
Abstract
Purpose
Few studies examine the clinical outcomes in patients undergoing minimally invasive transforaminal lumbar interbody fusion (MIS-TLIF) versus lateral lumbar interbody fusion (LLIF) for adjacent segment disease (ASD). We aim to compare the postoperative clinical trajectory through patient-reported outcome measures (PROMs) and minimum clinically important difference (MCID) in patients undergoing MIS-TLIF versus LLIF for ASD.
Methods
Patients were stratified into two cohorts based on surgical technique for ASD: MIS-TLIF versus LLIF. PROMs of 12-Item Short Form Physical Component Score (SF-12 PCS), visual analog scale (VAS) back, VAS leg, and Oswestry Disability Index (ODI) were collected at preoperative and postoperative 6-week/12-week/6-month/1-year time points. MCID attainment was calculated through comparison to established thresholds. Cohorts were compared through nonparametric inferential statistics.
Results
Fifty-four patients were identified, with 22 patients undergoing MIS-TLIF after propensity score matching. Patients undergoing MIS-TLIF for ASD demonstrated significant postoperative improvement up to 1-year VAS back, up to 1-year VAS leg, and 6-month through 1-year ODI (p ≤ 0.035, all). Patients undergoing LLIF demonstrated significant postoperative improvement in 6-month SF-12 PCS, 6-month through 1-year VAS back, 12-week through 6-month VAS leg, and 6-month to 1-year ODI (p ≤ 0.035, all). No significant differences were calculated between surgical techniques for PROMs or MCID achievement rates.
Conclusion
Patients undergoing either MIS-TLIF or LLIF for adjacent segment disease demonstrated significant postoperative improvement in pain and disability outcomes. Additionally, patients undergoing LLIF reported significant improvement in physical function. Both MIS-TLIF and LLIF are effective for the treatment of adjacent segment disease.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Spinal fusion introduces an immobile construct subject to greater bending moments and shear stresses at adjacent spinal segments, resulting in accelerated degeneration and symptoms of back and/or leg pain [5, 19, 1, 14]. Symptomatic manifestation of the degenerated adjacent segments, termed adjacent segment disease (ASD), may require decompression of the adjacent segment and extension of the fusion construct [1].
The minimally invasive transforaminal lumbar interbody fusion (MIS-TLIF) and lateral lumbar interbody fusion (LLIF) are two well-established surgical techniques utilized to treat adjacent segment disease [1, 22, 11, 9]. The MIS-TLIF involves a posterior approach for direct decompression of the neural elements, while LLIF involves a transpsoas approach for indirect decompression and direct access to the intervertebral disc [12]. Direct access to the disc space allows for larger interbody cage placement and, hence, greater correction of sagittal imbalance, coronal imbalance, and restoration of disc height [22, 11, 12].
Although there are studies examining direct versus indirect decompression in treating adjacent segment disease, these studies fail to directly compare the postoperative clinical outcomes in patients undergoing MIS-TLIF versus LLIF. Investigation into the clinical outcomes between surgical techniques for ASD may aid in surgical decision-making and management of postoperative expectations for patients. We aim to investigate this gap by querying patients undergoing MIS-TLIF or LLIF for adjacent segment disease in a single-surgeon database.
Methods
Patient population
Patient consent and Institutional Review Board approval (ORA #14051301) were acquired preceding the start of the current study. Patient records were queried from July 2009 to September 2022. Patients were included if they underwent MIS-TLIF or LLIF for adjacent segment disease. Patients were excluded if they were diagnosed with neoplasm, infection, or acute fracture. Patients were favored to undergo MIS-TLIF if they required direct decompression, had abnormal vascular anatomy, or had obstructive iliac crests. LLIF was favored if patients required greater correction of sagittal and/or coronal imbalance. All patients undergoing LLIF underwent additional posterior instrumentation.
Data collection
Patient demographics, perioperative characteristics, and inpatient complications were recorded. Age, gender, ethnicity, insurance type, body mass index (BMI), smoking status, hypertensive status, diabetic status, American Society of Anesthesiologists (ASA) classification, and Charlson Comorbidity Index (CCI) score were the demographic information collected. The number of contiguous fused levels, fusion level, operative time, estimated blood loss, length of stay, postoperative day (POD) 0 and 1 VAS pain, POD 0 and 1 narcotic consumption, and day of discharge were the perioperative characteristics recorded. Acute renal failure, altered mental status, postoperative anemia, arrhythmia, aspiration or reintubation, atelectasis, fever of unknown origin, ileus, urinary incontinence, nausea/vomiting, pleural effusion, pneumonia, pulmonary embolism, urinary retention, urinary tract infection, and venous thromboembolism were inpatient complications recorded.
The primary outcomes collected in this study were PROMs evaluating physical function, pain, and disability. The SF-12 PCS was utilized to evaluate physical function. The VAS back and VAS leg evaluated back and leg pain, respectively. The ODI was utilized to evaluate disability. These PROMs were collected at preoperative and postoperative 6-week, 12-week, 6-month, and 1-year time points.
Statistical analysis
Patients undergoing surgery for adjacent segment disease were stratified into two cohorts based on whether they underwent MIS-TLIF or LLIF. MCID achievement was determined through comparison of PROM improvement to established thresholds of 2.5 for SF-12 PCS, 2.1 for VAS back, 2.8 for VAS leg, and 14.9 for ODI [16, 15]. Categorical and continuous variables were compared between cohorts using the Fisher exact and Mann–Whitney U tests, respectively. After comparing the demographic characteristics between cohorts, propensity score-matched for age, BMI, smoking status, hypertensive status, and CCI scores. Postoperative improvement of PROMs was calculated using Wilcoxon ranked sign tests. All data were analyzed using Stata 17.0 (StataCorp LP, College Station, TX, USA). An alpha value of 0.05 was utilized to determine statistical significance.
Results
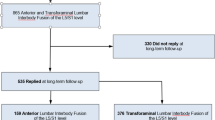
Prior to propensity score matching, a total of 69 patients were identified. There were 54 total patients, with 22 and 32 patients undergoing MIS-TLIF and LLIF, respectively, after matching for demographic characteristics. No significant differences between cohorts were calculated after propensity score matching. Demographic characteristics were skewed towards white (73.6%) patients. The proportion of patients receiving private insurance (44.4%) and workers’ compensation (44.4%) were equal. For self-identified gender, 37.0% were female. Patients typically had a moderate comorbidity burden, with 20.4%, 37.0%, and 16.7% with positive smoking, hypertensive, and diabetic statuses, respectively. The mean age, BMI, and CCI scores were 56.0 years, 32.0 kg/m2, and 2.2, respectively. Unmatched demographics are in Table 1, while matched demographics are in Table 2.
For perioperative characteristics, the fusion level and POD 0 narcotic consumption were significantly different between MIS-TLIF and LLIF cohorts (p ≤ 0.009, both). For fusion level, LLIF patients tended to undergo fusion at L3–L4 (37.5%), L2–L3 (28.1%), or L4–L5 (15.6%). MIS-TLIF patients tended to undergo fusion at L4–L5 (54.6%), L5–S1 (27.3%), or L3–L4 (18.2%). Most patients in either surgical technique underwent single-level fusion (90.7%). One patient underwent 3-level LLIF for degenerative scoliosis at L2–S1 and had a previous ALIF at L5–S1. For POD 0 narcotic consumption, MIS-TLIF patients utilized significantly greater narcotic consumption in OME of 116.7 compared to 59.8 in LLIF (p = 0.009). No other significant differences were noted in perioperative characteristics. The mean operative time, estimated blood loss, and length of stay were 170.4 min, 91.8 mL, and 46.9 h, respectively. Perioperative characteristics are in Table 3.
No significant differences were reported between cohorts for inpatient postoperative complications. Overall, most patients’ hospital courses were complicated by fever of unknown origin (20.4%), urinary retention (13.0%), or nausea/vomiting (7.4%). One patient undergoing MIS-TLIF suffered from altered mental status, while a separate patient undergoing MIS-TLIF suffered from atelectasis. Postoperative inpatient complications are in Table 4.
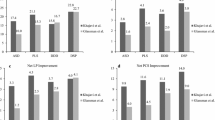
Patients undergoing MIS-TLIF reported significant postoperative improvement in 6-week to 1-year VAS back, 6-week to 1-year VAS leg, and 6-month to 1-year ODI (p ≤ 0.035, all). Patients undergoing LLIF reported significant postoperative improvement in 6-month SF-12 PCS, 6-week through 1-year VAS back, 12-week through 6-month VAS leg, and 6-month to 1-year ODI (p ≤ 0.035, all). No significant preoperative or postoperative differences in PROMs were calculated between cohorts. Greater than 50% of patients achieved MCID in MIS-TLIF for all domains. Greater than 50% of patients achieved MCID in LLIF for SF-12 PCS, VAS back, and VAS leg. No significant differences in MCID achievement were calculated between cohorts. Assessment of raw PROM scores is in Table 5, and MCID achievement rates are in Table 6.
Discussion
Independent of surgical technique, patients undergoing MIS-TLIF or LLIF for adjacent segment disease reported significant postoperative improvement in pain and physical function. Patients undergoing LLIF also demonstrated significant postoperative improvement in physical function. No significant differences were calculated between cohorts for postoperative PROM scores or MCID achievement rates. Either MIS-TLIF or LLIF are effective surgical interventions for adjacent segment disease.
Biomechanical finite element analysis (FEA) models have demonstrated considerably increased shear stress at the adjacent segments following a lumbar fusion [4, 8, 10]. One study calculated the shear stress at the upper adjacent segment to be as high as 43% in the fused segment model [4]. A separate article utilized FEA to determine significantly increased stress at the nucleus pulposus and annulus fibrosus after posterior lumbar interbody fusion (PLIF) and as disc degeneration progressed [8]. One additional study formed a FEA model with LLIF and bilateral pedicle screw placement for treatment of adjacent segment disease [10]. The authors calculated that placement of the interbody cage with bilateral pedicle screws in the adjacent segment provides sufficient structural stability and protective effects on the interbody cage placement compared to standalone cage placement [10]. Overall, these FEA studies demonstrate the increased stress applied to the adjacent segments due to an immobile construct and the efficacy in extending the immobile construct for adjacent segment disease.
In addition to these biomechanical studies, previous articles have examined the clinical and radiographic outcomes of utilizing direct and indirect decompression for adjacent segment disease. One study examining standalone LLIF versus laminectomy and posterior lateral fusion demonstrated that equivalent postoperative clinical outcomes in VAS back, VAS leg, and ODI scores, with significantly higher segmental lordosis (SL), lumbar lordosis (LL), and disc height in patients undergoing LLIF [11]. A separate article demonstrated that patients undergoing oblique lateral interbody fusion (OLIF) versus TLIF for adjacent segment disease had similar postoperative clinical outcomes in VAS back, VAS leg, and ODI, with the OLIF cohort experiencing greater improvement in sagittal balance [9]. A separate study examining postoperative clinical outcomes in OLIF versus PLIF reported clinical postoperative improvement in VAS, ODI, and Japanese Orthopedic Association (JOA) scores for the treatment of adjacent segment disease [21]. However, patients undergoing OLIF demonstrated superior VAS outcomes [21]. One case series demonstrated that patients undergoing LLIF for adjacent segment disease had significant improvements to disability and physical function outcomes, with improvements in SL, LL, and disc height [22]. Although none of these studies directly evaluated MIS-TLIF versus LLIF, these overall findings indicate that both indirect and decompression methods are effective in the treatment of adjacent segment disease in appropriately selected patients.
In this present study, patients undergoing MIS-TLIF for adjacent segment disease underwent surgical intervention at L4–5 and had higher POD 0 narcotic consumption compared to LLIF. Though the L4–5 intervertebral disc space is accessible through LLIF, the lumbar plexus courses more ventrally compared to the more cranial levels and may obscure up to 50% of the safety corridor [18, 13, 3]. Furthermore, abnormal vascular anatomy and high-riding iliac crests may preclude selection of LLIF at this level [7]. For postoperative pain management, patients undergoing MIS-TLIF required higher POD-0 narcotic consumption. One explanation may be due to the extensive retraction and dissection of the paraspinal muscles in TLIF [17, 20, 6]. As such, patients undergoing MIS-TLIF may require greater immediate postoperative pain management.
Patients undergoing either MIS-TLIF or LLIF for adjacent segment disease reported significant postoperative improvement for pain and disability outcomes in the current study. Patients demonstrated similar postoperative PROM scores and MCID achievement in pain and disability outcomes. Our results correspond to the majority of the previously cited literature [22, 11, 9, 21]. That is, patients undergoing direct versus indirect decompression demonstrated similar postoperative clinical outcomes in pain and disability outcomes [11, 9]. Overall, our findings suggest that either MIS-TLIF or LLIF are effective surgeries in treating adjacent segment disease.
For physical function, only patients undergoing LLIF reported significant postoperative improvement in physical function. Although patients undergoing MIS-TLIF did not report significant postoperative improvement in physical function, the mean SF-12 PCS score improved during the postoperative period. As such, the lack of significant improvement in the MIS-TLIF cohort may be the result of insufficient power. Still, the lack of significant differences between cohorts indicates the similar efficacy between MIS-TLIF and LLIF for adjacent segment disease.
This present study has several limitations. The lower patient numbers in each cohort may introduce insufficient power in our longitudinal analysis due to loss of follow-up. Furthermore, loss to follow-up introduces selection bias. One article studied this phenomenon and reported superior postoperative outcomes in patients who were initially lost to follow-up in clinic compared to patients who continued to follow in clinic [2]. Additionally, PROMs are inherently subjective and therefore are susceptible to response bias. As the most important aspect of patient selection was individual clinical evaluation, surgical technique was selected based on the anatomical characteristics highlighted in the Patient population. As such, the study design precludes the ability to entirely negate biases in patient selection. However, as the findings of this study indicate non-inferiority of either surgical technique in appropriately indicated patients, such biases may not have negatively influenced these results. Usage of a single-surgeon database limits the generalizability of these findings, as our cohort was typically White males. Despite this demographic predominance, the patients in our study typically reported a higher comorbidity burden. Future investigations may incorporate a multicenter analysis to aid in greater patient collection and generalizability.
Conclusion
Patients undergoing either MIS-TLIF or LLIF for adjacent segment disease demonstrated significant postoperative improvement in pain and disability outcomes. Patients undergoing LLIF additionally demonstrated postoperative improvement in physical function. Patients undergoing either MIS-TLIF or LLIF demonstrated equivalent postoperative improvement and MCID achievement rates in physical function, pain, and disability outcomes. MIS-TLIF and LLIF are similarly effective in treating adjacent segment disease.
Abbreviations
- ASA:
-
American Society of Anesthesiologists
- ASD:
-
Adjacent segment disease
- BMI:
-
Body mass index
- CCI:
-
Charlson comorbidity index
- EBL:
-
Estimated blood loss
- FEA:
-
Finite element analysis
- HNP:
-
Herniated nucleus pulposus
- JOA:
-
Japanese Orthopedic Association
- LLIF:
-
Lateral lumbar interbody fusion
- LL:
-
Lumbar lordosis
- LOS:
-
Length of stay
- MCID:
-
Minimum clinically important difference
- MIS-TLIF:
-
Minimally invasive transforaminal lumbar interbody fusion
- ODI:
-
Oswestry disability index
- OLIF:
-
Oblique lateral interbody fusion
- OME:
-
Oral morphine equivalents
- ORA:
-
Office of Regulatory Affairs
- PLIF:
-
Posterior lumbar interbody fusion
- POD:
-
Postoperative day
- PROMs:
-
Patient-reported outcome measures
- SF-12 PCS:
-
12-Item Short Form Physical Component Score
- SL:
-
Segmental lordosis
- VAS:
-
Visual analog scale
References
Chang SY, Chae IS, Mok S, Park SC, Chang BS, Kim H (2021) Can indirect decompression reduce adjacent segment degeneration and the associated reoperation rate after lumbar interbody fusion? A systemic review and meta-analysis. World Neurosurg 153:e435–e445
Chen DA, Vaishnav AS, Louie PK et al (2020) Patient reported outcomes in patients who stop following up: Are they doing better or worse than the patients that come back? Spine (Phila Pa 1976) 45(20):1435–1442
Davis TT, Bae HW, Mok JM, Rasouli A, Delamarter RB (2011) Lumbar plexus anatomy within the psoas muscle: implications for the transpsoas lateral approach to the L4-L5 disc. J Bone Joint Surg Am 93(16):1482–1487
Ebrahimkhani M, Arjmand N, Shirazi-Adl A (2021) Biomechanical effects of lumbar fusion surgery on adjacent segments using musculoskeletal models of the intact, degenerated and fused spine. Sci Rep 11(1):17892
Hilibrand AS, Robbins M (2004) Adjacent segment degeneration and adjacent segment disease: the consequences of spinal fusion? Spine J 4(6 Suppl):190S–194S
Hockley A, Ge D, Vasquez-Montes D et al (2019) Minimally invasive versus open transforaminal lumbar interbody fusion surgery: an analysis of opioids, nonopioid analgesics, and perioperative characteristics. Global Spine J 9(6):624–629
Jacob KC, Patel MR, Ribot MA et al (2022) Single-level TLIF versus LLIF at L4-5: a comparison of patient-reported outcomes and recovery ratios. J Am Acad Orthop Surg 30(4):e495–e505
Jiang S, Li W (2019) Biomechanical study of proximal adjacent segment degeneration after posterior lumbar interbody fusion and fixation: a finite element analysis. J Orthop Surg Res 14(1):135
Li GQ, Tong T, Wang LF (2022) Comparative analysis of the effects of OLIF and TLIF on adjacent segments after treatment of L4 degenerative lumbar spondylolisthesis. J Orthop Surg Res 17(1):203
Liang Z, Cui J, Zhang J et al (2020) Biomechanical evaluation of strategies for adjacent segment disease after lateral lumbar interbody fusion: is the extension of pedicle screws necessary? BMC Musculoskelet Disord 21(1):117
Louie PK, Haws BE, Khan JM et al (2019) Comparison of stand-alone lateral lumbar interbody fusion versus open laminectomy and posterolateral instrumented fusion in the treatment of adjacent segment disease following previous lumbar fusion surgery. Spine (Phila Pa 1976) 44(24):E1461–E1469
Mobbs RJ, Phan K, Malham G, Seex K, Rao PJ (2015) Lumbar interbody fusion: techniques, indications and comparison of interbody fusion options including PLIF, TLIF, MI-TLIF, OLIF/ATP LLIF and ALIF. J Spine Surg 1(1):2–18
Moro T, Kikuchi SI, Konno SI, Yaginuma H (2003) An anatomic study of the lumbar plexus with respect to retroperitoneal endoscopic surgery. Spine (Phila Pa 1976) 28(5):423–428 discussion 427-8
Okuda S, Yamashita T, Matsumoto T et al (2018) Adjacent segment disease after posterior lumbar interbody fusion: a case series of 1000 patients. Global Spine J. 8(7):722–727
Parker SL, Adogwa O, Paul AR et al (2011) Utility of minimum clinically important difference in assessing pain, disability, and health state after transforaminal lumbar interbody fusion for degenerative lumbar spondylolisthesis. J Neurosurg Spine 14(5):598–604
Parker SL, Mendenhall SK, Shau D et al (2012) Determination of minimum clinically important difference in pain, disability, and quality of life after extension of fusion for adjacent-segment disease. J Neurosurg Spine 16(1):61–67
Qin R, Wu T, Liu H, Zhou B, Zhou P, Zhang X (2020) Minimally invasive versus traditional open transforaminal lumbar interbody fusion for the treatment of low-grade degenerative spondylolisthesis: a retrospective study. Sci Rep 10(1):21851
Regev GJ, Chen L, Dhawan M, Lee YP, Garfin SR, Kim CW (2009) Morphometric analysis of the ventral nerve roots and retroperitoneal vessels with respect to the minimally invasive lateral approach in normal and deformed spines. Spine (Phila Pa 1976) 34(12):1330–1335
Trivedi NN, Wilson SM, Puchi LA, Lebl DR (2018) Evidence-based analysis of adjacent segment degeneration and disease after LIF: a narrative review. Global Spine J 8(1):95–102
Vora D, Kinnard M, Falk D et al (2018) A comparison of narcotic usage and length of post-operative hospital stay in open versus minimally invasive lumbar interbody fusion with percutaneous pedicle screws. J Spine Surg 4(3):516–521
Yang Z, Chang J, Sun L, Chen CM, Feng H (2020) Comparing oblique lumbar interbody fusion with lateral screw fixation and transforaminal full-endoscopic lumbar discectomy (OLIF-TELD) and posterior lumbar interbody fusion (PLIF) for the treatment of adjacent segment disease. Biomed Res Int 2020:4610128
Yasmeh S, Bernatz J, Garrard E, Bice M, Williams SK (2021) Clinical and radiographic outcomes of lateral interbody fusion for adjacent segment degeneration. Int J Spine Surg 15(1):74–81
Author information
Authors and Affiliations
Contributions
James W. Nie, BS: Conceptualization, methodology, visualization, formal analysis, software, investigation, writing—original draft, and writing—review and editing. Timothy J. Hartman, MD: Conceptualization, methodology, visualization, formal analysis, software, investigation, writing—original draft, and writing—review and editing. Eileen Zheng, BS: Project administration, data curation, investigation, and writing—review and editing. Keith R. MacGregor, BS: Project administration, data curation, investigation, and writing—review and editing. Omolabake O. Oyetayo, BS: Project administration, data curation, investigation, and writing—review and editing. Dustin H. Massel, MD: Conceptualization, methodology, supervision, resources, investigation, and writing—review and editing. Arash J. Sayari, MD: Conceptualization, methodology, supervision, resources, investigation, and writing—review and editing. Kern Singh, MD: Conceptualization, methodology, supervision, resources, investigation, and writing—review and editing.
Corresponding author
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Nie, J.W., Hartman, T.J., Zheng, E. et al. Postoperative clinical outcomes in patients undergoing MIS-TLIF versus LLIF for adjacent segment disease. Acta Neurochir 165, 1907–1914 (2023). https://doi.org/10.1007/s00701-023-05629-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-023-05629-z