
Abstract
Background
Music may be a safe and effective coping strategy for psychological management. The objectives of this review were to identify the effects of music interventions on anxiety, depression, and quality of life (QoL) among cancer patients receiving chemotherapy.
Methods
Fourteen databases were searched from the inception date to December 2020 to identify eligible randomized controlled trials (RCTs). Gray literature was also examined. The protocol of this systematic review was registered with PROSPERO (registration number: CRD42021223845). Two reviewers independently assessed eligibility, extracted data, and evaluated methodological quality. Meta-analysis was done. Subgroup analysis was conducted for intervention types, the person selecting music, music delivery method, timing, and session duration.
Results
Nine RCTs were identified, among which six were eligible for the meta-analysis. All studies were at a high risk of bias, and the overall quality of evidence was low to very low. The pooled results reveal that music intervention could reduce anxiety (SMD: − 0.29, 95% CI − 0.50 to − 0.08) and improve QoL (SMD: 0.42, 95% CI 0.02 to 0.82). However, it fails to affect depression (p = 0.79). The findings demonstrate no significant difference between patient-selected music and researcher-selected music, recorded music, and live music, while a length of 15–20 min/session and offering immediately before chemotherapy are more effective on anxiety than that of 30–45 min and delivering during chemotherapy.
Conclusions
Music intervention may be a beneficial tool for anxiety reduction and QoL among cancer patients receiving chemotherapy. More high-quality RCTs are needed to ascertain the true impact of those outcomes.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Anxiety and depression are two of the most common psychological symptoms in people diagnosed with cancer in general. The meta-analytical pooled prevalence of syndromal depression and anxiety disorder in cancer patients in oncological and hematological settings was 16.3% (66 studies, 95% CI 13.4–19.5) and 10.3% (16 studies, 95% CI 5.1–17.0), respectively [21]. Krebber et al. [17] conducted a meta-analysis of 211 studies to determine the prevalence of depression in cancer patients. They reported that the pooled prevalence of depression ranged from 8 to 24%. The figures were higher among cancer patients during chemotherapy. According to Nikbahsh et al. [23], the proportions of symptomatic depression and symptomatic anxiety among the patients who received chemotherapy as a single treatment were 66.7% and 77.8%, respectively. Depression and anxiety have an adverse impact on the QoL of individuals with cancer [23].
To alleviate the cancer patients’ anxiety and depression, music intervention was recommended. Emotions aroused by music are recognized by the amygdala and hippocampus [16]. The rhythm and melody of relaxing music act on the peripheral and hippocampus system could reduce cortisol levels [26], contributing positively to the improvement in the psychological disorder [10]. Music intervention is considered mind–body medicine [8], which can improve psychological and physical outcomes in cancer patients [4, 28]. A previous study showed that music could reduce anxiety and depression and improve the QoL for cancer patients during chemotherapy [19]. In terms of methodology, there are currently two types of music interventions in existence, including music therapy in which a trained therapist provides the intervention and music medicine in which the passive listening of recorded music is offered to patients by medical staff [5]. In clinical practice, music intervention can be performed in any setting because it is safe, does not require technologically advanced equipment, and does not interfere with patients’ privacy [8, 15].
There is a lack of systematic review revealing the effect of music intervention on anxiety, depression, and QoL, particularly focusing on adult cancer patients receiving chemotherapy. Thus, this systematic review aims to synthesize the evidence on the effects of music intervention on anxiety, depression, and QoL and to identify the best available evidence concerning the characteristics of music intervention such as duration, number of sessions, and frequency which could be applied on adult cancer patients receiving chemotherapy.
Methods
Information sources and search strategy
This review was conducted according to the updated guideline of the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) 2020 statement [25]. A literature search was performed in December 2020. Two independent reviewers searched the literature in fourteen databases, including The Cochrane Central Register of Controlled Trials (CENTRAL), PubMed, Ovid MEDLINE, PsycINFO, EMBASE, PsycARTICLES, Ovid Nursing Database, Joanna Briggs Institute EBP Database, Global Health, Scopus, British Nursing Index, AMED, and Web of Science. Gray literature was searched on Proquest Dissertations & Theses A&I, ClinicalTrials.gov, Open Grey, and ISRCTN registry. The initial search used subject headings (MESH) that related to neoplasms, drug therapy, music, anxiety, depression, and quality of life. After that, the relevant keywords were searched to identify the potential papers (Appendix).
Inclusion and exclusion criteria
This review included randomized controlled trials (RCTs). The publications included were written in English, with no limitation on publication year, and were full-text articles. The participants in the selected literature were older than 18 years with a diagnosis of any type of cancer receiving chemotherapy.
We included all trials in which music therapy or music medicine combined with standard care were compared with standard care alone. Studies with trials testing the effectiveness of music intervention on anxiety and/or depression and/or QoL were included.
We excluded the studies (1) combining music intervention with other interventions such as mindfulness or yoga, (2) involving animals, (3) the trial for diagnostic purposes, and (4) conference abstracts, study protocol, and ongoing studies without results.
Appraisal of included studies
The two reviewers independently assessed the quality of the studies using the Cochrane Risk of Bias Assessment Tool (ROB2) [14]. The tool includes five domains: randomization process, deviations from intended interventions, missing outcome data, outcome measurement, and selection of the reported result. Each domain is assessed as high risk, low risk, and some concerns by applying the Cochrane criteria for judging the risk of bias. For each study, if all domains were evaluated as low risk, the overall risk of bias was considered to be low. If any of the above domains were considered high risk or the assessment results in multiple domains showed some concerns, the overall risk of bias was considered to be high; otherwise, the overall risk of bias was considered to be having some concerns. The reviewers compared the appraisal results, and disagreements were resolved through consensus between reviewers or through a consultation with a third reviewer.
Study selection and data extraction
All studies retrieved from the databases and gray literature were recorded in EndnoteX9 software. Firstly, the duplicated papers were removed. Then, the studies were screened one by one based on the title and abstract. After this initial screening, the full text of related studies was retrieved and assessed for eligibility.
We extracted data using a standardized form, which was developed according to the present review features. The following information was extracted and recorded: (1) name of first author and year of publication, country; (2) study type; (3) sample size, type of cancer; (4) intervention group and control group; (5) outcome measures, instruments; and (6) results. The information related to music intervention was extracted and consisted of (1) timing of music intervention, (2) duration of a session, (3) intervention delivery schedules, (4) interventionists, (5) music genres, (6) music delivery methods, (7) listening methods, and (8) person selecting the music. The study selection and data extraction processes were independently performed by the two reviewers. Disagreements were resolved through a meeting with a third reviewer.
Data synthesis
The Cochrane Collaboration’s Review Manager (RevMan 5.4.1) [12] was used to generate pooled estimates of effect size. The comparison weighting mean differences (MD) were calculated when outcomes were measured using the same scale, while the standardized mean differences (SMD) were used for those using different scales, with corresponding 95% confidence intervals (CI). The fixed-effect model was used if the chi-square test indicated that there was insignificant heterogeneity (p > 0.10 or I2 ≤ 50%) [14, 30]; otherwise, the random effect model was adopted. The effect size was determined according to the guideline of Cohen [11]. Accordingly, 0.2 was considered a small effect; 0.5, medium; and 0.8, large. To explore the source heterogeneity and robust results, sensitivity analysis was used. Subgroup analyses were also conducted for different types of music interventions (music therapy versus music medicine), the person selecting the music (patient-selected music versus researcher-selected music), intervention delivery methods ( live music versus recorded music), timings of the interventions (before chemotherapy versus during chemotherapy), and length of intervention (15–20 min versus 30–45 min). For incomplete and missing data, the authors of the selected studies were contacted for further information. For those studies that did not provide eligible data for synthesis, descriptive analyses were adopted. Publication bias was not performed due to fewer than ten studies [14].
The Grading of Recommendation Assessment, Development and Evaluation (GRADE), which was developed by Cochrane [29], was used to rate the overall quality of evidence of each outcome. The quality of evidence was classified into four levels high, moderate, low, and very low. Study design, risk of bias, inconsistency, indirectness, imprecision, and reporting bias were considered to assess the confidence of evidence.
Result
Search result
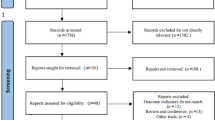
The systematic search yielded 2723 articles. After removing 684 duplicates, 2039 papers were left for titles and abstract screening, which further removed 1849 records that did not meet the inclusion criteria. Then, 190 full-text articles were reviewed, and further 154 studies found not meeting the inclusion criteria were excluded. Subsequently, 27 studies were rejected because of mixed intervention, ongoing study, and not meeting the study design. Finally, nine articles were included in this systematic review, including six studies for meta-analysis (Fig. 1).

PRISMA Flow Diagram
Study characteristics
The studies were published between 2007 and 2020; the studies were conducted in five jurisdictions such as Brazil [19], Germany [7, 27], Italy [8], Taiwan [10, 20], and the USA [9, 13, 22]. The sample size of the studies ranged from 33 to 143. The trials comprised 686 patients, including breast cancer [8, 10, 19] and hematological cancer [7, 9, 27], and the three remaining studies were on various types of cancers [13, 20, 22]. Effects were described according to outcome measures including anxiety (nine studies) [7,8,9,10, 13, 19, 20, 22, 27], depression (four studies) [10, 19, 22, 27], and QoL (three studies) [7, 19, 27]. The majority of the studies (seven studies) evaluated the short-term effectiveness of music (immediately after the intervention). Only two studies assessed the long-term effects such as after 1 week, after 3 weeks [10], and after 3 months [27] (Table 1). No study described the theoretical framework that underpinned the selected studies.
Effectiveness of music intervention on anxiety, depression, and QoL
The effectiveness of music intervention on anxiety
Anxiety was evaluated in nine studies [7,8,9,10, 13, 19, 20, 22, 27] involving 686 participants. Four instruments were used to measure anxiety: the Spielberger Anxiety Inventory scale, the Hospital Anxiety and Depression scale (HADS), the Beck Anxiety Inventory, and the visual analog scale (Table 1).
The majority of the studies (78%) showed the significant effects of music intervention on anxiety. Among the studies, Bro et al. [7] illustrated that the live music group showed a borderline reduction in anxiety, but the recorded music did not appear to impact the intervention benefits for anxiety (p = 0.18). Tuinmann et al. [27] revealed that music had no benefit on anxiety improvement. Similarly, Mondanaro et al. [22] reported that music intervention did not have a significant impact on anxiety and depression.
A meta-analysis of six trials [8, 10, 13, 19, 20, 27] examined anxiety among 373 participants indicating significantly lower anxiety among participants who received standard care combined with music interventions than those who received standard care alone (SMD: − 0.29, 95% CI − 0.50 to − 0.08, p = 0.006, I2 = 62%) (Fig. 2a). Sensitivity analysis showed no heterogeneity when excluding two studies because of a high risk of bias involved in the randomization process [10] and a high attrition rate [27]. The results of sensitivity analysis revealed a medium effect of music intervention on anxiety (SMD: − 0.62, 95% CI − 0.90 to − 0.34, p < 0.001, I2 = 0%) (Fig. 2b).

Forest plot of comparison: music intervention plus standard care versus standard care alone on anxiety. a All studies;b sensitivity analysis
The effectiveness of music intervention on depression
Studies used HADS and Beck Depression Inventory-2nd ed (Table 1) which were self-report instruments to measure clinical depression. Among four studies evaluating depression, two suggested that music intervention had a positive effect on depression [10, 19]. Chen et al. [10] reported that music did not help patients to reduce depression immediately after intervention and 3 weeks after the intervention, but it had a significant effect 1 week after the intervention. A study by Lima et al. [19] showed a medium effect of music intervention on depression (Cohen’s d = 0.69). However, two studies indicated no significant difference in depression between the music intervention group and the control group [22, 27]. Three studies [10, 19, 27] were eligible for meta-analysis without showing an overall statistically significant effect on depression (SMD = − 0.04, 95% CI − 0.32 to 0.24, p = 0.79, I2 = 0%) (Fig. 3a).

Forest plot of comparison: music intervention plus standard care versus standard care alone. a On depression; b on QoL
The effectiveness of music intervention on QoL
Three studies [7, 19, 27] evaluated the effect of music intervention on QoL. Two of the studies recruiting hematological cancer patients [7, 27] reported that music intervention did not show a significant effect on QoL. However, the remaining study by Lima et al. [19] revealed an increase in QoL among breast cancer patients. Two studies [19, 27] were eligible for the meta-analysis showing a small effect of music intervention on patients’ QoL (SMD: 0.42, 95% CI 0.02 to 0.82, p = 0.04, I2 = 18%) (Fig. 3b).
Intervention contents and subgroup analysis
Among the nine studies selected, six used music therapy [7, 9, 10, 13, 22, 27], and three used music medicine [8, 19, 20]. In the selected studies, the people who provided music medicine were nurses [8, 20] or medical doctors [19]. Recorded music [7,8,9,10, 19, 20] or live music [7, 13, 27] were applied in the studies. In the studies using music therapy guided by music therapists, the participants had more chances to be actively involved in the music activities such as playing musical instruments, singing [27], singing along to a music therapist with a guitar [13], or applying the guided music imagery [9] (Table 2).
Subgroup analysis compared the treatment benefits of music therapy versus music medicine on anxiety. Among the six studies that were eligible for meta-analysis, three studies evaluated the effects of music medicine [8, 19, 20] and three studies evaluated the effects of music therapy [10, 13, 27].The pooled effect of the three studies involving music medicine [8, 19, 20] (SMD: − 0.64, 95% CI − 0.96 to − 0.32, p < 0.001, I2 = 0%) was larger than that of the music therapy [10, 13, 27] on anxiety (SMD: − 0.09, 95% CI − 0.50 to 0.32, p = 0.11, I2 = 54%). The difference between the subgroups was statistically significant (p = 0.04) (Supplementary Fig. 1).
The most popular selected music in the studies were classical music, new age, relaxing nature sounds, film soundtrack, and folk music with a tempo of 60 to 80 beats/min [7, 8, 10]. The patients were allowed to choose their preferred music from their own collection or a list of music that was pre-selected by the researcher in seven of the studies [7,8,9,10, 13, 22, 27]. The participants were provided with headphones or earphones to block external or environmental sounds in four of the studies [7, 8, 10, 20] (Table 2). Findings revealed a significant effect of researcher-selected music on anxiety (SMD: − 0.52, 95% CI − 0.92 to − 0.11, p = 0.01, I2 = 0%), but no significance of the patient-selected music (SMD: − 0.21, 95% CI − 0.45 to 0.03, p = 0.09, I2 = 74%). However, there were no significant differences between the subgroups (p = 0.2) (Supplementary Fig. 2). A subgroup analysis comparing recorded music on anxiety (SMD: − 0.40, 95% CI − 0.89 to − 0.10, p = 0.11, I2 = 73%) with live music (SMD: − 0.26, 95% CI − 0.79 to 0.27, p = 0.34, I2 = 0%) found no statistically significant differences between the two types of music delivery methods (p = 0.71) (Supplementary Fig. 3).
The duration for each music session lasted from 15 min to 1 h. The timing of the intervention was when the patients were undergoing chemotherapy [7, 10, 13, 20, 22] or immediately before the chemotherapy [8, 19]. The therapist delivered music to the patients during hospitalization days in two of the studies but did not report the specific time [9, 27]. Four studies evaluated the effects of music intervention through a single music session [8, 10, 13, 20] and others evaluated the effects of multiple music sessions [7, 9, 19, 22, 27]. Among the studies conducted with multiple music sessions, the schedule of the intervention was different, including every 2 to 3 weeks [7, 19], twice a week [9, 27], and three music sessions/1 to 3 months [22]. The intervention ranged from one to five chemotherapy sessions (Table 2).
A subgroup analysis compared the effects of music intervention on anxiety before and during chemotherapy. Results showed no significant effect of music during chemotherapy (SMD: − 0.2, 95% CI − 0.47 to − 0.07, p = 0.15, I2 = 71%), but applying music intervention for the patients immediately before the chemotherapy resulted in a medium effect size that was statistically significant (SMD: − 0.71, CI − 1.14 to − 0.29, p < 0.001, I2 = 0%). There was a significant difference between subgroups (p = 0.04) (Supplementary Fig. 4).
A subgroup analysis comparing the duration of a music listening session on anxiety showed the length from 15 to 20 min led to a much larger and statistically significant pooled effect (SMD: −0.71, 95% CI −1.10 to −0.33, p < 0.01, I2 = 0%) than the length over 30 to 45 min (SMD: −0.17, 95% CI −0.52 to 0.19, p = 0.37, I2 = 51%). There was a significant difference between subgroups (p = 0.04) (Supplementary Fig. 5).
Critical appraisal result and quality of evidence
All studies were identified as having a high risk of bias. Concerning the randomization process, one study had a high risk of bias due to an imbalance of baseline between groups [10] and four studies presented some concerns because of insufficient information about the randomization method and/or allocation concealment [8, 9, 13, 20]. For biases due to deviations from intended interventions, all studies were considered as low risk. Two trials [9, 22] were assessed with a high risk of bias because of the high percentage of missing data and lack of attrition reasons. One study [27] was evaluated as having some concerns. The reason was that despite the high attrition rate, it was related to the participants’ health. All trials were evaluated as having a high risk for using the self-reporting method to measure the outcomes. In music intervention, the patients were aware of the intervention [4] and patient-reported outcomes would be affected by not blinding the patients [14]. Most of the studies were identified as having a low risk for selection of the reported results, except a study by Burns et al. [9], which was evaluated as high risk because they did not report all the results from different time points (Fig. 4).

Risk of bias summary: review authors’ judgements about the risk of bias item for each included study
The overall quality of evidence was assessed following GRADE as low on anxiety and depression and very low on QoL because of the small sample size, inconsistent results, and high risk of biases. The summary assessment is presented in Supplementary table 1.
Discussion
To the best of our knowledge, this is the first systematic review and meta-analysis to assess the effectiveness of music intervention on anxiety, depression, and QoL among cancer patients receiving chemotherapy. A total of nine studies were included in this review involving music therapy and music medicine.
Our review reveals that there is a significant effect of music intervention on the anxiety of adult cancer patients receiving chemotherapy. The finding is consistent with a systematic review of Bradt et al. [4], which selected studies that evaluated music on patients with cancer regardless of type, treatments, stages, and settings. The results suggested that music intervention had a positive impact on anxiety with a large effect. Similarly, a review of Bro et al. [6], which included studies assessing music intervention in patients undergoing active cancer treatment, revealed a large effect on anxiety (SMD: − 0.8).
However, music has no statistically significant effect on depression. Although Lima et al. [19] showed a medium effect (SMD: 0.55), the sample size of Lima’s study [19] was small (16 and 17 of each group). Thus, the results of Lima et al. [19] should be interpreted with caution. In terms of the effects of music intervention on QoL, although music intervention had a significant impact on the breast cancer population [19], there was no significant improvement of QoL on patients with hematopoietic malignancies [7, 27]. Maybe, the hematological cancer patients who receive high-dose chemotherapy experience higher distress and pain while undergoing hematopoietic stem cell transplantation. Furthermore, immunological changes (lymphocytes, immunoglobulins, NK-cells, T4/T8 ratio) cause more anxiety disorders than other types of cancer [13]. Thus, such serious psychological issues may not be reduced by music intervention and QoL remains poor.
The results revealed that music medicine had a stronger effect on anxiety than music therapy. This is similar to the results of Bradt et al. [4]. In our study, the smaller effects of music therapy on anxiety can be explained by differences in participants’ characteristics in the selected studies. Firstly, two studies in music medicine groups assessed breast cancer [8, 19] in stages I and II, while a study by Chen et al. [10] in the music therapy group recruited patients with breast cancer in all stages (around 50% of stages III and IV). The severity of stages III and IV may result in a higher level of anxiety. Therefore, the effect of music was much lower in Chen’s study [10]. Secondly, a study [27] in the music therapy group evaluated hematological cancer with high-dose chemotherapy. Thus, the high intensity and dosages of chemotherapy might affect the effectiveness of music therapy on anxiety reduction.
Delivery timing, types of delivery, or the person who selected the music varied among the selected studies. Subgroup analyses did not illustrate significant differences between the effects of patient-selected music and researcher-selected music, and recorded music and live music. A previous study reported that live music was more effective than pre-recorded music on anxiety [3]. Bro et al. [7] reported live music could reduce anxiety, but there was no significant effect of recorded music on the outcome in lymphoma patients during chemotherapy. Regarding the length of a music listening session, the subgroup analysis showed that the short duration (15–20 min) presented a larger effect than that of the long duration (30–45 min). The guidelines of the American Music Therapy Association [2] suggest that the length of music listening should not be over 50 min. According to a guideline for music therapy practice [1] in adult medical care, the length of shorter than 20 min is suitable for acute settings. In terms of the timing of the intervention, subgroup analysis also revealed that music delivered immediately before chemotherapy treatment had a greater effect than that of the music delivered during the chemotherapy. According to Stress and Coping theory [18], people may have psychological issues even before the stressful event if it is ambiguous or had they experienced the same situation before. While the patients are waiting for chemotherapy, they may suffer emotional symptoms such as anxiety. Listening to music immediately before chemotherapy may help the patients alleviate emotional disorders such as anxiety and depression. The tempo was reported in three studies in which music with 60–80 beats/min was used [7, 8, 10]. This tempo is restful [8], similar to the human heart rate, and is considered to be the best for generating relaxation [24]. More studies may be needed to reveal its effect on psychological symptoms.
Limitations and implications
There are several limitations of this review. Firstly, we only selected papers written in English. Secondly, all studies were assessed as having a high risk of biases. Lastly, a small number of studies were included, especially on depression and QoL outcomes. It affects the confidence of the evidence in this review.
However, this review provides some implications for future research. Firstly, further studies should comply with the rigor of the design concerning the randomization. Secondly, as most studies only evaluated immediately after the intervention, the long-term effect should be assessed in future studies. Thirdly, studies selected for this review were conducted in developed countries. Thus, more studies in developing and underdeveloped countries would contribute to broadening our understanding of the effects of music intervention in different sociocultural settings. Fourthly, there was a limitation in the number of studies evaluating depression and QoL, so more studies assessing these outcomes are needed. Finally, no RCT used theory to guide the study design. Future studies underpinning an appropriate theory are warranted. For clinical practice, the findings of this review suggest that the duration of a music listening session from 15 to 20 min, delivered immediately before chemotherapy, is more effective in reducing anxiety. It is recommended to choose relaxing music with a tempo of 60 to 80 beats/min [7, 8, 10].
Conclusion
Music intervention might be an effective tool to reduce anxiety and improve QoL among cancer patients receiving chemotherapy, but it does not show effects on depression. Choosing relaxing music with 60–80 beats/min, the length 15–20 min, and delivering immediately before chemotherapy is suggested to alleviate anxiety. It is recommended that future RCTs should adhere to methodological rigor.
Data Availability
All data generated or analyzed during this study are included in this published article (and its supplementary information files).
Code availability
None.
References
Allen J (2013) Guidelines for music therapy practice in adult medical care. Barcelona Publishers, Gilsum, N.H., US
American Music Therapy Association (2021) Music listening guideline. https://www.musictherapy.org/research/guidance_for_music_listening_programs/. Accessed 14 July 2021.
Bailey LM (1983) The effects of live music versus tape-recorded music on hospitalized cancer patients. Music Ther 3:17–28
Bradt J, Dileo C, Magill L, Teague A (2016) Music interventions for improving psychological and physical outcomes in cancer patients. Cochrane Database Syst Rev 8 https://doi.org/10.1002/14651858.CD006911.pub3
Bradt J, Potvin N, Kesslick A, Shim M, Radl D, Schriver E, Gracely EJ, Komarnicky-Kocher LT (2015) The impact of music therapy versus music medicine on psychological outcomes and pain in cancer patients: a mixed methods study. Support Care Cancer 23:1261–1271
Bro ML, Jespersen KV, Hansen JB, Vuust P, Abildgaard N, Gram J, Johansen C (2018) Kind of blue: a systematic review and meta-analysis of music interventions in cancer treatment. Psychooncology 27:386–400
Bro ML, Johansen C, Vuust P, Enggaard L, Himmelstrup B, Mourits-Andersen T, Brown P, d’Amore F, Andersen EAW, Abildgaard N, Gram J (2019) Effects of live music during chemotherapy in lymphoma patients: a randomized, controlled, multi-center trial. Support Care Cancer 27:3887–3896
Bulfone T, Quattrin R, Zanotti R, Regattin L, Brusaferro S (2009) Effectiveness of music therapy for anxiety reduction in women with breast cancer in chemotherapy treatment. Holist Nurs Pract 23:238–242
Burns DS, Azzouz F, Sledge R, Rutledge C, Hincher K, Monahan PO, Cripe LD (2008) Music imagery for adults with acute leukemia in protective environments: a feasibility study. Support Care Cancer 16:507–513
Chen SC, Yeh ML, Chang HJ, Lin MF (2020) Music, heart rate variability, and symptom clusters: a comparative study. Support Care Cancer 28:351–360
Cohen J (1988) Statistical power analysis for the behavioral sciences (2nd ed). Laurence Erlbaum Associates, Inc., Hillsdale, NJ. https://doi.org/10.4324/9780203771587
Collaboration TC (2020) Review Manager (RevMan) [Computer program]. Version 5:4
Ferrer AJ (2007) The effect of live music on decreasing anxiety in patients undergoing chemotherapy treatment. J Music Ther 44:242–255
Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA (2019) Cochrane handbook for systematic reviews of interventions. John Wiley & Sons
Jasemi M, Aazami S, Zabihi RE (2016) The effects of music therapy on anxiety and depression of cancer patients. Indian J Palliat Care 22:455
Koelsch S (2014) Brain correlates of music-evoked emotions. Nat Rev Neurosci 15:170–180
Krebber AMH, Buffart LM, Kleijn G, Riepma IC, de Bree R, Leemans CR, Becker A, Brug J, van Straten A, Cuijpers P, Verdonck-de Leeuw IM (2014) Prevalence of depression in cancer patients: a meta-analysis of diagnostic interviews and self-report instruments. Psychooncology 23:121–130
Lazarus RS (1984) Stress, appraisal, and coping Springer Pub. Co, New York
Lima TU, Moura ECR, Oliveira CMBd, Leal RJDC, Nogueira Neto J, Pereira EC, Nascimento RVB, Oliveira EJSGd, Leal PdC (2020) Impact of a music intervention on quality of life in breast cancer patients undergoing chemotherapy: a randomized clinical trial. Integr Cancer Ther 19:1534735420938430
Lin M-F, Hsieh Y-J, Hsu Y-Y, Fetzer S, Hsu M-C (2011) A randomised controlled trial of the effect of music therapy and verbal relaxation on chemotherapy-induced anxiety. J Clin Nurs 20(7–8):988–999
Mitchell AJ, Chan M, Bhatti H, Halton M, Grassi L, Johansen C, Meader N (2011) Prevalence of depression, anxiety, and adjustment disorder in oncological, haematological, and palliative-care settings: a meta-analysis of 94 interview-based studies. Lancet Oncol 12:160–174
Mondanaro JF, Sara GA, Thachil R, Pranjic M, Rossetti A, EunHye Sim G, Canga B, Harrison IB, Loewy JV (2021) The effects of clinical music therapy on resiliency in adults undergoing infusion: a randomized, controlled trial. J Pain Symptom Manage 61:1099–1108. https://doi.org/10.1016/j.jpainsymman.2020.10.032
Nikbakhsh N, Moudi S, Abbasian S, Khafri S (2014) Prevalence of depression and anxiety among cancer patients. Caspian J Intern Med 5:167–170
Nilsson U (2009) Caring music: music intervention for improved health. Update 2009:8–5
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, Chou R, Glanville J, Grimshaw JM, Hróbjartsson A, Lalu MM, Li T, Loder EW, Mayo-Wilson E, McDonald S, McGuinness LA, Stewart LA, Thomas J, Tricco AC, Welch VA, Whiting P, Moher D (2021) The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 372:n71
Santos MSD, Thomaz FM, Jomar RT, Abreu AMM, Taets G (2021) Music in the relief of stress and distress in cancer patients. Rev Bras Enferm 74:e20190838
Tuinmann G, Preissler P, Bohmer H, Suling A (2017) Bokemeyer C (2017) The effects of music therapy in patients with high-dose chemotherapy and stem cell support: a randomized pilot study. Psychooncology 26(3):377–384
Zhang J-M, Wang P, Yao J-x, Zhao L, Davis MP, Walsh D, Yue GH (2012) Music interventions for psychological and physical outcomes in cancer: a systematic review and meta-analysis. Support Care Cancer 20:3043–3053
Zhang Y, Akl EA, Schünemann HJ (2019) Using systematic reviews in guideline development: the GRADE approach. Res Synth Methods 10:312–329
Zhao J, Cui W, Tian B-p (2020) Efficacy of tocilizumab treatment in severely ill COVID-19 patients. Crit Care 24:524
Acknowledgements
The authors would like to acknowledge the Chinese University of Hong Kong Library, Dr. K C Choi for his assistance in statistics, and Dr. Thapa Chura Bahadur for his support in language editing.
Author information
Authors and Affiliations
Contributions
The idea for the review was from KTN, CWHC, and JX. The methodology was guided by CWHC, DNSC, and JX. The literature search and data analysis were performed by KTN, JX, and MZ. The first draft of the manuscript was written by KTN, and all authors commented and revised the original versions of the manuscripts. All authors read and approved the final manuscripts. The whole process of the review was supervised by CWHC.
Corresponding author
Ethics declarations
Ethics approval
Not applicable.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Nguyen, K.T., Xiao, J., Chan, D.N.S. et al. Effects of music intervention on anxiety, depression, and quality of life of cancer patients receiving chemotherapy: a systematic review and meta-analysis. Support Care Cancer 30, 5615–5626 (2022). https://doi.org/10.1007/s00520-022-06881-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00520-022-06881-2