
Abstract
Studies about the role of urban characteristics in modifying the health effect of temperature extremes are still unclear. This study is aimed at quantifying the morbidity risk of infectious diarrhea attributable to temperature extremes and the modified effect of a range of city-specific indicators. Distributed lag non-linear model and multivariate meta-regression were applied to estimate fractions of infectious diarrhea morbidity attributable to temperature extremes and to explore the effect modification of city-level characteristics. Extreme heat- and extreme cold-related infectious diarrhea amounted to 0.99% (95% CI: 0.57–1.29) and 1.05% (95% CI: 0.64–1.24) of the total cases, respectively. The attributable fraction of temperature extremes on infectious diarrhea varied between southern and northern China. Several city characteristics modified the association of extreme cold with infectious diarrhea, with a higher morbidity impact related to increased water consumption per capita and decreased latitude. Regions with higher levels of latitude or GDP per capita appeared to be more sensitive to extreme hot. In conclusion, exposure to temperature extremes was associated with increased risks of infectious diarrhea and the effect can be modified by urban characteristics. This finding can inform public health interventions to decrease the adverse effects of temperature extremes on infectious diarrhea.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Infectious diarrhea remains a significant cause of morbidity and mortality around the world. Globally, diarrhea diseases account for more than 1.6 million deaths in 2016 (Troeger et al. 2018). In China, diarrhea other than dysentery, cholera, typhoid, and paratyphoid is grouped as “other infectious diarrhea (OID)” in the National Notifiable Diseases Surveillance System (NNDSS), which is listed as a Class C notifiable infectious disease (Zheng et al. 2022). OID is one of the most common infectious diseases in China, and there were more than 1.28 million new cases reported in 2018 (DCFPH (Data Center for Public Health in China) 2018). Thus, it is critical to identify diarrhea-related risk factors.
Climate change is inextricably linked to health. In recent years, many epidemiological studies have shown evidence that meteorological factors, especially ambient temperatures, play an important role in the prevalence of infectious diarrhea (Hao et al. 2019). Temperature changes may affect the reproduction and extrinsic incubation period of diarrhea pathogens and even promote the emergence of new pathogens with large spatiotemporal variation (Alemayehu et al. 2020). However, the association between extreme temperatures and health outcomes and their relative importance remains controversial (Kephart et al. 2022). IPCC predicted that intensity and frequency of temperature extremes would increase during the 21st century (Tollefson 2021). Extreme weather may directly cause death and potentially change the dynamics of infectious diseases by impacting pathogens, hosts, transmission routes, and their living environmental and social conditions (Wu et al. 2016).
Previous studies have quantified the association between extreme temperatures and diarrhea disease in terms of relative risk (RR), but few have given a comparative assessment of the attributable burden (Wu et al. 2014). Measures of attributable risk are essential for the planning of public health interventions. The quantified attributable burden can help to understand how extreme temperatures affects human health and how its influence can be reduced (Pascal et al. 2018). Assessing the relative attributable risk of temperature extremes can be conductive to better understand the potential benefits of public health interventions and to allocate health care resources. Moreover, relatively little research has investigated the effect modification of urban characteristics on the morbidity burden of diarrhea diseases attributable to extreme temperatures. To fill this gap, we quantified the morbidity burden of OID attributable to temperature extremes based on national surveillance data in 16 Chinese cities during 2014−2016, and we further investigated the effect modifications of different urban characteristics on the morbidity burden of infectious diarrhea attributable to temperature extremes.
Materials and methods
Study design
According to surveillance data from China, the newly reported OID cases accounted for 86.20% of the total cases of infectious diarrhea in mainland China from 2014 to 2016 (DCFPH (Data Center for Public Health in China) 2016). Thus, OID is crucial for the control and prevention of infectious diarrhea. We collected time-series daily data of OID cases and meteorological variables from 16 cities in China (2014−2016). We chose daily mean temperature as the exposure index computed as the 24 h average based on hourly measurements from 16 national basic meteorological monitoring stations. We did a sensitivity analysis by modifying the modeling choices, changing the degrees of freedom (df) of temperature, the maximum lag days, and time, respectively. The appendix contains further information on data collection and results from the sensitivity analysis.
Study areas
The study period was from 2014 to 2016. We selected 16 cities in China shown in Fig. 1 as the basis of our analyses, with eight southern cities (Hefei, Shanghai, Chengdu, Wuhan, Hangzhou, Changsha, Fuzhou, and Guangzhou) and eight northern cities (Shenyang, Tianjin, Yinchuan, Shijiazhuang, Taiyuan, Jinan, Lanzhou, and Xi’an). The southern and northern cities were divided by the Qinling Mountain and Huai River (Yang et al. 2016). We chose the 16 cities for the following reasons: (1) these 16 capital cities were the representative cities of the corresponding provincial administrative regions, which basically capture the diversity of climates conditions in China; (2) an inclusion criterion of cumulative number of OID cases > 5000 was adopted to ensure sufficient statistical power; (3) the selected cities had relatively good sanitary conditions, and the possibility of under-reporting of infectious diseases was low.

Locations of the 16 Chinese cities in this study
Data collection
For each city, data on daily OID cases during 2014−2016 were obtained from the National Center for Disease Control and Prevention of China. All OID cases included in this study were diagnosed by serological test confirmation or clinical symptoms. According to the diagnostic criteria published by the Ministry of Health of the People’s Republic of China (WS271-2007), a clinically diagnosed OID is defined as loose or watery stools more than three times per day (Zheng et al. 2022). OID is categorized as category C notifiable infectious diseases in China. According to the National Communicable Disease Control Act, doctors in hospital or clinic must report each OID case to local health departments, and then these cases are mandatory to be reported online to the higher levels of the system through the NNDSS within 24 hours (Zhang et al. 2019).
Daily meteorological variables in the 16 cities over the same period were collected from the China Meteorological Data Sharing Service System (http://data.cma.gov.cn/), including mean temperature, relative humidity, and rainfall. The missing values of meteorological data are interpolated using the average of the adjacent three days. Socio-economic and urban development variables of the 16 cities were collected from the statistical yearbooks of each city. The greenness in specified area is measured by the Normalized Difference Vegetation Index (NDVI) in which higher values indicating a higher density of green vegetation. The monthly NDVI data with a 1 km spatial resolution were obtained from the Data Center for Resources and Environmental Sciences of the Chinese Academy of Sciences (http://www.resdc.cn). The monthly 1 km NDVI for each city was calculated using the maximum synthesis method based on the 1 km vegetation index data from SPOT/VEGETATION PROBA-V 1 KM PRODUCTS (http://www.vito-eodata.be). The city-specific NDVI was calculated as the average of monthly NDVI values (with a spatial resolution of 1 km) during the study period.
Statistical methods
Temperature percentile-morbidity relationship cumulated over 30 days
In the first stage, a distributed lag non-linear model (DLNM) combined with quasi-Poisson regression was used to investigate the temperature-morbidity relationship in each city. DLNM could simultaneously estimate the nonlinear exposure-response association and lag-response association through a cross-basis function (Gasparrini et al. 2010). The model was as follows:
where Yt denotes the daily case number of OID on day t and β is the intercept. According to the incubation periods of OID, the maximum lag time was set to 30 days to capture the lag structure of temperature effect (Zheng et al. 2022). cb(TP) represents a cross-basis function of temperature percentiles composed of a natural cubic spline with 4 df for the temperature dimension, and a natural cubic spline with 3 df for the lag dimension. Natural cubic splines (ns) with 3 df for daily relative humidity and cumulative precipitation were included in the model to adjust for their confounding effect. Long-term trend and seasonality were controlled using a natural cubic spline of calendar time with 8 df per year (Gasparrini et al. 2015). The first-order lagged item of the model residual error lag (res, 1) was included to control the autocorrelation (Bhaskaran et al. 2013). Given the temperature ranges of different cities vary widely in our study, we used a relative scale measurement of temperature to convert temperatures into the related city-specific percentiles, so as to unify the temperature ranges across cities (Wang et al. 2021). The daily temperature percentile for each city was calculated using the temperature values of that city during the study period, and the 50th percentile of ambient temperatures was defined as the reference.
Estimation of morbidity burden attributable to temperature extremes
In the second stage, a multivariate meta-analysis was conducted to obtain the pooled exposure-response relationship between temperatures and OID morbidity in 16 China cities (Gasparrini and Armstrong 2013). We obtained the best linear unbiased prediction (BLUP) for the city-specific effect estimates (Gasparrini et al. 2012). The BLUP is a weighted average between the city-specific association estimated in the first stage and the pooled association, where the weight is inversely proportional to the variance of the first stage estimates (Kim et al. 2019). In brief, the BLUP approach allows the cities that has lower number of cases to borrow information from cities with larger populations. Extreme heat and extreme cold were defined as temperatures above the 97.5th and below the 2.5th percentiles of city-specific temperatures, respectively (Yang et al. 2016). Referring to a procedure developed by Gasparinni et al., we calculated the city-specific attributable fractions (AF%, in percentage) of temperature extremes using a forward perspective (Gasparrini et al. 2015). In brief, the number of OID cases attributable to temperature extremes by summing the temperature-related cases occurring in days with temperature extremes, and then dividing by the total number of cases produced the AF%. We calculated empirical confidence intervals using Monte Carlo simulations, assuming a multivariate normal distribution of the first-stage reduced coefficients.
Association between urban characteristics and attributable fraction of temperature extremes
The possible nonlinear association between each urban characteristic and morbidity burden attributable to extreme heat and extreme cold was investigated by fitting two separate multilevel meta-regression models with two levels (cities nested within regions) using urban characteristic as exposure and annual average temperatures as covariate (Sera et al. 2019; Sera et al. 2021). The inclusion of region as a random effect allowed the two-level meta-regression model to account for region differences. Associations between the urban characteristics and extreme temperature-related AF% were expressed as the AF% change for a standard deviation increase of the indicators.
R software (version 3.5.3) with the dlnm, mvmeta, and mixmeta packages were used for data analysis. We chose 0.05 (two-tailed) as our statistically significant level.
Results
Table 1 shows the descriptive statistics from 16 large Chinese cities. A total of 471,871 OID cases occurred during the study period. The daily mean OID cases ranged from 5 to 98 in study cities. Different cities experienced a wide range of temperatures, with city-specific annual mean temperature ranged from 8.1°C in Lanzhou to 22.0°C in Guangzhou.
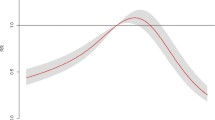
Figure 2 presents the pooled associations between temperature percentiles and OID incidence in different geographical regions cumulated over 30 days. Results indicate that high temperatures significantly enhanced the risk of OID in northern China, with the peak RR of 2.20 (95% CI: 1.43, 3.37) at the 84th percentile of ambient temperatures. This suggests a possible “harvesting effect” for extreme high temperatures. By contrast, the risk of OID generally escalated quickly and linearly in southern China on cold days, with the highest RR of 2.58 (95% CI: 1.55, 4.30) at the 0th percentile of ambient temperatures.

Meta-pooled cumulative effects between temperatures percentiles and OID morbidity in different geographical regions
Figure 3 shows the estimated attributable fraction related to temperature extremes in each city. Our findings show that the attributable fraction of temperature extremes varied among different regions. Extreme heat was responsible for a higher morbidity burden of OID in northern region of China, whereas the attributable fraction of OID cases caused by extreme cold was higher than extreme heat in most southern cities. In total, we estimated that 0.99% (95% CI: 0.57, 1.29) and 1.05% (95% CI: 0.64, 1.24) of the OID morbidity were attributable to extreme heat and extreme cold, respectively (Table S1).

Fraction of OID morbidity attributable to temperature extremes in 16 Chinese cities
After adjusting for annual mean temperatures, the association between urban characteristics and extreme temperature-related AF% is depicted in Fig. 4. We found that extreme cold-related AF% was negatively associated with latitude and longitude, whereas it was positively correlated with water consumption per capita and NDVI in winter. Cities with higher levels of latitude or GDP per capita appeared to be more sensitive to extreme hot exposure.

The relationship between urban characteristics and the AF% of temperature extremes
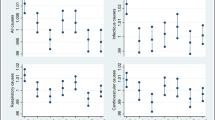
A linear association of latitude and temperature extremes AF% was observed in our study (Fig. 5). The association between extreme cold and longitude was an approximately V-shape, with a maximum AF% difference of 0.08 (95% CI: 0.03, 0.13) at 123 degrees East. We also found that the extreme cold AF% increased by water consumption per capita, and the maximum change was 1.76 (95% CI: 0.41, 3.11) at 256.56 m3 per person. The association between extreme cold AF% and NDVI in winter was an inverted V-shape curve, with the AF% rising to a peak when NDVI value was 0.37, then having a decreasing trend. A similar non-linear relationship was found for extreme heat AF% and GDP per capita.

Associations between urban characteristics and the AF% due to temperature extremes
The model residuals were approximately independent over time and following the normal distribution (Fig. S1 and Fig. S2). Sensitive analyses showed that the estimates of attributable fractions attributable to temperature extremes were broadly similar when we changed the maximum lag days, the df for temperatures and the df for time trend (Table S2). The shapes of association between temperature percentiles and morbidity remained robust when we change the maximum lag days (Fig. S3).
Discussion
We conducted a multi-site time-series analysis of 16 large cities in China on the attributable fraction of temperature extremes on infectious diarrhea morbidity and how urban characteristics affect vulnerability to temperature extremes. Results showed that most of the morbidity burden was attributable to the contribution of cold days in the south and hot days in the north. This study also reveals that the morbidity burden of infectious diarrhea contributed by extreme temperatures can be modified by varies urban characteristics. Our findings are helpful for increasing public health awareness about the adverse effects of temperature extremes on infectious diarrhea.
In line with previous studies, we found temperature extremes increased the morbidity risk of infectious diarrhea, and extremes cold and extreme heat were responsible for 0.99% and 1.05% of OID morbidity, respectively. A review study revealed that most identified studies support positive relationship between extreme heat and diarrhea (Uibel et al. 2022). Another study found maximum temperature contributed 52% and 63% in predicting the morbidity of diarrhea disease for children and older adult groups, respectively (Chou et al. 2010). Alternatively, Hasan et al. showed that suitable cold temperatures for an extended time could accelerate the onset and intensity of Rotavirus Diarrhea (Hasan et al. 2018). A study in Hongkong, China, showed the adjusted relative risk for gastrointestinal infection admissions increased about 2% per unit increase in the number of cold days (Chong et al. 2021). Several underlying mechanisms have been postulated for the increased risk of diarrhea associated with temperature extremes. One main potential mechanism leading to extreme heat-related cases is that hot temperatures may promote the proliferation and survival of diarrhea pathogens, such as Salmonella and Escherichia coli (Wang et al. 2018a). Moreover, increased consumption of unsanitary water and raw food during hot days may account for the increased risk of infection (Wang et al. 2021). Rotavirus is a common diarrhea pathogens during cold days, and extreme cold may promote the fecal-oral transmission of Rotavirus (Chong et al. 2021). In addition, people tend to spend more time indoors in cold weather and thus may lead to higher exposure to contaminated surfaces, air, food, and water for vulnerable groups (Wang et al. 2018b).
A linear increasing trend of RR was observed at low temperature percentiles in the southern region, reflecting the potential risk of extreme cold in a climate change perspective. Research on the relationship between human health and ambient temperatures was mainly focused on the effects of extreme heat in the context of global warming (Gasparrini et al. 2015). Our findings indicate that public health plans and adaptive measures should be extended and refocused to reducing the morbidity burden of cold temperature-related infectious diarrhea in southern regions.
We found that temperature extremes are responsible for excess morbidity of OID, with important differences between cities. Generally, the southern cities are characterized by relatively stronger attributable risk of extreme cold on OID, whereas extreme heat-related burden was higher in norther cities. This result was consistent with previous studies. A Swedish study suggests that northern populations have not adapted to the heat as have been done for cold (Rocklöv and Forsberg 2008). Additionally, people in warmer regions tend to have higher thermal thresholds, the temperature at which the harmful effects of heat begins to occur, suggesting acclimatization (Huang et al. 2011). Our study also illustrates that there is a negative association between longitude and extreme cold-related AF%. Previous studies have shown modification effects of longitude on the temperatures-health impacts (Tian et al. 2019; Guo et al. 2016). The geographical latitude and longitude are closely linked to weather types. As a vast country with substantial geographic variations in China, there are various climatic features in China. This suggested that the great geographical diversity should be taken into account when quantifying the health impacts of temperature extremes at the country level.
In our study, the impact of extreme heat was higher in more developed cities characterized by a higher GDP per capita, which is similar to the findings of previous studies (Tan et al. 2010; Sera et al. 2019). China has experienced rapid urban development in recent decades, the continued urbanization and increased anthropogenic activities have significantly altered the atmospheric and surface properties of the Earth, and have thus altered the urban energy balance and affected the thermal environment in cities (Yang et al. 2019). As a result, there is a distinct temperature difference between urban areas and their surrounding hinterland due to the heat storage capacity of the built environment, a phenomenon known as the urban heat island effect (Sera et al. 2019). Previous studies have shown that the urban heat island effect may greatly increase the energy consumption during summer months and lead to increased heat stress and heat health risks for residents (Vargo et al. 2016; Cui et al. 2017). Moreover, the accessibility of extreme heat protection measures may also contribute to these differences (Li et al. 2014). This result may imply that preparedness of the health system for extreme heat temperatures should be improved, particularly given the projected increases in heat extremes events related to global warming and growing urbanization in the future (Filho et al. 2019).
The results showed that the extreme cold-related attributable risks increased with the water consumption per capita. This could be due to drinking contaminated water during cold days. Therefore, water quality monitoring in areas with high water consumption should be strengthened in winter. Our results also indicated that extreme cold-related AF% was positively correlated with NDVI value in winter. The was similar to the results from a study in China, which found that the ratio of relative risk for the highest to lowest quartiles of greenness for mortality risk on extreme cold days was 2.08 (95% CI: 0.12, 36.2) among old adults in China (Qiu et al. 2021). Interestingly, we also observed an inverted V-shaped curve on the association between NDVI in winter and extreme cold-related attributable risk, with higher greenness exposure could alleviate the attributable risk when NDVI value above 0.37. The plausible mechanism supporting this result remains unclear, but some studies revealed that increasing level of greenness might be one of the good strategies to alleviate adverse effects of non-optimum temperature, including increased physical and social activity as well as mental health and well-being (Qiu et al. 2021; Denpetkul and Phosri 2021). There is a dearth of literature on the quantitative relationship between greenness and extreme cold worldwide, and thus the complex relationship between greenness and cold temperature effects warrants further investigation.
Our analysis has two main strengths. To our best knowledge, this is the first multicity study to estimate the attributable risk of infectious diarrhea due to temperature extremes in China. The observed north-south differences have important implication for the planning of public-health interventions and to protect the vulnerable populations. Additionally, we further investigated the potential effect modification of various urban characteristics on the association between OID and temperature extremes, and evidence from this study can help inform public health practices and urban planning under a variety of climate change and urban development scenarios.
Several limitations of our study should be noted. First, people often spent more time indoors during extreme weather conditions, leading to underestimating the true morbidity burden of temperature extremes on infectious diarrhea. Second, our study did not further analyze the effects of temperature extremes on different OID pathogens due to the unavailable data. Surveillance efforts for diarrheal pathogens are needed in future study to verify the effect of different etiological factors on infectious diarrhea. Third, the OID cases obtained from NDSS may not cover all cases since some people with mild clinical symptoms may not seek help in hospitals or clinics. Fourth, infectious diarrhea includes dysentery, cholera, typhoid, and paratyphoid and OID in China. For limitations by data accessibility, only OID cases in 16 cities were included in this study, and the findings need to be further validated by studies with wider coverage and more comprehensive infectious diarrhea data.
Conclusion
In conclusion, we found that temperature extremes are an important cause of the excess incidence of infectious diarrhea and the effect can be modified by urban characteristics. Our findings can provide a practical reference for the prevention of infectious diarrhea under temperature extremes conditions in China.
Data availability
The data that support the findings of this study are available from the Chinese Center for Disease Control and Prevention, but restrictions apply to the availability of these data, which were used under license for the current study and so are not publicly available. Data are however available from the authors upon reasonable request and with permission of Chinese Center for Disease Control and Prevention.
References
Alemayehu B, Ayele BT, Melak F, Ambelu A (2020) Exploring the association between childhood diarrhea and meteorological factors in Southwestern Ethiopia. Sci Total Environ 741:140189. https://doi.org/10.1016/j.scitotenv.2020.140189
Bhaskaran K, Gasparrini A, Hajat S, Smeeth L, Armstrong B (2013) Time series regression studies in environmental epidemiology. Int J Epidemiol 42(4):1187–1195. https://doi.org/10.1093/ije/dyt092
Chong KC, Chan EYY, Lee TC, Kwok KL, Lau SYF, Wang P et al (2021) A 21-year retrospective analysis of environmental impacts on paediatric acute gastroenteritis in an affluent setting. Sci Total Environ 764:142845. https://doi.org/10.1016/j.scitotenv.2020.142845
Chou W, Wu J, Wang Y, Huang H, Sung F, Chuang C (2010) Modeling the impact of climate variability on diarrhea-associated diseases in Taiwan (1996–2007). Sci Total Environ 409:43–51. https://doi.org/10.1016/j.scitotenv.2010.09.001
Cui Y, Yan D, Hong T, Ma J (2017) Temporal and spatial characteristics of the urban heat island in Beijing and the impact on building design and energy performance. Energy 130:286–297. https://doi.org/10.1016/j.energy.2017.04.053
DCFPH (Data Center for Public Health in China), 2016. National Notifiable Infectious Disease Database. http://www.phsciencedata.cn/Share/kysjml.jsp. Accessed date: 4th March 2022.
DCFPH (Data Center for Public Health in China), 2018. National Notifiable Infectious Disease Database http://www.phsciencedata.cn/Share/kysjml.jsp, Accessed date: 4th March 2022.
Denpetkul T, Phosri A (2021) Daily ambient temperature and mortality in Thailand: estimated effects, attributable risks, and effect modifications by greenness. Sci Total Environ 791:148373. https://doi.org/10.1016/j.scitotenv.2021.148373
Filho WL, Balogun AL, Olayide OE, Azeiteiro UM, Ayal DY, Muñoz PDC et al (2019) Assessing the impacts of climate change in cities and their adaptive capacity: Towards transformative approaches to climate change adaptation and poverty reduction in urban areas in a set of developing countries. Sci Total Environ 692:1175–1190. https://doi.org/10.1016/j.scitotenv.2019.07.227
Gasparrini A, Armstrong B, Kenward MG (2010) Distributed lag non-linear models. Stat Med 29(21):2224–2234. https://doi.org/10.1002/sim.3940
Gasparrini A, Armstrong B, Kenward MG (2012) Multivariate meta-analysis for non-linear and other multi-parameter associations. Stat Med 31(29):3821–3839. https://doi.org/10.1002/sim.5471
Gasparrini A, Armstrong B (2013) Reducing and meta-analysing estimates from distributed lag non-linear models. BMC Med Res Methodol 13:1. https://doi.org/10.1186/1471-2288-13-1
Gasparrini A, Guo Y, Hashizume M, Lavigne E, Zanobetti A, Schwartz J et al (2015) Mortality risk attributable to high and low ambient temperature: a multicountry observational study. Lancet 386:369–375. https://doi.org/10.1016/S0140-6736(14)62114-0
Guo C, Yang J, Guo Y, Ou QQ, Shen SQ, Ou CQ et al (2016) Short-term effects of meteorological factors on pediatric hand, foot, and mouth disease in Guangdong, China: a multi-city time-series analysis. BMC Infect Dis 16(1):524. https://doi.org/10.1186/s12879-016-1846-y
Hao Y, Liao W, Ma W, Zhang J, Zhang N, Zhong S et al (2019) Effects of ambient temperature on bacillary dysentery: a multi-city analysis in Anhui Province, China. Sci Total Environ 671:1206–1213. https://doi.org/10.1016/j.scitotenv.2019.03.443
Hasan MA, Mouw C, Jutla A, Akanda AS (2018) Quantification of rotavirus diarrheal risk due to hydroclimatic extremes over South Asia: prospects of satellite-based observations in detecting outbreaks. Geohealth 2:70–86. https://doi.org/10.1002/2017GH000101
Huang C, Barnett AG, Wang X, Vaneckova P, FitzGerald G, Tong S (2011) Projecting future heat-related mortality under climate change scenarios: a systematic review. Environ Health Perspect 119:1681–1690. https://doi.org/10.1289/ehp.1103456
Kim Y, Kim H, Gasparrini A, Armstrong B, Honda Y, Chung Y (2019) Suicide and ambient temperature: a multi-country multi-city study. Environ Health Perspect 127(11):117007. https://doi.org/10.1289/EHP4898
Kephart JL, Sánchez BN, Moore J, Schinasi LH, Bakhtsiyarava M, Ju Y (2022) City-level impact of extreme temperatures and mortality in Latin America. Nat Med 28(8):1700–1705. https://doi.org/10.1038/s41591-022-01872-6
Li Y, Lan L, Wang Y, Yang C, Tang W, Cui G et al (2014) Extremely cold and hot temperatures increase the risk of diabetes mortality in metropolitan areas of two Chinese cities. Environ Res 134:91–97. https://doi.org/10.1016/j.envres.2014.06.022
Pascal M, Wagner V, Corso M, Laaidi K, Ung A, Beaudeau P (2018) Heat and cold related-mortality in 18 French cities. Environ Int 121(Pt 1):189–198. https://doi.org/10.1016/j.envint.2018.08.049
Qiu C, Ji JS, Bell ML (2021) Effect modification of greenness on temperature-mortality relationship among older adults: a case-crossover study in China. Environ Res 197:111112. https://doi.org/10.1016/j.envres.2021.111112
Rocklöv J, Forsberg B (2008) The effect of temperature on mortality in Stockholm 1998--2003: a study of lag structures and heatwave effects. Scand J Public Health 36(5):516-523. https://doi.org/10.1177/1403494807088458
Sera F, Armstrong B, Tobias A, Vicedo-Cabrera AM, Åström C, Bell ML et al (2019) How urban characteristics affect vulnerability to heat and cold: a multi-country analysis. Int J Epidemiol 48:1101–1112. https://doi.org/10.1093/ije/dyz008
Sera F, Armstrong B, Abbott S, Meakin S, O'Reilly K, von Borries R et al (2021) A cross-sectional analysis of meteorological factors and SARS-CoV-2 transmission in 409 cities across 26 countries. Nat Commun 12(1):5968. https://doi.org/10.1038/s41467-021-25914-8
Tan J, Zheng Y, Tang X, Guo C, Li L, Song G et al (2010) The urban heat island and its impact on heat waves and human health in Shanghai. Int J Biometeorol 54:75–84. https://doi.org/10.1007/s00484-009-0256-x
Tian Y, Liu H, Si Y, Cao Y, Song J, Li M et al (2019) Association between temperature variability and daily hospital admissions for cause-specific cardiovascular disease in urban China: a national time-series study. PLoS Med 16(1):e1002738. https://doi.org/10.1371/journal.pmed.1002738
Tollefson J (2021) IPCC climate report: Earth is warmer than it’s been in 125,000 years. Nature 596(7871):171–172. https://doi.org/10.1038/d41586-021-02179-1
Troeger C, Blacker BF, Khalil IA, Rao PC, Cao S, Zimsen SR et al (2018) Estimates of the global, regional, and national morbidity, mortality, and aetiologies of diarrhoea in 195 countries: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Infect Dis 18:1211–1228. https://doi.org/10.1016/S1473-3099(18)30362-1
Uibel D, Sharma R, Piontkowski D, Sheffield PE, Clougherty JE (2022) Association of ambient extreme heat with pediatric morbidity: a scoping review. Int J Biometeorol 66(8):1683–1698. https://doi.org/10.1007/s00484-022-02310-5
Vargo J, Stone B, Habeeb D, Liu P, Russell A (2016) The social and spatial distribution of temperature-related health impacts from urban heat island reduction policies. Environ Sci Policy 66:366–374. https://doi.org/10.1016/j.envsci.2016.08.012
Wang H, Liu Z, Xiang J, Tong MX, Lao J, Liu Y et al (2021) Effect of ambient temperatures on category C notifiable infectious diarrhea in China: an analysis of national surveillance data. Sci Total Environ 759:143557. https://doi.org/10.1016/j.scitotenv.2020.143557
Wang P, Goggins WB, Chan EYY (2018a) Associations of Salmonella hospitalizations with ambient temperature, humidity and rainfall in Hong Kong. Environ Int 120:223–230. https://doi.org/10.1016/j.envint.2018.08.014
Wang P, Goggins WB, Chan EYY (2018b) A time-series study of the association of rainfall, relative humidity and ambient temperature with hospitalizations for rotavirus and norovirus infection among children in Hong Kong. Sci Total Environ 643:414–422. https://doi.org/10.1016/j.scitotenv.2018.06.189
Wu J, Yunus M, Streatfield PK, Emch M (2014) Association of climate variability and childhood diarrhoeal disease in rural Bangladesh, 2000–2006. Epidemiol Infect 142:1859–1868. https://doi.org/10.1017/S095026881300277X
Wu X, Lu Y, Zhou S, Chen L, Xu B (2016) Impact of climate change on human infectious diseases: empirical evidence and human adaptation. Environ Int 86:14–23. https://doi.org/10.1016/j.envint.2015.09.007
Yang J, Yin P, Zhou M, Ou C, Li M, Li J et al (2016) The burden of stroke mortality attributable to cold and hot ambient temperatures: epidemiological evidence from China. Environ Int 92-93:232–238. https://doi.org/10.1016/j.envint.2016.04.001
Yang Q, Huang X, Tang Q (2019) The footprint of urban heat island effect in 302 Chinese cities: temporal trends and associated factors. Sci Total Environ 655:652–662. https://doi.org/10.1016/j.scitotenv.2018.11.171
Zhang N, Song D, Zhang J, Liao W, Miao K, Zhong S et al (2019) The impact of the 2016 flood event in Anhui Province, China on infectious diarrhea disease: an interrupted time-series study. Environ Int 127:801–809. https://doi.org/10.1016/j.envint.2019.03.063
Zheng H, Wang Q, Fu J, Ding Z, Cheng J, Xu Z et al (2022) Geographical variation in the effect of ambient temperature on infectious diarrhea among children under 5 years. Environ Res 216:114491. https://doi.org/10.1016/j.envres.2022.114491
Acknowledgements
We would like to thank Chinese Center for Disease Control and Prevention, National Meteorological Information Center of China, for sharing the data needed for this study.
Funding
This study was supported by the Special Foundation of Basic Science and Technology Resources Survey of Chinese Ministry of Science and Technology (No. 2017FY101202), the Natural Science Foundation of Shandong Province in China (ZR2021QH318), and the Shandong Excellent Young Scientists Fund Program (Overseas) (2022HWYQ-055).
Author information
Authors and Affiliations
Contributions
Data analysis and writing of the first draft of the manuscript were performed by Haitao Wang. Baofa Jiang and Qi Zhao provided assistance for data acquisition and data analysis. Chengchao Zhou and We Ma participated in the coordination of the study and reviewed the manuscript. All authors commented on previous versions of the manuscript and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval
Ethical approval for the analysis of this de-identified data was granted by the Ethics Review Committee, School of Public Health, Shandong University (20190402).
Conflict of interest
The authors declare no competing interests.
Supplementary information
ESM 1
(DOCX 3361 kb)
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Wang, H., Jiang, B., Zhao, Q. et al. Temperature extremes and infectious diarrhea in China: attributable risks and effect modification of urban characteristics. Int J Biometeorol 67, 1659–1668 (2023). https://doi.org/10.1007/s00484-023-02528-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00484-023-02528-x