
Abstract
Background
Patients receiving intensive chemotherapy can experience increased distressed related to both the cancer diagnosis and treatment isolation. If not addressed, distress can lead to anxiety, depression, and post-traumatic stress disorder. The purpose of this study was to determine the feasibility and possible benefits of a music imagery intervention for patients hospitalized in a protective environment for the treatment of acute leukemia or high-grade non-Hodgkin’s lymphoma.
Materials and methods
Adults receiving intensive myelosuppressive chemotherapy in a protective environment were randomized to standard care or standard care plus music imagery. The music imagery sessions occurred twice weekly for up to eight sessions. Patients were encouraged to use the music imagery daily.
Results
The principal criteria of feasibility were rate of consent, rate of completion of scheduled sessions, and rate of questionnaire completion. Forty-nine out of 78 patients consented, a 63% consent rate. Seventy-two percent of all scheduled music imagery sessions were completed. The rate of questionnaire completion was 60% with missing data because of illness severity and early discharge. The principal outcomes of benefit (e.g., efficacy) were positive and negative affects, fatigue, and anxiety. Both groups improved over time on all outcomes (all p < 0.001). However, a subgroup of individuals with low baseline negative affect who received the intervention reported significantly less anxiety at discharge than individuals with low baseline negative affect who did not receive the intervention.
Conclusions
Music imagery is feasible for adults with acute leukemia in protected environments. Patients with lower initial distress may benefit from a music imagery program in terms of reduced anxiety at discharge.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Patients with acute leukemia (AL) or high-grade non-Hodgkin’s lymphoma (HG-NHL) who receive intensive myelosuppressive chemotherapy typically require a prolonged hospitalization because of the high incidence of infectious, hemorrhagic, and muco-cutaneous complications and the need for frequent blood product transfusion. In addition, to reduce the risk of infection, patients stay in a protective environment that consists of a high-efficiency particulate air (HEPA)-filtered room and limited access to visitors. Patients who are treated in protective environments experience loneliness and increased feelings of being shut in that can exacerbate the high levels of psychological distress associated with the diagnosis of cancer [1, 2]. If not addressed, psychological distress can result in long-term adjustment disorders including extended anxiety and/or depression [3].
A variety of psychotherapeutic interventions, such as cognitive restructuring, group support, relaxation training, hypnosis, and guided imagery, may decrease psychological distress during cancer treatment [4]. A recent systematic review of guided imagery randomized controlled trials concluded that guided imagery may be psycho-supportive and increase comfort in cancer patients. However, the variability in outcomes suggests that guided imagery alone is an inadequate intervention in terms of reducing psychological distress [5].
The concurrent use of music and imagery is believed to be more beneficial because the imagery experience is regulated by the harmonic and structural properties of the music [6]. Music enhances imagery by making images more vivid [7–9], increasing involvement in the imagery experience [10], making images more accessible, and increasing image duration and quality [8, 9]. We speculate that the music coordinates activation of multiple cortical association areas, explaining the vividness of the imagery experience and the lack of cognitive control needed to experience imagery while listening to music [11]. Additionally, the associative properties of music function to activate existing emotional and cognitive schemas making them available for processing [12].
The combination of music and guided imagery has been shown to decrease anxiety and improve mood. Healthy adults (n = 14) and college students (n = 26) reported significantly improved mood after music imagery sessions when compared to wait-list [13, 14], cognitive intervention, or no treatment control conditions [15]. Clients on a chemical-dependency unit (n = 9) also reported lower state anxiety scores upon completion of a series of ten music imagery sessions when compared to no treatment control [16]. Burns reported that four cancer survivors experienced improvement in anxiety after a series of ten music imagery sessions [17].
Despite these positive findings, two issues potentially reduce generalizability to more acute settings. First, the reporting of music imagery trials have not typically included recruitment or attrition rates, so it is unclear whether medical patients find these types of interventions acceptable. Furthermore, a majority of these studies have recruited healthy individuals as participants [13–15]. Only one study explored the use of music imagery for chemical dependency patients [16], and only one explored the use of a music imagery intervention in cancer survivors [17]. It is unknown whether completing a music imagery protocol will be too taxing for individuals who are undergoing intensive medical procedures. Patients may not be willing to participate in a trial close to the time of a life-threatening diagnosis and during a treatment that has a high level of physical and emotional demands. Therefore, both the ability to recruit very sick participants and their ability to complete a full protocol (e.g., music imagery sessions and data collection assessments) are unknown.
Thus, the aims of the current trial were to (1) determine the feasibility of a music imagery protocol for patients hospitalized in a protective environment during the treatment of AL or HG-NHL and (2) the effect of the intervention on levels of affect, fatigue, and anxiety. Research hypotheses related to feasibility were:
-
1.
Greater than 60% of those patients approached to participate in the music imagery study will consent to study participation.
-
2.
Patients randomized to the music imagery protocol will complete 80% of the scheduled intervention sessions.
-
3.
Patients will be able to complete at least 90% of the questions at each assessment period.
The research hypothesis related to benefit (e.g., efficacy) was:
-
4.
Compared to those receiving standard care, AL or non-Hodgkin’s lymphoma patients randomly assigned to receive the music imagery intervention will demonstrate higher positive affect and lower negative affect, fatigue, and anxiety.
Materials and methods
The Indiana University Simon Cancer Center Scientific Review Committee and the Institutional Review Board of Indiana University–Purdue University in Indianapolis approved the study. Informed consent was obtained from each participant before the completion of any study related procedures. A Leukemia Nurse Coordinator (Hincher or Rutledge) identified patients who were greater than 18 years of age, had the ability to read and understand English, and were admitted to the Hematology–Oncology Unit at Indiana University Hospital for the treatment of AL or HG-NHL. Patients were excluded if they were not cognitively able to participate in the intervention or answer the self-report questionnaires. Study personnel (Sledge or Burns) discussed the study with potential participants within 2 days of hospital admission. After written informed consent, all patients completed self-report instruments to assess affect, fatigue, and anxiety (described below). Participants were then randomized to receive standard care or standard care plus music imagery.
Standard care consisted of hospitalization in a HEPA-filtered room with restricted access to visitors for administration of intensive chemotherapy followed by supportive care including prophylactic and empiric antibiotics, transfusion support, and nutritional support as required. A team composed of an attending physician, two resident physicians, and an advanced practice nurse cared for the patient. Individuals assigned to standard care plus music imagery met with the same board-certified music therapist throughout hospitalization. A board-certified music therapist is an individual who has successfully completed an academic and clinical training program approved by the American Music Therapy Association, passed a written, objective examination demonstrating competency in the music therapy profession, and participates in continuing education [18].
The initial music imagery session occurred within 3 days of admission and then twice weekly over the course of the hospital stay through week 4. We anticipated up to eight sessions. The target duration for each session was 45 min. The music imagery sessions with the therapist included two components: education and experience. During the education portion of the session, the therapist provided information about how to use music imagery exercises. The experience portion of the session included two elements: relaxation and music imagery [19]. This portion of the session was designed to provide the participant an opportunity to practice music imagery techniques, provide the participant with a successful music imagery experience, and answer any questions the participant may have regarding the use of music imagery. When the session was completed, the therapist provided the equipment needed to use the music imagery exercises without the therapist being present (playback machine and compact disc containing four 20-min music imagery exercises). The music therapist encouraged participants to use the music imagery exercises at least once a day during their hospital stay. If desired, participants could use the intervention more frequently. A journal was left so the participant could record the use of the equipment, how many exercises were used in between meetings with the therapist, and the perceived effectiveness of the music imagery exercise(s). During the subsequent therapist visits, participants had the opportunity to ask questions regarding the use of music imagery or change music imagery selections and experience a music imagery session led by the therapist.
The music for the study included several selections of light classical and new age music. The music therapist chose music for each specific patient based on an assessment of the patient’s musical preferences, current emotional state, and energy level. Generally, the more emotional and less energetic the participant, the more simple and structured the music selections.
Power analysis
To obtain an estimate of the sample size needed to address the second aim of benefit, we used effect sizes for anxiety, as measured by the State-Anxiety Inventory (STAI) S-Anxiety scores. In one published music therapy study, the STAI was found to have a SD of 12.00, a pre–post-test change score of 8.78, and an effect size of. 73. To detect this effect size, with 0.8 power and a p of 0.05, we planned to enroll 30 participants into each condition [20, 21].
Measures
Affect was measured with the Positive Affect and Negative Affect Schedule (PANAS) [22] consisting of two ten-item summated scales that, respectively, measure positive and negative affect. The Positive Affect (PA) scale evaluates the extent to which a person feels enthusiastic, active, and alert. High PA scores indicate high energy, full concentration, and pleasurable engagement; low PA scores indicate sadness and lethargy. The Negative Affect (NA) scale evaluates the extent to which a person feels distress and unpleasant engagement. High NA scores indicate elevated anger, contempt, disgust, guilt, fear, and nervousness. For the purpose of this study, respondents were asked to indicate their present feelings. Coefficient alphas for the PA and NA scales for “at this moment” instructions have been reported as 0.89 and 0.85, respectively [22]. For this study, alpha reliabilities for PA were 0.86 and 0.89 for NA.
The Functional Assessment of Chronic Illness Therapy—Fatigue scale (FACIT-F) was used to assess fatigue. The FACIT-F is a 13-item, symptom-specific subscale of the Functional Assessment of Cancer Therapy measurement system [23]. Respondents are asked to indicate how true each statement has been for them during the past 7 days. Each item includes a five-point (0–4) response scale ranging from “Not at all” (0) and “Very much” (4). Cronbach alpha for the 13-item scale was reported as 0.93 [23]. For the current study, alpha reliability was 0.91.
Anxiety was measured with the STAI Form Y-1 [24], which consists of 20 items that evaluate how respondents feel “right now, at this moment.” The qualities evaluated by the STAI S-Anxiety scale are feelings of apprehension, tension, nervousness, and worry. Scores have been shown to increase in response to physical danger and psychological stress and decrease as a result of relaxation training. Each STAI item is scored 1–4. Scores are obtained by summing the responses to the 20 items. Scores range from 20 to 80. Alpha coefficients for working adults, students, and military recruits have ranged from 0.86 to 0.95, with a median coefficient of 0.93 [24]. Alpha reliability for the present sample was 0.92.
The Music Imagery Use journal was also developed to determine whether or not patients would use the music imagery exercises in between sessions with the therapist. For each in-between session, patients were asked to record how many of the music imagery sessions they listened to and the perceived effectiveness on a five-point scale (1 = not effective, 5 = completely effective).
Results
Baseline characteristics of the sample are reported in Table 1. Intervention and standard care groups were not significantly different on any of these baseline characteristics (p > 0.05).
Feasibility
The three principal criteria for defining feasibility were the rate of consent, percent of completed music imagery sessions, and completed measurement instruments.
Rate of consent
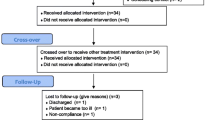
Seventy-eight patients were approached for participation in this trial over the 24-month study period; 29 refused, resulting in a 63% consent rate (see Fig. 1). The three most common reasons for refusal were: overwhelmed by treatment (n = 9), not interested (n = 8), and too sick (n = 6). Therefore, 49 individuals were randomized to either standard care (n = 24) or standard care plus music imagery (n = 25). Individuals who declined to consent were no different in terms of gender, age, or diagnosis.

Recruitment flow
The study sample included 19 men and 30 women, and a majority were married (65%). Nineteen people withdrew early from the study for a final sample of 30 participants. The most common reason for study withdrawal was that the patient was too sick to either complete the measures or carry out the intervention (n = 6). Additionally, four patients voluntarily withdrew from the study participation, four patients were transferred to the intensive care unit, and three patients passed away while in the hospital. Two individuals did not complete questionnaires at the clinic follow-up.
Completed music imagery sessions
Participants who were randomized to the music imagery group were scheduled to meet with the music therapist twice a week for up to eight total sessions. Seventy-two percent of all scheduled sessions were completed when we account for dropouts or early discharge. Eleven individuals completed 100% of scheduled sessions, and four completed at least 75% of scheduled sessions. Patients were also asked to use the music imagery exercises once a day and keep track of usage using a journal created specifically for this study. While patients and family members reported to the music therapist (Sledge) that they had used the music in between sessions, no one completed corresponding journal entries. Reasons for incomplete journal entries were generally related to feeling too sick or not remembering.
Rate of questionnaire completion
To determine patients’ tolerance for completing measures on a weekly basis, we looked at the pattern of questionnaire completion throughout the study period. Each measurement session included the three measures, which were scheduled for completion each week. Forty-nine participants completed an average of 60% of the measurement instruments. Thirteen participants completed 100% of the measurement instruments. Week 4 and discharge (63 and 61%) had the highest amount of missing data regardless of group assignment. As stated previously, no one completed the music imagery use journal.
Benefits
Finally, we were also interested in whether or not the intervention was helpful in improving positive affect and reducing negative affect, fatigue, and anxiety compared to standard care. To test for an intervention effect during hospitalization, a repeated-measures analysis of variance (ANOVA) was used to calculate the differences between intervention and standard care groups for time points 2, 3, 4, and 5. Group membership (music imagery or standard care) constituted the independent variable; scores from the primary outcome measures, including the PANAS NA, PANAS PA, FACT-F, and STAI constituted the outcome variables.
The analysis of the mean scores over time indicated that both groups improved in terms of greater positive affect, less negative affect, less fatigue, and less anxiety (all p < 0.001). Additionally, there was no indication that the intervention was significantly more beneficial than standard care. However, when we analyzed patients by level of baseline PANAS NA (higher levels being indicative of greater distress), patients with low negative affect at baseline who received music imagery had lower anxiety at the time of discharge compared to standard care individuals who had low negative affect at baseline (mean of 48 vs 23, p = 0.02, n = 18). These anxiety score values correspond to the 80th and 20th percentile, respectively, when compared to the general population norms. Therefore, among individuals within the low baseline negative affect subgroup, those who received the intervention reported significantly less anxiety than individuals who did not receive the intervention. The reduction appears to be clinically meaningful.
Discussion
Cancer patients treated in isolation units, such as patients with AL and HG-NHL often experience loneliness and increased feelings of being shut in, leading to elevated levels of distress [2, 25]. Nearly half of patients treated in isolation exhibit anxiety and fatigue during treatment [2, 26–28]. If not treated, these high levels of distress can last years after treatment, leading to extended anxiety and possibly post-traumatic stress disorder [3].
Previous research indicates that both imagery and music are beneficial in terms of alleviating distress and improving quality of life [13–17]. However, we needed to determine if a combination of these two modalities was acceptable to patients at the beginning of treatment, if it was feasible to implement this intervention within the structure of a randomized trial, and if there was any indication of benefit.
We defined feasibility as including consent rates, percentage of completed music imagery sessions, and percentage of completed instruments. Specifically, we were interested in whether or not patients would be willing to consent and participate in a music trial so close to the time of diagnosis and during intensive treatment. Consent rates in music therapy trials are rarely reported; however, those available indicate a wide variability (30–80%) in acceptance of music therapy research [29, 30]; therefore, we consider the current study’s recruitment rate of 63% acceptable.
Additionally, there was a high rate of music imagery intervention completion. As expected, reasons for not completing sessions were typically due to extreme complications from their disease process or treatment. Data collection was also deterred by high levels of treatment side effects or early discharge. Given the level of intervention completion, however, we believe that further research within this area is feasible.
Previous research conducted within this patient population indicates that the initial hospital experience and the shock of the cancer diagnosis influence distress and anxiety rates at the beginning of treatment. Once patients acclimate to the hospital surroundings, emotional distress often subsides but not to pretreatment levels [31]. Our findings are consistent with this previous research. This natural acclimation to the hospital environment presents difficulties in assessing the benefits of an intervention as the effects of the intervention may be hidden. Music-based interventions as well as other psychosocial interventions must be extremely powerful to demonstrate robust effects.
A subset of individuals experienced a positive intervention effect in which there was greater benefit from participating in the music imagery sessions than in standard care. This subset of patients was less distressed at the beginning of treatment than those who did not demonstrate a beneficial intervention effect. It may have been difficult for those individuals who were experiencing higher distress to engage in the music imagery intervention and/or use the music imagery without the therapist. These explanations are consistent with literature suggesting that the ability to engage in the intervention influences the effectiveness of the intervention [32]. In this case, high negative affect, indicating feelings of distress that include anger, contempt, disgust, guilt, fear, and nervousness, influenced the effectiveness of the music imagery. A heightened level of distress increases attentional fatigue and decreases concentration, both required to engage in a self-directed cognitive intervention such as music imagery [33]. Future studies will involve a more structured therapist-led music intervention designed to provide more support for highly distressed individuals. However, the current intervention seems to be beneficial for those with lower baseline levels of distress.
Study limitations and future research
Assessing the feasibility of studying music imagery-based interventions brought to light additional considerations for future research. One important limitation is the lack of a sufficient control group; it is possible that decreases in anxiety were associated with the additional attention given to the patients in the intervention group. Future studies need to employ a control condition that accounts for elements considered “inert” within the intervention protocol such as the attention of the interventionist. Therefore, including comparison to a third attention-control condition will be important.
The demands of completing evaluations on a weekly basis raise several issues for consideration. During the third and fourth weeks of hospitalization, the rate of instrument completion dropped considerably, mostly because of disease severity. While the evaluation was usually completed in less than 15 min, the number of instruments used during hospitalization needs to be carefully scrutinized. Additionally, there was some indication from patients that the measures did not accurately reflect their hospital experience. Future studies will include qualitative interviews that can assess the meaningfulness of the music imagery intervention during hospitalization, so that further quantitative studies can use instruments that reflect the nature of patients’ experience.
Finally, music imagery is just one intervention that can be used during hospitalization for acute illness. In practice, music therapists and other health care providers use a combination of receptive and interactive music interventions to address therapeutic goals and to teach coping strategies. Meta-analyses indicate that interactive live-music therapy sessions are more beneficial than receptive [34]. However, research also indicates that newly diagnosed cancer patients receiving chemotherapy who are experiencing elevated levels distress prefer receptive modalities [35]. Various music-assisted relaxation methods are highly effective in decreasing arousal [36]. Future research discerning the benefits of particular treatment modalities within music therapy will assist clinicians in determining best practice guidelines for oncology patients.
References
Campbell T (1999) Feelings of oncology patients about being nursed in protective isolation as a consequence of cancer chemotherapy treatment. J Adv Nurs 30(2):439–447
Sasaki T, Akaho R, Sakamaki H et al (2000) Mental disturbances during isolation in bone marrow transplant patients with leukemia. Bone Marrow Transplant 25(3):315–318
Greenberg DB, Kornblith AB, Herndon JE et al (1997) Quality of life for adult leukemia survivors treated on clinical trials of Cancer and Leukemia Group B during the period 1971–1988: predictors for later psychologic distress. Cancer 80(10):1936–1944
Meyer T, Mark M (1995) Effects of psychosocial interventions with adult cancer patients: A meta-analysis of randomized experiments. Health Psychol 14:101–108
Roffe L, Schmidt K, Ernst E (2005) A systematic review of guided imagery as an adjuvant cancer therapy. Psycho-Oncol 14(8):607–617
Thaut MH (2002) Toward a cognition-affect model in neuropsychiatric music therapy. In: Unkefer RF, Thaut MH (eds) Music therapy in the treatment of adults with mental disorders: theoretical bases and clinical interventions. MMB Music, St. Louis, pp 86–103
McKinney CH (1990) The effect of music on imagery. J Music Ther 27:34–46
McKinney CH, Tims FC (1995) Differential effects of selected classical music on the imagery of high versus low imagers: two studies. J Music Ther 32:22–45
Quittner A, Glueckauf R (1983) The facilitative effects of music on visual imagery: a multiple measures approach. J Ment Imag 7:105–119
Band J (1996) The influence of selected music and structured vs. unstructured inductions on mental imagery. Doctoral dissertation, University of South Carolina
Burns DS (2000) The effect of classical music on absorption and control of mental imagery. J Assoc Music Imag 7:39–50
Kerr T, Walsh J, Marshall A (2001) Emotional change processes in music-assisted reframing. J Music Ther 38(3):193–211, Fall
McKinney CH, Antoni MH, Kumar AM, Kumar M (1995) Effects of guided imagery and music on depression and beta-endorphin levels in healthy adults: a pilot study. J Assoc Music Imag 4:67–78
McKinney CH, Antoni MH, Kumar M, Tims FC, McCabe PM (1997) Effects of guided imagery and music (GIM) therapy on mood and cortisol in healthy adults. Health Psychol 16(4):390–400, Jul
Russell LA (1992) Comparisons of cognitive, music, and imagery techniques on anxiety reduction with university students. J Coll Stud Dev 33:516–523
Hammer SE (1996) The effects of guided imagery through music on state and trait anxiety. J Music Ther 33:47–70
Burns DS (2001) The effect of the bonny method of guided imagery and music on the mood and life quality of cancer patients. J Music Ther 38(1):51–65, Spring
CBMT. The certification board for music therapists. Available at: http://www.cbmt.org/. Accessed July 17, 2007
Grocke DE, Wigram T (2007) Receptive methods in music therapy: techniques and clinical applications for music therapy clinicians, educators and students, 1st edn. Jessica Kingsley, London
Summer L (1994) Considering classical music for use in psychiatric music therapy. Music Ther Perspect 12(2):130–133
Summer L (1992) Music: the aesthetic elixer. J Assoc Music Imag 1:43–53
Watson D, Clark LA, Tellegen A (1988) Development and validation of brief measures of positive and negative affect: the PANAS scales. J Pers Soc Psychol 54(6):1063–1070
Cella D (1998) Factors influencing quality of life in cancer patients: anemia and fatigue. Semin Oncol 25(3 Suppl 7):43–46, June
Spielberger CD (1983) Manual for the state-trait anxiety inventory. Consulting Psychologists, Palo Alto, CA
Lee SJ, Loberiza FR, Antin JH et al (2005) Routine screening for psychosocial distress following hematopoietic stem cell transplantation. Bone Marrow Transplant 35(1):77–83, Jan
Montgomery C, Pocock M, Titley K, Lloyd K (2003) Predicting psychological distress in patients with leukaemia and lymphoma. J Psychosom Res 54(4):289–292, Apr
Schumacher A, Kessler T, Buchner T, Wewers D, van de Loo J (1998) Quality of life in adult patients with acute myeloid leukemia receiving intensive and prolonged chemotherapy—a longitudinal study. Leukemia 12(4):586–592
Persson L, Hallberg IR, Ohlsson O (1997) Survivors of acute leukaemia and highly malignant lymphoma–retrospective views of daily life problems during treatment and when in remission. J Adv Nurs 25(1):68–78, Jan
Lane D (1991) The effect of a single music therapy session on hospitalized children as measured by salivary immunoglobulin A, speech pause time, and a patient opinion Likert scale. Dissertation, Cleveland, Case Western Reserve
Cassileth BR, Vickers AJ, Magill LA (2003) Music therapy for mood disturbance during hospitalization for autologous stem cell transplantation: a randomized controlled trial. Cancer 98(12):2723–2729, Dec 15
Zittoun R, Achard S, Ruszniewski M (1999) Assessment of quality of life during intensive chemotherapy or bone marrow transplantation. Psycho-oncology 8(1):64–73, Jan–Feb
Kwekkeboom KL, Kneip J, Pearson L (2003) A pilot study to predict success with guided imagery for cancer pain. Pain Manag Nurs 4(3):112–123, Sep
Cimprich B (1995) Symptom management: loss of concentration. Sem Oncol Nurs 11(4):279–288
Standley J (2000) Music research in medical/dental treatment: an update of a prior meta-analysis. In: Smith DS (ed) Effectiveness of music therapy procedures: documentation of research and clinical practice, 3rd edn. American Music Therapy Association, Silver Springs, MD, pp 1–64
Burns DS, Sledge RB, Fuller LA, Daggy JK, Monahan PO (2005) Cancer patients’ interest and preferences for music therapy. J Music Ther 42(3):185–199, Fall
Pelletier CL (2004) The effect of music on decreasing arousal due to stress: a meta-analysis. J Music Ther 41(3):192–214
Acknowledgment
The project described was supported by Grant number 5F32AT001144-02 from the National Center for Complementary and Alternative Medicine and the Burdette-Kunkel Award from the Walther Cancer Institute. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the National Center for Complementary and Alternative Medicine, National Institutes of Health.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Burns, D.S., Azzouz, F., Sledge, R. et al. Music imagery for adults with acute leukemia in protective environments: a feasibility study. Support Care Cancer 16, 507–513 (2008). https://doi.org/10.1007/s00520-007-0330-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00520-007-0330-z