
Abstract
Mild cognitive impairment (MCI) and chemosensory dysfunction are non-motor symptoms of Parkinson’s disease (PD), but their association is unclear. We explored if MCI and the involvement of single cognitive domains influence olfaction and taste in PD. The role of demographic, clinical and neuropsychiatric variables was tested. We recruited 50 PD patients without dementia, no other reasons for cognitive impairment, no condition that could influence evaluation of cognition, olfaction and taste. They underwent a full neuropsychological and chemosensory (i.e., olfaction and taste) test with the Sniffin’ Sticks Extended test (SSET), Whole Mouth test (WMT) and Taste Strips test (TST). Fifty age- and sex-matched healthy subjects served as controls. Olfactory function and sweet identification were worse in PD than controls. MCI negatively influenced odor identification. Factors associated with poor olfactory function were age, overall cognition, apathy, and visuospatial dysfunction. Sour identification was affected by MCI and executive dysfunction, and salty identification by executive dysfunction. MCI, age and executive dysfunction worsened TST score. Awareness of olfactory dysfunction was impaired in PD with MCI. Education positively influenced SSET and TST scores. Our data confirmed that olfaction is abnormal in PD, while taste was only slightly impaired. Olfaction was worse in PD patients with visuospatial dysfunction, while sour and salty identification was worse in those with MCI and executive dysfunction, suggesting different underlying anatomical abnormalities. Future studies should incorporate neuroimaging and cerebrospinal fluid data to confirm this hypothesis. SSET odor identification and TST sour identification could be explored as quick screening tests for PD-MCI.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Converging studies indicate that olfactory dysfunction has a prevalence of up to 90% in Parkinson’s disease (PD) and it may occur before motor symptoms (Doty et al. 1988, 2015; Haugen et al. 2016). Olfactory bulb is involved by synuclein pathology very early in PD (Braak and Del 2009; Jellinger 2015), and smell impairment has been proposed as a pre-clinical PD biomarker (Fullard et al. 2016). Taste dysfunction, even if not as severe as olfactory deficit, was reported to a variable extent in PD (Sienkiewicz-Jarosz et al. 2005, 2013; Lang et al. 2006; Shah et al. 2009; Deeb et al. 2010; Kim et al. 2011; Cecchini et al. 2014, 2015) and was found to be stable and persistent in a longitudinal study (Ricatti et al. 2017). Neurodegeneration in the frontal operculum or the orbitofrontal cortex, which are involved late in disease course (Braak and Del 2009), has been suggested as the anatomical substrate of taste deficit in PD (Shah et al. 2009; Deeb et al. 2010; Cecchini et al. 2014, 2015; Jellinger 2015).
Cognitive impairment can occur in early disease stages (Wills et al. 2016), and it may range from mild cognitive impairment (MCI) to dementia, with PD-related MCI (PD-MCI) representing a risk factor for PD-dementia (Federico et al. 2017). PD-MCI has represented a vague clinical condition (Jellinger 2013), since the publication of the Movement Disorder Society diagnostic criteria (Litvan et al. 2012). Neuropsychiatric symptoms, such as depression and apathy, may coexist with MCI in PD and stand among the most common non-motor PD features (Monastero et al. 2013; Herman et al. 2015; Weintraub et al. 2015). Olfaction was found to be impaired in Alzheimer’s disease (AD) and related MCI (Djordjevic et al. 2008; Ottaviano et al. 2016; Jung et al. 2019), but PD- and AD-related MCI are known to differ in terms of predominantly involved cognitive domain and underlying neuropathological changes (Besser et al. 2016).
Apart from a single study on Korean patients that reported PD-MCI to be more likely associated with severe olfactory dysfunction than PD with normal cognition (Park et al. 2018), the association between MCI and chemosensory impairment in PD is largely unexplored. In particular, open questions on this topic include (a) whether olfaction and taste are differentially affected by PD-MCI, (b) the role of single cognitive domain dysfunction, and (c) whether individual features of chemosensory function (i.e., threshold, discrimination, identification) are differentially involved in PD-MCI.
To offer new information on this topic, we recruited a group of PD patients, who underwent a thorough neuropsychological testing and a comprehensive subjective and objective chemosensory evaluation. Patients were stratified according to the presence of MCI and the involvement of single cognitive domains. The effect of demographic, clinical, and neuropsychiatric covariates on olfaction and taste was also explored. Patients with PD-dementia were excluded.
Materials and methods
Subjects
We evaluated 108 consecutive PD patients at the Department of Neuroscience, Verona University Hospital, Italy. Inclusion criteria were: (a) diagnosis of idiopathic PD; (b) no PD-associated dementia (Jellinger 2018); (c) no other reasons for cognitive impairment (e.g., delirium, cerebrovascular disease, head trauma, metabolic abnormalities, medication adverse effects); (d) no other PD-related conditions (e.g., severe motor impairment, psychosis, severe motor fluctuations or dyskinesia, excessive daytime sleepiness) that could have influenced assessment of cognition (Litvan et al. 2012; Federico et al. 2017), olfaction and taste; (e) no history of ear nose and throat disorders, middle ear surgery, head or face trauma, Bell’s palsy, systemic diseases or any other clinical condition that could have interfered with olfaction and taste evaluation (Cecchini et al. 2018).
After screening for inclusion criteria (Fig. 1), 50 patients (21 females, 29 males; age: 68.1 ± 10.5 years, interquartile range, IQR 57.8–77.3; education: 9.1 ± 3.8 years, IQR 5.0–13.0) were included in the study.

Flow diagram of the study and reasons for patients’ exclusion
PD motor symptoms were measured with the modified Hoehn-Yahr (H-Y) scale and the Movement Disorder Society unified Parkinson’s disease rating motor subscale (UPDRS-III). Total levodopa equivalent daily dose (LEDD, mg) was calculated according to conversion formulae (Tomlinson et al. 2010).
Fifty healthy subjects matched for sex (27 females, 23 males; n.s. vs. patients), age (67.5 ± 9.4 years, IQR 60.0–72.8; n.s.) and education (9.5 ± 4.5 years, IQR 4.5–13.8; n.s.) served as controls. Controls were screened for cognition with Montreal cognitive assessment (MoCA), and underwent a clinical history collection to rule out conditions that could have interfered with olfaction and taste evaluation (point e) of inclusion criteria for patients.
All procedures were in accordance with the guidelines of the local ethical committee. Participants gave written consent prior to inclusion in the study, which was conducted according to the 1964 Declaration of Helsinki and its later amendments.
Neuropsychological assessment
All patients were in a stable ON condition and underwent the mini mental state examination (MMSE), MoCA and a comprehensive 15-test neuropsychological battery that were performed by an expert neuropsychologist (AF) in a quiet room (Federico et al. 2015, 2017; Goldman et al. 2015). According to the Movement Disorder Society level II criteria for PD-MCI, the cognitive battery included at least two tests for each of the five cognitive domains (i.e., memory, attention, executive function, visuospatial function and language) and the diagnosis of PD-MCI required the abnormality of at least two tests (Litvan et al. 2012).
Memory was examined with the Rey’s auditory verbal learning immediate and recall tests (Carlesimo et al. 1996). Attention and working memory were assessed with the digit span forward (Mondini et al. 2011), attentional matrices parts I and II (Della Sala et al. 1992), and trail making test part A (Mondini et al. 2011).
Executive function was explored with the frontal assessment battery (Appollonio et al. 2005), phonemic fluency test (Mondini et al. 2011) and the Stroop task (Brugnolo et al. 2016). Visuospatial function was assessed with the Benton judgement of line orientation test (Benton et al. 1978), the intersecting pentagons derived from the MMSE (Federico et al. 2017) and the clock copying test (Goldman et al. 2015). Language was evaluated with the short form of the Boston naming test (Fastenau et al. 1998), object naming test and verb naming test (Capasso and Miceli 2001).
Depression was assessed with the Hamilton depression rating (HAM–D) scale. Apathy was evaluated with the apathy evaluation self-report (AES–S) scale (Marin et al. 1991).
Chemosensory evaluation
All subjects were asked to rate their olfaction and taste as better- than-normal, normal, or less-than-normal. Olfaction and taste were evaluated in a well-ventilated room with validated tests based on a forced-choice paradigm (Burghart, Wedel, Germany). Smell was assessed by the Sniffin’ Sticks Extended test (SSET) (Hummel et al. 2007). The SSET is composed of three subtests, namely odor threshold (T; i.e., detecting the lowest concentration), odor discrimination (D; i.e., separating a specific odor from others) and odor identification (I; i.e., naming a specific odor). The sum of the SSET scores (TDI score) defines the olfactory performance of subject as normosmia (TDI score ≥ 30.5), hyposmia (TDI < 30.5 and > 16), and functional anosmia (i.e., total loss or minimal residual smell perception; TDI ≤ 16) (Weintraub et al. 2015).
Taste was examined by the Whole Mouth test (WMT) and the Taste Strips test (TST) (Mueller et al. 2003; Hummel et al. 2007; Landis et al. 2009). The WMT is a rapid screening test for the four basic tastes and consists of four supra-threshold taste solutions (sweet, sour, salty, bitter) sprayed into the mouth. TST is a validated and detailed procedure for the evaluation of taste sensitivity using sixteen spoon-shaped filter strips impregnated with four concentrations of the four basic tastes. The TST strips are placed on the tongue and the subject is asked to identify the taste quality from a list of four descriptors (sweet, sour, salty, and bitter) in a forced choice paradigm. Before each strip administration, the mouth is rinsed with water. The sum of TST correct identifications defines the taste performance as normogeusia (TST score ≥ 9), hypogeusia (TST score < 9), and complete ageusia (i.e., no sensation to the highest concentrations of all the four solutions) (Landis et al. 2009).
Statistical analysis
The normality of distribution was analyzed with the skewness-kurtosis test. Continuous variables were explored with t test in case of normal distribution, and non-parametrical Mann–Whitney U test when the distribution was not normal. Pearson’s χ2 test with Yates’ correction was applied to dichotomous variables. Spearman’s rho coefficient was used to explore the correlation between olfaction and taste scores. Linear regression multivariate analysis (backward model) was used to explore the influence of the demographic (age, sex, education), clinical (PD duration, H-Y, UPDRS-III, LEDD), cognitive (MMSE, MoCA, MCI, cognitive domain involved) and neuropsychiatric (HAD, AES-S) covariates on SSET and TST measures. P < 0.05 (two-tailed) was taken as the significance threshold for all the tests. Bonferroni’s correction was applied when analysing SSET and TST scores according to the involvement of single cognitive domains.
Results
Neuropsychological findings
PD-MCI was present in 26 patients (PD-MCI + group, 52%; single-domain MCI: n = 13, multiple-domain MCI: n = 13), and absent in 24 of them (PD-MCI—group, 48%) (Federico et al. 2017). Among demographic and clinical characteristics, UPDRS-III, MMSE and MoCA were significantly worse in PD-MCI + than PD-MCI–, while the other variables did not differ between the two groups (Table 1). Among cognitive domains, memory and executive functions were significantly more involved in PD-MCI + than PD-MCI—(Table 1).
Olfaction
SSET scores were significantly worse in patients (D: 7.8 ± 2.1; I: 7.0 ± 3.3; TDI: 20.0 ± 6.4) than controls (D: 10.6 ± 2.6, p < 0.001; I: 12.2 ± 2.6, p < 0.001; TDI: 27.4 ± 5.8, p < 0.001) except for T (PD, 5.1 ± 3.4; controls: 4.5 ± 2.5; n.s.; Fig. 2a).

Box plot showing the Sniffin’ Sticks Extended test (SSET) scores. a Scores from healthy controls (CTRL, white boxes) and Parkinson’s disease patients (PD, light grey boxes) for odor threshold (T), odor discrimination (D), odor identification (I), and the sum of the SSET scores (TDI). b Scores from PD patients without mild cognitive impairment (MCI −, white boxes) and those with mild cognitive impairment (MCI +, light grey boxes) for T, D, I, and TDI. Panel C: scores from PD patients with no involvement of visuospatial function to neuropsychological testing (VS–, white boxes) and those with abnormal visuospatial function (VS +, light grey boxes) for T, D, I, and TDI. *Marks significant comparison (a, bp < 0.05; cp < 0.01 because Bonferroni’s correction was applied). Open circles show min/max outliers
Among the SSET subtest scores, I was significantly worse in PD-MCI + (6.2 ± 3.0) than PD-MCI − (8.0 ± 3.4; p = 0.046), while the other scores did not significantly differ between PD-MCI + (T: 5.0 ± 3.4; D: 7.5 ± 2.1; TDI: 18.8 ± 6.7) and PD-MCI − (T: 5.2 ± 3.4; D: 8.1 ± 2.1; TDI: 21.3 ± 6.1; n.s. for all comparisons; Fig. 2b). When analyzing SSET scores according to the involved cognitive domains, TDI was significantly worse in PD patients with abnormal (13.5 ± 5.2) than those with preserved visuospatial function (21.1 ± 5.6; p = 0.003; Fig. 2c), while the other SSET scores were not influenced by the involvement of the other cognitive domains.
Taste
Nearly all PD patients and controls correctly identified the four WMT spray solutions (PD: 98% controls: 96%; n.s.).
Among TST scores, sweet was significantly worse in patients (3.2 ± 0.8) than controls (3.6 ± 0.6; p = 0.007), while the other taste qualities and the TST global score did not differ between PD (sour: 2.0 ± 1.1; salty: 3.1 ± 0.9; bitter: 3.2 ± 0.9; TST: 11.6 ± 2.4) and controls (sour: 2.2 ± 1.0; salty: 3.3 ± 1.0; bitter: 3.1 ± 1.0; TST: 12.0 ± 2.2; n.s. for all comparisons; Fig. 3a).

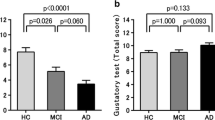
Box plot showing the Taste Strip test (TST) scores. a Scores from healthy controls (CTRL, white boxes) and Parkinson’s disease patients (PD, light grey boxes) for sweet, sour, salty, bitter and the sum TST scores (TST). b Scores from PD patients without mild cognitive impairment (MCI −, white boxes) and those with mild cognitive impairment (MCI +, light grey boxes) for sweet, sour, salty, bitter and TST. c Scores from PD patients with no involvement of executive function to neuropsychological testing (EX −, white boxes) and those with abnormal executive function (EX +, light grey boxes) for sweet, sour, salty, bitter and TST. *Marks significant comparison (a, bp < 0.05; cp < 0.01 because Bonferroni’s correction was applied). Open circles show min/max outliers
Sour and TST global score were significantly worse in PD-MCI + (sour: 1.6 ± 1.1; TST: 10.9 ± 2.3) than PD-MCI − (sour: 2.4 ± 0.9, p = 0.003; TST: 12.4 ± 2.3, p = 0.01), while the other taste qualities did not significantly differ between the two groups (PD-MCI +: sweet, 3.2 ± 0.8; salty, 2.9 ± 0.8; bitter, 3.2 ± 0.7; PD-MCI −: sweet, 3.3 ± 0.9; salty, 3.3 ± 0.9; bitter, 3.4 ± 0.9; n.s. for all comparisons; Fig. 3b).
Sour, salty and TST global scores were significantly worse in PD patients with abnormal (sour: 1.6 ± 1.1; salty: 2.8 ± 0.8; TST: 10.8 ± 2.7) than those with preserved executive function (sour: 2.4 ± 0.8, p = 0.008; salty: 3.4 ± 0.8, p = 0.008; TST: 12.6 ± 1.6, p = 0.005; Fig. 3c), while the other scores were not influenced by the involvement of the other cognitive domains.
Correlation between olfaction and taste total scores
Spearman’s rho correlation coefficient (Bonferroni’s corrected to account for the three comparisons) showed no significant correlation either in the whole PD group (rho = 0.03, n.s.) or according to the presence of MCI (PD-MCI −: rho = 0.34, n.s.; PD-MCI+: rho = 0.02, n.s.; Fig. 4).

Scatterplot showing the correlation between Sniffin’ Sticks Extended test (SSET) sum of the odor threshold, discrimination, and identification (TDI) score, and the Taste Strip test (TST) sum score in PD patients without mild cognitive impairment (MCI −, open circles; continuous trend line) and those with mild cognitive impairment (MCI +, closed circles; dashed trend line). No correlation was statistically significant (Spearman’s rho coefficient)
Concordance between self-rating assessment and measures of chemosensory function
Olfaction was reported as less-than-normal in 27 PD patients (54%; PD-MCI +: n = 14, PD-MCI −: n = 13; n.s.). Functional anosmia was found in 17 (34%; PD-MCI +: n = 10, PD-MCI −: n = 7; n.s.) and hyposmia in 29 PD patients (58% PD-MCI +: n = 14, PD-MCI −: n = 15; n.s.). PD-MCI − patients who reported olfaction as less-than-normal had worse TDI (20.0 ± 5.7) than those who reported normal/better-than-normal olfaction (24.0 ± 5.5; p = 0.042). In contrast, TDI did not significantly differ in PD-MCI + patients according to subjective complaints (less-than-normal olfaction: 18.5 ± 5.9; normal/better-than-normal olfaction: 19.3 ± 8.0; n.s.).
Taste was reported as less-than-normal in five PD patients (PD-MCI +: n = 3, PD-MCI −: n = 2; n.s.). Hypogeusia was found in two PD patients (PD-MCI +: n = 1, PD-MCI − group: n = 1; n.s.) and ageusia in one PD-MCI + patient. The small number of patients reporting abnormal taste hampered further analyses to compare subjective complaints to taste measures.
Multivariate analysis
Multivariate linear regression was applied to explore the influence of demographic and clinical covariates on olfaction and taste in patients. TDI score was positively influenced by education and negatively influenced by age, MMSE, AES-S, and visuospatial dysfunction (Table 2). TST score was positively influenced by education and negatively influenced by age, and executive dysfunction (Table 2).
Discussion
Our findings were that: (a) olfactory function and sweet identification were worse in PD than controls, (b) odor identification was worse in PD-MCI + than PD-MCI −, TDI score was worse in PD with visuospatial dysfunction, and age, MMSE and AES-S negatively influenced TDI score; (c) sour identification was worse in PD with MCI and executive dysfunction, salty identification was worse in PD with executive dysfunction, and age significantly worsened TST score; (d) olfaction and taste measures were not cross-correlated; (e) awareness of olfactory dysfunction was impaired in PD with MCI; (f) education positively influenced TDI and TST scores.
We confirmed olfaction to be largely abnormal in PD (Rahayel et al. 2012). We found all SSET measures, except odor threshold, to be worse in PD than controls. This finding is in accordance with previous reports of PD to be more impaired in odor identification and recognition than threshold, the former ones being considered more cognitively demanding than the latter (Hedner et al. 2010; Rahayel et al. 2012; Cecchini et al. 2016). However, this point is still a matter of debate, because threshold tests require temporal decisions among weak stimuli implying considerable cognitive involvement, and are generally less sensitive to chemosensory deficits. Moreover, threshold measures were found to be impacted in AD, PD, and multiple sclerosis (Mesholam et al. 1998; Doty et al. 2017; Good et al. 2017).
Among taste scores, only sweet identification was worse in PD than controls. This finding confirms taste to be slightly impaired in PD (Sienkiewicz-Jarosz et al. 2005, 2013; Lang et al. 2006; Shah et al. 2009; Deeb et al. 2010; Kim et al. 2011; Cecchini et al. 2014, 2015). Differences in PD populations, cognitive impairment and methods to assess taste across studies might have hampered the definition of a robust psychophysical marker of taste damage in PD. Genetic factors influencing taste should be considered (Risso et al. 2016). Indeed, previous studies showed an increase in phenylthiocarbamide (Moberg et al. 2007) and the bitter compound 6-n-propylthiouracil non-taster status (Cossu et al. 2018) in PD. In addition, our inclusion criteria ruled out other causes of chemosensory dysfunction and might have resulted in a very selected population.
We found PD-MCI + to be associated with worse odor identification. This finding is partially in keeping with a previous report, whereby all measures of a Korean SSET version were worse in PD with MCI than cognitively-intact PD (Weintraub et al. 2015). The different odor types in the two SSET versions might explain the discrepancies between the two studies. However, in the Korean study (Park et al. 2018), odor identification was the most severely affected measure, probably because this subtest is cognitively demanding, and thus is involved early in cognitively-affected PD (Djordjevic et al. 2008). Odor identification test was found to predict PD patients at risk of cognitive impairment (Damholdt et al. 2011), long-term cognitive decline in PD (Fullard et al. 2016; Domellöf et al. 2017), and the most impaired olfactory measure in AD-related MCI (Roalf et al. 2017), and in older-adult Down syndrome, which is associated with AD neuropathology (Cecchini et al. 2016). In keeping with a previous report of more rapid cognitive decline in early PD patients with hyposmia at diagnosis (Gjerde et al. 2018), our finding suggests odor identification could represent a quick screening test for PD-MCI, if confirmed in larger studies.
Patients with visuospatial dysfunction showed worse TDI score than those with preserved visuospatial domain, and MMSE and visuospatial dysfunction predicted worse TDI score in the multivariate analysis. These findings are in keeping with previous reports of olfactory dysfunction as predictor of early cognitive decline and post-operative delirium (Baba et al. 2012; Fullard et al. 2016; Kim et al. 2016; Domellöf et al. 2017), severe hyposmia and visuospatial impairment as risk factors for dementia in PD (Baba et al. 2012), and olfaction abnormalities as biomarker of cholinergic denervation (Bohnen et al. 2010; Bohnen and Müller 2013). Visuospatial dysfunction and hyposmia share parieto-temporal and limbic metabolic and electroencephalographic changes in PD (Baba et al. 2012; Iannilli et al. 2017; Wu et al. 2018). AD pathology, which preferentially involves limbic and posterior cortices, may coexist with Lewy bodies in PD and is associated with worse cognition (Irwin et al. 2013). AD cerebrospinal fluid (CSF) biomarkers may predict long-term cognitive decline in PD (Baba et al. 2012). Our data indicate a possible correlation between MCI, in particular visuospatial dysfunction, olfaction impairment and AD pathology, which may predict conversion to dementia, in PD. They suggest later cortical contribution to olfaction impairment that summates to early olfactory bulb degeneration (Park et al. 2018). However, only six PD patients had visuospatial dysfunction and future studies on larger populations should confirm these findings.
In keeping with three previous studies (Cramer et al. 2010; Hong et al. 2015; Masala et al. 2018), but in contrast with another one (Morley et al. 2011), we found apathy to worsen olfaction. Differences among patient populations and methods to assess olfaction may explain the discrepancy between studies. Smell is associated with emotional memory, and apathy may blunt responses to pleasant and unpleasant olfactory stimuli (Masala et al. 2018). Lower grey matter volume was found in the insula, limbic and temporal areas in PD with apathy (Alzaharani et al. 2016); these cortical areas show reduced metabolism in PD with hyposmia (Baba et al. 2012).
We found cognition to have a strong effect on taste performance, in that sour identification was worse in PD-MCI + than PD-MCI −; PD with executive dysfunction showed worse sour and salty identification, while MCI and executive dysfunction negatively influenced TST score in the multivariate analysis. Taste abnormalities have been ascribed to cortical involvement, because first and second-order gustatory neurons are spared in PD (Braak and Del 2009; Cecchini et al. 2014). Brain regions that were reported to differ between PD-MCI and cognitively-intact PD include insula and the prefrontal cortex (Mihaescu et al. 2018), which are also involved in taste perception (Cecchini et al. 2015). PD-MCI is characterized by prevalent executive dysfunction (Federico et al. 2017; Park et al. 2018) that is associated with prefrontal cortex abnormalities (de Bondt et al. 2016). These findings point to shared cortical substrates for MCI and taste abnormalities and are in keeping with a functional genomics report of olfactory and taste receptor alteration in the prefrontal cortex in PD (Garcia-Esparcia et al. 2013). Sour identification could be tested as a screening tool for PD-MCI in future studies.
Sweet identification, which was worse in PD vs. controls, was not influenced by cognition, probably because it plays a key role in energy intake and the reward systems (Ricatti et al. 2017).
In accordance with previous studies (Doty et al. 2017), age negatively influenced olfaction and taste. Age did not significantly differ across our groups (PD vs. controls, PD-MCI + vs. PD-MCI −) and thus did not represent a potential confounder.
In keeping with their separate anatomical pathways (Shah et al. 2009; Cecchini et al. 2015), olfaction and taste scores did not correlate to each other in our sample, suggesting the two chemosensory modalities should be examined separately.
Many PD patients were unaware of their olfactory deficits. These findings confirm previous reports (Deeb et al. 2010; White et al. 2016). The lower awareness in PD-MCI is in keeping with a previous study (Kawasaki et al. 2016). Olfaction should be always objectively explored with validated tests in PD, especially in PD-MCI.
In line with previous reports on normal subjects (Orhan et al. 2012), education positively influenced olfaction and taste performance. Chemosensory evaluation is a cognitively demanding task that can be influenced by education, context and experience (Kobayashi and Kennedy 2002). However, education did not differ across groups and did not represent a bias in this study.
The severity of motor symptoms was significantly different in the two PD groups, as the Movement Disorder Society UPDRS-III score was worse in PD-MCI + than PD-MCI −. However, this variable was not significant in the multivariate analysis, suggesting it did not influence chemosensory function.
Our control sample was composed of normal controls without cognitive impairment, thus a comparison between PD-MCI + and controls with MCI was not possible. In any case, such comparison would have been disputable, because PD-MCI is known to be clinically and pathologically distinct from AD-related MCI (Besser et al. 2016).
Limitations of our report include the small sample size, the absence of follow-up cognitive testing, neuroimaging data and CSF biomarkers. Moreover, for the sake of easiness, we used whole mouth taste testing, which is not sensitive to regional differences that have been documented in PD, whereby anterior tongue regions appear to be more sensitive than posterior ones (Sienkiewicz-Jarosz et al. 2005, 2013; Doty et al. 2015). Future multicentre studies should overcome these limitations. Another limitation is that TDI and TST are composite measures not independent from the sum of single olfaction and taste scores. However, TDI and TST are widely used in the clinical setting to define the severity of chemosensory dysfunction. Moreover, a previous study exploring factors contributing to olfactory dysfunction concluded that combined testing of several components of olfaction, especially including assessment of thresholds, provides the most significant approach to the diagnosis of smell loss (Lötsch et al. 2008).
In conclusion, we found MCI and the dysfunction of executive and visuospatial domains to be associated with worse olfaction and taste, suggesting shared pathology between cognitive and chemosensory dysfunction in PD. SSET odor identification and TST sour identification could be tested as quick screening tools for PD-MCI in larger multicentre studies.
References
Alzahrani H, Antonini A, Venneri A (2016) Apathy in mild Parkinson’s disease: neuropsychological and neuroimaging evidence. J Parkinsons Dis 6:821–832. https://doi.org/10.3233/JPD-160809
Appollonio I, Leone M, Isella V, Piamarta F, Consoli T, Villa ML, Forapani E, Russo A, Nichelli P (2005) The Frontal Assessment Battery (FAB): normative values in an Italian population sample. Neurol Sci 26:108–116. https://doi.org/10.1007/s10072-005-0443-4
Baba T, Kikuchi A, Hirayama K, Nishio Y, Hosokai Y, Kanno S, Hasegawa T, Sugeno N, Konno M, Suzuki K, Takahashi S, Fukuda H, Aoki M, Itoyama Y, Mori E, Takeda A (2012) Severe olfactory dysfunction is a prodromal symptom of dementia associated with Parkinson’s disease: a 3 year longitudinal study. Brain 135:161–169. https://doi.org/10.1093/brain/awr321
Benton AL, Varney NR, Hamsher KS (1978) Visuospatial judgment. A clinical test. Arch Neurol 35:364–367. https://doi.org/10.1001/archneur.1978.00500300038006
Besser LM, Litvan I, Monsell SE, Mock C, Weintraub S, Zhou XH, Kukull W (2016) Mild cognitive impairment in Parkinson’s disease versus Alzheimer’s disease. Parkinsonism Relat Disord 27:54–60. https://doi.org/10.1016/j.parkreldis.2016.04.007
Bohnen NI, Müller ML (2013) In vivo neurochemical imaging of olfactory dysfunction in Parkinson’s disease. J Neural Transm 120:571–576. https://doi.org/10.1007/s00702-012-0956-y
Bohnen NI, Müller ML, Kotagal V, Koeppe RA, Kilbourn MA, Albin RL, Frey KA (2010) Olfactory dysfunction, central cholinergic integrity and cognitive impairment in Parkinson’s disease. Brain 133:1747–1754. https://doi.org/10.1093/brain/awq079
Braak H, Del TK (2009) Neuroanatomy and pathology of sporadic Parkinson’s disease. Adv Anat Embryol Cell Biol 201:1–119
Brugnolo A, De Carli F, Accardo J, Amore M, Bosia LE, Bruzzaniti C, Cappa SF, Cocito L, Colazzo G, Ferrara M, Ghio L, Magi E, Mancardi GL, Nobili F, Pardini M, Rissotto R, Serrati C, Girtler N (2016) An updated Italian normative dataset for the Stroop color word test (SCWT). Neurol Sci 37:365–372. https://doi.org/10.1007/s10072-015-2428-2
Capasso R, Miceli G (2001) Esame Neuropsicologico per l’Afasia (E.N.P.A.). Springer, Milan
Carlesimo GA, Caltagirone G, Gainotti G, Fadda L, Gallassi R, Lorusso S, Marfia G, Marra C, Nocentini U, Parnetti L (1996) The mental deterioration battery: normative data, diagnostic reliability and qualitative analyses of cognitive impairment. Eur Neurol 36:378–384. https://doi.org/10.1159/000117297
Cecchini MP, Osculati F, Ottaviani S, Boschi F, Fasano A, Tinazzi M (2014) Taste performance in Parkinson’s disease. J Neural Transm (Vienna) 121:119–122. https://doi.org/10.1007/s00702-013-1089-7
Cecchini MP, Fasano A, Boschi F, Osculati F, Tinazzi M (2015) Taste in Parkinson’s disease. J Neurol 262:806–813. https://doi.org/10.1007/s00415-014-7518-1
Cecchini MP, Viviani D, Sandri M, Hähner A, Hummel T, Zancanaro C (2016) Olfaction in people with down syndrome: a comprehensive assessment across four decades of age. PLoS One 11:e0146486. https://doi.org/10.1371/journal.pone.0146486
Cecchini MP, Cardobi N, Sbarbati A, Monaco S, Tinazzi M, Tamburin S (2018) Post-traumatic taste disorders: a case series. J Neurol 265:836–844. https://doi.org/10.1007/s00415-018-8776-0
Cossu G, Melis M, Sarchioto M, Melis M, Melis M, Morelli M, Tomassini Barbarossa I (2018) 6-n-propylthiouracil taste disruption and TAS2R38 nontasting form in Parkinson’s disease. Mov Disord 33:1331–1339. https://doi.org/10.1002/mds.27391
Cramer CK, Friedman JH, Amick MM (2010) Olfaction and apathy in Parkinson’s disease. Parkinsonism Relat Disord 16:124–126. https://doi.org/10.1016/j.parkreldis.2009.09.004
Damholdt MF, Borghammer P, Larsen L, Ostergaard K (2011) Odor identification deficits identify Parkinson’s disease patients with poor cognitive performance. Mov Disord 26:2045–2050. https://doi.org/10.1002/mds.23782
de Bondt CC, Gerrits NJ, Veltman DJ, Berendse HW, van den Heuvel OA, van der Werf YD (2016) Reduced task-related functional connectivity during a set-shifting task in unmedicated early-stage Parkinson’s disease patients. BMC Neurosci 17:20. https://doi.org/10.1186/s12868-016-0254-y
Deeb J, Shah M, Muhammed N, Gunasekera R, Gannon K, Findley LJ, Hawkes CH (2010) A basic smell test is a sensitive as dopamine transporter scan: comparison of olfaction, taste and DaTSCAN in the diagnosis of Parkinson’s disease. QJM 103:941–952. https://doi.org/10.1093/qjmed/hcq142
Della Sala S, Laiacona M, Spinnler H, Ubezio C (1992) A cancellation test: its reliability in assessing attentional deficits in Alzheimer’s disease. Psychol Med 22:885–901. https://doi.org/10.1017/S0033291700038460
Djordjevic J, Jones-Gotman M, De Sousa K, Chertkow H (2008) Olfaction in patients with mild cognitive impairment and Alzheimer’s disease. Neurobiol Aging 29:693–706. https://doi.org/10.1016/j.neurobiolaging.2006.11.014
Domellöf ME, Lundin KF, Edström M, Forsgren L (2017) Olfactory dysfunction and dementia in newly diagnosed patients with Parkinson’s disease. Parkinsonism Relat Disord 38:41–47. https://doi.org/10.1016/j.parkreldis.2017.02.017
Doty RL, Deems DA, Stellar S (1988) Olfactory dysfunction in parkinsonism: a general deficit unrelated to neurologic signs, disease stage, or disease duration. Neurology 38:1237–1244
Doty RL, Nsoesie MT, Chung I, OsmanIan A, Pawasarat I, Caulfield J, Hurtig H, Silas J, Dubroff J, Duda JE, Ying GS, Tekeli H, Leon-Sarmiento FE (2015) Taste function in early stage treated and untreated Parkinson’s disease. J Neurol 262:547–557. https://doi.org/10.1007/s00415-014-7589-z
Doty RL, Chen JH, Overend J (2017) Taste quality confusions: influences of age, smoking, PTC taster status, and other subject characteristics. Perception 46:257–267. https://doi.org/10.1177/0301006616685577
Fastenau PS, Denburg NL, Mauer BA (1998) Parallel short forms for the Boston Naming test: psychometric properties and norms for older adults. J Clin Exp Neuropsychol 20:828–834
Federico A, Maier A, Vianello G, Mapelli D, Trentin M, Zanette G, Picelli A, Gandolfi M, Tamburin S (2015) Screening for mild cognitive impairment in Parkinson’s disease: comparison of the Italian versions of three neuropsychological tests. Parkinsons Dis 2015:681976. https://doi.org/10.1155/2015/681976
Federico A, Trentin M, Zanette G, Mapelli D, Picelli A, Smania N, Tinazzi M, Tamburin S (2017) Diagnosing mild cognitive impairment in Parkinson’s disease: which tests perform best in the Italian population?. Neurol Sci 38:1461–1468. https://doi.org/10.1007/s10072-017-3000-z
Fullard ME, Tran B, Xie SX, Toledo JB, Scordia C, Linder C, Purri R, Weintraub D, Duda JE, Chahine LM, Morley JF (2016) Olfactory impairment predicts cognitive decline in early Parkinson’s disease. Parkinsonism Relat Disord 25:45–51. https://doi.org/10.1016/j.parkreldis.2016.02.013
Garcia-Esparcia P, Schlüter A, Carmona M, Moreno J, Ansoleaga B, Torrejón-Escribano B, Gustincich S, Pujol A, Ferrer I (2013) Functional genomics reveals dysregulation of cortical olfactory receptors in Parkinson disease: novel putative chemoreceptors in the human brain. J Neuropathol Exp Neurol 72:524–539. https://doi.org/10.1097/NEN.0b013e318294fd76
Gjerde KV, Müller B, Skeie GO, Assmus J, Alves G, Tysnes OB (2018) Hyposmia in a simple smell test is associated with accelerated cognitive decline in early Parkinson’s disease. Acta Neurol Scand 138:508–514. https://doi.org/10.1111/ane.13003
Goldman JG, Holden S, Ouyang B, Bernard B, Goetz CG, Stebbins GT (2015) Diagnosing PD-MCI by MDS task force criteria: how many and which neuropsychological tests? Mov Disord 30:402–406. https://doi.org/10.1002/mds.26084
Good KP, Tourbier IA, Moberg P, Cuzzocreo JL, Geckle RJ, Yousem DM, Pham DL, Doty RL (2017) Unilateral olfactory sensitivity in multiple sclerosis. Physiol Behav 168:24–30. https://doi.org/10.1016/j.physbeh.2016.10.017
Haugen J, Müller MLTM, Kotagal V, Albin RL, Koeppe RA, Scott PJH, Frey KA, Bohnen NI (2016) Prevalence of impaired odor identification in Parkinson disease with imaging evidence of nigrostriatal denervation. J Neural Transm 123:421–424. https://doi.org/10.1007/s00702-016-1524-7
Hedner M, Larsson M, Arnold N, Zucco GM, Hummel T (2010) Cognitive factors in odor detection, odor discrimination, and odor identification tasks. J Clin Exp Neuropsychol 32:1062–1067. https://doi.org/10.1080/13803391003683070
Herman T, Weiss A, Brozgol M, Wilf-Yarkoni A, Giladi N, Hausdorff JM (2015) Cognitive function and other non-motor features in non-demented Parkinson’s disease motor subtypes. J Neural Transm 122:1115–1124. https://doi.org/10.1007/s00702-014-1349-1
Hong JY, Sunwoo MK, Ham JH, Lee JJ, Lee PH, Sohn YH (2015) Apathy and olfactory dysfunction in early Parkinson’s disease. J Mov Disord 8:21–25. https://doi.org/10.14802/jmd.14029
Hummel T, Kobal G, Gudziol H, Mackay – Sim A (2007) Normative data for the “Sniffin’ Sticks” including tests of odor identification, odor discrimination, and olfactory thresholds: an upgrade based on a group of more than 3000 subjects. Eur Arch Otorhinolaryngol 264:237–243. https://doi.org/10.1007/s00405-006-0173-0
Iannilli E, Stephan L, Hummel T, Reichmann H, Haehner A (2017) Olfactory impairment in Parkinson’s disease is a consequence of central nervous system decline. J Neurol 264:1236–1246. https://doi.org/10.1007/s00415-017-8521-0
Irwin DJ, Lee VM, Trojanowski JQ (2013) Parkinson’s disease dementia: convergence of alpha-synuclein, tau and amyloid-beta pathologies. Nat Rev Neurosci 14:626–636. https://doi.org/10.1038/nrn3549
Jellinger KA (2013) Mild cognitive impairment in Parkinson disease: heterogenous mechanisms. J Neural Transm 120:157–167. https://doi.org/10.1007/s00702-012-0771-5
Jellinger KA (2015) Neuropathobiology of non-motor symptoms in Parkinson disease. J Neural Transm 122:1429–1440. https://doi.org/10.1007/s00702-015-1405-5
Jellinger KA (2018) Dementia with Lewy bodies and Parkinson’s disease-dementia: current concepts and controversies. J Neural Transm 125:615–650. https://doi.org/10.1007/s00702-017-1821-9
Jung HJ, Shin IS, Lee JE (2019) Olfactory function in mild cognitive impairment and Alzheimer’s disease: a meta-analysis. Laryngoscope 129:362–369. https://doi.org/10.1002/lary.27399
Kawasaki I, Baba T, Takeda A, Mori E (2016) Loss of awareness of hyposmia is associated with mild cognitive impairment in Parkinson’s disease. Parkinsonism Relat Disord 22:74–79. https://doi.org/10.1016/j.parkreldis.2015.11.015
Kim HJ, Jeon BS, Lee JY, Cho YJ, Hong KS, Cho JY (2011) Taste function in patients with Parkinson’s disease. J Neurol 258:1076–1079. https://doi.org/10.1007/s00415-010-5884-x
Kim MS, Yoon JH, Kim HJ, Yong SW, Hong JM (2016) Olfactory dysfunction is related to postoperative delirium in Parkinson’s disease. J Neural Transm 123:589–594. https://doi.org/10.1007/s00702-016-1555-0
Kobayashi C, Kennedy LM (2002) Experience-induced changes in taste identification of monosodium glutamate. Physiol Behav 75:57–63. https://doi.org/10.1016/S0031-9384(01)00634-5
Landis BN, Welge-Luessen A, Brämerson A, Bende M, Mueller CA, Nordin S, Hummel T (2009) ‘‘Taste strips’’ a rapid, lateralized, gustatory bedside identification test based on impregnated filter papers. J Neurol 256:242–248. https://doi.org/10.1007/s00415-009-0088-y
Lang CJ, Leuschner T, Ulrich K, Stössel C, Heckmann JG, Hummel T (2006) Taste in dementing diseases and parkinsonism. J Neurol Sci 248:177–184
Litvan I, Goldman JG, Tröster AI, Schmand BA, Weintraub D, Petersen RC et al (2012) Diagnostic criteria for mild cognitive impairment in Parkinson’s disease: Movement Disorder Society task force guidelines. Mov Disord 27:349–356. https://doi.org/10.1002/mds.24893
Lötsch J, Reichmann H, Hummel T (2008) Different odor tests contribute differently to the evaluation of olfactory loss. Chem Sens 33:17–21
Marin RS, Biedrzycki RC, Firinciogullari S (1991) Reliability and validity of the Apathy Evaluation Scale. Psychiatry Res 38:143–162. https://doi.org/10.1016/0165-1781(91)90040-V
Masala C, Solla P, Liscia A, Defazio G, Saba L, Cannas A, Cavazzana A, Hummel T, Haehner A (2018) Correlation among olfactory function, motors’ symptoms, cognitive impairment, apathy, and fatigue in patients with Parkinson’s disease. J Neurol 265:1764–1771. https://doi.org/10.1007/s00415-018-8913-9
Mesholam RI, Moberg PJ, Mahr RN, Doty RL (1998) Olfaction in neurodegenerative disease: a meta-analysis of olfactory functioning in Alzheimer’s and Parkinson’s diseases. Arch Neurol 55:84–90
Mihaescu AS, Masellis M, Graff-Guerrero A, Kim J, Criaud M, Cho SS, Ghadery C, Valli M, Strafella AP (2018) Brain degeneration in Parkinson’s disease patients with cognitive decline: a coordinate-based meta-analysis. Brain Imaging Behav. https://doi.org/10.1007/s11682-018-9922-0
Moberg PJ, Balderston CC, Rick JH, Roalf DR, Weintraub D, Kleiner-Fisman G, Stern MB, Duda JE (2007) Phenylthiocarbamide (PTC) perception in Parkinson disease. Cogn Behav Neurol 20:145–148
Monastero R, Di Fiore P, Ventimiglia GD, Camarda R, Camarda C (2013) The neuropsychiatric profile of Parkinson’s disease subjects with and without mild cognitive impairment. J Neural Transm 120:607–611. https://doi.org/10.1007/s00702-013-0988-y
Mondini S, Mapelli D, Vestri A, Arcara G, Bisiacchi PS (2011) Esame neuropsicologico Breve 2, ENB-2. Raffaello Cortina Editore, Milan
Morley JF, Weintraub D, Mamikonyan E, Moberg PJ, Siderowf AD, Duda JE (2011) Olfactory dysfunction is associated with neuropsychiatric manifestations in Parkinson’s disease. Mov Disord 26:2051–2057. https://doi.org/10.1002/mds.23792
Mueller C, Kallert S, Renner B, Stiassny K, Temmel AF, Hummel T, Kobal G (2003) Quantitative assessment of gustatory function in a clinical context using impregnated ‘‘taste strips’’. Rhinology 41:2–6
Orhan KS, Karabulut B, Keleş N, Değer K (2012) Evaluation of factors concerning the olfaction using the Sniffin’ Sticks test. Otolaryngol Head Neck Surg 146:240–246. https://doi.org/10.1177/0194599811425019
Ottaviano G, Frasson G, Nardello E, Martini A (2016) Olfaction deterioration in cognitive disorders in the elderly. Aging Clin Exp Res 28:37–45. https://doi.org/10.1007/s40520-015-0380-x
Park JW, Kwon DY, Choi JH, Park MH, Yoon HK (2018) Olfactory dysfunctions in drug-naïve Parkinson’s disease with mild cognitive impairment. Parkinsonism Relat Disord 46:69–73. https://doi.org/10.1016/j.parkreldis.2017.11.334
Rahayel S, Frasnelli J, Joubert S (2012) The effect of Alzheimer’s disease and Parkinson’s disease on olfaction: a meta-analysis. Behav Brain Res 231:60–74. https://doi.org/10.1016/j.bbr.2012.02.047
Ricatti MJ, Ottaviani S, Boschi F, Fasano A, Tinazzi M, Cecchini MP (2017) A prospective evaluation of taste in Parkinson’s disease. J Neural Transm (Vienna) 124:347–352. https://doi.org/10.1007/s00702-016-1638-y
Risso DS, Mezzavilla M, Pagani L, Robino A, Morini G, Tofanelli S, Carrai M, Campa D, Barale R, Caradonna F, Gasparini P, Luiselli D, Wooding S, Drayna D (2016) Global diversity in the TAS2R38 bitter taste receptor: revisiting a classic evolutionary PROPosal. Sci Rep 6:25506. https://doi.org/10.1038/srep25506
Roalf DR, Moberg MJ, Turetsky BI, Brennan L, Kabadi S, Wolk DA, Moberg PJ (2017) A quantitative meta-analysis of olfactory dysfunction in mild cognitive impairment. J Neurol Neurosurg Psychiatry 88:226–232. https://doi.org/10.1136/jnnp-2016-314638
Shah M, Deeb J, Fernando M, Noyce A, Visentin E, Findley LJ, Hawkes CH (2009) Abnormality of taste and smell in Parkinson’s disease. Parkinsonism Relat Disord 15:232–237. https://doi.org/10.1016/j.parkreldis.2008.05.008
Sienkiewicz-Jarosz H, Scinska A, Kuran W, Ryglewicz D, Rogowski A, Wrobel E, Korkosz A, Kukwa A, Kostowski W, Bienkowski P (2005) Taste responses in patients with Parkinson’s disease. J Neurol Neurosurg Psychiatry 76:40–46. https://doi.org/10.1136/jnnp.2003.033373
Sienkiewicz-Jarosz H, Scinska A, Swiecicki L, Lipczynska-Lojkowska W, Kuran W, Ryglewicz D, Kolaczkowski M, Samochowiec J, Bienkowski P (2013) Sweet liking in patients with Parkinson’s disease. J Neurol Sci 329:17–22. https://doi.org/10.1016/j.jns.2013.03.005
Tomlinson CL, Stowe R, Patel S, Rick C, Gray R, Clarke CE (2010) Systematic review of levodopa dose equivalency reporting in Parkinson’s disease. Mov Disord 25:2649–2653. https://doi.org/10.1002/mds.23429
Weintraub D, Simuni T, Caspell-Garcia C, Coffey C, Lasch S, Siderowf A et al (2015) Cognitive performance and neuropsychiatric symptoms in early, untreated Parkinson’s disease. Mov Disord 30:919–927. https://doi.org/10.1002/mds.26170
White TL, Sadikot AF, Djordjevic J (2016) Metacognitive knowledge of olfactory dysfunction in Parkinson’s disease. Brain Cogn 104:1–6. https://doi.org/10.1016/j.bandc.2016.01.004
Wills AA, Elm JJ, Ye R, Chou KL, Parashos SA, Hauser RA, Bodis-Wollner I, Hinson VK, Christine CW, Schneider JS, The NINDS NET-PD Investigators (2016) Cognitive function in 1736 participants in NINDS exploratory trials in PD long-term study-1. Parkinsonism Relat Disord 33:127–133. https://doi.org/10.1016/j.parkreldis.2016.10.005
Wu L, Liu FT, Ge JJ, Zhao J, Tang YL, Yu WB, Yu H, Anderson T, Zuo CT, Chen L, Wang J (2018) Clinical characteristics of cognitive impairment in patients with Parkinson’s disease and its related pattern in 18 F-FDG PET imaging. Hum Brain Mapp. https://doi.org/10.1002/hbm.24311
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
MPC, AF and ST designed the study. MPC, AF, AZ, EM, CM, MT and ST collected the data. MPC, AF and ST analysed the data and made the statistical analysis. All Authors contributed to the interpretation of the data. MPC, AF and ST drafted the original version of the manuscript, which was revised critically by AZ, EM, CM and MT. All Authors approved the final version of the manuscript to be published.
Corresponding authors
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Cecchini, M.P., Federico, A., Zanini, A. et al. Olfaction and taste in Parkinson’s disease: the association with mild cognitive impairment and the single cognitive domain dysfunction. J Neural Transm 126, 585–595 (2019). https://doi.org/10.1007/s00702-019-01996-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00702-019-01996-z