovial fluid expression of TNFα and interferon γ (IFNγ), two common pro-inflammatory cytokines [36]. Synoviocytes exposed to 1% hypoxia exhibited elevated accumulation of 8-oxodG and 4-HNE [25]. 4-HNE significantly increased secretion of IL-8, a key pro-inflammatory factor [18]. TNF blocking therapy can significantly inhibit oxidative stress and hypoxia-induced mitochondrial mutations, thereby improving inflammation [37]. Furthermore, TNFα significantly induces mtDNA mutation, coupled with increased ROS production, mitochondrial membrane potential, and mitochondrial mass in RAFLS [36].
All together, these evidences suggest that mitochondrial dysfunction promotes the release of proinflammatory mediators and the aggregation of inflammatory cells, thus promoting the inflammation of synoviocytes. Notably, these inflammatory mediators, released by mitochondrial dysfunction, in turn stimulate the new synoviocytes, leading to mitochondrial damage in new synovial cells, creating a vicious cycle (Fig. 2).

Mitochondrial dysfunction promotes the inflammation of synoviocytes. Mitochondria-derived ROS that be known as mtROS, are produced as a byproduct of the mitochondrial electron transport chain. Hypoxia-induced mitochondrial dysfunction drives mtROS overproduction and results in elevated accumulation of 4-HNE, which promotes the expression of IL-8. TL1A/TNFR2 axis may amplify the expression of IL-1β, IL-6, and IL-8 by regulating mtROS production. mtROS are strongly implicated in TNF-α and may mediate the activation of NF-κB. Similarly, ROS can mediate IL-1β-induced COX-2 expression in human synovial fibroblasts. TL1A/TNFR2, tumor necrosis factor like cytokine 1A/tumor necrosis factor receptor 2; mtROS, mitochondria produce reactive oxygen species; 4-HNE, 4-hydroxynonenal; IL, interleukin; TNF-α, tumor necrosis factor α; NF-κB, nuclear factor kappa-B; COX-2, cyclooxygenase-2
Abnormal mitochondrial structure and function inhibit the apoptosis of synoviocytes
Apoptosis is the activation of the death pathway of cells induced by specific endogenous and exogenous signals. As the main executor of endogenous pathway of programmed cell death, mitochondria have many mediators to regulate apoptosis. The key for the initiation of mitochondrial-mediated apoptosis pathway is the increased permeability of the outer membrane of mitochondria, which leads to the apoptotic factors of mitochondria, such as Cyto c, AIF, and Smac, into the cytoplasm. (Fig. 3).

Abnormal mitochondrial function inhibits the apoptosis of synoviocytes. TNFα activate Bid by caspase-8, which impairs mitochondrial integrity by promoting the aggregation of Bax and Bak. The activation of NF-κB by TNFα upregulates the anti-apoptotic molecule A1; TL1A, IL-17, IL-6, and IL-15 upregulate the anti-apoptotic molecule Bcl-2; IL-15 upregulates the anti-apoptotic molecule Bcl-xl; together, these factors maintain mitochondrial integrity by inhibiting the aggregation of Bax and Bak. Following the deficiency of mitochondrial integrity, cytochrome c is released, activating caspase 9 and subsequently caspase 3, which performs DNA fragmentation via a CAD. In addition, Smac/DIABLO and Omi/HtrA2 can block the activity of IAPs. AIF and EndoG can perform DNA fragmentation directly. TNFα, tumor necrosis factor α; NF-κB, nuclear factor kappa-B; TL1A, tumor necrosis factor like cytokine 1A; IL, interleukin; CAD, caspase-activated DNase; Smac/DIABLO, Second mitochondria-derived activator of caspases/direct inhibitor of apoptosis-binding protein with low pI; Omi /HtrA2, heat requirement A2 protein; IAPs, inhibitor of apoptosis proteins
Structural changes in mitochondria may play an important role in the resistance to apoptosis of synoviocytes. In 1988, a team of researchers linked mitochondrial abnormalities to synoviocytes by finding large, abnormally expanded mitochondria in early RAFLS [38]. Studies which were performed to assess the role of extracellular cytochrome c proposed that the decrease of Cyto c level reflects its consumption in synovial tissue to resist apoptosis [39]. In addition, the experiment demonstrates the decreased expression of Cyto c in TL1A-treated RAFLS, which might contribute to making RAFLS more resistant to apoptosis [31]. Interestingly, Kim et al. reported that IL-17, a well-known pro-inflammatory cytokine, impairs apoptosis in RAFLS via mitochondrial dysfunction-mediated autophagy (a phenomenon in which cells clear aging and damaged mitochondria) [40].
The Bcl-2 family protein is a key regulatory molecule of cell apoptosis, and mitochondria are the targets for its regulation of the internal apoptotic pathway. The integrity of the mitochondrial outer membrane is regulated by the balance between pro-apoptotic factors and anti-apoptotic factors in the Bcl-2 family protein [41, 42]. Evidence also suggests that enhanced expression of anti-apoptotic factors of Bcl-2 family members such as Bcl-2 and Bcl-xl in synoviocytes contributes to the survival of synoviocytes [43, 44]. The potential mechanisms of Bcl-2 family member expression change have been examined. The recent research shows that IL-17 reduces the expression of the genes for oxidative phosphorylation complex components, which may result in impaired respiratory capacity in mitochondria of FLS. Furthermore, IL-17 is a potent inhibitor of apoptosis of synoviocytes by increasing the expression of Bcl-2 [40]. IL-15, a cytokine with antiapoptotic properties, can also increase the expression of Bcl-xl and Bcl-2, thus promoting the apoptosis of synoviocytes [45]. In addition, study confirms that IL-6/sIL-6R complex might contribute to inhibit apoptosis in FLS via increased expression of Bcl-2 and NF-κB activation [46]. Similarly, TL1A/TNFR2-mediated mitochondrial dysfunction contributes to making FLS more resistant to apoptosis via increased expression of Bcl-2 and downregulation of apoptotic factor caspase-8 [31].
NF-κB, a signal pathway known to have an anti-apoptotic effect, has been shown to be activated by TNFα, which might upregulate the anti-apoptotic molecules A1, thus promoting the resistance of synoviocytes to apoptosis. Inhibition of NF-κB activation sensitized FLS to TNFα-induced apoptosis via cleavage and activation of Bid, a pro-apoptotic of Bcl-2 family members, by caspase-8. In addition, the activation of NF-κB was found to block the activation of caspase-8 [8, 47, 48].
It has been confirmed that hypoxia induces the Bcl-2/adenovirus E1B 19-kd protein-interacting protein 3 (BNIP-3) excessive expression, so as to promote apoptosis of synoviocytes. But its proapoptotic effects may be inhibited by TNFα and IL-1β [49]. This provides a link between inflammation and resistance to apoptosis.
In general, the resistance of synoviocytes to apoptosis is a rather complex process in which changes in the structure and function of mitochondria play an important role. Cytokines such as IL-15, IL-17, IL-6, TNFα, and TL1A, signal pathways such as NF-κB, and hypoxic state of the synovial tissue are also involved (Fig. 3).
Mitochondrial abnormalities promote the invasiveness of synoviocytes
Synoviocytes invasion is an important cause of cartilage and bone destruction, and the mechanisms are complex. FLS produce several enzymes such as matrix metalloproteinases (MMP) and collagenases that are important for their invasive features and contribute to tissue destruction. In addition, the invading synoviocytes express several adhesion molecules, such as VCAM-1 and various integrins that influence adjacent chondrocytes to produce enzymes that degrade the local extracellular matrix [4, 50]. Henrotin, Y. E et al. reported that ROS produced by FLS stimulates FLS to secrete MMP, inhibits cartilage matrix synthesis, and accelerates bone resorption [51]. In addition, hypoxia-induced abnormal mitochondrial morphology and mitochondrial dysfunction induce lactate secretion in FLS, which in turn induced FLS invasion [52]. Thus, mitochondrial abnormalities promote the invasiveness of synoviocytes.
Mitochondrial abnormalities promote synoviocytes proliferation
Synovial proliferation occurs mainly due to the accumulation of FLS and MLS. Compared with FLS, MLS has little or no proliferation in vitro [4]. By and large, synoviocytes proliferation is difficult to prove. Growth of the synoviocytes population is more likely due to an imbalance between cell proliferation, survival, and death. Basic fibroblast growth factor (bFGF) is a kind of heparin-binding protein that promotes cell division and can induce the proliferation and differentiation of many kinds of cells [53]. Studies suggest that hypoxia-induced abnormal mitochondrial morphology of RAFLS might induce secretion of bFGF in vitro, thus leading to synoviocytes proliferation [52]. 4-HNE, an important product of mitochondrial dysfunction, also has been shown to significantly increase bFGF secretion [18]. In addition, research suggests that ROS produced by mitochondria can increase mtDNA mutational burden. If the mutation occurs in genes promoting cell survival, mtDNA mutational may promote synoviocytes proliferation [35]. All together, these experiments confirmed the relationship between mitochondrial abnormalities and synoviocytes proliferation.
Mitochondria are involved in the pathogenesis of diseases
The mitochondria in RA pathogenesis
RA is a complex autoimmune disease characterized by synovial hyperplasia and infiltration of inflammatory cells, leading to pannus and destruction of articular cartilage and bone [54]. A large number of scientific studies have confirmed that the continuous activation and invasion of RAFLS play a very important role in the inflammatory response and cartilage and bone damage, so it has been regarded as the main target cell of RA by scholars in recent years.
Over the past few years, a growing body of research has strongly suggested that mitochondrial dysfunction plays an important role in RA. Injury and necrosis of synoviocytes induce the release of mitochondrial damage-associated molecular patterns (DAMPs), such as N-formyl peptides, mtDNA, and ATP, from damaged mitochondria, which trigger innate or adaptive immune responses by activating cell surface receptors or intracellular receptors, thus promote the release of proinflammatory mediators and the aggregation of inflammatory cells [55]. In addition, the hypoxic environment in the synovial membrane can also cause mitochondrial dysfunction of synoviocytes and increase of mtROS, leading to the formation of oxidative stress. Oxidative stress results in peroxidation of biological molecules including DNA, lipids, and proteins such as 4-HNE and 8-oxo-dG. These molecules further promote glycolysis and perpetuate inflammation [56, 57]. Experimental and clinical studies report that compared with OA, synoviocytes of RA has the obvious anti-apoptotic ability in vivo and in vitro [58]. Several studies have found that changes in mitochondrial function and structure can promote the resistance of synoviocytes to apoptosis. In addition, cytokines such as IL-15, IL-17, IL-6, TNFα, and TL1A, signal pathway such as NF-κB, and hypoxic state of the synovial tissue are also involved.
The incidence of RA increases with age. Some studies suggest that RA may be caused by premature aging of the immune system. Mitochondrial dysfunction is a feature of aging. Induction of ROS and mtDNA mutations in synovium are relevant to RA pathogenesis. However, mtDNA mutation frequency in RA was independent of age [59]. In addition, the increase of mtDNA mutations was found only when compared with OA and not when compared with psoriatic arthritis [35, 36].
Mitochondria have also become a key target for the treatment of RA. Methotrexate (MTX), a basic drug of the disease-modifying anti-rheumatic drug (DMARD), induces apoptosis of synoviocytes by the alteration of the intracellular ROS levels. Studies have shown that whether methotrexate can induce synoviocytes apoptosis is an indication of the effectiveness of the drug [60]. As a proinflammatory cytokine with the function of increasing mitochondrial ROS production, TNF-α plays a crucial role in the pathogenesis of rheumatoid arthritis. Successful anti-TNF-α treatment alters the levels of early mitochondrial genome alterations, improving synovial hypoxia and joint inflammation [37, 61]. In addition, C. Derambure et al. reported that pre-silencing of genes involved in the electron transport chain (ETC) pathway is associated with responsiveness to abatacept, a selective T cell co-stimulation modulators [62]. Topatinib is a novel oral small molecule drug for RA, blocking cytokine signal in the cell by inhibiting JAK1, inhibiting abnormal immune signal transduction. Experiments report that tofacitinib significantly decreased mitochondrial membrane potential, mitochondrial mass, and reactive oxygen species production by RAFLS and differentially regulated key mitochondrial genes [63]. In particular, studies have pointed out that apoptosis induction of fibroblast-like synoviocytes by mitochondrial pathway is an important molecular-mechanism for herbal medicine along with its components in treating rheumatoid arthritis [64].
The mitochondria in OA pathogenesis
Osteoarthritis (OA) is a chronic degenerative disease characterized by chronic pain and dysfunction. The main pathological features of osteoarthritis include osteophyte formation, subchondral osteosclerosis, abnormal vascularization, and degeneration of articular cartilage [65]. Numerous studies have confirmed that mitochondrial dysfunction in chondrocytes can play an important role in OA pathogenesis, including disabling respiratory chain activity and resulting in chondrocyte biosynthesis defects, producing ROS to induce the inflammation of cartilage, degrading extracellular matrix by inducing chondrocytes to secrete matrix metalloproteinase, and promoting apoptosis of chondrocytes by activating mitochondrial mediated apoptosis pathway [66,67,68]. However, involvement in the super early pathogenesis of OA, synovitis, and synovial-related inflammatory factors can also induce the degradation and destruction of articular cartilage, thus promoting the development of OA [1]. Therefore, in recent years, more and more scholars have shifted their focus from cartilage to synovium.
Mitochondrial dysfunction in synoviocytes promotes the development of OA by promoting the inflammatory response of synoviocytes and reducing the survival ability of synoviocytes. In cultured synoviocytes, hypoxia can induce the loss of mitochondrial membrane potential (MMP), thus promoting the generation of ROS, which might active the NF-kB signal pathway and increase the level of TNF-α-induced proinflammatory cytokines such as C-C chemokine ligand 5 (CCL5), IL-1β, and IL-6 [69]. These results suggest that hypoxia-induced mitochondrial dysfunction in synoviocytes may play a role in inducing inflammation, contributing to osteoarthritis pathogenesis. Because NO is increased in OA, and NO is known to induce the generation of ROS, studies were performed to investigate the effects of NO on survival and activity of osteoarthritis FLS. Sodium nitroprusside (SNP), a NO donor compound, at 0.5 mM increase the activity of complexes I and III, but reduce citrate synthase activity, which indicates a decrease in mitochondrial mass. Furthermore, SNP decrease Bcl-2 and procaspase-3 protein expression [70]. This experiment showed that NO could induce mitochondrial dysfunction, thus reducing the survival rate of osteoarthritis FLS.
Aging and OA are closely linked; mitochondrial dysfunction is characterized by reduced mitochondrial integrity (quality, quantity, and DNA content) and impaired function of electron transport chains in both aging and OA. The researchers confirmed that age-related elevated levels of ROS and oxidative stress can disrupt normal physiological signaling such as insulin-like growth factor 1 (IGF1) and mitogen-activated protein kinase (MAPK) signaling pathways, which contribute to osteoarthritis [71]. In addition, considering the close link between aging and mtDNA, the researchers investigated the correlation between OA and the 4977-bp mtDNA deletion. They concluded that accumulation of the 4977-bp deletion of mtDNA in knee cartilage increases with age, which may be involved in the occurrence of OA [72]. In particular, studies have shown a relationship between mtDNA haplogroups and OA [67]. The group of Jie Fang has demonstrated recently that Cluster TJ can help reduce the prevalence, slowing down the radiographic changes; however, the impacts came mainly from type J and type T, respectively [73]. In addition, folate deficiency induces apoptosis of synoviocytes by promoting the overproduction of ROS from NADPH oxidase/mitochondrial complex II and calcium perturbation [74].
In conclusion, mitochondria play an important role in synoviocytes, whose dysfunction can not only induce synovitis, but also promote the apoptosis of synoviocytes, which promotes the occurrence and development of OA.
The mitochondria in psoriatic arthritis pathogenesis
Psoriatic arthritis (PsA) is an inflammatory joint disease associated with psoriasis, with a psoriatic rash accompanied by pain, swelling, tenderness, stiffness, and dyskinesia. The end-stage of this disease can lead to impaired skeletal sites of rigidity and deformation [75]. The pathogenesis of the disease is unclear. Studies have shown that an increased number of FLS and osteoclasts in the synovial membrane of PsA patients, and deregulation of apoptosis may contribute to the perpetuation of the inflammatory process, which means that PsA may have some similar mechanisms to rheumatoid arthritis [76, 77].
Mitochondrial dysfunction could contribute to the pathogenesis of psoriasis (Ps) and Ps-arthritis (PsA). Recent studies reported that altered levels of oxidative metabolites, for example, hydroperoxides and carbonyl groups, were detected in PsA patients when compared to healthy person [77]. A similar study, showed a higher ROS production and DNA damage were found in synovial fluid of PsA patients when compared to an OA group [78]. In addition, similar to RA, hypoxia-induced mitochondrial dysfunction can induce oxidative stress and the production of pro-inflammatory cytokines in synovial fluid of PsA patients [79]. These studies confirm the role of mitochondrial dysfunction in PsA. In particular, to test the association between mtDNA variants and Ps/PsA, Pablo and his colleague found a significantly lower frequency of haplogroup J among patients with PsA. Haplogroup J contains some mtDNA functional variant linked to a reduced ROS production, so this also suggests that mtDNA may have a role in PsA [80].
Conclusion
Mitochondria in synoviocytes are important mediators in the pathogenesis of OA and RA. The integrity and proper functioning of the mitochondria are important for maintaining the function of synoviocytes. Mitochondrial dysfunction in synoviocytes can induce and aggravate inflammatory responses. Changes in mitochondrial structure and function with the involvement of multiple cytokines, signal pathway, and hypoxic state of synovial tissue alter the response of synoviocytes to apoptotic stimulation. In addition, mitochondrial abnormalities in synoviocytes promote the synoviocytes invasion and proliferation.
Although the important role of mitochondria in synoviocytes has been confirmed by scholars in recent years, the data on their specific mechanisms are limited and need to be further explained. Moreover, considering the role of mitochondria in promoting inflammation and causing oxidative damage, it will also be necessary to explore more specific mechanisms of natural anti-inflammatory and antioxidant drugs on mitochondria.
References
Mathiessen A, Conaghan PG (2017) Synovitis in osteoarthritis: current understanding with therapeutic implications. Arthritis Res Ther 19(1):18. https://doi.org/10.1186/s13075-017-1229-9
Bartok B, Firestein GS (2010) Fibroblast-like synoviocytes: key effector cells in rheumatoid arthritis. Immunol Rev 233(1):233–255. https://doi.org/10.1111/j.0105-2896.2009.00859.x
Chang SK, Gu Z, Brenner MB (2010) Fibroblast-like synoviocytes in inflammatory arthritis pathology: the emerging role of cadherin-11. Immunol Rev 233(1):256–266. https://doi.org/10.1111/j.0105-2896.2009.00854.x
Tu J, Hong W, Zhang P, Wang X, Korner H, Wei W (2018) Ontology and function of fibroblast-like and macrophage-like synoviocytes: how do they talk to each other and can they be targeted for rheumatoid arthritis therapy? Front Immunol 9:1467. https://doi.org/10.3389/fimmu.2018.01467
Brennan FM, McInnes IB (2008) Evidence that cytokines play a role in rheumatoid arthritis. J Clin Invest 118(11):3537–3545. https://doi.org/10.1172/JCI36389
Muller-Ladner U, Ospelt C, Gay S, Distler O, Pap T (2007) Cells of the synovium in rheumatoid arthritis. Synovial fibroblasts. Arthritis Res Ther 9(6):223. https://doi.org/10.1186/ar2337
Martinou JC, Youle RJ (2011) Mitochondria in apoptosis: Bcl-2 family members and mitochondrial dynamics. Dev Cell 21(1):92–101. https://doi.org/10.1016/j.devcel.2011.06.017
Calvani R, Joseph AM, Adhihetty PJ, Miccheli A, Bossola M, Leeuwenburgh C, Bernabei R, Marzetti E (2013) Mitochondrial pathways in sarcopenia of aging and disuse muscle atrophy. Biol Chem 394(3):393–414. https://doi.org/10.1515/hsz-2012-0247
Phull AR, Nasir B, Haq IU, Kim SJ (2018) Oxidative stress, consequences and ROS mediated cellular signaling in rheumatoid arthritis. Chem Biol Interact 281:121–136. https://doi.org/10.1016/j.cbi.2017.12.024
Lunec J, Herbert K, Blount S, Griffiths HR, Emery P (1994) 8-Hydroxydeoxyguanosine. A marker of oxidative DNA damage in systemic lupus erythematosus. FEBS Lett 348(2):131–138. https://doi.org/10.1016/0014-5793(94)00583-4
Zhong H, Yin H (2015) Role of lipid peroxidation derived 4-hydroxynonenal (4-HNE) in cancer: focusing on mitochondria. Redox Biol 4:193–199. https://doi.org/10.1016/j.redox.2014.12.011
Nissanka N, Moraes CT (2018) Mitochondrial DNA damage and reactive oxygen species in neurodegenerative disease. FEBS Lett 592(5):728–742. https://doi.org/10.1002/1873-3468.12956
Wang T, Wang G, Zhang Y, Zhang J, Cao W, Chen X (2019) Effect of lentivirus-mediated overexpression or silencing of MnSOD on apoptosis of resveratrol-treated fibroblast-like synoviocytes in rheumatoid arthritis. Eur J Pharmacol 844:65–72. https://doi.org/10.1016/j.ejphar.2018.12.001
Mitsunaga S, Hosomichi K, Okudaira Y, Nakaoka H, Suzuki Y, Kuwana M, Sato S, Kaneko Y, Homma Y, Oka A, Shiina T, Inoko H, Inoue I (2015) Aggregation of rare/low-frequency variants of the mitochondria respiratory chain-related proteins in rheumatoid arthritis patients. J Hum Genet 60(8):449–454. https://doi.org/10.1038/jhg.2015.50
Blanco FJ, Rego-Perez I (2018) Mitochondria and mitophagy: biosensors for cartilage degradation and osteoarthritis. Osteoarthr Cartil 26(8):989–991. https://doi.org/10.1016/j.joca.2018.05.018
Kowaltowski AJ, de Souza-Pinto NC, Castilho RF, Vercesi AE (2009) Mitochondria and reactive oxygen species. Free Radic Biol Med 47(4):333–343. https://doi.org/10.1016/j.freeradbiomed.2009.05.004
Droge W (2002) Free radicals in the physiological control of cell function. Physiol Rev 82(1):47–95. https://doi.org/10.1152/physrev.00018.2001
Balogh E, Veale DJ, McGarry T, Orr C, Szekanecz Z, Ng CT, Fearon U, Biniecka M (2018) Oxidative stress impairs energy metabolism in primary cells and synovial tissue of patients with rheumatoid arthritis. Arthritis Res Ther 20(1):95. https://doi.org/10.1186/s13075-018-1592-1
Roemer FW, Guermazi A, Felson DT, Niu J, Nevitt MC, Crema MD, Lynch JA, Lewis CE, Torner J, Zhang Y (2011) Presence of MRI-detected joint effusion and synovitis increases the risk of cartilage loss in knees without osteoarthritis at 30-month follow-up: the MOST study. Ann Rheum Dis 70(10):1804–1809. https://doi.org/10.1136/ard.2011.150243
Baker K, Grainger A, Niu J, Clancy M, Guermazi A, Crema M, Hughes L, Buckwalter J, Wooley A, Nevitt M, Felson DT (2010) Relation of synovitis to knee pain using contrast-enhanced MRIs. Ann Rheum Dis 69(10):1779–1783. https://doi.org/10.1136/ard.2009.121426
Meyer A, Laverny G, Bernardi L, Charles AL, Alsaleh G, Pottecher J, Sibilia J, Geny B (2018) Mitochondria: an organelle of bacterial origin controlling inflammation. Front Immunol 9:536. https://doi.org/10.3389/fimmu.2018.00536
Collins LV, Hajizadeh S, Holme E, Jonsson IM, Tarkowski A (2004) Endogenously oxidized mitochondrial DNA induces in vivo and in vitro inflammatory responses. J Leukoc Biol 75(6):995–1000. https://doi.org/10.1189/jlb.0703328
Gu Y, Wang C, Roifman CM, Cohen A (2003) Role of MHC class I in immune surveillance of mitochondrial DNA integrity. J Immunol 170(7):3603–3607. https://doi.org/10.4049/jimmunol.170.7.3603
Ospelt C, Gay S (2005) Somatic mutations in mitochondria: the chicken or the egg? Arthritis Res Ther 7(5):179. https://doi.org/10.1186/ar1809
Biniecka M, Fox E, Gao W, Ng CT, Veale DJ, Fearon U, O'Sullivan J (2011) Hypoxia induces mitochondrial mutagenesis and dysfunction in inflammatory arthritis. Arthritis Rheum 63(8):2172–2182. https://doi.org/10.1002/art.30395
Zhou R, Tardivel A, Thorens B, Choi I, Tschopp J (2010) Thioredoxin-interacting protein links oxidative stress to inflammasome activation. Nat Immunol 11(2):136–140. https://doi.org/10.1038/ni.1831
Fahmi H, He Y, Zhang M, Martel-Pelletier J, Pelletier JP, Di Battista JA (2001) Nimesulide reduces interleukin-1beta-induced cyclooxygenase-2 gene expression in human synovial fibroblasts. Osteoarthr Cartil 9(4):332–340. https://doi.org/10.1053/joca.2000.0393
Woo CH, Eom YW, Yoo MH, You HJ, Han HJ, Song WK, Yoo YJ, Chun JS, Kim JH (2000) Tumor necrosis factor-alpha generates reactive oxygen species via a cytosolic phospholipase A2-linked cascade. J Biol Chem 275(41):32357–32362. https://doi.org/10.1074/jbc.M005638200
Valcarcel-Ares MN, Riveiro-Naveira RR, Vaamonde-Garcia C, Loureiro J, Hermida-Carballo L, Blanco FJ, Lopez-Armada MJ (2014) Mitochondrial dysfunction promotes and aggravates the inflammatory response in normal human synoviocytes. Rheumatology (Oxford) 53(7):1332–1343. https://doi.org/10.1093/rheumatology/keu016
Vaamonde-Garcia C, Loureiro J, Valcarcel-Ares MN, Riveiro-Naveira RR, Ramil-Gomez O, Hermida-Carballo L, Centeno A, Meijide-Failde R, Blanco FJ, Lopez-Armada MJ (2017) The mitochondrial inhibitor oligomycin induces an inflammatory response in the rat knee joint. BMC Musculoskelet Disord 18(1):254. https://doi.org/10.1186/s12891-017-1621-2
Al-Azab M, Qaed E, Ouyang X, Elkhider A, Walana W, Li H, Li W, Tang Y, Adlat S, Wei J, Wang B, Li X (2020) TL1A/TNFR2-mediated mitochondrial dysfunction of fibroblast-like synoviocytes increases inflammatory response in patients with rheumatoid arthritis via reactive oxygen species generation. FEBS J. https://doi.org/10.1111/febs.15181
Bulua AC, Simon A, Maddipati R, Pelletier M, Park H, Kim KY, Sack MN, Kastner DL, Siegel RM (2011) Mitochondrial reactive oxygen species promote production of proinflammatory cytokines and are elevated in TNFR1-associated periodic syndrome (TRAPS). J Exp Med 208(3):519–533. https://doi.org/10.1084/jem.20102049
Hu HL, Zhang ZX, Chen CS, Cai C, Zhao JP, Wang X (2010) Effects of mitochondrial potassium channel and membrane potential on hypoxic human pulmonary artery smooth muscle cells. Am J Respir Cell Mol Biol 42(6):661–666. https://doi.org/10.1165/rcmb.2009-0017OC
Shokolenko I, Venediktova N, Bochkareva A, Wilson GL, Alexeyev MF (2009) Oxidative stress induces degradation of mitochondrial DNA. Nucleic Acids Res 37(8):2539–2548. https://doi.org/10.1093/nar/gkp100
Da Sylva TR, Connor A, Mburu Y, Keystone E, Wu GE (2005) Somatic mutations in the mitochondria of rheumatoid arthritis synoviocytes. Arthritis Res Ther 7(4):R844–R851. https://doi.org/10.1186/ar1752
Harty LC, Biniecka M, O'Sullivan J, Fox E, Mulhall K, Veale DJ, Fearon U (2012) Mitochondrial mutagenesis correlates with the local inflammatory environment in arthritis. Ann Rheum Dis 71(4):582–588. https://doi.org/10.1136/annrheumdis-2011-200245
Biniecka M, Kennedy A, Ng CT, Chang TC, Balogh E, Fox E, Veale DJ, Fearon U, O'Sullivan JN (2011) Successful tumour necrosis factor (TNF) blocking therapy suppresses oxidative stress and hypoxia-induced mitochondrial mutagenesis in inflammatory arthritis. Arthritis Res Ther 13(4):R121. https://doi.org/10.1186/ar3424
Eerola E, Pulkki K, Pelliniemi LJ, Vuorio E, Toivanen A (1988) Abnormal mitochondria in cultured synovial fibroblasts in rheumatoid and reactive arthritis? Br J Rheumatol 27(Suppl 2):128–131. https://doi.org/10.1093/rheumatology/xxvii.suppl_2.128
Pullerits R, Bokarewa M, Jonsson IM, Verdrengh M, Tarkowski A (2005) Extracellular cytochrome c, a mitochondrial apoptosis-related protein, induces arthritis. Rheumatology (Oxford) 44(1):32–39. https://doi.org/10.1093/rheumatology/keh406
Kim EK, Kwon JE, Lee SY, Lee EJ, Kim DS, Moon SJ, Lee J, Kwok SK, Park SH, Cho ML (2017) IL-17-mediated mitochondrial dysfunction impairs apoptosis in rheumatoid arthritis synovial fibroblasts through activation of autophagy. Cell Death Dis 8(1):e2565. https://doi.org/10.1038/cddis.2016.490
Chipuk JE, Green DR (2008) How do BCL-2 proteins induce mitochondrial outer membrane permeabilization? Trends Cell Biol 18(4):157–164. https://doi.org/10.1016/j.tcb.2008.01.007
Ola MS, Nawaz M, Ahsan H (2011) Role of Bcl-2 family proteins and caspases in the regulation of apoptosis. Mol Cell Biochem 351(1–2):41–58. https://doi.org/10.1007/s11010-010-0709-x
Busteed S, Bennett MW, Molloy C, Houston A, Stone MA, Shanahan F, Molloy MG, O'Connell J (2006) Bcl-x(L) expression in vivo in rheumatoid synovium. Clin Rheumatol 25(6):789–793. https://doi.org/10.1007/s10067-005-0191-0
Perlman H, Georganas C, Pagliari LJ, Koch AE, Haines K 3rd, Pope RM (2000) Bcl-2 expression in synovial fibroblasts is essential for maintaining mitochondrial homeostasis and cell viability. J Immunol 164(10):5227–5235. https://doi.org/10.4049/jimmunol.164.10.5227
Kurowska M, Rudnicka W, Kontny E, Janicka I, Chorazy M, Kowalczewski J, Ziolkowska M, Ferrari-Lacraz S, Strom TB, Maslinski W (2002) Fibroblast-like synoviocytes from rheumatoid arthritis patients express functional IL-15 receptor complex: endogenous IL-15 in autocrine fashion enhances cell proliferation and expression of Bcl-x(L) and Bcl-2. J Immunol 169(4):1760–1767. https://doi.org/10.4049/jimmunol.169.4.1760
Kim SK, Park KY, Yoon WC, Park SH, Park KK, Yoo DH, Choe JY (2011) Melittin enhances apoptosis through suppression of IL-6/sIL-6R complex-induced NF-kappaB and STAT3 activation and Bcl-2 expression for human fibroblast-like synoviocytes in rheumatoid arthritis. Joint Bone Spine 78(5):471–477. https://doi.org/10.1016/j.jbspin.2011.01.004
Wang CY, Mayo MW, Korneluk RG, Goeddel DV, Baldwin AS Jr (1998) NF-kappaB antiapoptosis: induction of TRAF1 and TRAF2 and c-IAP1 and c-IAP2 to suppress caspase-8 activation. Science 281(5383):1680–1683. https://doi.org/10.1126/science.281.5383.1680
Liu H, Pope RM (2003) The role of apoptosis in rheumatoid arthritis. Curr Opin Pharmacol 3(3):317–322. https://doi.org/10.1016/s1471-4892(03)00037-7
Kammouni W, Wong K, Ma G, Firestein GS, Gibson SB, El-Gabalawy HS (2007) Regulation of apoptosis in fibroblast-like synoviocytes by the hypoxia-induced Bcl-2 family member Bcl-2/adenovirus E1B 19-kd protein-interacting protein 3. Arthritis Rheum 56(9):2854–2863. https://doi.org/10.1002/art.22853
Muller-Ladner U, Kriegsmann J, Franklin BN, Matsumoto S, Geiler T, Gay RE, Gay S (1996) Synovial fibroblasts of patients with rheumatoid arthritis attach to and invade normal human cartilage when engrafted into SCID mice. Am J Pathol 149(5):1607–1615
Henrotin YE, Bruckner P, Pujol JP (2003) The role of reactive oxygen species in homeostasis and degradation of cartilage. Osteoarthr Cartil 11(10):747–755. https://doi.org/10.1016/s1063-4584(03)00150-x
Biniecka M, Canavan M, McGarry T, Gao W, McCormick J, Cregan S, Gallagher L, Smith T, Phelan JJ, Ryan J, O'Sullivan J, Ng CT, Veale DJ, Fearon U (2016) Dysregulated bioenergetics: a key regulator of joint inflammation. Ann Rheum Dis 75(12):2192–2200. https://doi.org/10.1136/annrheumdis-2015-208476
Nguyen TH, Paluck SJ, McGahran AJ, Maynard HD (2015) Poly (vinyl sulfonate) facilitates bFGF-induced cell proliferation. Biomacromolecules 16(9):2684–2692. https://doi.org/10.1021/acs.biomac.5b00557
Sparks JA (2019) Rheumatoid arthritis. Ann Intern Med 170(1):ITC1–ITC16. https://doi.org/10.7326/AITC201901010
Fearon U, Canavan M, Biniecka M, Veale DJ (2016) Hypoxia, mitochondrial dysfunction and synovial invasiveness in rheumatoid arthritis. Nat Rev Rheumatol 12(7):385–397. https://doi.org/10.1038/nrrheum.2016.69
Quinonez-Flores CM, Gonzalez-Chavez SA, Pacheco-Tena C (2016) Hypoxia and its implications in rheumatoid arthritis. J Biomed Sci 23(1):62. https://doi.org/10.1186/s12929-016-0281-0
McGarry T, Biniecka M, Veale DJ, Fearon U (2018) Hypoxia, oxidative stress and inflammation. Free Radic Biol Med 125:15–24. https://doi.org/10.1016/j.freeradbiomed.2018.03.042
Karami J, Aslani S, Tahmasebi MN, Mousavi MJ, Sharafat Vaziri A, Jamshidi A, Farhadi E, Mahmoudi M (2019) Epigenetics in rheumatoid arthritis; fibroblast-like synoviocytes as an emerging paradigm in the pathogenesis of the disease. Immunol Cell Biol 98:171–186. https://doi.org/10.1111/imcb.12311
Chalan P, van den Berg A, Kroesen BJ, Brouwer L, Boots A (2015) Rheumatoid arthritis, immunosenescence and the hallmarks of aging. Curr Aging Sci 8(2):131–146. https://doi.org/10.2174/1874609808666150727110744
Lee SY, Park SH, Lee SW, Lee SH, Son MK, Choi YH, Chung WT, Yoo YH (2014) Synoviocyte apoptosis may differentiate responder and non-responder patients to methotrexate treatment in rheumatoid arthritis. Arch Pharm Res 37(10):1286–1294. https://doi.org/10.1007/s12272-014-0365-x
Miesel R, Murphy MP, Kroger H (1996) Enhanced mitochondrial radical production in patients which rheumatoid arthritis correlates with elevated levels of tumor necrosis factor alpha in plasma. Free Radic Res 25(2):161–169. https://doi.org/10.3109/10715769609149921
Derambure C, Dzangue-Tchoupou G, Berard C, Vergne N, Hiron M, D'Agostino MA, Musette P, Vittecoq O, Lequerre T (2017) Pre-silencing of genes involved in the electron transport chain (ETC) pathway is associated with responsiveness to abatacept in rheumatoid arthritis. Arthritis Res Ther 19(1):109. https://doi.org/10.1186/s13075-017-1319-8
McGarry T, Orr C, Wade S, Biniecka M, Wade S, Gallagher L, Low C, Veale DJ, Fearon U (2018) JAK/STAT blockade alters synovial bioenergetics, mitochondrial function, and proinflammatory mediators in rheumatoid arthritis. Arthritis Rheumatol 70(12):1959–1970. https://doi.org/10.1002/art.40569
Zhang Q, Liu J, Zhang M, Wei S, Li R, Gao Y, Peng W, Wu C (2019) Apoptosis induction of fibroblast-like synoviocytes is an important molecular-mechanism for herbal medicine along with its active components in treating rheumatoid arthritis. Biomolecules 9(12). https://doi.org/10.3390/biom9120795
Abramoff B, Caldera FE (2020) Osteoarthritis: pathology, diagnosis, and treatment options. Med Clin North Am 104(2):293–311. https://doi.org/10.1016/j.mcna.2019.10.007
Wu L, Liu H, Li L, Liu H, Cheng Q, Li H, Huang H (2014) Mitochondrial pathology in osteoarthritic chondrocytes. Curr Drug Targets 15(7):710–719. https://doi.org/10.2174/1389450115666140417120305
Blanco FJ, Rego I, Ruiz-Romero C (2011) The role of mitochondria in osteoarthritis. Nat Rev Rheumatol 7(3):161–169. https://doi.org/10.1038/nrrheum.2010.213
Vaamonde-Garcia C, Riveiro-Naveira RR, Valcarcel-Ares MN, Hermida-Carballo L, Blanco FJ, Lopez-Armada MJ (2012) Mitochondrial dysfunction increases inflammatory responsiveness to cytokines in normal human chondrocytes. Arthritis Rheum 64(9):2927–2936. https://doi.org/10.1002/art.34508
Zhou S, Wen H, Cai W, Zhang Y, Li H (2019) Effect of hypoxia/reoxygenation on the biological effect of IGF system and the inflammatory mediators in cultured synoviocytes. Biochem Biophys Res Commun 508(1):17–24. https://doi.org/10.1016/j.bbrc.2018.11.099
Cillero-Pastor B, Martin MA, Arenas J, Lopez-Armada MJ, Blanco FJ (2011) Effect of nitric oxide on mitochondrial activity of human synovial cells. BMC Musculoskelet Disord 12:42. https://doi.org/10.1186/1471-2474-12-42
Loeser RF, Collins JA, Diekman BO (2016) Ageing and the pathogenesis of osteoarthritis. Nat Rev Rheumatol 12(7):412–420. https://doi.org/10.1038/nrrheum.2016.65
Chang MC, Hung SC, Chen WY, Chen TL, Lee CF, Lee HC, Wang KL, Chiou CC, Wei YH (2005) Accumulation of mitochondrial DNA with 4977-bp deletion in knee cartilage--an association with idiopathic osteoarthritis. Osteoarthr Cartil 13(11):1004–1011. https://doi.org/10.1016/j.joca.2005.06.011
Zhao Z, Li Y, Wang M, Jin Y, Liao W, Zhao Z, Fang J (2020) Mitochondrial DNA haplogroups participate in osteoarthritis: current evidence based on a meta-analysis. Clin Rheumatol 39:1027–1037. https://doi.org/10.1007/s10067-019-04890-x
Hsu HC, Chang WM, Wu JY, Huang CC, Lu FJ, Chuang YW, Chang PJ, Chen KH, Hong CZ, Yeh RH, Liu TZ, Chen CH (2016) Folate deficiency triggered apoptosis of synoviocytes: role of overproduction of reactive oxygen species generated via NADPH oxidase/mitochondrial complex II and calcium perturbation. PLoS One 11(1):e0146440. https://doi.org/10.1371/journal.pone.0146440
Veale DJ, Fearon U (2018) The pathogenesis of psoriatic arthritis. Lancet 391(10136):2273–2284. https://doi.org/10.1016/S0140-6736(18)30830-4
Dalbeth N, Pool B, Smith T, Callon KE, Lobo M, Taylor WJ, Jones PB, Cornish J, McQueen FM (2010) Circulating mediators of bone remodeling in psoriatic arthritis: implications for disordered osteoclastogenesis and bone erosion. Arthritis Res Ther 12(4):R164. https://doi.org/10.1186/ar3123
Chimenti MS, Sunzini F, Fiorucci L, Botti E, Fonti GL, Conigliaro P, Triggianese P, Costa L, Caso F, Giunta A, Esposito M, Bianchi L, Santucci R, Perricone R (2018) Potential role of cytochrome c and tryptase in psoriasis and psoriatic arthritis pathogenesis: focus on resistance to apoptosis and oxidative stress. Front Immunol 9:2363. https://doi.org/10.3389/fimmu.2018.02363
Firuzi O, Spadaro A, Spadaro C, Riccieri V, Petrucci R, Marrosu G, Saso L (2008) Protein oxidation markers in the serum and synovial fluid of psoriatic arthritis patients. J Clin Lab Anal 22(3):210–215. https://doi.org/10.1002/jcla.20243
Kumagai T, Matsukawa N, Kaneko Y, Kusumi Y, Mitsumata M, Uchida K (2004) A lipid peroxidation-derived inflammatory mediator: identification of 4-hydroxy-2-nonenal as a potential inducer of cyclooxygenase-2 in macrophages. J Biol Chem 279(46):48389–48396. https://doi.org/10.1074/jbc.M409935200
Coto-Segura P, Santos-Juanes J, Gomez J, Alvarez V, Diaz M, Alonso B, Corao AI, Coto E (2012) Common European mitochondrial haplogroups in the risk for psoriasis and psoriatic arthritis. Genet Test Mol Biomarkers 16(6):621–623. https://doi.org/10.1089/gtmb.2011.0266
Funding
This study was supported by Science and Technology Innovation Program in Hunan province (2018SK2077).
Author information
Authors and Affiliations
Contributions
Muzhe Li generated the idea. Muzhe Li and Xuling Luo prepared the original draft. Zhiwei Chen critically revised the paper. Xin Long supervised the project. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Disclosures
None.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Li, M., Luo, X., Long, X. et al. Potential role of mitochondria in synoviocytes. Clin Rheumatol 40, 447–457 (2021). https://doi.org/10.1007/s10067-020-05263-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10067-020-05263-5