
Abstract
Objectives
The objective of this prospective clinical study was to evaluate the performance of chair-side generated crowns after 48 months.
Materials and methods
Forty-one posterior full contour crowns made of a machinable lithium disilicate ceramic (e.max CAD LT) were inserted in 34 patients applying a chair-side CAD/CAM technique. One crown per patient was randomly selected for evaluation at baseline, after 6, 12, 24, 36, and 48 months according to modified US Public Health Service criteria.
Results
After a mean observation time of 51 months (min, 48 months; max, 56 months; SD ± 2.3 months), 29 crowns were available for re-examination. Within the observation period, one failure occurred due to a crown fracture after 2.8 years. Four abutment teeth revealed signs of biological complications: Two abutment changed sensibility perception from positive to negative within the first 13 month. Two abutment teeth showed secondary caries below the crown margin, one after the 24, and another after the 48 month recall. Both abutments received cervical adhesive composite fillings. The failure-free rate was 96.3 % after 4 years according to Kaplan–Meier (CI: upper bound, 4.4 years; lower bound, 4.7 years).
Conclusions
Due to the fact that the secondary caries was not caused as a result of an inaccuracy of the crown margins and the endodontic complications were in a normal range, the clinical performance of the crowns was completely satisfying.
Clinical relevance
The chair-side application of lithium disilicate crowns can be recommended.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
According to the literature, lithium disilicate ceramics offer reliable material properties for crown restorations. Originally, the material was brought on market as IPS Empress 2 (Ivoclar-Vivadent, Schaan, Liechtenstein) and was processed as a laboratory press-material. In their review article, Della Bona and Kelly [1] point out that the survival rates of IPS Empress 2 crowns was between 95 and 100 % within an observation period of 5 years. One of the studies cited is the prospective study published by Marquardt and Strub [2], who reported a survival rate of 100 % observing 27 IPS Empress 2 posterior crowns. Whereas the former lithium disilicate ceramic (IPS Empress 2) modifications only could be used as framework materials due to limited esthetics, the material IPS e.max (LT = low translucency) (Ivoclar-Vivadent, Schaan, Liechtenstein) is also indicated for full contour crowns. In a randomized controlled clinical trial, Etman et al. described the clinical performance of 30 crowns each made from three different crown materials (IPS e.max Press, Procera All ceram and metal ceramic) in 48 patients. After 3 years, they found no statistically significant difference between these laboratory-based systems [3] with respect to the survival rates. The all-ceramic systems revealed 96.6 % and the metal-ceramic system 100 %. IPS e.max is now provided as press material (IPS e.max Press) and as computer-aided design/computer-aided manufacturing (CAD/CAM) material (IPS e.max CAD). The introduction of the latter material enabled the chair-side application. The main objective of the chair-side concept using CAD/CAM techniques is the single visit appointment for providing a tooth colored restoration [4]. The advantage is the immediate definitive protection of the tooth without any provisional phase. The machinable lithium disilicate ceramic slightly differs from the pressable lithium disilicate ceramic due to material properties and the fabrication process. For the pressable ceramic e.max Press, a flexural strength of 400 ± 40 MPa and a fracture toughness from 2.5 to 3.0 MPa × m0.5 is reported [5], whereas the CAD/CAM material e.max CAD exhibits a flexural strength of 360 MPa (±60 MPa) and a fracture toughness between 2.0 and 2.5 MPa × m0.5 [6]. The latter material is provided in a machinable metasilicate state of bluish color, showing a fracture strength of 130 MPa (±30 MPa) and a fracture toughness of 0.9–1.1 MPa × m0.5. A try-in procedure of the bluish metasilicate restoration with respect to fit, proximal and occlusal contacts is allowed by the manufacturer’s recommendations. The final material properties and a tooth colored shade are obtained by a crystallization firing at 840 °C, which takes approximately 25 min [6]. From the practical point of view, this ceramic seemed to show some major advantages in comparison to common silicate ceramics on the one hand and zirconia oxide ceramics on the other hand, especially for chair-side indication: Due to its material properties, the lithium disilicate material was a reliable alternative for single crown indication. The chance to accomplish the try-in procedure in the blue meta-silicate status, where the material can easily be ground, enhances the clinical chair-side procedure. Due to its application as a full contour crown material with sufficient esthetics, an additional veneering could become needless. A firing time of about 30 min was acceptable for a single visit appointment in a well-organized practice. Therefore, the aim of this prospective clinical trial was to evaluate this lithium disilicate ceramic for chair side application. Thus, the working hypothesis stated was that the failure-free rate and the complication-free rate (primary outcomes) of chair-side fabricated single crowns were comparable to other all ceramic materials and fabricating systems suitable for single crowns. Secondary outcome variables also comprised esthetics and patient acceptance.
Material and methods
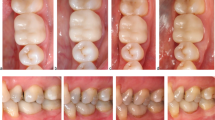
The patients, who took part in the study, had to show the indication for a posterior crown, and they had to give their written consent. Beside the crown indication, the following inclusion criteria had to be fulfilled according to the study protocol: healthy adult patients, if the abutment teeth were not vital a successful root canal treatment had to be accomplished at least 6 months before definitive restoration, healthy periodontal conditions (pocket depths ≤3.5 mm, any other signs of inflammation) of the tooth to be treated and the adjacent teeth, good oral hygiene (if PSI code was >3 additional oral hygiene treatment and education before inclusion), no comprehensive treatment needs of the dentition, the patient should have been presumable able to attend the post-operative examinations. Pregnant patients, patients with CMD and persons with xerostomia were excluded from the study. The study was approved by the ethic committee of the University of Leipzig (application number 103-2006). Thirty-four patients with a mean age at insertion of 46.5 years (min, 26.2 years; max, 73.8 years, SD ± 13.1 years) were provided with 41 lithium disilicate crowns. Seven patients received two crowns. Due to the fact that, in clinical studies, the assessment of restorations should be limited to one single unit of the same material per patient [7], for those patients who received two crowns, one crown was selected by random for further clinical observation. An Excel (MS excel 2010) random generator was used for this procedure. The topographic distribution of the abutments is shown in Fig. 1. Thirteen patients were male, and 21 were female. Twenty-seven crowns were inserted on molars and seven crowns on bicuspids. Seventeen teeth (50 %) were successfully endodontically treated before crown insertion. Five of these teeth received an adhesive built-up, 11 were restored with fiber posts and adhesive cores before preparation, and one maintained its metal post and core. According to the clinical investigators’ protocol, all crowns had to be fabricated chair-side. Fourteen of them were done in a private practice (SF); the others were provided in the department of Prosthodontics and Material Science of the University of Leipzig by three operators (SR = 10, HT = 7, and BS = 3). As finish line, a shoulder preparation or a distinct chamfer of 1.0 mm width had to be applied. A minimum ceramic thickness in the cusp area and at the fissure line of at least 2.0 and 1.5 mm had to be accomplished, respectively. If the preparation margin was located iso- or subgingival retraction cords were inserted, so that the finish line was clearly visible. The Cerec devices used in the dental clinic and in private practice were Cerec 3 units, which were equipped with a camera that emitted infrared light with a wave length of approximately 820 nm. All operators were calibrated before taking part in the study. They had to successfully complete a Cerec course that was held by an International Certified Cerec Trainer of the International Society of Computerized Dentistry, who also took part in the study as an operator (S. R.). In this course, a standardized procedure was taught. All crowns had to be fabricated in the so-called Articulation mode-Software version 2.9. The Articulation mode comprised three different digital 3D models:
-
1.
The virtual 3D model of the preparation. Three single optical impressions were done from the occlusal direction capturing the distal adjacent tooth, the abutment tooth in the direction of the insertion axis of the crown (so called master acquisition), and of the mesial adjacent tooth. An overlap of at least 40 % of the single exposures guaranteed the stitching of the single exposures and, thus, the calculation of the entire 3D model. If it was necessary to get additional information of the proximal areas of the adjacent teeth, a maximum of two more tilted photographs were done. The latter acquisitions were carefully checked because a too steep angulation in relation to the occlusal acquisitions could lead to artifacts when the single acquisitions were stitched together to the 3D model. If this was the case, the tilted pictures were erased and repeated in a lower angulation.
-
2.
In order to get information about the antagonists of the prepared tooth, a silicone material (Metal Bite, R-dental, Hamburg, Germany) was put on the abutment tooth without overlapping the adjacent teeth, and the patient was asked to close in maximum intercuspation. Immediately after the setting of the silicone, the mesial and distal adjacent teeth and the static bite registration between them were captured with the camera. Thus, a “static bite 3D model” was obtained. Due to the fact that the adjacent teeth in the preparation and the static bite model were identical, the software was enabled to superimpose the static bite virtually on the prepared tooth, so that the antagonist in its maximum intercuspation could be considered when designing the crown on the computer screen.
-
3.
The articulation mode additionally allowed to capture a third 3D model, which provided information of the dynamic motion of the antagonists: The silicone material was used to generate a functional bite registration (functionally guided pathway). Again three single optical impressions were done like described for the static bite registration in order to get a 3D model of the functionally guided pathway.

The number and the FDI localisation of the 34 observed lithium disilicate crowns are displayed
Finally the three models, the preparation model, the static bite registration model, and the dynamic bite registration model were virtually superimposed. Then, on the computer screen, the crowns were designed. The preparation margin was drawn by the use of the semiautomatically margin finder. If the preparation margin was on a similar level as the inserted retraction cord or the gingiva, the grayscale mode was switched on so that it was easier to determine the margin. After the virtual proposal of the crown, the design tools of the software were used to improve the shape of the crown, if necessary. Beside the proximal contacts, the occlusal contact points were designed as well. For molar crowns and bicuspids a minimum number of three and two centric stops were tried to achieve, respectively. The virtual contacts were displayed on the crown in a color code. Green color described contacts that penetrated the static bite from 0 to 50 μm, yellow color depicted premature contacts from 50 to 100 μm, and red areas indicated contacts that exceeded 100 μm. Mainly, the “form minus” or “form plus” design tools for coarse reductions or additions were used. The aim was to achieve slight green contacts. Due to the fact that the dynamic bite registration was available, too, the traces of the antagonist teeth could be displayed, and it was possible to reduce the occlusal surface of the designed crown if the occlusal shape penetrated the dynamic bite registration. This could be done manually also using the “form minus” tool or by an automatically grinding tool. Finally, the occlusal contacts were checked again. The crowns were milled from a lithium disilicate block in its metasilicate blue status, applying Cerec 3 milling units. The inner surface was machined by a cylindrical diamond bur with a diameter of 1.6 mm with a spacer presetting of 60 μm. After checking the proximal, internal, and occlusal fit, the crowns were put into the furnace for crystallization, which was associated with a shrinkage of 0.2 % and a transition from a bluish to a tooth colored restoration. After a final try-in, the restorations were adhesively luted. The intaglio surface of the restorations was etched with hydrofluoric acid (IPS Empress etch, Vivadent-Ivoclar) for 20 s, and after carefully rinsing and drying, a silane coupling agent was applied for 60 s (Monobond S, Vivadent-Ivoclar) and dried with oil-free air. The tooth surface was carefully cleaned mechanically with hand-instruments and with pumice. Core built-ups were not treated additionally, e.g., by sandblasting. If necessary, a retraction cord was inserted in order to obtain a proper preparation margin. Rubberdam application was not necessary according to the manufacturer’s recommendation. The crowns were inserted with the dual cure self-adhesive resin cement Multilink Sprint (Ivocar-Vivadent). Base and catalyst were automatically mixed by a mixing tip. The inner contour of the crown was filled with Multilink Sprint. Especially at the crown margin, a continuous coating of the ceramic material with the luting material was assured. Then, the crown was inserted and fixed in its final position under finger pressure. Excess was immediately removed. Additionally, the luting material was polymerized from mesio-oral, mesio-buccal, disto-oral, disto-buccal, and occlusal directions for at least 40 s each. The light curing devices were checked so that the irradiance was at least 600 mW/cm2, and if different curing modes were available, the standard mode was chosen. After insertion, the static and dynamic occlusions were checked again.
The primary outcome variables were the failure-free rate and the complication-free rate. All events that were observed were subdivided into biological and technical complications. Biological ones were secondary caries, abutment fracture, and endodontic interventions. Technical complications comprised crown fracture, loss of retention, and chipping of the ceramic. Failures were events that led to the removal of the crown. Within the prospective clinical trial, the crowns were examined at baseline, after 6, 12, 24, 36, and 48 month by two independent examiners according to the modified US Public Health Service (USPHS) criteria (Table 1) [8]. The occlusal relationship of the crowns was additionally assessed by the application of a rating scale that fitted to the principle of the USPHS criteria (Table 2). The examiners were not involved in the treatment procedures before. Statistics including Kaplan–Meier analysis were done with SPSS for windows (version 15).
Results
Study group
At the 4-year recall (mean observation time, 51 months; min, 48 months; max, 56 months; SD ± 2.3 months), 29 patients with one crown each were available. The mean age was 51 years (minimum, 30.3 years; maximum, 77.9 years; SD ± 12.7 years). Four patients with one crown each were lost during the recall program at 4 years: one patient died, one patient moved so far away that she was not able to show up, and two patients were lost because they changed their contact address without informing the recall team. The single USPHS ratings with respect to the criteria surface, color, adhesive gap, tooth and crown integrity, proximal contact, endodontic complications, occlusion, complaints, and compliance from baseline to 4 years are displayed in Table 3. At baseline, one patient had severe complaints, and he simultaneously rated the criterion compliance with “C.” After grinding off a premature contact both ratings turned to excellent ratings.
Biological complications
One crowned tooth of one of those patients who were lost during the observation period did not react on the sensitivity test at baseline. This crown was included in the survival statistic as an endodontic complication. The patient was observed until the 24-month recall with no further complications. Another abutment tooth received endodontic treatment after 1.1 years. The operator removed the crown without damage and reinserted it. This crown was observed until the 4-year recall. At the 24- and at the 48-month recall, one abutment tooth each showed caries near the crown margin. The caries was removed, and an adhesive composite filling was applied below the crown margin.
Technical complications
One crown showed decementation after 2 years. The abutment was caries free, and after the removal of residual cement, the crown was etched for 20 s with hydrofluoric acid, and after silane application, it was recemented with RelyX Unicem (3 M Espe, Seefeld, Germany). Between the 24- and 36-month recall, at 2.8 years, one crown of a lower right second molar fractured. This patient was not examined any more, but the crown was counted as a failure event.
Kaplan–Meier analysis
Exclusively, the crown fracture led to the removal of one of the study crowns; thus, the failure-free rate was 96.3 % after a period of 4.6 years (Fig. 2). The complication-free rate comprising all events after 4 years was 83 %, whereas the rate dropped down to 71 % after 4.3 years (Fig. 2).

Kaplan–Meier analysis of the failure free and complication free rate of 29 crowns in 29 patients after an observation period of 4 years. The fracture after 2.8 year is included (crown 30)
Discussion
To the authors’ knowledge, the study presented is one of only few evaluations [9] that reports on lithium disilicate crowns that were exclusively fabricated applying the chair-side method.
As secondary variables, criteria like color appearance and functional design comprising static and dynamic occlusion, proximal contacts, and adequate morphology were of special interest because only virtual models were used. Although at the beginning of the study, only blocks in the basic shades Vita A1, A2, A3, and B1 were available, the color adaptation in comparison to the adjacent dentition was rated excellent or good (Table 3). If an individualization was necessary, it was mostly done in one step together with the crystallization process, what meant that the shading pastes had to be applied on the bluish crown, then, crystallization spray or paste was put on. At the 1-year recall, out of the 15 crowns that were assessed as good, 11 obtained the subrating slightly too light and five received a slightly too dark. Within the observation time, there was a shift from slightly too dark at the 1-year recall to slightly opaque at 4 years (N = 5). None of the 29 observed crowns was assessed as slightly too dark. The reason for that rating may be explained by the use of the LT (=low translucency) blocks and that the items “dark” and “opaque” sometimes are overlapping. Nine crowns were assessed as slightly too bright at 4 years. In conclusion, the color results for posterior teeth were satisfying. In order to consider the function in a particular way when designing the occlusal morphology of the crown on the computer screen, a dynamic and static registration of the opposing teeth were additionally applied (for details, please see “Materials and methods”). Despite of that technique, one crown exhibited a nonocclusion at the 6-month recall. From the 1-year recall up to the 3 years re-evaluation, all crowns showed ratings of excellent or good [Table 2 (definition) and Table 3 (ratings)] with regard to dynamic and static occlusion. These results show that the oral cavity is an unsteady biological system where some shortcomings could be compensated over time without further damage like obvious tooth movements or CMD. On the other hand, one crown shifted from good to sufficient at 4 years. Besides a harmonic morphology, adequate proximal contact is essential for a correct function. At the 4-year recall, one contact situation was too wide, and the patient described sometimes food retention without injury (rating insufficient = Charly). She also wanted to obtain her restoration and refused any treatment, although the rating would consequently recommend a prophylactic replacement. Two teeth exhibited a proximal contact each that was too weak (distance >100 μm, no trauma of the papilla). It has to be noticed that at the 1-year recall, all contact were rated excellent or good. The examination of the contact points is defined clearly by the use of a 50-μm thick matrix band: A strong contact when inserting the matrix band into the proximal area of two teeth means an excellent contact, a strong contact with a double layered matrix band is rated as good, and if a gap between the proximal areas is just visible, the rating sufficient has to be noted. Thus, the three ratings that were below good could be explained by tooth movements—perhaps if the stability of the respective quadrant was weakened by, e.g., extractions. This should be examined at the 5-year recall. In a further clinical study evaluating e.max Press lithium disilicate crowns, the rating with respect to anatomic form was 100 % alpha [3]. One explanation may be that the criteria defined in the present study were more detailed (modified USPHS [8]), and additional detailed assessment criteria for occlusion (Table 2) were applied. Another reason might be that, in the study conducted by Etman et al., the restorations were exclusively fabricated lab-side, and in the present study, all crowns were virtually designed. It also has to be stressed that the criteria occlusion, proximal contact, integrity crown, and surface, which all comprise aspects of morphology, all were rated excellent (alpha1), good (alpha 2), or sufficient (Bravo) at the 12-, 24-, and the 36-month recall.
Fasbinder et al. also provided chair-side lithium disilicate crowns in a clinical trial. Twenty-three were luted with a composite resin (Multilink Auto Mix, Vivadent Ivoclar, Schaan), and 39 were cemented with an experimental resin cement. Three of those crowns debonded during the observation period and were recemented. Most probably, the resin was the cement that was brought on market as Multilink Sprint (Ivoclar Vivadent) and used as well in the present study. Due to the fact that the debonded crowns were recemented without any damage, Fasbinder reported a 100 % survival rate after 2 years. In the present study, one crown debonded and was recemented as well. One reason for retention loss might be that the abutment height was little <3 mm.
Two secondary caries events within the 4 years were recognized. Sailer at el. [10] concluded that the increased secondary caries rate of restorations was caused by increased marginal inaccuracies. The marginal accuracy of 20 of the crowns that were inserted within the present study revealed a median and mean marginal accuracy of 100 and 81 μm, respectively [11]. These values may lead to the conclusion that it is possible to gain clinically satisfactorily fitting crowns, so that it is unlikely that marginal inaccuracies are responsible for the two secondary caries events in the present study.
In the study, root canal treated and vital teeth were included. At the beginning of the study, 17 of the crowned teeth were already endodontically treated, so that the number of teeth that showed positive sensitivity was relatively low. The inclusion of endodontically treated teeth had a practical reason. The indication of a crown can only be justified if the tooth is severely decayed—otherwise, an adhesive onlay (or even an inlay) restoration is indicated. Severely decayed teeth are often root canal treated. In order to get an appropriate number of single crowns within an acceptable time period, it was necessary to include these teeth as well. Although with respect to sensitivity only 50 % of the teeth were under risk, all other criteria could be examined.
Two endodontic complications cannot be seen as representative for a system immanent shortcoming. Above all, the preparation and pretreatment guidelines were similar to a common crown treatment comparable to metal-ceramic restorations. The two endodontic complications occurred up to the 2-year recall [12].
In comparison to all-ceramic and metal-ceramic single crown systems where a separate veneering is essential and fracture events of the layering material are reported in different frequencies [13], the surface of all full contour crowns observed after 4 years in the present study was assessed as excellent or good.
With regard to catastrophic events (failures), one fracture occurred in the present study. Fragments of the fractured crown could be saved, and the SEM evaluation revealed that the recommended thickness was not kept as shown in Fig. 3. In the study protocol, a minimum thickness of 1.5 mm was stipulated in the fissure line. This event showed that this recommendation was overlooked during clinical application and consequently led to a catastrophic failure. In the SEM picture, the luting material Multilink Sprint is clearly visible. This may lead to the conclusion that the bond to the ceramic was stronger than the adhesion to the abutment substrate. Later on, Multilink Sprint was withdrawn from the market. The reason provided by the manufacturer was its instability during storage. This composite material contained <5 % methacrylated phosphoric ester, obviously responsible for its promised self-adhesive properties. Benzoylperoxide (<1 %) was responsible as starter for the auto-polymerization. With respect to the debonded crown, unfortunately, it was not possible to examine whether the tooth–composite or the composite–crown interface was weaker. The abutment height of <3 mm showed that the retentive shape of the tooth was a decisive factor for crown retention.

SEM of the fractured crown. As the measurement shows the minimum thickness of the occlusal surface was approximately 870 μm and hence far below the recommended minimum thickness of 1.5 mm
Etman et al. [3] reported one crown failure within an observation period of 3 years due to fracture. The study comprised 30 full contoured lithium disilicate ceramic crowns (e.max Press). Concluding, the present study revealed that the results of the chair-side processed lithium disilicate crowns lead to clinically satisfying results that are comparable to conventional and lab-side fabricated crowns. Due to the lack of a control group, the results of the present study have to be compared to the findings of other studies. Pjertursson et al. [13] reported in their review article of an estimated 5-year survival rate of 96.4, 95.4, and 94.5 % for alumina oxide, reinforced glass-ceramic, and InCeram crowns, respectively. The authors emphasized that these data refer to anterior and posterior crowns and that the survival rates are lower, if solely posterior crowns are analyzed [13]. Metal-ceramic crowns showed a survival rate of 95.6 %. Within the limitation of a 4-year observation period, the present results may lead to the conclusion that chair-side fabricated posterior lithium disilicate crowns could be seen as an alternative to other crown systems.
References
Della Bona A, Kelly JR (2008) The clinical success of all-ceramic restorations. J Am Dent Assoc 139(Suppl):8S–13S
Marquardt P, Strub JR (2006) Survival rates of IPS empress 2 all-ceramic crowns and fixed partial dentures: results of a 5-year prospective clinical study. Quintessence Int 37(4):253–259
Etman MK, Woolford MJ (2010) Three-year clinical evaluation of two ceramic crown systems: a preliminary study. J Prosthet Dent 103(2):80–90. doi:10.1016/S0022-3913(10)60010-8
Giordano R (2006) Materials for chairside CAD/CAM-produced restorations. J Am Dent Assoc 137(Suppl):14S–21S
Holand W, Schweiger M, Frank M, Rheinberger V (2000) A comparison of the microstructure and properties of the IPS Empress 2 and the IPS Empress glass-ceramics. J Biomed Mater Res 53(4):297–303
Wiedhahn K (2007) From blue to white: new high-strength material for Cerec–IPS e.max CAD LT. Int J Comput Dent 10(1):79–91
Hickel R, Roulet JF, Bayne S, Heintze SD, Mjor IA, Peters M, Rousson V, Randall R, Schmalz G, Tyas M, Vanherle G (2007) Recommendations for conducting controlled clinical studies of dental restorative materials. Clin Oral Investig 11(1):5–33. doi:10.1007/s00784-006-0095-7
Kramer N, Ebert J, Petschelt A, Frankenberger R (2006) Ceramic inlays bonded with two adhesives after 4 years. Dent Mater 22(1):13–21
Fasbinder DJ, Dennison JB, Heys D, Neiva G (2010) A clinical evaluation of chairside lithium disilicate CAD/CAM crowns: a two-year report. J Am Dent Assoc 141(Suppl 2):10S–14S
Sailer I, Feher A, Filser F, Gauckler LJ, Luthy H, Hammerle CH (2007) Five-year clinical results of zirconia frameworks for posterior fixed partial dentures. Int J Prosthodont 20(4):383–388
Reich S, Uhlen S, Gozdowski S, Lohbauer U (2011) Measurement of cement thickness under lithium disilicate crowns using an impression material technique. Clin Oral Investig 15:521–526. doi:10.1007/s00784-010-0414-x
Reich S, Fischer S, Sobotta B, Klapper HU, Gozdowski S (2010) A preliminary study on the short-term efficacy of chairside computer-aided design/computer-assisted manufacturing-generated posterior lithium disilicate crowns. Int J Prosthodont 23(3):214–216
Pjetursson BE, Sailer I, Zwahlen M, Hammerle CH (2007) A systematic review of the survival and complication rates of all-ceramic and metal-ceramic reconstructions after an observation period of at least 3 years. Part I: single crowns. Clin Oral Implants Res 18(Suppl 3):73–85
Acknowledgments
The study was supported by Vivadent-Ivoclar.
Conflict of interest
The author SR has held oral presentations receiving a separate and appropriate honorarium, and he has held courses that were supported by Vivadent-Ivoclar with material.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Reich, S., Schierz, O. Chair-side generated posterior lithium disilicate crowns after 4 years. Clin Oral Invest 17, 1765–1772 (2013). https://doi.org/10.1007/s00784-012-0868-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-012-0868-0