
Abstract
Gastric cancer is a significant global health problem. It is the fifth most common cancer and third leading cause of cancer-related death worldwide (Torre et al. in CA Cancer J Clin 65(2):87–108, 2015). Despite advances in treatment, overall prognosis remains poor, due to tumour relapse and metastasis. There is an urgent need for novel therapeutic approaches to improve clinical outcomes in gastric cancer. The cancer stem cell (CSC) model has been proposed to explain the high rate of relapse and subsequent resistance of cancer to current systemic treatments (Vermeulen et al. in Lancet Oncol 13(2):e83–e89, 2012). CSCs have been identified in many solid malignancies, including gastric cancer, and have significant clinical implications, as targeting the CSC population may be essential in preventing the recurrence and spread of a tumour (Dewi et al. in J Gastroenterol 46(10):1145–1157, 2011). This review seeks to summarise the current evidence for CSC in gastric cancer, with an emphasis on candidate CSC markers, clinical implications, and potential therapeutic approaches.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Cancer stem cells
Cancer stem cell theory
A key issue in oncology is whether cancer growth is driven by the majority of tumour cells or by a rare subpopulation of cancer stem cells (CSCs). There are several proposed models. The clonal evolution model states that each cell within a tumour has equal potential of undergoing genetic/epigenetic changes which confer growth advantages and subsequent new tumour growth [4]. The cancer stem cell (CSC) model, on the other hand, proposes that the growth of the tumour is driven by a small population of self-sustaining cells with the stem cell properties of longevity, infinite proliferation, and an ability to differentiate into the entire heterogeneous population of the tumour [5]. Integral to the CSC model is a subpopulation at the apex of the hierarchy (usually comprising <5 % of the cancer), responsible for the formation, maintenance, and continued growth of the tumour [3]. Stem cells can symmetrically divide into identical daughter stem cells with self-renewal capacity, or asymmetrically divide into both a differentiated progenitor cell and a stem cell [6].
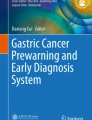
Recent refinements to the CSC theory propose a more dynamic model, with a fluid CSC population regulated by the tumour cell environment rather than a rigid hierarchical structure [2, 5]. It is now apparent that a CSC phenotype can be induced in differentiated cancer cells by exposure to growth factors secreted from stromal cells, suggesting a bidirectional pathway between the CSC and differentiated cell populations [7, 8]. Furthermore, research has shown that some types of leukaemic stem cells are subjected to clonal evolution [9]. The reacquisition of self-renewal properties in non-CSC populations, in addition to the genotypic and phenotypic heterogeneity within CSCs, highlights the fluidity of the CSC population in both number and character (Fig. 1).

Three models of tumour growth and their clinical implications. a The clonal model, where each cell has the potential to acquire additional mutations which confer a growth advantage. Chemotherapy selects a treatment-resistant subclone, which subsequently reconstitutes the tumour mass. b The hierarchical cancer stem cell (CSC) model, whereby a small population of self-renewing CSCs are responsible for all tumour growth, giving rise to progenitor cells, which subsequently de-differentiate into the bulk of the tumour which has lost the capacity for self-renewal. The chemoresistant CSC population is enriched by chemotherapy, and is able to restore the tumour bulk. c The dynamic CSC model is a more refined model, demonstrating the bidirectional flow of cells between the stem cell and differentiated compartments. This model highlights the need to combine a CSC-targeted agent with chemotherapy. The targeted agent eliminates the chemoresistant CSC population, preventing the reconstitution of the tumour bulk, while the chemotherapy reduces the tumour bulk of differentiated cells, stopping these cells from de-differentiating to replenish the CSC population
CSCs are defined functionally rather than by cellular origin, with CSCs having superior tumour initiation, growth, and metastatic potential to that of other tumour cells [10]. In vitro studies with cultured gastric CSCs have found these cells to be more resistant to chemotherapy and radiotherapy [11, 12], possibly due to high expression of anti-apoptotic proteins, increased efficiency of DNA repair, and alterations in cell cycle kinetics [5, 6]. CSCs are responsible for the renewal of tumour mass following systemic treatment and the development of treatment-resistant subclones [6]. The long proliferative lifespan and repeated DNA replication events in CSCs render them more susceptible to further mutation and epigenetic changes, creating additional malignant clones [13].
The first definitive evidence of a CSC population was provided by Bonnet et al. [14], who demonstrated that a cell population defined by the CD34+/38− phenotype was able to serially reproduce acute myeloid leukaemia (AML) in immunodeficient mice. Importantly, this cell population was not only capable of self-renewal, but could reconstitute the full spectrum of cell populations seen in AML. This approach has been used to isolate CSCs in solid malignancies including breast cancer [15], prostate cancer [16], pancreatic cancer [17, 18], melanoma [19], colon cancer [20, 21], brain cancer [22, 23], and liver cancer [24], supporting the model of cancer growth initiated and maintained by CSCs. The presence of CSCs in solid malignancies has been confirmed in lineage tracing studies, which identified a subpopulation of cells that reconstitute the entire tumour following chemotherapy [25].
Experimental evidence for CSCs must demonstrate both self-renewal and an ability to differentiate into the heterogeneous cell populations that constitute a tumour [26]. Serial transplantation in animal models fulfils these criteria, and has been proposed as the best functional assay for identification of CSCs [26]. An alternative experimental model is in vitro spheroid colony formation of candidate CSCs in culture media, as continued growth of colonies indicates self-renewal [27]. Although serial passage in animal models is considered the gold standard, the two methods seem to provide similar results in identifying candidate CSCs [27].
The CSC model has important clinical implications, as it implies that anti-neoplastic treatments should focus on eliminating both a small population of CSCs within the tumour and the rapidly dividing but terminally differentiated bulk cancer cells [26]. Figure 1 provides schematic illustrations of the various models.
Cancer stem cells and metastases
The unique CSC properties of self-renewal and multi-lineage differentiation suggest a likely role in the initiation and progression of distant metastatic disease. Although there is no direct experimental evidence of CSCs as the origin of metastases, many studies have provided supporting data [28]. Various works have shown that the presence of unique tumour subpopulations with CSC markers is integral to the development of metastatic disease in a number of malignancies, including pancreatic [17], colorectal [29], and breast [30] cancer, as depletion of this population prevented the metastatic spread of the tumour [17]. Dieter et al. [31] demonstrated differential contributions of individual CSC clones to the growth of primary and metastatic tumours, and identified a subpopulation of CSCs in colon cancer solely responsible for the formation of metastases. In addition, immunohistochemical studies in gastric cancer have shown an increased risk of metastatic disease associated with CSC marker expression in the primary tumour [32, 33].
A proposed mechanism underlying the metastatic progression of cancer is the epithelial-mesenchymal transition (EMT) [34], which is the process whereby tumour cells lose epithelial characteristics and acquire a mesenchymal phenotype to facilitate cancer metastasis and survival. It is becoming increasingly evident that EMT and CSC phenotypes are largely overlapping, providing properties of invasion, tumour seeding, drug resistance, and survival. CSCs in primary tumours are thought to metastasize to distant sites via EMT [35]. Furthermore, a CSC phenotype can be obtained through induction of an EMT state [36, 37]. Tumour cells disseminated in the blood (circulating tumour cells) are enriched for both EMT and CSC phenotypes [38]. Gastric cancer patients who have detectable circulating tumour cells (CTCs) that express CSC markers have a poorer prognosis than those who have CTCs without CSC markers [39]. This is reinforced by clinical evidence of an association between EMT and CSCs, with immunohistochemical expression of CD44, a gastric CSC marker, significantly correlated with expression of EMT markers such as Snail-1 and ZEB1 in resected gastric cancer [40]. Gastric CSCs isolated from a cell line have shown increased expression of EMT markers (including Snail, Twist, and vimentin) and CD44 [41]. Moreover, analysis of the combined expression of CD44 and EMT markers was predictive of poorer disease-free and overall survival (OS) in a multivariate model, consistent with the aggressive phenotype of cells expressing CSC and EMT markers [40].
Identification of cancer stem cells
A key issue in the study of CSCs is the ability to develop reproducible and reliable methods for CSC isolation and identification. The American Association for Cancer Research (AACR) defines CSCs as subpopulations of cells within a tumour that possess the capacity for self-renewal and generation of heterogeneous lineages of cancer cells that constitute the tumour [26]. As discussed above, two experimental methods are used to confirm a population of cells as CSCs: serial passage of tumours in animal models and tumour-spheroid assays. Animal model serial transplantation is regarded as the gold standard, as it is considered a physiologically relevant functional assay for demonstrating self-renewal and lineage capacity [26]. Some groups have questioned this paradigm, however, as the rarity of CSCs found in human cancers may be the result of an inadequate local environment in the xenograft [42, 43]. Tumour spheroid assays are a more rapid method (as serial transplantation can take several months), and have been shown to increase expression of stem cell markers, although there are potential pitfalls, as not all isolated CSCs form spheroids [12, 44].
There are many challenges in identifying a CSC population within a tumour. First, as discussed above, the CSC population is dynamic, with bidirectional flow between the CSC and differentiated cell populations. Second, the CSC markers currently in use are not specific, and are expressed on both non-malignant cells and early progenitor cells that have lost stem cell features but retained phenotypic markers. Third, multiple populations of CSCs may exist within a tumour mass, and combinations of multiple markers may be required to identify the complete CSC population.
Candidate CSCs are identified predominantly by one of two methods: the side population assay or the expression of CSC surface markers.
Side population assay
The side population (SP) assay identifies the fraction of cells that efflux Hoechst dye through ATP binding cassette (ABC) transporters. It is a highly preserved marker of stem cells across a variety of tissues and tumours, with a higher capacity for self-renewal, leading some authors to suggest that the SP subset may represent a universal CSC population [45]. However, the SP assay is hampered by poor specificity, with differentiated adults cells in the gastrointestinal tract demonstrating a SP phenotype [46].
The results regarding SP assays as a potential CSC marker in gastric cancer are inconsistent. Zhange et al. [47] showed CSC properties in SP cells from the MKN-45 cell line but not the BGC-823 cell line. Although some studies in gastric cancer lines have shown CSC properties in the SP [48, 49], others have found no difference compared to a non-SP subset [11, 50, 51]. Overall, therefore, the utility of the SP assay for identification of gastric CSCs remains controversial.
Expression of cell surface markers
An integral tool in the identification and isolation of candidate CSCs is the expression of unique combinations of cell surface markers. This approach has allowed the isolation of CSCs in many solid malignancies using flow cytometry or magnetic cell sorting. CSC markers identified to date are expressed in an overlapping manner on a variety of tumours, as well as on normal stem cells. A summary of the most common markers described for solid tumours is provided in Table 1. Many of these potential markers are found in gastric cancer.
Gastric cancer stem cells
Origin of gastric cancer stem cells
The origin of gastric CSCs remains uncertain. One possible source is gastric stem cells which have lost regulated quiescence. The existence of multipotent gastric stem cells that give rise to all major epithelial cell types has been demonstrated in mouse models [52]. There are multiple populations of gastric stem cells. The Lgr5+ cells arise at the base of the gastric gland and continuously differentiate into all antral unit cells, while the villin+ cells are located at the isthmus and are a quiescent stem cell population which require cytokine stimulation for activation, serving as a stem cell source if the Lgr5+ cells are damaged [53–55]. Sox2+ cells, present in the antrum and corpus, are able to differentiate into all cell types found in a gastric unit, and ablation of the Sox2+ population prevents renewal of gastric epithelium [56]. Other populations of differentiated gastric cells, such as chief cells expressing the marker Troy, have been shown to de-differentiate and function as multipotent stem cells, acting as reserve stem cell populations [57].
Aberrant genetic and epigenetic mutations in these gastric stem cells, in conjunction with stimulating factors from the microenvironment, may lead to the formation of CSCs [13]. In one study, for example, APC deletion in Lgr5+ stem cells in a mouse model led to the rapid development of adenomas, due to the expansion of the stem cell compartment [54]. Wu et al. [53] demonstrated co-localisation of CSC markers (CD26, CD44, ALDH1, CD133) with Lgr5+ cells in gastric cancer, suggesting they may be functionally related. Similarly, Sox2 expression was found to be altered during the pathogenesis of gastric cancer [58, 59], although reports are contradictory as to whether Sox2 is over-expressed and oncogenic [60, 61] or down-regulated and anti-oncogenic, with lower Sox2 levels associated with poorer clinical outcomes [58, 62]. Another proposed gastrointestinal stem cell marker, doublecortin-like kinase (Dclk1), is highly expressed on cells in the stem cell zone of mouse gastric glands [63]. K-ras-induced chronic inflammation in K19-K-ras-V12 transgenic mice led to expansion of the Dclk1+ cell population during the development of high-grade dysplasia [64].
An alternative hypothesis suggests that gastric CSCs arise from bone marrow-derived mesenchymal stem cells—pluripotent adult stem cells that are recruited to peripheral organs in response to chronic inflammation. Their function is to assist in regeneration after failure of local stem cells [65]. Bone marrow-derived cells (BMDC) have been shown to repopulate gastric mucosa in response to chronic inflammation due to H. Pylori infection, and may contribute to carcinogenesis [66, 67]. In a mouse model infected with H. pylori, almost a quarter of high-grade dysplastic gastric lesions included BMDC [68]. These cells are thought to differentiate in the gastric mucosa by cell–cell fusion with local gastric epithelial cells and in the context of further chronic inflammation, induce EMT and the emergence of CSCs [65, 69]. It is important to note, however, that despite these provocative findings, the majority of dysplastic lesions do not arise from BMDC. Further studies are needed to fully explore the pathogenesis of gastric CSCs.
Gastric CSC markers
CD44
CD44 is a transmembrane glycoprotein expressed on leukocytes, endothelial cells, hepatocytes, and mesenchymal cells, and has a variety of physiological roles, including matrix adhesion, cell migration, and differentiation [70]. CD44 has been proposed as a mediator of signal transduction of oncogenic pathways such as the human epidermal growth factor receptor (HER) [71]. Cancer cells with high CD44 expression have enhanced resistance to reactive oxygen species as a result of increased glutathione synthesis and upregulation of antioxidant genes [72]. The first evidence of gastric CSCs was demonstrated with the self-renewal and heterogeneous lineage of a CD44+ subpopulation [11]. There are now numerous studies supporting CD44 as a marker for CSC in gastric cancer (Table 2; details of studies available in Supplementary Table 1). Two studies, however, were unable to demonstrate stem cell properties in the CD44+ purified subset of patient-derived gastric cancer cells, perhaps due to inappropriate microenvironments in mouse models [73, 74]. CSC populations have also been identified using a combination of CD44+ and other markers, including EpCAM [75, 76], CD54+ [77], and CD24 [78].
Notwithstanding the above-referenced works, CD44 is not a specific or sensitive marker for gastric CSC. The true CSC population has been estimated at <5 % of CD44+ cells [11], and CD44 is widely expressed on non-malignant tissue. Other markers are required in addition to CD44 to improve the specificity of CSC identification.
CD44 variants
CD44 is encoded by the 20-exon CD44 gene, with exons 1–5 encoding the constant region of the extracellular domain and exons 16–20 spliced together to form the standard isoform [76]. The variant exons 6–15 are subject to alternative splicing, and can be assembled in different combinations with the standard exon to generate variant isoforms [76]. CD44 variants (designated as CD44v) have been proposed as a more specific CSC marker than CD44 given their more restricted distribution pattern. Generally, expression of CD44v on gastric cancers cells correlates well with CD44 expression [32, 76].
There is only limited evidence of CD44v as a CSC marker. Lau et al. [76] showed that CD44v8-10 was the predominant CD44v expressed on CD44+ gastric cancer cells (79 % of CD44+ cells), and demonstrated self-renewal and heterogeneous lineage in serial transplants of CD44v8–10 in mouse models. Although the CD44v8-10+ fraction was more tumorigenic in mouse models, both the CD44v8-10+ and CD44v8-10- cells were able to form tumour spheres [76]. While CD44v appears to be a more specific marker for gastric cancer than CD44, more research is needed to elucidate its biological role and confirm CSC characteristics.
CD133
CD133 is a transmembrane glycoprotein plasma membrane protein found on embryonic epithelial structures and hematopoietic stem cells [79]. It has been proposed to function as an organiser of plasma membrane topology, and to play a role in maintaining appropriate lipid composition within the plasma membrane [80]. CD133 has been identified as a CSC marker in a variety of solid tumours (Table 1).
Most studies have identified CSCs using AC133, an antibody that detects a glycosylated epitope of CD133 [81]. Some authors have recommended caution in using CD133 as a marker to identify CSC, after they showed downregulation of CD133 epitopes (including the target of AC133) during differentiation but constant CD133 protein expression, suggesting that differentiated cells may express CD133, but with masked epitopes due to differential glycosylation [82]. Post-translational modification of CD133 may play a role in invasion and metastases, and may influence antibody binding by altering the epitope’s accessibility [81].
Consequently, there is debate regarding the utility of CD133 as a CSC marker in gastric cancer. Although some studies have demonstrated CSC properties with the CD133+ subpopulation, several groups have found contrasting results, with CD133- cells able to initiate tumours [11, 73, 76] (Table 2; Supplementary Table 1).
ALDH1
Aldehyde dehydrogenase (ALDH) is a family of enzymes that play a role in cellular detoxification, differentiation, and drug resistance via oxidation of cellular aldehydes [83]. ALDH1 functions as a modulator of cell proliferation and stem cell differentiation, and is a marker of CSCs in a variety of cancers (Table 1). High ALDH1 activity confers resistance to chemotherapeutic agents [84]. ALDHhigh cell populations are identified with the ALDEFLUOR assay or by the ALDH1 antibody, and have been shown to correlate with CD44 expression [85].
Katsuno et al. [86] demonstrated CSC properties, including self-renewal, heterogeneous lineage, and increased tumorigenicity, in ALDH1+ cells isolated from gastric cancer cell lines. Interestingly, they found that TGF-β inhibited the function of the CSC population, in contrast to other cancers [86]. Studies demonstrating the CSC properties of ALDH1 in gastric cancer are summarised in Table 2 and Supplementary Table 1.
Other potential CSC markers
Numerous other molecules have been identified as potential gastric CSC markers, and these are addressed below. However, it is important to bear in mind that the evidence for these molecules as markers is either limited or contradictory. Further studies are thus required to either confirm or refute their utility as markers of the CSC population.
CD24 is a cell surface adhesion molecule expressed on leukocytes, normal gastric parietal cells, and intestinal stem cells [87]. CD24 expression is associated with aggressive clinicopathological features in gastric cancer, and facilitates cell migration and invasion in gastric cancer cells [87, 88]. Evidence for CD24 as a CSC marker in gastric cancer is conflicting. Zang et al. [78] found that the CD44+/CD24+ cell population isolated CSCs in gastric cancer cell lines, while Takaishi et al. [11] were unable to find evidence of CSC characteristics in a CD24+ population in spheroid and mouse models.
The epithelial cellular adhesion molecule (EpCAM) is a transmembrane glycoprotein detected in the majority of epithelial tissues, with roles in cell adhesion, signalling, migration, proliferation, and differentiation [89]. EpCAM is over-expressed in gastric cancer and gastric cancer cell lines [85, 90]. Several studies have shown that gastric CSCs lie within the EpCAM+ population, with the EpCAM− population unable to form tumours in mouse models or tumour spheres [75, 76]. However, other, more specific markers are needed in addition to EpCAM, as the majority of gastric cancer cells are EpCAM-positive.
CD49f, a subunit of laminin receptors, has been used to isolate CSCs in prostate, breast, brain, and colon cancer [74]. Fukamachi et al. [74] demonstrated CSC properties of self-renewal, heterogeneous lineage, and chemotherapy resistance in the CD49f-selected cells from primary gastric cancer mouse xenografts. Further studies are needed to confirm CD49f stem cell properties.
CD54 [also known as intercellular adhesion molecule 1 (ICAM-1)] is an adhesion molecule essential for the arrest and transmigration of leukocytes out of blood vessels, and is widely expressed on immune, stromal, and malignant cells [91]. Decreased CD54 expression on resected gastric cancer is associated with poorer prognosis and increased risk of lymphatic spread [92]. CD44+/54+ cells isolated from primary gastric cancers and peripheral blood samples demonstrated superior tumorigenicity, multiple lineage capability, and self-renewal compared to CD44− or CD54− cells, suggestive of a CSC population in both the primary tumour and the circulation [77].
CD90 is expressed in bone marrow-derived mesenchymal stem cells, hematopoietic stem cells, and keratinocytic stem cells, and has been used to identify CSC populations in liver, breast, and brain cancer [93]. CD90+ cells isolated from patient-derived gastric cancer xenografts demonstrated self-renewal and a heterogeneous lineage [93]. CSCs obtained by preconditioning a gastric cancer cell line with chemotherapy displayed increased expression of CD90 as well as bonafide CSC markers [41].
CD71 (also known as the transferrin receptor) is a membrane protein highly expressed on myocytes, keratinocytes, hepatocytes, pancreatic cells, and erythroid precursors, with a physiological role in mediating the uptake of transferrin-iron complexes. CD71 has been proposed as a negative selection marker, with the CD71-negative subpopulation of a gastric cancer cell line displaying chemoresistance, self-renewal, heterogeneous lineage, and increased tumorigenicity in mouse models [94].
Finally, several transcription factors, including Sox2, Oct4, and Nanog are expressed on gastric stem cells and have been proposed as potential CSC markers. Gastric CSCs enriched by the side population assay or spheroid formation have higher expression of Sox2, Oct4, and Nanog than parental cells [12]. As discussed above, however, studies evaluating the association between clinicopathological variables with immunohistochemical expression of Sox2 in resected gastric cancer have shown conflicting results [58, 59, 62, 95]. Similarly, although some studies have shown poorer prognosis associated with Oct4 expression in resected gastric cancer [96, 97], another large patient series found the opposite result [60].
Clinical implications of gastric cancer stem cells
Gastric CSC marker expression and patient prognosis
CSC marker expression in cancer tissue is emerging as a clinically relevant prognostic biomarker in the management of gastric cancer. Most studies have shown a correlation between advanced pathological features, such as tumour size, invasion, and metastatic spread, and expression of CSC markers. In addition, CD44 and CD133 expression was found to be an independent predictor of lower rates of disease-free survival (in resected gastric cancer) and overall survival (see Table 3). These findings support the preclinical evidence of CD44 and CD133 as CSC markers, as patients with tumours expressing these markers would be expected to have a poorer prognosis due to the CSC traits of chemo-radioresistance, increased tumorigenicity, and metastatic potential.
CD44 is expressed on up to 80 % of primary gastric cancer resection specimens [98] and is associated with more advanced clinicopathological features and poorer prognosis (Table 3). A meta-analysis of 18 studies examining CD44 expression in gastric cancer—albeit limited by significant methodological flaws, including a lack of qualitative analysis of included studies and considerable heterogeneity in pooled results—found statistically significant associations with advanced tumour stage [pooled odds ratio (OR) = 2.05, 95 % confidence interval (CI) 1.12–3.75, P = 0.02], tumor size (pooled OR = 1.42, 95 % CI 1.08–1.87, P = 0.01), and lymph node (LN) metastasis (pooled OR = 1.50, 95 % CI 1.14–1.98, P = 0.004) [99]. Although four studies have shown CD44+ expression to be an independent predictor of survival, it is important to note that the two largest case series did not show an impact of CD44 expression on overall survival [100, 101]. The heterogeneity in results is likely due to variation in experimental procedures and patient populations. A full table summarising all studies evaluating CD44 expression in gastric cancer is included in the supplementary materials (Supplementary Table 2).
Despite the contradictory preclinical data, the role of CD133 as a CSC marker is supported by numerous immunohistochemical studies in resected primary gastric cancer, showing a consistent association with numerous high-risk clinicopathological features and an independent correlation with poorer disease-free and overall survival (Table 3; Supplementary Table 2). A recent meta-analysis found strong evidence that CD133 expression in resected gastric cancer was associated with poorer 5-year overall survival (OR = 0.2, 95 % CI 0.14–0.29, p < 0.00001), although it should be noted that all included studies were conducted in Asian populations, limiting the applicability to Western populations [102]. Furthermore, another recent study, which detected circulating CSCs using CD133 and ABCG2 as markers, found that the presence of peripheral blood CD133+ cells correlated with poorer prognosis, and that passage of isolated CD133+/ABCG2+ cells was possible in mouse models, showing self-renewal, heterogeneous lineage, and increased tumorigenicity [103].
CD44 variant expression appears to be more specific for malignant tissue. Expression of CD44 variants v5, v6, and v9, in resected gastric cancer is associated with adverse clinical outcomes, including worse overall survival, more advanced tumours, and lymphovascular invasion (Table 4). A meta-analysis found that CD44v6 expression was related to LN metastasis (pooled OR = 2.26, 95 % CI 1.40–3.64, P = 0.0008), lymphatic invasion (pooled OR = 1.45, 95 % CI 1.05–2.01, P = 0.02), and venous invasion (pooled OR = 1.62, 95 % CI 1.20–2.18, P = 0.001), but not tumour stage (pooled OR = 0.68, 95 % CI 0.36–1.28, P = 0.23) [99].
ALDH1 expression has been shown to be associated with poor prognostic clinicopathological features in resected primary gastric cancer, although it is not significantly associated with poorer survival [83].
Targeting CSCs in gastric cancer
The CSC model has important clinical implications for cancer treatment. There is strong evidence that CSCs are resistant to traditional chemotherapy and radiotherapy, and are enriched in the residual tumour after such treatment [11, 78, 104, 105]. The CSCs subsequently renew the tumour bulk by developing treatment-resistant clones. Consequently, a specific and efficacious CSC-targeted therapy is needed in order to completely eliminate the cancer. These targeted treatments should be administered in conjunction with conventional chemotherapy/radiotherapy as a means to reduce the tumour bulk and minimise the risk of differentiated cancer cells acquiring CSC-like properties [2].
Targeting cancer stem cell surface markers
One proposed method of CSC-specific treatment is the use of drugs targeted at CSC surface markers. As discussed above, there are significant challenges with this approach given the widespread expression of these markers on non-malignant tissue and the rarity of CSCs in the tumour. Although there is promising data emerging from the preclinical setting in the targeting of CD44, CD133, EpCAM, and CD90 (discussed below), the largest hurdle will be demonstrating safety and efficacy in vivo.
Methodologies targeting CD44 include anti-CD44 monoclonal antibodies [106] and anti-CD44 antibody or aptamer-labelled liposomes [107, 108]. The CD44 ligand, hyaluronic acid, has also been used to label nanocarriers and conjugates, with demonstrated efficacy in reducing CD44+ cells in pancreatic [109] and gastric cancer [110, 111]. Although these studies have shown promise in reducing CSC populations, the clinical utility of these agents may be limited by off-target toxicities [112, 113].
Similarly, CD133 has been successfully targeted in preclinical models by anti-CD133 antibody-cytotoxic conjugates in breast [114], ovarian [115], hepatocellular, and gastric cancer [116]. Smith et al. [116] developed a CD133-cytotoxic conjugate that inhibited the growth of gastric cancer cell lines in vitro.
The anti-EpCAM antibody MT201 has shown tumour suppression properties in preclinical studies in prostate and colon cancer, and has advanced to human trials [116, 117]. A phase I study demonstrated reasonable tolerability in combination with chemotherapy in heavily pretreated breast cancer, with further studies evaluating efficacy underway [118].
It may also be possible to reduce the CSC population through indirect targeting. Jiang et al. [93] noted that candidate CSC marker CD90 correlated with HER2 expression in gastric cancer. While chemotherapy enriched the CD90+ population in a primary cancer culture, a combination of chemotherapy and anti-HER2 treatment (trastuzumab) significantly reduced the CD90+ population and prevented tumour growth [93]. The underlying mechanism driving this result remains unclear, but is an interesting hypothesis to explain why some breast cancer patients with normal HER2 gene expression benefit from trastuzumab [119].
Targeting the cancer stem cell signalling pathways
CSCs are formed as a result of aberrations in important normal stem cell signalling pathways, such as Hedgehog (HH), Notch, and Wnt [13], which have been shown to be important potential targets for treating CSCs [120].
The Wnt/β-catenin pathway plays a physiological role in balancing the proliferation, differentiation, and “stemness” of cells, with over-activation leading to tumorigenesis [121]. It is an important pathway in the regulation of CSCs, and many of the cell surface markers discussed above, including CD44, CD24, and EpCAM, are Wnt targets [122]. Blockage of the Wnt pathways reduces the self-renewal capacity of gastric cancer tumour spheres [123]. One study demonstrated that gastric cancer cells over-expressing Wnt-1 resulted in larger mouse xenograft tumours compared to those with controls cells, with increased expression of CSC markers such as CD44 [124]. When salinomycin was used to suppress Wnt and β-catenin expression, the tumours were smaller, with reduced CSC populations [124]. Another group showed that the disruption of Wnt signalling in CD44+ selected gastric cancer cells using a Wnt-1 antagonist (Dickkopf-1) delivered by adenovirus serotype 5 served to inhibit cancer cell survival, colony formation, and invasion [125]. These agents are awaiting clinical validation.
Aberrant activation of the HH pathway causes neoplastic transformation in a variety of tumours, including gastric cancer [126]. HH signalling maintains the CSC phenotype, and in vitro targeting of the HH pathway reduces the tumorigenicity and invasive capability of gastric cancer spheroids [104] and reverses chemoresistance [127]. Yoon et al. [104] retrospectively performed immunohistochemistry on gastric cancer samples from a negative randomised phase II trial examining the addition of an HH inhibitor (vismodegib) to chemotherapy in gastric cancer, and found improved survival in patients expressing CSC markers (CD44). This exciting finding is the first evidence of CSC expression as a predictive biomarker in gastric cancer, and demonstrates the immediate clinical applicability of targeting CSC pathways as an adjunct to chemotherapy.
Notch signalling has an important role in gastric epithelial stem cell homeostasis, and has been implicated in gastric cancer tumorigenesis [128–130]. Gamma-secretase inhibitors that block the Notch pathway act to reduce CSC markers and cancer growth [131]. They are currently in early clinical trials, but may be limited by toxicity due to their non-specific activity.
Conclusions
Gastric cancer continues to be a highly lethal malignancy, despite the use of multimodal treatment approaches. Strong preclinical and clinical evidence supports the existence of gastric CSCs. CSCs are a small population of tumours cells that, enriched by chemotherapy, provide a source for the reconstitution and spread of the tumour. The failure of conventional treatments to achieve a significant increase in survival rates despite improvements in tumour response can thus be explained by the CSC model.
Gastric CSCs have important clinical ramifications. Expression of CSC markers has been shown to be a clinically relevant biomarker in resected gastric cancer. The cancer stem cell model also provides a new paradigm for managing patients with gastric cancer. Preclinical studies have shown the value of targeting validated and experimental CSC pathways and markers to reduce their stem cell-like characteristics, thus enabling a more complete treatment of gastric cancer. We await the results of further studies to evaluate the efficacy and safety of incorporating CSC treatments into clinical care.
References
Torre LA, Bray F, Siegel RL, et al. Global cancer statistics, 2012. CA Cancer J Clin. 2015;65(2):87–108.
Vermeulen L, de Sousa e Melo F, Richel DJ, et al. The developing cancer stem-cell model: clinical challenges and opportunities. Lancet Oncol. 2012;13(2):e83–9.
Dewi DL, Ishii H, Kano Y, et al. Cancer stem cell theory in gastrointestinal malignancies: recent progress and upcoming challenges. J Gastroenterol. 2011;46(10):1145–57.
Ding L, Raphael BJ, Chen F, et al. Advances for studying clonal evolution in cancer. Cancer Lett. 2013;340(2):212–9.
O’Connor ML, Xiang D, Shigdar S, et al. Cancer stem cells: a contentious hypothesis now moving forward. Cancer Lett. 2014;344(2):180–7.
Reya T, Morrison SJ, Clarke MF, et al. Stem cells, cancer, and cancer stem cells. Nature. 2001;414(6859):105–11.
Vermeulen L, De Sousa EMF, van der Heijden M, et al. Wnt activity defines colon cancer stem cells and is regulated by the microenvironment. Nat Cell Biol. 2010;12(5):468–76.
Liu S, Ginestier C, Ou SJ, et al. Breast cancer stem cells are regulated by mesenchymal stem cells through cytokine networks. Cancer Res. 2011;71(2):614–24.
Notta F, Mullighan CG, Wang JC, et al. Evolution of human BCRABL1 lymphoblastic leukaemia-initiating cells. Nature. 2011;469(7330):362–7.
Shackleton M, Quintana E, Fearon ER, et al. Heterogeneity in cancer: cancer stem cells versus clonal evolution. Cell. 2009;138(5):822–9.
Takaishi S, Okumura T, Tu S, et al. Identification of gastric cancer stem cells using the cell surface marker CD44. Stem Cells. 2009;27(5):1006–20.
Liu J, Ma L, Xu J, et al. Spheroid body-forming cells in the human gastric cancer cell line MKN-45 possess cancer stem cell properties. Int J Oncol. 2013;42(2):453–9.
Xu G, Shen J, Ou Yang X, et al. Cancer stem cells: the ‘heartbeat’ of gastric cancer. J Gastroenterol. 2013;48(7):781–97.
Bonnet D, Dick JE. Human acute myeloid leukemia is organized as a hierarchy that originates from a primitive hematopoietic cell. Nat Med. 1997;3(7):730–7.
Al-Hajj M, Wicha MS, Benito-Hernandez A, et al. Prospective identification of tumorigenic breast cancer cells. PNAS. 2003;100(7):3983–8.
Collins AT, Berry PA, Hyde C, et al. Prospective identification of tumorigenic prostate cancer stem cells. Cancer Res. 2005;65(23):10946–51.
Hermann PC, Huber SL, Herrler T, et al. Distinct populations of cancer stem cells determine tumor growth and metastatic activity in human pancreatic cancer. Cell Stem Cell. 2007;1(3):313–23.
Li C, Heidt DG, Dalerba P, et al. Identification of pancreatic cancer stem cells. Cancer Res. 2007;67(3):1030–7.
Fang D, Nguyen TK, Leishear K, et al. A tumorigenic subpopulation with stem cell properties in melanomas. Cancer Res. 2005;65(20):9328–37.
O’Brien CA, Pollett A, Gallinger S, et al. A human colon cancer cell capable of initiating tumour growth in immunodeficient mice. Nature. 2007;445(7123):106–10.
Ricci-Vitiani L, Lombardi DG, Pilozzi E, et al. Identification and expansion of human colon-cancer-initiating cells. Nature. 2007;445(7123):111–5.
Singh SK, Hawkins C, Clarke ID, et al. Identification of human brain tumour initiating cells. Nature. 2004;432(7015):396–401.
Singh SK, Clarke ID, Terasaki M, et al. Identification of a cancer stem cell in human brain tumors. Cancer Res. 2003;63(18):5821–8.
Ma S, Chan KW, Hu L, et al. Identification and characterization of tumorigenic liver cancer stem/progenitor cells. Gastroenterology. 2007;132(7):2542–56.
Chen J, Li Y, Yu TS, et al. A restricted cell population propagates glioblastoma growth after chemotherapy. Nature. 2012;488(7412):522–6.
Clarke MF, Dick JE, Dirks PB, et al. Cancer stem cells–perspectives on current status and future directions: AACR Workshop on cancer stem cells. Cancer Res. 2006;66(19):9339–44.
Takaishi S, Okumura T, Wang TC. Gastric cancer stem cells. J Clin Oncol. 2008;26(17):2876–82.
Sampieri K, Fodde R. Cancer stem cells and metastasis. Sem Can Biol. 2012;22(3):187–93.
Pang R, Law WL, Chu AC, et al. A subpopulation of CD26+ cancer stem cells with metastatic capacity in human colorectal cancer. Cell Stem Cell. 2010;6(6):603–15.
Croker AK, Goodale D, Chu J, et al. High aldehyde dehydrogenase and expression of cancer stem cell markers selects for breast cancer cells with enhanced malignant and metastatic ability. J Cell Mol Med. 2009;13(8b):2236–52.
Dieter SM, Ball CR, Hoffmann CM, et al. Distinct types of tumor-initiating cells form human colon cancer tumors and metastases. Cell Stem Cell. 2011;9(4):357–65.
Mayer B, Jauch KW, Gunthert U, et al. De-novo expression of CD44 and survival in gastric cancer. Lancet. 1993;342(8878):1019–22.
Chen S, Hou JH, Feng XY, et al. Clinicopathologic significance of putative stem cell marker, CD44 and CD133, in human gastric carcinoma. J Surg Oncol. 2013;107(8):799–806.
Meng F, Wu G. The rejuvenated scenario of epithelial-mesenchymal transition (EMT) and cancer metastasis. Cancer Metastasis Rev. 2012;31(3–4):455–67.
Gupta PB, Chaffer CL, Weinberg RA. Cancer stem cells: mirage or reality? Nat Med. 2009;15(9):1010–2.
Mani SA, Guo W, Liao MJ, et al. The epithelial-mesenchymal transition generates cells with properties of stem cells. Cell. 2008;133(4):704–15.
Morel AP, Lievre M, Thomas C, et al. Generation of breast cancer stem cells through epithelial-mesenchymal transition. PLoS One. 2008;3(8):e2888.
Tinhofer I, Saki M, Niehr F, et al. Cancer stem cell characteristics of circulating tumor cells. Int J Radiat Biol. 2014;90(8):622–7.
Li M, Zhang B, Zhang Z, et al. Stem cell-like circulating tumor cells indicate poor prognosis in gastric cancer. BioMed Res Int. 2014;2014:981261.
Ryu HS, do Park J, Kim HH, et al. Combination of epithelial-mesenchymal transition and cancer stem cell-like phenotypes has independent prognostic value in gastric cancer. Hum Pathol. 2012;43(4):520–8.
Xue Z, Yan H, Li J, et al. Identification of cancer stem cells in vincristine preconditioned SGC7901 gastric cancer cell line. J Cell Biochem. 2012;113(1):302–12.
Kelly PN, Dakic A, Adams JM, et al. Tumor growth need not be driven by rare cancer stem cells. Science. 2007;317(5836):337.
Marx J. Molecular biology. Cancer’s perpetual source? Science. 2007;317(5841):1029–31.
Yang L, Ping YF, Yu X, et al. Gastric cancer stem-like cells possess higher capability of invasion and metastasis in association with a mesenchymal transition phenotype. Cancer Lett. 2011;310(1):46–52.
Zhou S, Schuetz JD, Bunting KD, et al. The ABC transporter Bcrp1/ABCG2 is expressed in a wide variety of stem cells and is a molecular determinant of the side-population phenotype. Nat Med. 2001;7(9):1028–34.
Golebiewska A, Brons NH, Bjerkvig R, et al. Critical appraisal of the side population assay in stem cell and cancer stem cell research. Cell Stem Cell. 2011;8(2):136–47.
Zhang H, Xi H, Cai A, et al. Not all side population cells contain cancer stem-like cells in human gastric cancer cell lines. Dig Dis Sci. 2013;58(1):132–9.
Nishii T, Yashiro M, Shinto O, et al. Cancer stem cell-like SP cells have a high adhesion ability to the peritoneum in gastric carcinoma. Cancer Sci. 2009;100(8):1397–402.
Fukuda K, Saikawa Y, Ohashi M, et al. Tumor initiating potential of side population cells in human gastric cancer. Int J Oncol. 2009;34(5):1201–7.
She JJ, Zhang PG, Wang X, et al. Side population cells isolated from KATO III human gastric cancer cell line have cancer stem cell-like characteristics. World J Gastroenterol. 2012;18(33):4610–7.
Burkert J, Otto WR, Wright NA. Side populations of gastrointestinal cancers are not enriched in stem cells. J Pathol. 2008;214(5):564–73.
Bjerknes M, Cheng H. Multipotential stem cells in adult mouse gastric epithelium. Am J Physiol Gastrointest Liver Physiol. 2002;283(3):G767–77.
Wu C, Xie Y, Gao F, et al. Lgr5 expression as stem cell marker in human gastric gland and its relatedness with other putative cancer stem cell markers. Gene. 2013;525(1):18–25.
Barker N, Huch M, Kujala P, et al. Lgr5(+ve) stem cells drive self-renewal in the stomach and build long-lived gastric units in vitro. Cell Stem Cell. 2010;6(1):25–36.
Qiao XT, Ziel JW, McKimpson W, et al. Prospective identification of a multilineage progenitor in murine stomach epithelium. Gastroenterology. 2007;133(6):1989–98.
Arnold K, Sarkar A, Yram MA, et al. Sox2(+) adult stem and progenitor cells are important for tissue regeneration and survival of mice. Cell Stem Cell. 2011;9(4):317–29.
Stange DE, Koo BK, Huch M, et al. Differentiated Troy+ chief cells act as reserve stem cells to generate all lineages of the stomach epithelium. Cell. 2013;155(2):357–68.
Wang S, Tie J, Wang R, et al. SOX2, a predictor of survival in gastric cancer, inhibits cell proliferation and metastasis by regulating PTEN. Cancer Lett. 2015;358(2):210–9.
Li XL, Eishi Y, Bai YQ, et al. Expression of the SRY-related HMG box protein SOX2 in human gastric carcinoma. Int J Oncol. 2004;24(2):257–63.
Matsuoka J, Yashiro M, Sakurai K, et al. Role of the stemness factors sox2, oct3/4, and nanog in gastric carcinoma. J Surg Res. 2012;174(1):130–5.
Hutz K, Mejias-Luque R, Farsakova K, et al. The stem cell factor SOX2 regulates the tumorigenic potential in human gastric cancer cells. Carcinogenesis. 2014;35(4):942–50.
Otsubo T, Akiyama Y, Yanagihara K, et al. SOX2 is frequently downregulated in gastric cancers and inhibits cell growth through cell-cycle arrest and apoptosis. Br J Cancer. 2008;98(4):824–31.
Giannakis M, Stappenbeck TS, Mills JC, et al. Molecular properties of adult mouse gastric and intestinal epithelial progenitors in their niches. J Biol Chem. 2006;281(16):11292–300.
Okumura T, Ericksen RE, Takaishi S, et al. K-ras mutation targeted to gastric tissue progenitor cells results in chronic inflammation, an altered microenvironment, and progression to intraepithelial neoplasia. Cancer Res. 2010;70(21):8435–45.
Bessede E, Staedel C, Acuna Amador LA, et al. Helicobacter pylori generates cells with cancer stem cell properties via epithelial-mesenchymal transition-like changes. Oncogene. 2014;33(32):4123–31.
Houghton J, Stoicov C, Nomura S, et al. Gastric cancer originating from bone marrow-derived cells. Science. 2004;306(5701):1568–71.
Okumura T, Wang SS, Takaishi S, et al. Identification of a bone marrow-derived mesenchymal progenitor cell subset that can contribute to the gastric epithelium. Lab Invest. 2009;89(12):1410–22.
Varon C, Dubus P, Mazurier F, et al. Helicobacter pylori infection recruits bone marrow-derived cells that participate in gastric preneoplasia in mice. Gastroenterology. 2012;142(2):281–91.
Bessede E, Dubus P, Megraud F, et al. Helicobacter pylori infection and stem cells at the origin of gastric cancer. Oncogene. 2015;34(20):2547–55.
Ponta H, Sherman L, Herrlich PA. CD44: from adhesion molecules to signalling regulators. Nat Rev Mol Cell Biol. 2003;4(1):33–45.
Olsson E, Honeth G, Bendahl PO, et al. CD44 isoforms are heterogeneously expressed in breast cancer and correlate with tumor subtypes and cancer stem cell markers. BMC Cancer. 2011;11:418.
Ishimoto T, Nagano O, Yae T, et al. CD44 variant regulates redox status in cancer cells by stabilizing the xCT subunit of system xc(−) and thereby promotes tumor growth. Cancer Cell. 2011;19(3):387–400.
Rocco A, Liguori E, Pirozzi G, et al. CD133 and CD44 cell surface markers do not identify cancer stem cells in primary human gastric tumors. J Cell Physiol. 2012;227(6):2686–93.
Fukamachi H, Seol HS, Shimada S, et al. CD49f(high) cells retain sphere-forming and tumor-initiating activities in human gastric tumors. PLoS One. 2013;8(8):e72438.
Han ME, Jeon TY, Hwang SH, et al. Cancer spheres from gastric cancer patients provide an ideal model system for cancer stem cell research. Cell Mol Life Sci. 2011;68(21):3589–605.
Lau WM, Teng E, Chong HS, et al. CD44v8-10 is a cancer-specific marker for gastric cancer stem cells. Cancer Res. 2014;74(9):2630–41.
Chen T, Yang K, Yu J, et al. Identification and expansion of cancer stem cells in tumor tissues and peripheral blood derived from gastric adenocarcinoma patients. Cell Res. 2012;22(1):248–58.
Zhang C, Li C, He F, et al. Identification of CD44+ CD24+ gastric cancer stem cells. J Cancer Res Clin. 2011;137(11):1679–86.
Yin AH, Miraglia S, Zanjani ED, et al. AC133, a novel marker for human hematopoietic stem and progenitor cells. Blood. 1997;90(12):5002–12.
Mizrak D, Brittan M, Alison M. CD133: molecule of the moment. J Pathol. 2008;214(1):3–9.
Irollo E, Pirozzi G. CD133: to be or not to be, is this the real question? Am J Transl Res. 2013;5(6):563–81.
Kemper K, Sprick MR, de Bree M, et al. The AC133 epitope, but not the CD133 protein, is lost upon cancer stem cell differentiation. Cancer Res. 2010;70(2):719–29.
Wakamatsu Y, Sakamoto N, Oo HZ, et al. Expression of cancer stem cell markers ALDH1, CD44 and CD133 in primary tumor and lymph node metastasis of gastric cancer. Pathol Int. 2012;62(2):112–9.
Muzio G, Maggiora M, Paiuzzi E, et al. Aldehyde dehydrogenases and cell proliferation. Free Radic Biol Med. 2012;52(4):735–46.
Nishikawa S, Konno M, Hamabe A, et al. Aldehyde dehydrogenase high gastric cancer stem cells are resistant to chemotherapy. Int J Oncol. 2013;42(4):1437–42.
Katsuno Y, Ehata S, Yashiro M, et al. Coordinated expression of REG4 and aldehyde dehydrogenase 1 regulating tumourigenic capacity of diffuse-type gastric carcinoma-initiating cells is inhibited by TGF-beta. J Pathol. 2012;228(3):391–404.
Fujikuni N, Yamamoto H, Tanabe K, et al. Hypoxia-mediated CD24 expression is correlated with gastric cancer aggressiveness by promoting cell migration and invasion. Cancer Sci. 2014;105(11):1411–20.
Chou YY, Jeng YM, Lee TT, et al. Cytoplasmic CD24 expression is a novel prognostic factor in diffuse-type gastric adenocarcinoma. Ann Surg Oncol. 2007;14(10):2748–58.
Imano M, Itoh T, Satou T, et al. High expression of epithelial cellular adhesion molecule in peritoneal metastasis of gastric cancer. Target Oncol. 2013;8(4):231–5.
Wenqi D, Li W, Shanshan C, et al. EpCAM is overexpressed in gastric cancer and its downregulation suppresses proliferation of gastric cancer. J Cancer Res Clin Oncol. 2009;135(9):1277–85.
Schildberg FA, Wojtalla A, Siegmund SV, et al. Murine hepatic stellate cells veto CD8 T cell activation by a CD54-dependent mechanism. Hepatology. 2011;54(1):262–72.
Yashiro M, Sunami T, Hirakawa K. CD54 expression is predictive for lymphatic spread in human gastric carcinoma. Dig Dis Sci. 2005;50(12):2224–30.
Jiang J, Zhang Y, Chuai S, et al. Trastuzumab (herceptin) targets gastric cancer stem cells characterized by CD90 phenotype. Oncogene. 2012;31(6):671–82.
Ohkuma M, Haraguchi N, Ishii H, et al. Absence of CD71 transferrin receptor characterizes human gastric adenosquamous carcinoma stem cells. Ann Surg Oncol. 2012;19(4):1357–64.
Lin S, Qi W, Han K, et al. Prognostic value of SOX2 in digestive tumors: a meta-analysis. Hepatol Gastroenterol. 2014;61(133):1274–8.
Li N, Deng W, Ma J, et al. Prognostic evaluation of Nanog, Oct4, Sox2, PCNA, Ki67 and E-cadherin expression in gastric cancer. Med Oncol. 2015;32(1):433.
Kong D, Su G, Zha L, et al. Coexpression of HMGA2 and Oct4 predicts an unfavorable prognosis in human gastric cancer. Med Oncol. 2014;31(8):130.
Wang T, Ong CW, Shi J, et al. Sequential expression of putative stem cell markers in gastric carcinogenesis. Br J Cancer. 2011;105(5):658–65.
Wang W, Dong LP, Zhang N, et al. Role of cancer stem cell marker CD44 in gastric cancer: a meta-analysis. Int J Clin Exp Med. 2014;7(12):5059–66.
Liu YJ, Yan PS, Li J, et al. Expression and significance of CD44 s, CD44v6, and nm23 mRNA in human cancer. World J Gastroenterol. 2005;11(42):6601–6.
Kim JY, Bae BN, Kim KS, et al. Osteopontin, CD44, and NFkappaB expression in gastric adenocarcinoma. Cancer Res Treat. 2009;41(1):29–35.
Wen L, Chen XZ, Yang K, et al. Prognostic value of cancer stem cell marker CD133 expression in gastric cancer: a systematic review. PLoS One. 2013;8(3):e59154.
Xia P, Song CL, Liu JF, et al. Prognostic value of circulating CD133(+) cells in patients with gastric cancer. Cell Prolif. 2015;48(3):311–7.
Yoon C, do Park J, Schmidt B, et al. CD44 expression denotes a subpopulation of gastric cancer cells in which Hedgehog signaling promotes chemotherapy resistance. Clin Cancer Res. 2014;20(15):3974–88.
Xu ZY, Tang JN, Xie HX, et al. 5-Fluorouracil chemotherapy of gastric cancer generates residual cells with properties of cancer stem cells. Int J Biol Sci. 2015;11(3):284–94.
Du YR, Chen Y, Gao Y, et al. Effects and mechanisms of anti-CD44 monoclonal antibody A3D8 on proliferation and apoptosis of sphere-forming cells with stemness from human ovarian cancer. Int J Gynecol Cancer. 2013;23(8):1367–75.
Alshaer W, Hillaireau H, Vergnaud J, et al. Functionalizing liposomes with anti-CD44 Aptamer for selective targeting of cancer cells. Bioconjug Chem. 2015;26(7):1307–13.
Wang L, Su W, Liu Z, et al. CD44 antibody-targeted liposomal nanoparticles for molecular imaging and therapy of hepatocellular carcinoma. Biomaterials. 2012;33(20):5107–14.
Noh I, Kim HO, Choi J, et al. Co-delivery of paclitaxel and gemcitabine via CD44-targeting nanocarriers as a prodrug with synergistic antitumor activity against human biliary cancer. Biomaterials. 2015;53:763–74.
Yao HJ, Zhang YG, Sun L, et al. The effect of hyaluronic acid functionalized carbon nanotubes loaded with salinomycin on gastric cancer stem cells. Biomaterials. 2014;35(33):9208–23.
Serafino A, Zonfrillo M, Andreola F, et al. CD44-targeting for antitumor drug delivery: a new SN-38-hyaluronan bioconjugate for locoregional treatment of peritoneal carcinomatosis. Curr Cancer Drug Targets. 2011;11(5):572–85.
Tanaka Y, Makiyama Y, Mitsui Y. Anti-CD44 monoclonal antibody (IM7) induces murine systemic shock mediated by platelet activating factor. J Autoimmun. 2002;18(1):9–15.
Vugts DJ, Heuveling DA, Stigter-van Walsum M, et al. Preclinical evaluation of 89Zr-labeled anti-CD44 monoclonal antibody RG7356 in mice and cynomolgus monkeys: prelude to Phase 1 clinical studies. MAbs. 2014;6(2):567–75.
Swaminathan SK, Roger E, Toti U, et al. CD133-targeted paclitaxel delivery inhibits local tumor recurrence in a mouse model of breast cancer. J Control Rel. 2013;171(3):280–7.
Skubitz AP, Taras EP, Boylan KL, et al. Targeting CD133 in an in vivo ovarian cancer model reduces ovarian cancer progression. Gynecol Oncol. 2013;130(3):579–87.
Smith LM, Nesterova A, Ryan MC, et al. CD133/prominin-1 is a potential therapeutic target for antibody-drug conjugates in hepatocellular and gastric cancers. Br J Cancer. 2008;99(1):100–9.
Ammons WS, Bauer RJ, Horwitz AH, et al. In vitro and in vivo pharmacology and pharmacokinetics of a human engineered monoclonal antibody to epithelial cell adhesion molecule. Neoplasia. 2003;5(2):146–54.
Schmidt M, Ruttinger D, Sebastian M, et al. Phase IB study of the EpCAM antibody adecatumumab combined with docetaxel in patients with EpCAM-positive relapsed or refractory advanced-stage breast cancer. Ann Oncol. 2012;23(9):2306–13.
Paik S, Kim C, Wolmark N. HER2 status and benefit from adjuvant trastuzumab in breast cancer. N Engl J Med. 2008;358(13):1409–11.
Wu WK, Cho CH, Lee CW, et al. Dysregulation of cellular signaling in gastric cancer. Cancer Lett. 2010;295(2):144–53.
Kanwar SS, Yu Y, Nautiyal J, et al. The Wnt/beta-catenin pathway regulates growth and maintenance of colonospheres. Mol Cancer. 2010;9:212.
Takahashi-Yanaga F, Kahn M. Targeting Wnt signaling: can we safely eradicate cancer stem cells? Clin Cancer Res. 2010;16(12):3153–62.
Cai C, Zhu X. The Wnt/beta-catenin pathway regulates self-renewal of cancer stem-like cells in human gastric cancer. Mol Med Rep. 2012;5(5):1191–6.
Mao J, Fan S, Ma W, et al. Roles of Wnt/beta-catenin signaling in the gastric cancer stem cells proliferation and salinomycin treatment. Cell Death Dis. 2014;5:e1039.
Wang B, Liu J, Ma LN, et al. Chimeric 5/35 adenovirus-mediated Dickkopf-1 overexpression suppressed tumorigenicity of CD44(+) gastric cancer cells via attenuating Wnt signaling. J Gastroenterol. 2013;48(7):798–808.
Berman DM, Karhadkar SS, Maitra A, et al. Widespread requirement for Hedgehog ligand stimulation in growth of digestive tract tumours. Nature. 2003;425(6960):846–51.
Song Z, Yue W, Wei B, et al. Sonic hedgehog pathway is essential for maintenance of cancer stem-like cells in human gastric cancer. PLoS One. 2011;6(3):e17687.
Kim TH, Shivdasani RA. Notch signaling in stomach epithelial stem cell homeostasis. J Exp Med. 2011;208(4):677–88.
Yeh TS, Wu CW, Hsu KW, et al. The activated Notch1 signal pathway is associated with gastric cancer progression through cyclooxygenase-2. Cancer Res. 2009;69(12):5039–48.
Brzozowa M, Mielanczyk L, Michalski M, et al. Role of Notch signaling pathway in gastric cancer pathogenesis. Contemp Oncol. 2013;17(1):1–5.
Purow B. Notch inhibition as a promising new approach to cancer therapy. Adv Exp Med Biol. 2012;727:305–19.
Botchkina G. Colon cancer stem cells–from basic to clinical application. Cancer Lett. 2013;338(1):127–40.
Zhan HX, Xu JW, Wu D, et al. Pancreatic cancer stem cells: new insight into a stubborn disease. Cancer Lett. 2015;357(2):429–37.
Carrasco E, Alvarez PJ, Prados J, et al. Cancer stem cells and their implication in breast cancer. Eur J Clin Invest. 2014;44(7):678–87.
Jackson M, Hassiotou F, Nowak A. Glioblastoma stem-like cells: at the root of tumor recurrence and a therapeutic target. Carcinogenesis. 2015;36(2):177–85.
Lundin A, Driscoll B. Lung cancer stem cells: progress and prospects. Cancer Lett. 2013;338(1):89–93.
Lang D, Mascarenhas JB, Shea CR. Melanocytes, melanocyte stem cells, and melanoma stem cells. Clin Dermatol. 2013;31(2):166–78.
Sharpe B, Beresford M, Bowen R, et al. Searching for prostate cancer stem cells: markers and methods. Stem Cell Rev. 2013;9(5):721–30.
Fukamachi H, Shimada S, Ito K, et al. CD133 is a marker of gland-forming cells in gastric tumors and Sox17 is involved in its regulation. Cancer Sci. 2011;102(7):1313–21.
Zhu Y, Yu J, Wang S, et al. Overexpression of CD133 enhances chemoresistance to 5-fluorouracil by activating the PI3K/Akt/p70S6K pathway in gastric cancer cells. Oncol Rep. 2014;32(6):2437–44.
Zhi QM, Chen XH, Ji J, et al. Salinomycin can effectively kill ALDH(high) stem-like cells on gastric cancer. Biomed Pharmacother. 2011;65(7):509–15.
Yu D, Shin HS, Choi G, et al. Proteomic analysis of CD44(+) and CD44(−) gastric cancer cells. Mol Cell Biochem. 2014;396(1–2):213–20.
Hong RL, Lee WJ, Shun CT, et al. Expression of CD44 and its clinical implication in diffuse-type and intestinal-type gastric adenocarcinomas. Oncology. 1995;52(4):334–9.
Ghaffarzadehgan K, Jafarzadeh M, Raziee HR, et al. Expression of cell adhesion molecule CD44 in gastric adenocarcinoma and its prognostic importance. World J Gastroenterol. 2008;14(41):6376–81.
Nosrati A, Naghshvar F, Khanari S. Cancer Stem Cell Markers CD44, CD133 in Primary Gastric Adenocarcinoma. Int J Mol Cell Med. 2014;3(4):279–86.
Lee HH, Seo KJ, An CH, et al. CD133 expression is correlated with chemoresistance and early recurrence of gastric cancer. J Surg Oncol. 2012;106(8):999–1004.
Yu JW, Zhang P, Wu JG, et al. Expressions and clinical significances of CD133 protein and CD133 mRNA in primary lesion of gastric adenocacinoma. J Exp Clin Cancer Res. 2010;29:141.
Zhao P, Li Y, Lu Y. Aberrant expression of CD133 protein correlates with Ki-67 expression and is a prognostic marker in gastric adenocarcinoma. BMC Cancer. 2010;10:218.
Hashimoto K, Aoyagi K, Isobe T, et al. Expression of CD133 in the cytoplasm is associated with cancer progression and poor prognosis in gastric cancer. Gastric Cancer. 2014;17(1):97–106.
Jiang Y, He Y, Li H, et al. Expressions of putative cancer stem cell markers ABCB1, ABCG2, and CD133 are correlated with the degree of differentiation of gastric cancer. Gastric Cancer. 2012;15(4):440–50.
Muller W, Schneiders A, Heider KH, et al. Expression and prognostic value of the CD44 splicing variants v5 and v6 in gastric cancer. J Pathol. 1997;183(2):222–7.
Yamaguchi A, Goi T, Yu J, et al. Expression of CD44v6 in advanced gastric cancer and its relationship to hematogenous metastasis and long-term prognosis. J Surg Oncol. 2002;79(4):230–5.
Okayama H, Kumamoto K, Saitou K, et al. CD44v6, MMP-7 and nuclear Cdx2 are significant biomarkers for prediction of lymph node metastasis in primary gastric cancer. Oncol Rep. 2009;22(4):745–55.
Xin Y, Grace A, Gallagher MM, et al. CD44V6 in gastric carcinoma: a marker of tumor progression. Appl Immunohistochem Mol Morphol. 2001;9(2):138–42.
Chen JQ, Zhan WH, He YL, et al. Expression of heparanase gene, CD44v6, MMP-7 and nm23 protein and their relationship with the invasion and metastasis of gastric carcinomas. World J Gastroenterol. 2004;10(6):776–82.
Kurozumi K, Nishida T, Nakao K, et al. Expression of CD44 variant 6 and lymphatic invasion: importance to lymph node metastasis in gastric cancer. World J Surg. 1998;22(8):853–7 (discussion 7-8).
Yasui W, Kudo Y, Naka K, et al. Expression of CD44 containing variant exon 9 (CD44v9) in gastric adenomas and adenocarcinomas: relation to the proliferation and progression. Int J Oncol. 1998;12(6):1253–8.
Go SI, Ko GH, Lee WS, et al. CD44 variant 9 serves as a poor prognostic marker in early gastric cancer, but not in advanced gastric cancer. Can Res Treat. 2015. doi:10.4143/crt.2014.227.
Hirata K, Suzuki H, Imaeda H, et al. CD44 variant 9 expression in primary early gastric cancer as a predictive marker for recurrence. Br J Cancer. 2013;109(2):379–86.
Yong CS, Ou Yang CM, Chou YH, et al. CD44/CD24 expression in recurrent gastric cancer: a retrospective analysis. BMC Gstroenterol. 2012;12:95.
Cao L, Hu X, Zhang J, Liang P, Zhang Y. CD44(+) CD324(−) expression and prognosis in gastric cancer patients. J Surg Oncol. 2014;110(6):727–33.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Funding
Funding sources include the Cancer Institute New South Wales for the CONCERT-Translational Cancer Research Centre and Illawarra Health and Medical Research Institute, University of Wollongong.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Brungs, D., Aghmesheh, M., Vine, K.L. et al. Gastric cancer stem cells: evidence, potential markers, and clinical implications. J Gastroenterol 51, 313–326 (2016). https://doi.org/10.1007/s00535-015-1125-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00535-015-1125-5