
Abstract
Objective
The objective of this study was to systematically estimate the effectiveness and safety of annulus closure device (ACD) implantation in discectomy for patients with lumbar disc herniation (LDH).
Methods
A systematic search was performed on PubMed, EMBASE and the Cochrane Library for randomized controlled trial (RCT) from inception until April 16, 2022. Trials which investigated comparisons between with and without ACD implantation in discectomy for LDH patients were identified.
Results
In total, five RCTs involving 2380 patients with LDH underwent discectomy were included. The included patients were divided into ACD group and control group (CTL). Significant differences were found in the rate of re-herniation (ACD: 7.40%, CTL: 17.58%), reoperation (ACD: 5.39%, CTL: 13.58%) and serious adverse event (ACD: 10.79%, CTL: 17.14%) between ACD group and CTL group. No significant difference was found in VAS-BACK, VAS-LEG, ODI and SF-12 PCS between ACD and CTL. The surgical time of ACD was longer than CTL with statistical significance. In subgroup analyses based on discectomy type, significant differences were found in the rate of re-herniation (ACD: 10.73%, CTL: 21.27%), reoperation (ACD: 4.96%, CTL: 13.82%) and serious adverse event (ACD: 7.59%, CTL: 16.89%) between ACD and CTL in limited lumbar discectomy (LLD).
Conclusion
Discectomy either with or without ACD implantation is considered to achieve similar clinical outcomes. Whereas, the ACD implantation in LLD is associated with lower re-herniation and reoperation rate but prolonged surgical time for LDH patients. Researches on cost-effectiveness and effect of ACD implantation in different discectomy are needed in the future.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Since Mixter and Barr have first reported the surgical treatment for symptomatic lumbar disc herniation (LDH) in 1934 [1], discectomy is regarded as major treatment of symptomatic LDH. With the continuous advancement of minimally invasive surgery, various surgical approaches for lumbar discectomy have been invented and proposed, such as micro-discectomy, micro-endoscopic discectomy (MED), percutaneous endoscopic discectomy (PED), full-endoscopic discectomy (FED) and unilateral biportal endoscopic discectomy (UBE) [2,3,4,5,6]. Whereas, the problems of postoperative re-herniation and reoperation have not been solved [7, 8], which has become a consensus of high cost and poor prognosis [9, 10]. Therefore, the reduction of recurrence rate and reoperation rate has always been a research hotspot [11].
A study reported that postoperative re-herniation could be related to annular defects due to lumbar discectomy [12]. Moreover, Miller et al. [13] suggested that patients with large postoperative annular defects (≥ 6 mm width) had a 2.5-fold higher rate of re-herniation, compared with patients who had small annular defects (< 6 mm width) after discectomy. Hence, repairing annular defects to reduce the re-herniation rate and reoperation rate has been proposed in recent years, which was performed by implantation of an annular closure device (ACD)—Barricaid™ (Intrinsic Therapeutics, Inc., Woburn, MA, USA) or Xclose Tissue Repair System (Anulex Technologies, Minnetonka, MN) [14, 15]. Many clinical studies have been published focusing on their effectiveness. Some trials suggested that implantation of ACD resulted in better clinical outcomes [16, 17] and reduced the risk of symptomatic re-herniation and reoperation [18,19,20]. However, Bailey et al. [14] held different opinions, suggesting that the differences of re-herniation rate between groups at all follow-up time points were not statistically significant in their study. Considering the effect of these devices for preventing re-herniation remained controversial among individual studies, we performed this study to systematically estimate the effectiveness and safety of ACD implantation in lumbar discectomy for patients with LDH.
Materials and methods
Protocol and registration
The review protocol of this study was prospectively registered (PROSPERO, CRD42022309101), following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement and checklist.
Search methods and selection criteria
We performed a systematic search on PubMed, EMBASE and the Cochrane Library for randomized controlled trials (RCTs) from inception until April 16, 2022. Trials compared lumbar disc herniation (LDH) patients who underwent discectomy with and without implantation of ACD were identified. Keywords were used as annulus closure device, discectomy and lumbar disc herniation.
The selection criteria for including RCTs in this study were shown as follows: (1) performed the comparison between patients with LDH that underwent discectomy with and without the implantation of ACD; (2) participants were adults who suffer symptomatic LDH; (3) contained at least one outcome of interest. RCTs were excluded if: Interventions were different from the previous description; Or original data were not available.
Data extraction and statistical analyses
Two researchers extracted the data for meta-analysis independently. Description and outcomes of included trials were checked carefully. The primary outcomes were the rates of re-herniation and reoperation between ACD group and control (CTL) group. Secondary outcomes were visual analogue scale (VAS), oswestry disability index (ODI), physical component summary of 12-item short-form health survey (SF-12 PCS), surgical time and serious adverse event (SAE) between ACD group and CTL group. To compare the different effect of ACD between surgical techniques more precisely, subgroup analyses were performed based on the surgery type. Mean difference (MD) and 95% confidence interval (CI) were used for presenting the continuous outcomes. Dichotomous outcomes were presented by odds ratio (OR) and 95% CI. RevMan software (version 5.3) was used to perform all analyses. Between-study heterogeneity was evaluated using chi-squared test and I2. If the P value was < 0.05, statistical heterogeneity exists. In this situation, a random-effects model was utilized. P < 0.05 was considered to be statistically significant.
Assessment of risk of bias
The Cochrane Collaboration’s risk of bias criteria were used to evaluated the risk of bias in each included trial. The classifications of bias were based on seven items: random sequence generation (selection bias), allocation concealment (selection bias), blinding of participants and personnel (performance bias), blinding of outcome assessment (detection bias), incomplete outcome data (attrition bias), selective reporting (reporting bias) and other bias. Each item was rated as low risk, unclear risk, or high risk.
Results
Study selection and characteristics
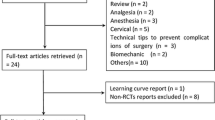
A total of 358 unique records were retrieved yielding 143 studies after removing duplications. One hundred and thirty studies were excluded according to the title and abstract screening. After removing duplications and full-text screening, eight trials were eliminated yielding five trials meeting the inclusion criteria for meta-analysis in this study (Fig. 1). The description and outcomes of all included trials are shown in Table 1. Five trials involving 2380 patients with symptomatic LDH underwent discectomy were included in this study [14, 21,22,23,24]. The sample size in these trials ranged from 60 to 727. All included trials contained explicit inclusion and exclusion criteria. Four trials performed discectomy with the implantation of bone-anchored annular closure device and one trials used Xclose Tissue Repair System as annular closure device. Three trials performed limited lumbar discectomy (LLD) and one trial performed limited micro-discectomy. The other trial reported that investigators performed discectomies per their standard practice, conducting with standard or tubular retractors, with or without use of an operating microscope or loupes.

Flow diagram showing the selection process of RCTs for meta-analysis
Meta-analysis results
Significant differences were found in the rate of re-herniation (ACD: 7.40%, CTL: 17.58%; OR: 0.43; 95% CI [0.31, 0.58], P < 0.001, I2 = 0%), reoperation (ACD: 5.39%, CTL: 13.58%; OR: 0.36; 95% CI [0.24, 0.53], P < 0.001, I2 = 0%) and SAE (ACD: 10.79%, CTL: 17.14%; OR: 0.52; 95% CI [0.33, 0.83], P = 0.006, I2 = 60%) between ACD group and CTL group at 24 months after surgery (Fig. 2). No significant difference was found in VAS-leg (MD, − 0.23 [95% CI − 0.69 to 0.23], P = 0.33, I2 = 0%) and VAS-back (MD, − 0.14 [95% CI − 0.60 to 0.33], P = 0.56, I2 = 0%) (Fig. 3). No statistical significance was found in SF-12 PCS (MD, − 0.56 [95% CI − 2.10 to 0.98], P = 0.48, I2 = 0%) between ACD group and CTL group, and the surgical time of ACD group was longer than CTL group with statistical significance (MD, 18.11 [95% CI 13.50 to 22.72], P < 0.001, I2 = 0%) (Fig. 3). There was no significant difference between ACD group and CTL group in ODI (MD, 0.59 [95% CI − 1.85 to 3.03], P = 0.64, I2 = 52%) (Fig. 3).

Pooling results of the ACD group and the CLT group. The results were shown as follows: re-herniation rate, reoperation rate and severe adverse event rate

Pooling results of the ACD group and the CLT group. The results were shown as follows: VAS-leg, VAS-back, SF-12 PCS, surgical time and ODI
Subgroup analysis results
In subgroup analyses based on the surgery type, significant differences were found in the rate of re-herniation (ACD: 10.73%, CTL: 21.27%; OR: 0.44; 95% CI [0.31, 0.63], P < 0.001, I2 = 0%), reoperation (ACD: 4.96%, CTL: 13.82%; OR: 0.33; 95% CI [0.21, 0.51], P < 0.001, I2 = 0%) and SAE (ACD: 7.59%, CTL: 16.89%; OR: 0.40; 95% CI [0.27, 0.60], P < 0.001, I2 = 0%) between ACD group and CTL group at 24 months after LLD (Fig. 4). The frequency of vertebral endplate changes in ACD group was superior to CTL group at 24 months after LLD (OR: 11.85; 95% CI [8.83, 15.90], P < 0.001, I2 = 0%) (Fig. 4).

Pooling results of subgroup analyses based on surgery type. The results were shown as follows: re-herniation rate, reoperation rate, severe adverse event rate and vertebral endplate changes
Risk of bias
The risk of bias in each included trial was evaluated following the Cochrane Collaboration’s risk of bias criteria. The appropriate random sequence generation was reported in all five trials and the allocation concealment in four trials [14, 21,22,23,24]. One trial was double-blind randomized controlled trial where surgeons and participants were blinded [22]. Trial of Bailey et al. [14] failed in blinding of outcome assessment. There was an industry funding in three trials [21, 23, 24], which was the reason that the other bias was unclear risk (Fig. 5).

Risk of bias summary
Discussion
The re-herniation rate (ACD: 7.40%, CTL: 17.58%) and reoperation rate (ACD: 5.39%, CTL: 13.58%) of ACD group were lower than CTL group with statistical significance at 24 months after surgery. Moreover, we performed a series of subgroup analyses based on surgery type. After discectomy was first reported as a surgical treatment for symptomatic LDH in 1934, O’Connell described an aggressive method for removing intervertebral disc, namely aggressive lumbar discectomy (ALD) [25]. ALD included removing the herniated disc fragment and scaling the remaining disc. Another method for disc removal described by Spengler and Williams emphasized removing the herniated disc alone without invasion of the disc space, namely LLD [26, 27]. LLD and ALD are both commonly used in clinical practice and have their own disadvantages. McGirt et al. [28] suggested that LLD was associated with lower incidence of long-term recurrent back pain but a higher incidence of re-herniation compared with ALD. In this presenting study, three trials performed LLD and one trial performed limited micro-discectomy [21,22,23,24]. The trial by Bailey et al. [14] reported that investigators performed discectomies per their standard practice, conducting with standard or tubular retractors, with or without use of an operating microscope or loupes. Sensitivity analysis showed that the data by Bailey et al. had no effect on the results. Moreover, the results of subgroup analyses showed that significant differences were found in the rate of re-herniation (ACD: 10.73%, CTL: 21.27%) and reoperation (ACD: 4.96%, CTL: 13.82%) at 24 months after LLD. The findings of this study suggested that the implantation of ACD was associated with lower re-herniation and reoperation rate specially for patients underwent LLD. And high-quality RCTs with sufficiently large sample sizes evaluating effect of ACD implantation in different methods of discectomy are needed in the future.
No significant difference was found in VAS-back, VAS-leg, ODI and SF-12 PCS between ACD group and CTL group in our study. Whereas, the comparison of ODI between ACD and CTL existed a high statistical heterogeneity (I2 = 52%). The number of participations in Cho’s trial was lower compared to other included trials. Moreover, about 70% participations in Cho’s trial was available at 2-year follow-up, which might limit the veracity of their conclusions of long-term outcome. Hence, we performed a sensitivity analysis when analyzing ODI. After omitting Cho’s study, there was no statistical heterogeneity found (I2 = 0%) and the result was not affected. These findings in this study indicated that the implantation of ACD did not affect the clinical outcomes, such as pain relief and disability recovery after lumbar discectomy in 2-year follow-up. However, a few clinical trials held different opinions. Kienzler et al. and Nanda et al. [17, 19] suggested that addition of a bone-anchored ACD in lumbar discectomy was associated with better long-term (over 3 or 4 years after surgery) pain and disability relief compared to discectomy alone. Bouma et al. [16] set subgroups by age and suggested that both younger and older patients derived better benefits in clinical outcomes with bone-anchored ACD implantation compared with discectomy alone.
The surgical time of ACD group was longer than CTL group with statistical significance in this study. The prolonged surgical time is associated with complications such as surgical site infection and it is a universal goal for surgeons to decreased surgical time continuously [29,30,31]. The introduction of a new technique into presenting surgery always requires surgeon to gain experience and overcome a learning curve to decrease the surgical time. Therefore, it is important for surgeon to weigh if the increase in surgical time caused by a new technique could be justified by the benefits it provides. The methods on reducing the additional surgical time for ACD implantation needs further research in the future.
Vertebral endplate changes (VEPC) are common in lumbar spine and could be classified as Schmorl’s nodes, fracture, erosion, or calcification [32]. Brayda-Bruno et al. [33] reported that the “notched” and “Schmorl’s nodes” were the most common classification of VEPC, and VEPC was found to be associated with disc degeneration and signal alterations on MRI. Moreover, Feng et al. [34] suggested that cartilaginous endplate avulsion could be associated with residual pain after lumbar discectomy. The study of Zehra et al. [35] also noted that increased endplate defect was directly associated with facet joint changes, leading to pain. The VEPC of ACD group were superior to CTL group at 24 months after LLD in this presenting study. Whereas, VEPC had no impact on SAE rate and various clinical outcomes such as ODI, VAS and SF-12 PCS based on our results. Future studies should focus on long-term follow-up and evaluate the long-term effect of VEPC after ACD implantation on surgical outcomes.
At present, Barricaid™ is the most popular annular closing device on the market. The Xclose device is no longer available right now, and there is other solution called AnchorKnot® used in some centers [36, 37]. Ament et al. performed a cost-effectiveness analysis of ACD implantation for lumbar discectomy in 2019 [38]. They suggested that the ACD implantation was highly cost-effective compared to lumbar discectomy alone at 2 years after surgery for LDH patients with large postoperative annular defects (≥ 6 mm). According to its effect and prolonged surgical time, we suggested that ACD implantation should be treated with caution. As the results shown in this presenting study, there is currently no strong evidence suggesting that discectomy with ACD implantation is economically favorable and surgically safer compared to standard discectomy. At present, the subgroup suitable for ACD implantation could be LDH patients undergoing LLD with large annular defects (≥ 6 mm).
The objective of this study was to systematically estimate the effectiveness and safety of ACD implantation in lumbar discectomy for patients with LDH. There were two studies based on fewer number and mixed clinical trials (randomized or non-randomized) on similar topic with low credibility [39, 40]. In this meta-analysis, we recruited five RCTs which performed the comparison between ACD and CTL after discectomy, including 2380 patients (1289 in ACD group and 1091 in CTL group). Moreover, subgroup analyses were performed based on the surgery type to compare the effect of ACD implantation between surgical techniques more precisely. Whereas, there were still several limitations in this study. First, the cost-effectiveness of ACD implantation in discectomy for patients with LDH was not available in the included trials. Second, clear allocation concealment was not presented in some included trials.
Conclusion
Discectomy either with or without ACD implantation is considered to achieve similar clinical outcomes. Whereas, the ACD implantation in LLD is associated with lower re-herniation and reoperation rate but prolonged surgical time for LDH patients. We suggested that ACD implantation should be treated with caution. More independently high-quality RCTs with sufficiently large sample sizes reporting cost-effectiveness and evaluating the effect of ACD implantation in different discectomy are needed.
Abbreviations
- ACD:
-
Annulus closure device
- LDH:
-
Lumbar disc herniation
- LLD:
-
Limited lumbar discectomy
- SCIE:
-
Science citation index expanded
- WoS:
-
Web of Science
- PRISMA:
-
Preferred reporting items for systematic reviews and meta-analyses
- RCT:
-
Randomized controlled trial
- MED:
-
Micro-endoscopic discectomy
- PED:
-
Percutaneous endoscopic discectomy
- UBE:
-
Unilateral biportal endoscopic discectomy
- VAS:
-
Visual analogue scale
- SEA:
-
Serious adverse event
- ODI:
-
Oswestry disability index
- SF-12 PCS:
-
Physical component summary of 12-item short-form health survey
- MD:
-
Mean difference
- 95% CI:
-
95% Confidence interval
- OR:
-
Odds ratio
- ALD:
-
Aggressive lumbar discectomy
- VEPC:
-
Vertebral endplate changes
- NA:
-
Not available
- Exp:
-
Experimental group
- CTL:
-
Control group
References
Mixter WJ, Barr JS (1934) Rupture of the intervertebral disc with involvement of the spinal canal. N Engl J Med 211:210–215. https://doi.org/10.1056/nejm193408022110506
Kim SK, Kang SS, Hong YH, Park SW, Lee SC (2018) Clinical comparison of unilateral biportal endoscopic technique versus open microdiscectomy for single-level lumbar discectomy: a multicenter, retrospective analysis. J Orthop Surg Res 13:22. https://doi.org/10.1186/s13018-018-0725-1
Mayer HM, Brock M, Berlien HP, Weber B (1992) Percutaneous endoscopic laser discectomy (PELD). A new surgical technique for non-sequestrated lumbar discs. Acta Neurochir Suppl (Wien) 54:53–58. https://doi.org/10.1007/978-3-7091-6687-1_7
Foley KT, Smith MM, Rampersaud YR (1999) Microendoscopic approach to far-lateral lumbar disc herniation. Neurosurg Focus 7:e5. https://doi.org/10.3171/foc.1999.7.6.6
Ruetten S, Komp M, Godolias G (2005) An extreme lateral access for the surgery of lumbar disc herniations inside the spinal canal using the full-endoscopic uniportal transforaminal approach-technique and prospective results of 463 patients. Spine (Phila Pa 1976) 30:2570–2578. https://doi.org/10.1097/01.brs.0000186327.21435.cc
Yeung AT, Tsou PM (2002) Posterolateral endoscopic excision for lumbar disc herniation: surgical technique, outcome, and complications in 307 consecutive cases. Spine (Phila Pa 1976) 27:722–731. https://doi.org/10.1097/00007632-200204010-00009
Cheng J, Wang H, Zheng W, Li C, Wang J, Zhang Z, Huang B, Zhou Y (2013) Reoperation after lumbar disc surgery in two hundred and seven patients. Int Orthop 37:1511–1517. https://doi.org/10.1007/s00264-013-1925-2
Heindel P, Tuchman A, Hsieh PC, Pham MH, D’Oro A, Patel NN, Jakoi AM, Hah R, Liu JC, Buser Z, Wang JC (2017) Reoperation rates after single-level lumbar discectomy. Spine (Phila Pa 1976) 42:E496-e501. https://doi.org/10.1097/brs.0000000000001855
Ambrossi GL, McGirt MJ, Sciubba DM, Witham TF, Wolinsky JP, Gokaslan ZL, Long DM (2009) Recurrent lumbar disc herniation after single-level lumbar discectomy: incidence and health care cost analysis. Neurosurgery 65:574–578. https://doi.org/10.1227/01.Neu.0000350224.36213.F9
Adogwa O, Parker SL, Shau DN, Mendenhall SK, Aaronson O, Cheng JS, Devin CJ, McGirt MJ (2012) Cost per quality-adjusted life year gained of revision neural decompression and instrumented fusion for same-level recurrent lumbar stenosis: defining the value of surgical intervention. J Neurosurg Spine 16:135–140. https://doi.org/10.3171/2011.9.Spine11308
Aihara T, Endo K, Sawaji Y, Suzuki H, Urushibara M, Kojima A, Matsuoka Y, Takamatsu T, Murata K, Kusakabe T, Maekawa A, Yamamoto K (2020) Five-year reoperation rates and causes for reoperations following lumbar microendoscopic discectomy and decompression. Spine (Phila Pa 1976) 45:71–77. https://doi.org/10.1097/brs.0000000000003206
Carragee EJ, Han MY, Suen PW, Kim D (2003) Clinical outcomes after lumbar discectomy for sciatica: the effects of fragment type and anular competence. J Bone Joint Surg Am 85:102–108
Miller LE, McGirt MJ, Garfin SR, Bono CM (2018) Association of annular defect width after lumbar discectomy with risk of symptom recurrence and reoperation: systematic review and meta-analysis of comparative studies. Spine (Phila Pa 1976) 43:E308-e315. https://doi.org/10.1097/brs.0000000000002501
Bailey A, Araghi A, Blumenthal S, Huffmon GV (2013) Prospective, multicenter, randomized, controlled study of anular repair in lumbar discectomy: two-year follow-up. Spine (Phila Pa 1976) 38:1161–1169. https://doi.org/10.1097/BRS.0b013e31828b2e2f
Klassen PD, Bernstein DT, Köhler HP, Arts MP, Weiner B, Miller LE, Thomé C (2017) Bone-anchored annular closure following lumbar discectomy reduces risk of complications and reoperations within 90 days of discharge. J Pain Res 10:2047–2055. https://doi.org/10.2147/jpr.S144500
Bouma GJ, Ardeshiri A, Miller LE, Van de Kelft E, Bostelmann R, Klassen PD, Flüh C, Kuršumović A (2019) Clinical performance of a bone-anchored annular closure device in older adults. Clin Interv Aging 14:1085–1094. https://doi.org/10.2147/cia.S208098
Nanda D, Arts MP, Miller LE, Köhler HP, Perrin JM, Flüh C, Vajkoczy P (2019) Annular closure device lowers reoperation risk 4 years after lumbar discectomy. Med Devices (Auckl) 12:327–335. https://doi.org/10.2147/mder.S220151
Kienzler JC, Fandino J, Van de Kelft E, Eustacchio S, Bouma GJ (2021) Risk factors for early reherniation after lumbar discectomy with or without annular closure: results of a multicenter randomized controlled study. Acta Neurochir (Wien) 163:259–268. https://doi.org/10.1007/s00701-020-04505-4
Kienzler JC, Klassen PD, Miller LE, Assaker R, Heidecke V, Fröhlich S, Thomé C (2019) Three-year results from a randomized trial of lumbar discectomy with annulus fibrosus occlusion in patients at high risk for reherniation. Acta Neurochir (Wien) 161:1389–1396. https://doi.org/10.1007/s00701-019-03948-8
van den Brink W, Flüh C, Miller LE, Klassen PD, Bostelmann R (2019) Lumbar disc reherniation prevention with a bone-anchored annular closure device: 1-year results of a randomized trial. Medicine (Baltimore) 98:e17760. https://doi.org/10.1097/md.0000000000017760
Barth M, Weiß C, Bouma GJ, Bostelmann R, Kursumovic A, Fandino J, Thomé C (2018) Endplate changes after lumbar discectomy with and without implantation of an annular closure device. Acta Neurochir (Wien) 160:855–862. https://doi.org/10.1007/s00701-017-3463-y
Cho PG, Shin DA, Park SH, Ji GY (2019) Efficacy of a novel annular closure device after lumbar discectomy in Korean patients : a 24-month follow-up of a randomized controlled trial. J Korean Neurosurg Soc 62:691–699. https://doi.org/10.3340/jkns.2019.0071
Kuršumović A, Kienzler JC, Bouma GJ, Bostelmann R, Heggeness M, Thomé C, Miller LE, Barth M (2018) Morphology and clinical relevance of vertebral endplate changes following limited lumbar discectomy with or without bone-anchored annular closure. Spine (Phila Pa 1976) 43:1386–1394. https://doi.org/10.1097/brs.0000000000002632
Thomé C, Klassen PD, Bouma GJ, Kuršumović A, Fandino J, Barth M, Arts M, van den Brink W, Bostelmann R, Hegewald A, Heidecke V, Vajkoczy P, Fröhlich S, Wolfs J, Assaker R, Van de Kelft E, Köhler HP, Jadik S, Eustacchio S, Hes R, Martens F (2018) Annular closure in lumbar microdiscectomy for prevention of reherniation: a randomized clinical trial. Spine J 18:2278–2287. https://doi.org/10.1016/j.spinee.2018.05.003
O’Connell JE (1951) Protrusions of the lumbar intervertebral discs, a clinical review based on five hundred cases treated by excision of the protrusion. J Bone Joint Surg Br 33-b:8–30. https://doi.org/10.1302/0301-620x.33b1.8
Williams RW (1978) Microlumbar discectomy: a conservative surgical approach to the virgin herniated lumbar disc. Spine (Phila Pa 1976) 3:175–182
Spengler DM (1982) Lumbar discectomy. Results with limited disc excision and selective foraminotomy. Spine (Phila Pa 1976) 7:604–607
McGirt MJ, Ambrossi GL, Datoo G, Sciubba DM, Witham TF, Wolinsky JP, Gokaslan ZL, Bydon A (2009) Recurrent disc herniation and long-term back pain after primary lumbar discectomy: review of outcomes reported for limited versus aggressive disc removal. Neurosurgery 64:338–344. https://doi.org/10.1227/01.Neu.0000337574.58662.E2
Cheng H, Chen BP, Soleas IM, Ferko NC, Cameron CG, Hinoul P (2017) Prolonged operative duration increases risk of surgical site infections: a systematic review. Surg Infect (Larchmt) 18:722–735. https://doi.org/10.1089/sur.2017.089
Cheng H, Clymer JW, Po-Han Chen B, Sadeghirad B, Ferko NC, Cameron CG, Hinoul P (2018) Prolonged operative duration is associated with complications: a systematic review and meta-analysis. J Surg Res 229:134–144. https://doi.org/10.1016/j.jss.2018.03.022
Held MB, Boddapati V, Sarpong NO, Cooper HJ, Shah RP, Geller JA (2021) operative duration and short-term postoperative complications after unicompartmental knee arthroplasty. J Arthroplast 36:905–909. https://doi.org/10.1016/j.arth.2020.09.007
Wang Y, Videman T, Battié MC (2012) Lumbar vertebral endplate lesions: prevalence, classification, and association with age. Spine (Phila Pa 1976) 37:1432–1439. https://doi.org/10.1097/BRS.0b013e31824dd20a
Brayda-Bruno M, Albano D, Cannella G, Galbusera F, Zerbi A (2018) Endplate lesions in the lumbar spine: a novel MRI-based classification scheme and epidemiology in low back pain patients. Eur Spine J 27:2854–2861. https://doi.org/10.1007/s00586-018-5787-6
Feng ZY, Hu XJ, Zheng QQ, Battié MC, Chen Z, Wang Y (2021) Cartilaginous endplate avulsion is associated with modic changes and endplate defects, and residual back and leg pain following lumbar discectomy. Osteoarthr Cartil 29:707–717. https://doi.org/10.1016/j.joca.2021.01.010
Zehra U, Cheung JPY, Bow C, Lu W, Samartzis D (2019) Multidimensional vertebral endplate defects are associated with disc degeneration, modic changes, facet joint abnormalities, and pain. J Orthop Res 37:1080–1089. https://doi.org/10.1002/jor.24195
Bateman AH, Balkovec C, Akens MK, Chan AH, Harrison RD, Oakden W, Yee AJ, McGill SM (2016) Closure of the annulus fibrosus of the intervertebral disc using a novel suture application device-in vivo porcine and ex vivo biomechanical evaluation. Spine J 16:889–895. https://doi.org/10.1016/j.spinee.2016.03.005
Guardado AA, Baker A, Weightman A, Hoyland JA, Cooper G (2022) Lumbar intervertebral disc herniation: annular closure devices and key design requirements. Bioengineering (Basel). https://doi.org/10.3390/bioengineering9020047
Ament J, Thaci B, Yang Z, Kulubya E, Hsu W, Bouma G, Kim KD (2019) Cost-effectiveness of a bone-anchored annular closure device versus conventional lumbar discectomy in treating lumbar disc herniations. Spine (Phila Pa 1976) 44:5–16. https://doi.org/10.1097/brs.0000000000002746
Choy WJ, Phan K, Diwan AD, Ong CS, Mobbs RJ (2018) Annular closure device for disc herniation: meta-analysis of clinical outcome and complications. BMC Musculoskelet Disord 19:290. https://doi.org/10.1186/s12891-018-2213-5
Miller LE, Allen RT, Duhon B, Radcliff KE (2020) Expert review with meta-analysis of randomized and nonrandomized controlled studies of Barricaid annular closure in patients at high risk for lumbar disc reherniation. Expert Rev Med Devices 17:461–469. https://doi.org/10.1080/17434440.2020.1745061
Acknowledgements
This study was supported by National Natural Science Foundation of China (NO: 81871803). The funder had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interests
The authors have no conflict of interest to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Li, WS., Li, GY., Yan, Q. et al. The effectiveness and safety of annulus closure device implantation in lumbar discectomy for patients with lumbar disc herniation: a systematic review and meta-analysis. Eur Spine J 32, 2377–2386 (2023). https://doi.org/10.1007/s00586-023-07629-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-023-07629-0