
Abstract
Objectives
Nowadays, all-ceramic materials are routinely used within the treatment of patients in dentistry. The objective of this prospective clinical trial was the evaluation of chair-side generated monolithic lithium disilicate crowns after 10 years.
Materials and methods
Forty-one posterior full contour crowns made of lithium disilicate ceramics were inserted with a self-adhesive resin cement in 34 patients (20 university/14 private practice) using a chair-side CAD/CAM technique. One crown per patient was randomly selected for evaluation according to the modified US Public Health Service criteria.
Results
After a mean examination time of 10.1 years, 26 crowns were available for re-examination. Within the observation period, five failures occurred due to one crown fracture after 2.9 years, an abutment fracture after 6.0 years, one severe endodontic problem after 6.1 years, a root fracture after 7.0 years, and a replacement of one crown caused by a carious lesion after 10 years. Complications occurred as retention loss of one crown, two carious lesions, and a change in sensibility perception of two abutment teeth. All events were associated with molars. The Kaplan-Meier analysis revealed a survival rate of 83.5% and a complication-free rate of 71.0% after 10 years.
Conclusion
Due to the small amount of technical complications and failures, the clinical performance of monolithic lithium disilicate crowns was completely satisfying.
Clinical relevance
The insertion of chair-side fabricated monolithic lithium disilicate crowns can be recommended for long-term use in the posterior region.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Teeth act as a human feature of beauty. It is suggested that spacing and tooth coloration exert an influence on the attractiveness of both sexes’ faces [1].The majority of the American population seems to be aware of that actuality, considering the fact that 60% of the American dentists see more than 100 patients per year for cosmetic dentistry procedures [2].
Since the introduction of full-ceramic materials, the patient’s desire for esthetics has become much easier to realize. As an alternative material, veneered metal-ceramics can be used, as they show close to perfect survival rates between 95.9–97.1% after 10 years [3, 4]. However, the veneering technique carries the risk of undesirable chipping (annual chipping rate 0.53%). For porcelain-infused zirconia, the annual complication rate (0.64%) is even higher than that for metal-ceramics [5]. Such a complication affects the occlusal and approximal stability of the restauration and causes an unwelcomed esthetic disadvantage for the patients.
That is why dentists have to meet the challenge of choosing an esthetic but most of all long-term stable restorative material.The monolithic applicationof full-ceramic materials might be a possibility to avoid the complication of chipping.
As a consequence, the question occurs if monolithic fabricated restorations can be recommended for long-term use.
Generally, it is reported that the application of full-ceramic crowns in the posterior area has a higher risk of failure than in the anterior area [6,7,8,9,10].
Only two publications have investigated the long-term behavior of monolithic ceramics. One of these studies examined the 12-year survival rate of monolithic feldspathic crowns within a range from 75.0 to 94.7% for the premolar region and up to 95.0% for the molar region, both rates depending on the preparation design [11]. The other investigation examined monolithic lithium disilicate (press technique) fixed dental prostheses with a 10-year survival of 87.9% [12].
Furthermore, the survival of lithium disilicate crowns as a core material was analyzed, considering an 8- to 10-year survival rate of 86.1–95.5% [13,14,15,16,17]. Regarding both, veneered and monolithic leucite-reinforced glass-ceramic posterior crowns, a publication described an 11-year survival rate of 84.4% [18].
The monitoring of veneered alumina single crowns revealed competitive values to silica-based ceramics with a rate of 83.9% after 10 years [19]. In contrast, glass-infiltrated alumina crowns yielded a failure-free rate of 68.3% after 15 years in the posterior area [9].
Based on the development of the computer-aided design/computer-aided manufacturing (CAD/CAM), it has become possible to prepare, design, and restore a tooth within one appointment. Therefore, the lithium disilicate material is highly qualified as it can be milled in a metasilicate status. Within this bluish shade status, it has a reduced flexural strength of 120 MPa×m0.5, facilitating asimple and fast milling process in the dental practice. Throughout the crystallization process in the furnace, a high flexural strength up to 360 ± 60 MPa×m0.5is obtained [20]. Based on these mechanical facilities, lithium disilicate ceramics can be cemented adhesively and even conventionally [21]. Especially for a subgingival preparation design and the required cementation method, this is an important aspect for the choice of material. Thus, it is no surprise that lithium disilicate crowns are the preferred choice for single crowns by dentists [2, 22].
To date, no long-term investigations on monolithic, chair-side fabricated single crowns made of lithium disilicate are available. Even the clinical quality of these crowns after 10 years has not been reported before.
The aim of this study is to evaluate the clinical performance of chair-side generated monolithic lithium disilicate crowns after 10 years. The working hypothesis is that these crowns are competitive to single crowns made of other materials or with different fabrication methods in the posterior area regarding the complication- and failure-free rates.
Material and methods
Between 2006 and 2007, 34 patients (mean age 46.5 years ± 13.1 years; 26.2–73.8 years; 62% female) with a need for single crown restorations were consecutively recruited.Within the study group, seven patients received two crowns. Considering scientific recommendations, only one crown per patient was selected randomly for further report and statistical evaluation (n = 34) [23]. Out of the 34 crowns, 26 crowns were inserted on molars and eight crowns on premolars, whereas 17 abutment teeth had been successfully endodontically treated.
According to the study protocol, patients were excluded due to xerostomia, temporomandibular disorders, or pregnancy. The abutment tooth needed to be vital or had to have a successful root canal treatment at least 6 months before restoration.The tooth to be treated and the adjacent teeth required healthy periodontal conditions (pocket depths ≤ 3.5 mm, no signs of inflammation).The requirements of the Helsinki Declaration were observed, and the patients gave their signed informed consent. The study was approved by the ethics committee of the University of Leipzig (no. 103-2006).
Chair-side, the crowns were fabricated in a private dental practice (14 crowns) as well as in the Department of Prosthodontics and Materials Science of the University of Leipzig (20crowns). All crowns were milled out of lithium disilicate (IPS e.max CAD LT, Ivoclar Vivadent, Schaan, Liechtenstein). The study protocol required a preparation design as following: a shoulder or a distinct chamfer of 1.0 mm width as finish line; a minimum ceramic thickness in the cusp area and at the fissure line of at least 2.0 mm and 1.5 mm, respectively. Afterwards, the optical impressions were taken with an infrared camera, and the crowns were fabricated using the Articulation mode (Cerec 3, Software version 2.9, Sirona, Salzburg, Austria). After milling (Cerec 3 milling unit, Sirona), the metasilicate status was used to clinically evaluate and correct the bluish crown in proximal, internal, and occlusal fit. Subsequently, the restorations were stained and glazed (IPS e.max CAD Crystall/Glaze Paste, IvoclarVivadent) followed by the crystallization and stain/glaze firing in one step (Programat CS, IvoclarVivadent). Before the adhesive cementation, the intaglio surface of the crowns was etched with hydrofluoric acid (IPS Empress etch, IvoclarVivadent) for 20 seconds, and a silane coupling agent was applied for 60 seconds (Monobond S, IvoclarVivadent). The tooth surface was cleaned mechanically with pumice and hand instruments. The restorations were inserted with the dual cure self-adhesive resin cement (Multilink Sprint, IvoclarVivadent). More detailed information is available in the 4- and 6-year publications [24, 25].
Within this prospective clinical trial, the crowns were examined at baseline, after 6 months, 1 to 6 years, and 10 years. The primary outcome variables were the failure-free rate and the complication-free rate. Subdividing all events into biological and technical, the biological complications were carious lesion below the crown margin, abutment fracture, and endodontic interventions. The technical complications comprised crown fracture, loss of retention, and chipping of the ceramic. Failures were defined as events leading to the replacement of the crown or the extraction of the abutment tooth. To evaluate the clinical quality of the single crowns, the modified US Public Health Service (USPHS) criteria were used [24]. Two independent dentists not involved in the treatment procedure examined the study crowns after10 years. In case of discrepancies of the ratings, the differences were subsequently discussed and an agreement was found.
Statistics including the Kaplan-Meier analysis, log-rank test, and Wilcoxon-rank test were examined (IBM SPSS Statistics 24, IBM, Ehningen, Germany). The level of significance was set to p < 0.05.
Results
After 10.1 years (SD ± 0.2 years), 26 out of 34 crowns were available for re-examination. The mean patients’age was 55.4 years (SD ± 11.2 years; 73% female). Three patients were lost during the 10-year recall program: two patients had died and one patient had moved. Five crowns could not be examined during the 10-year recall, since they had shown severe failures within the observation period.
Clinical quality (modified USPHS criteria)
According to the modified USPHS criteria, the parameters surface, color, adhesive gap, tooth and crown integrity, endodontic complication, complaints, and compliance were examined. The results for baseline, 5-year, and 10-year recall are available in Table 1.
Except for two crowns showing a change of sensibility perception within the first 2 years, all crowns scored either Alpha or Bravo after 10 years. Regarding the criterion “surface,” statistically significant differences were found for the increase of Alpha 2 scores between baseline and 10-year recall (p = 0.012, Wilcoxon signed-rank test).Moreover, the criterion “adhesive gap” was evaluated with an increased Alpha 2 score (p = 0.005, Wilcoxon signed-rank test).
Biological complications
Seven biological complications were detected. One tooth did not react on the sensitivity test at baseline. The patient was observed until the 10-year recall. A dental x-ray after 10 years showed no apical radiolucency. The sensitivity was still uncertain, but the patient had no complaints. The tooth was included as endodontic complication in the survival statistics. Another abutment tooth received endodontic treatment after 1.1 years, whereby the crown could be removed without any damage and reinserted after a successful root canal treatment.
After 48 months, one patient had a carious lesion below the crown margin. It was removed and a composite filling was applied.
There were two severe biological complications after 6 years: one tooth needed to be extracted because of an apical infection, and another tooth had an abutment fracture caused by a carious lesion. That is why this crown could not be reinserted again.
At the time of the 7-year recall, the mesial root of a lower molar showed a longitudinal fracture and needed to be extracted (Fig. 1). All of these three events were counted as failure.

One abutment tooth (FDI 46) showed a longitudinal root fracture after 7 years
During the recall period, one patient had already shown different carious lesions near the crown margin (24, 36, 48, 60 months) that was captured as complication after 24 months. Shortly before the 10-year re-examination, this study crown needed to be replaced due to a newly occurring carious lesion. This event was counted as failure only, since a complication had already been registered after 24 months.
Technical complications
Two technical complications were identified. One molar crown showed a loss of retention after 2 years. The abutment had no carious lesion and the restoration could be recemented. After the removal of residual cement, the crown was etched for 20 seconds with hydrofluoric acid, and after silane application, it was inserted with a self-adhesive resin cement (RelyX Unicem, 3 M, Seefeld, Germany). This was regarded as a complication.
After 2.8 years, a fracture of a lithium disilicate crown occurred to another molar. This was regarded as a failure.
Kaplan-Meier analysis
The failure-free rate after 10 years was 83.5% with a 95% confidence interval (CI) ranging between 70.2 and 96.8%. The complication-free rate after 10 years was 71.0% [95% CI 54.9–87.1%] considering all biological and technical events.The Kaplan-Meier analysis for the failure-free and the complication-free rate is represented in Fig. 2.

Kaplan-Meier analysis of the failure-free and complication-free rates of monolithic lithium disilicate crowns after an observation period of 10 years (n = 26). One crown had shown a carious lesion near the crown margin and was counted as complication after 24 months. Shortly before the 10-year recall, this crown needed to be replaced and was registered as failure only, since it had already been included as complication before
All of the complications (n = 9) occurred at molar abutment teeth (p = 0.005, log-rank test). For more detail, see Table 2.
Without randomization (n 10years = 33), the Kaplan-Meier analysis revealed a failure-free rate of 86.6% [95% CI 75.6–97.6%] after 10 years. The complication-free rate was 76.3% [95% CI 62.8–89.8%].
Discussion
According to the authors’ knowledge, for the first time, this study presents long-term results for longevity and clinical quality of chair-side generated monolithic lithium disilicate crowns after 10 years. The 10-year survival rate for the restorations in this study was examined with 83.5% and the complication-free rate was analyzed with 71.0%.
The five occurring failures were mostly caused by biological events (n = 4). One of these abutment teeth had a root fracture stabilized by the lithium disilicate crown (Fig. 1). The solitary technical complication occurred to one study crown after 2.9 years. Subsequently, their fragments were evaluated using a scanning electron microscope analysis. Revealing an occlusal thickness of 871 μm, this study’s preparation protocol and the recently recommended minimal thickness of 1.0 mm [26] were not realized for the fractured study crown.
In respect to hard tooth structure loss, the latest recommendation for 1.0 mm minimal thickness of adhesively cemented lithium disilicate crowns expresses an advantage over metal-ceramic crowns. Nonetheless, metal-ceramic crowns are a durable alternative to all-ceramic materials providing excellent survival rates of 95.9–97.1% after 10 years [3, 4]. Anyhow, this material combination has esthetical shortcomings and carries the risk of chipping.
The results of this recent investigation revealed a competitive longevity outcome of monolithic lithium disilicate crowns compared to values between 75.0 and 95.0% for monolithic glass ceramic crowns after 12 years [11]. Concerning veneered silica ceramics presenting 8- to 10-year survival rates of 86.1–95.5% and veneered oxide-ceramics demonstrating a 10-year failure-free rate of 83.9%, a similar rate was found within this study [13,14,15,16,17, 19]. Nonetheless, it should be taken into account that most of the all-ceramic investigations did not focus on crowns in the posterior region only. Presumably, this is the major reason for their slightly better survival rates [6,7,8,9, 13]. Additionally, as it was found in this study and in a clinical investigation examining monolithic lithium disilicate crowns with feather-edge preparation design [10], there might be a difference in the success of restorations inserted on premolars in contrast to molars, too.
In terms of the complication chipping, monolithic lithium disilicate materials are an esthetic and stable alternative, showing no chipping after 10 years.
The comparison of the modified USPHS criteria in the recent study showed mostly excellent to good ratings. The criterion “surface” increasingly scored Alpha 2 ratings after 10 years. This might be due to the wear of the lithium disilicate material [27, 28].
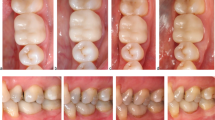
The color of the crowns was evaluated with Alpha scores only indicating a stable color behavior of monolithic lithium disilicate (Fig. 3). Competitive ratings were detected for other all-ceramic materials [11, 14, 18].

Clinical picture of one posterior lithium disilicate crown (FDI 36) at baseline (left), at 5-year recall (middle), and at 10-year recall (right)
Furthermore, the adhesive gap showed discoloration in the 10-year examination. In previous studies, this tendency was investigated for self-adhesive resin cements [29,30,31] causally, pointing out factors like wear of the luting material as well as patient-related parameters such as diet, smoking habits, and oral hygiene. Nonetheless, in general, the authors characterized an acceptable marginal integrity [30, 31]. This is emphasized by the good evaluations for “adhesive gap” within our study.
The limitations of this study are the lack of a comparison group and a limited sample size. Strengths of this investigation are unique long-term data, the prospective character, and the two fold examination at each recall including a subsequent agreement in case of differences. This procedure ensures the best reliability of the results.
Conclusion
Within the limitations of this prospective clinical study, monolithic lithium disilicate crowns (e.max CAD LT, IvoclarVivadent) presented a 10-year survival rate of 83.5%. This is similar to the survival of other all-ceramic restorations. In comparison to metal-ceramic crowns, the use of monolithic lithium disilicate crowns in the posterior area reveals slightly decreased results for longevity, but provides better esthetics as well as no risk of chipping. The chair-side CAD/CAM technique enables the fabrication of stable crowns even in the private practice.
References
Hendrie CA, Brewer G (2012) Evidence to suggest that teeth act as human ornament displays signalling mate quality. PLoS One 7:e42178. https://doi.org/10.1371/journal.pone.0042178
American Academy of Cosmetic Dentistry (2015) Cosmeticdentistry: state of the industry. Survey 2015. http://www.aacd.com/proxy/files/Publications%20and%20Resources/AACD%20State%20of%20the%20Cosmetic%20Dentistry%20Industry%202015.pdf. Accessed 18 August 2017
Walton TR (2013) The up to 25-year survival and clinical performance of 2,340 high gold-based metal-ceramic single crowns. Int J Prosthodont 26:151–160. https://doi.org/10.11607/ijp.3136
Behr M, Zeman F, Baitinger T et al (2014) The clinical performance of porcelain-fused-to-metal precious alloy single crowns: chipping, recurrent caries, periodontitis, and loss of retention. Int J Prosthodont 27:153–160. https://doi.org/10.11607/ijp.3440
Sailer I, Makarov NA, Thoma DS et al (2015) All-ceramic or metal-ceramic tooth-supported fixed dental prostheses (FDPs)? A systematic review of the survival and complication rates. Part I: Single crowns (SCs). Dent Mater 31:603–623. https://doi.org/10.1016/j.dental.2015.02.011
Heintze SD, Rousson V (2010) Fracture rates of IPS Empress all-ceramic crowns—a systematic review. Int J Prosthodont 23:129–133
Kassardjian V, Varma S, Andiappan M et al (2016) A systematic review and meta analysis of the longevity of anterior and posterior all-ceramic crowns. J Dent 55:1–6. https://doi.org/10.1016/j.jdent.2016.08.009
Pjetursson BE, Sailer I, Zwahlen M et al (2007) A systematic review of the survival and complication rates of all-ceramic and metal-ceramic reconstructions after an observation period of at least 3 years. Part I: Single crowns. Clin Oral Implants Res 18(Suppl 3):73–85. https://doi.org/10.1111/j.1600-0501.2007.01467.x
Rinke S, Tsigaras A, Huels A et al (2011) An 18-year retrospective evaluation of glass-infiltrated alumina crowns. Quintessence Int 42:625–633
Schmitz JH, Cortellini D, Granata S et al (2017) Monolithic lithium disilicate complete single crowns with feather-edge preparation design in the posterior region: a multicentric retrospective study up to 12 years. Quintessence Int 20:601–608. https://doi.org/10.3290/j.qi.a38678
Otto T, Mörmann WH (2015) Clinical performance of chairside CAD/CAM feldspathic ceramic posterior shoulder crowns and endocrowns up to 12 years. Int J Comput Dent 18:147–161
Kern M, Sasse M, Wolfart S (2012) Ten-year outcome of three-unit fixed dental prostheses made from monolithic lithium disilicate ceramic. J Am Dent Assoc 143:234–240
Valenti M, Valenti A (2009) Retrospective survival analysis of 261 lithium disilicate crowns in a private general practice. Quintessence Int 40:573–579
Toman M, Toksavul S (2015) Clinical evaluation of 121 lithium disilicate all-ceramic crowns up to 9 years. Quintessence Int 46:189–197. https://doi.org/10.3290/j.qi.a33267
Teichmann M, Gockler F, Weber V et al (2017) Ten-year survival and complication rates of lithium-disilicate (Empress 2) tooth-supported crowns, implant-supported crowns, and fixed dental prostheses. J Dent 56:65–77. https://doi.org/10.1016/j.jdent.2016.10.017
Gehrt M, Wolfart S, Rafai N et al (2013) Clinical results of lithium-disilicate crowns after up to 9 years of service. Clin Oral Investig 17:275–284. https://doi.org/10.1007/s00784-012-0700-x
Simeone P, Gracis S (2015) Eleven-year retrospective survival study of 275 veneered lithium disilicate single crowns. Int J Periodontics Restor Dent 35:685–694. https://doi.org/10.11607/prd.2150
Fradeani M, Redemagni M (2002) An 11-year clinical evaluation of leucite-reinforced glass-ceramic crowns: a retrospective study. Quintessence Int 33:503–510
Galindo ML, Sendi P, Marinello CP (2011) Estimating long-term survival of densely sintered alumina crowns: a cohort study over 10 years. J Prosthet Dent 106:23–28. https://doi.org/10.1016/S0022-3913(11)60089-9
Wiedhahn K (2007) From blue to white: new high-strength material for Cerec-IPS e.max CAD LT. Int J Comput Dent 10:79–91
KernM, ThompsonVP, BeuerF et al (2017) All-ceramics at a glance: an introduction to the indications, material selection, preparation and insertion techniques for all-ceramic restorations, 3rd English edition. AG Keramik, Ettlingen
Makhija SK, Lawson NC, Gilbert GH et al (2016) Dentist material selection for single-unit crowns: findings from the National Dental Practice-Based Research Network. J Dent 55:40–47. https://doi.org/10.1016/j.jdent.2016.09.010
Hickel R, Roulet J-F, Bayne S et al (2007) Recommendations for conducting controlled clinical studies of dental restorative materials. Clin Oral Invest 11:5–33. https://doi.org/10.1007/s00784-006-0095-7
Reich S, Schierz O (2013) Chair-side generated posterior lithium disilicate crowns after 4 years. Clin Oral Investig 17:1765–1772. https://doi.org/10.1007/s00784-012-0868-0
Rauch A, Reich S, Schierz O (2017) Chair-side generated posterior monolithic lithium disilicate crowns: clinical survival after 6 years. Clin Oral Investig 21:2083–2089. https://doi.org/10.1007/s00784-016-1998-6
Ivoclar VivadentAG IPS e.max CAD for PrograMill. http://www.ivoclarvivadent.de/de-de/zahnarzt/material/ips-emax-cad-for-programill. Accessed 18 Aug 2017
Zhang Z, Yi Y, Wang X et al (2017) A comparative study of progressive wear of four dental monolithic, veneered glass-ceramics. J Mech Behav Biomed Mater 74:111–117. https://doi.org/10.1016/j.jmbbm.2017.05.035
Lawson NC, Bansal R, Burgess JO (2016) Wear, strength, modulus and hardness of CAD/CAM restorative materials. Dent Mater 32:e275–e283. https://doi.org/10.1016/j.dental.2016.08.222
Belli R, Pelka M, Petschelt A et al (2009) In vitro wear gap formation of self-adhesive resin cements: a CLSM evaluation. J Dent 37:984–993. https://doi.org/10.1016/j.jdent.2009.08.006
Peumans M, Voet M, de MJ et al (2013) Four-year clinical evaluation of a self-adhesive luting agent for ceramic inlays. Clin Oral Investig 17:739–750. https://doi.org/10.1007/s00784-012-0762-9
Federlin M, Hiller K-A, Schmalz G (2014) Effect of selective enamel etching on clinical performance of CAD/CAM partial ceramic crowns luted with a self-adhesive resin cement. Clin Oral Investig 18:1975–1984. https://doi.org/10.1007/s00784-013-1173-2
Funding
This study was supported by Ivoclar Vivadent, Schaan, Principality of Liechtenstein.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors AR and LD declare no conflict of interest. The author SR has held oral presentations receiving a separate and appropriate honorarium. SR and OS held courses that were supported with material by Ivoclar Vivadent.
Ethical approval
The study was approved by the ethics committee of the University of Leipzig (no. 103-2006).
Informed consent
The requirements of Helsinki Declaration were observed, and the patients gave their signed informed consent.
Rights and permissions
About this article

Cite this article
Rauch, A., Reich, S., Dalchau, L. et al. Clinical survival of chair-side generated monolithic lithium disilicate crowns:10-year results. Clin Oral Invest 22, 1763–1769 (2018). https://doi.org/10.1007/s00784-017-2271-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-017-2271-3