
Abstract
Previous studies have explored the effect between ambient temperature and infectious diarrhea (ID) mostly using relative risk, which provides limited information in practical applications. Few studies have focused on the disease burden of ID caused by temperature, especially for different subgroups and cities in a multi-city setting. This study aims to estimate the effects and attributable risks of temperature on category C ID and explore potential modifiers among various cities in Guangdong. First, distributed lag non-linear models (DLNMs) were used to explore city-specific associations between daily mean temperature and category C ID from 2014 to 2016 in Guangdong and pooled by applying multivariate meta-analysis. Then, multivariate meta-regression was implemented to analyze the potential heterogeneity among various cities. Finally, we assessed the attributable burden of category C ID due to temperature, low (below the 5th percentile of temperature) and high temperature (above the 95th percentile of temperature) for each city and subgroup population. Compared with the 50th percentile of daily mean temperature, adverse effects on category C ID were found when the temperature was lower than 12.27 ℃ in Guangdong Province. Some city-specific factors (longitude, urbanization rate, population density, disposable income per capita, and the number of medical technicians and beds per thousand persons) could modify the relationship of temperature-category C ID. During the study period, there were 60,505 category C ID cases (17.14% of total cases) attributable to the exposure of temperature, with the attributable fraction (AF) of low temperature (4.23%, 95% empirical confidence interval (eCI): 1.79–5.71%) higher than high temperature (1.34%, 95% eCI: 0.86–1.64%). Males, people under 5 years, and workers appeared to be more vulnerable to temperature, with AFs of 29.40%, 19.25%, and 21.49%, respectively. The AF varied substantially at the city level, with the largest AF of low temperature occurring in Shaoguan (9.58%, 95% eCI: 8.36–10.09%), and that of high temperature occurring in Shenzhen (3.16%, 95% eCI: 2.70–3.51%). Low temperature was an important risk factor for category C ID in Guangdong Province, China. The exposure–response relationship could be modified by city-specific characteristics. Considering the whole population, the attributable risk of low temperature was much higher than that of high temperature, and males, people under 5 years, and workers were vulnerable populations.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Infectious diarrhea (ID) is a group of intestinal infectious diseases caused by various pathogenic microorganisms (including bacteria, viruses, and parasites) and their products, with diarrhea as the main symptom (Kelly 2019). It remains a severe public health issue, with an estimated 1.7 billion morbidities and 1.4–1.9 million diarrhea-related deaths annually worldwide (Leung et al. 2016; Levy et al. 2016). In China, a total of 20,518,684 ID cases were detected during the ten years from 2004 to 2013 (Yang et al. 2017). To facilitate the management of ID, ID not caused by cholera, dysentery, typhoid, and paratyphoid is defined as other infectious diarrhea (OID) and classified into category C notifiable infectious diseases (Yang et al. 2017). In 2014 and 2015, 867,545 and 937,616 OID cases were reported respectively in China, with incidences ranging from 3.8 to 506.7 per 100,000 people at the provincial level (Zhang and Zhang 2017). Meanwhile, the problem is particularly acute in Guangdong Province. According to the Announcement of Infectious Diseases of the Chinese Public Health Science Data Center (https://www.phsciencedata.cn/), Guangdong has been the province with the most of OID cases annually from 2009 to 2016, and the number continues to rise rapidly.
Climate change, the fluctuation of weather conditions over a long period of time, has been considered one of the greatest threats to human health in the twenty-first century (Khan et al. 2019; WHO 2018). Evidences showed that climate change can affect the distribution and survival of vectors, and the physiological functions and immune statuses of the human body to a certain extent, thereby changing the incidence and prevalence of infectious diseases (Barrett et al. 2015; Wei et al. 2014). The outbreak, emergence, and re-emergence of infectious diarrheal diseases are strongly affected by climate change, and it is estimated that between 2030 and 2050, 48,000 people will die from diarrhea, especially in developing countries (El-Sayed &Kamel 2020, Khan et al. 2019). Some documents have proved that temperature is the main meteorological factor affecting the onset of ID (Tao et al. 2015). For instance, a multi-city study in mainland China found that there is an M-shaped relationship between temperature and OID (Wang et al. 2021). In Jinan, China, every 5 °C increase of temperature leads to a 61% increase in bacillary dysentery at lag one week, while in Guangzhou, low temperature can increase the ID count (Liu et al. 2019; Wang et al. 2019). In Tamil Nadu, India, a significantly positive correlation was found between weekly average temperature and diarrhea at lag 1–3 weeks (Mertens et al. 2019). In Cape Town, when the lowest and highest temperatures increase by 5 ℃, the count of ID of children increases by 15% and 6%, respectively, after adjusting for autocorrelation at lag one week (Musengimana et al. 2016).
However, previous studies mostly quantified the relationship of temperature-OID via relative risk (RR). Although RR is helpful for epidemiologists in determining whether connections exist between given factors and diseases, it cannot reflect the actual effects of exposures from the public health perspective (Northridge 1995). By contrast, attributable risk assessment is a method that can comprehensively consider the exposure effect and the exposure rate to assess the population attributable burden caused by risk factors (Yang et al. 2016). It represents the proportion or number of cases that can be prevented without being exposed to the specific risk factor and provides crucial information for health policymakers to formulate interventions and allocate health resources (Cheng et al. 2017).
Several studies have shown that the association between temperature and disease may vary in different cities, which could be caused by geographic, socio-economic, and other city-specific characteristics (Fu et al. 2021; Huang et al. 2015; Zhao et al. 2018). However, a detailed screening of all characteristics was lacking to explore the potential heterogeneity of temperature-OID in Guangdong Province. Furthermore, the prevalence of infectious diarrhea varies in different populations due to differences in immunity and adaptability of subgroups (Qu et al. 2012), while limited studies have compared the temperature-OID relationship and morbidity burden due to temperature among gender, age, and occupation subgroups in a multi-city setting.
To fill the above research gap, we used surveillance data of 21 prefecture-level cities to obtain the temperature-OID relationship of each subgroup in Guangdong Province. We also collected geographic, socio-economic, and health resource indicators of each city to analyze the potential heterogeneity. Finally, we estimated the disease burden for each city and subgroup to identify vulnerable regions and populations. The results will contribute to the formulation of prevention strategies and the allocation of health resources.
Methods
Study site
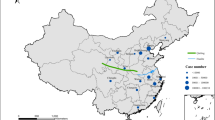
Guangdong Province (latitude 20°09′-25°31′N and longitude 109°45′-117°20′E) is located in southern China. It contains 21 prefecture-level cities with a total population of 109.99 million at the end of 2016 (https://data.cnki.net/area/Yearbook/). Guangdong Province features a subtropical monsoon climate, with sufficient light, heat, and precipitation resources each year (Wang et al. 2019). The position of Guangdong is presented in Fig. 1.

Location of Guangdong Province in China (a) and the distribution of OID cases in 21 prefecture-level cities (b). There are 21 cities in Guangdong, arranged according to the number of other infectious diarrhea (OID) cases as follows: Shenzhen, Guangzhou, Meizhou, Jiangmen, Dongguan, Foshan, Zhaoqing, Qingyuan, Zhuhai, Yangjiang, Zhongshan, Shantou, Jieyang, Maoming, Shanwei, Huizhou, Shaoguan, Zhanjiang, Heyuan, Yunfu, Chaozhou
Data collection
Daily reported OID cases in Guangdong Province from 1 January 2014 to 31 December 2016 were obtained from the Chinese Center for Disease Control and Prevention (China CDC). All OID cases were diagnosed according to the criterion (WS 271–2007) published by the Ministry of Health of the People’s Republic of China in 2007 (Wang et al. 2021). Based on the Law of National Communicable Diseases Control, OID cases must be reported within 24 h via the internet-based National Notifiable Infectious Disease Reporting Information System (NIDRIS) once diagnosed (Deng et al. 2015). The reported information consists of age, gender, occupation, onset date, and the administrative code of residence.
Daily meteorological data, including mean temperature, wind speed, relative humidity, and accumulated precipitation were collected from fixed monitoring stations in Guangdong, provided by the China Meteorological Data Sharing Service System (http://data.cma.gov.cn/). If cities had more than one weather station, we chose the station nearest to the city center. The missing meteorological data were interpolated with the average value of the five adjacent days.
We also collected city-specific characteristics between 2014 and 2016, including geographic factors (i.e., latitude and longitude), demographic characteristics (i.e., population density, urbanization rate, and primary school students per thousand persons), economic indicators (i.e., GDP and disposable income per capita), and health resource information (i.e., the number of medical technicians and beds per thousand persons) from the Guangdong Statistical Yearbook (Zhao et al. 2021). More details were given in Table A1.
Statistical analysis
We applied a two-stage time-series analysis. In the first stage, taking the median temperature of all cities as the reference, distributed lag non-linear models (DLNMs) with a quasi-Poisson distribution were used to estimate the associations of temperature-OID for 21 cities. DLNM could simultaneously describe the delayed and non-linear effects of a specific exposure, which has been confirmed to apply well in environmental epidemiology (Gasparrini et al. 2015). The model was as follows:
where \(E\left({Y}_{t}\right)\) represents the expected number of OID on day t; \(\beta\) is the intercept; and \(cb\left({Temperature}_{t,l}\right)\) denotes a cross-basis function to fit both delayed and non-linear effects of temperature. The maximum lag days l were set to 35 according to previous research (Liu et al. 2018). The \(ns\left(Humidity,3\right)+ns\left(Precipitation,3\right)+ns\left(Wind,3\right)\) were enrolled to adjust for the confounding of other meteorological variables, and the \(ns(time,7\times 3)\) was designed to control seasonality and long-term trends (Liu et al. 2020). The lagged residual error \(lag(res,1)\) was incorporated to control autocorrelation.
In the second stage, a multivariate meta-analysis was adopted to pool the city-specific effects to obtain the overall cumulative and lag effects of temperature-OID in Guangdong (Gasparrini et al. 2012). Then, meta-regression was applied to analyze the possible city-specific modifiers, and the multivariate extensions of I2 statistics and Cochran Q test were chosen to assess the residual heterogeneity (Gasparrini &Armstrong 2013). The goodness of meta-regression was evaluated by the Akaike information criterion (AIC) and Bayesian information criterion (BIC). Finally, the attributable risks (including attributable fraction, AF; and attributable number, AN) of temperatures on OID for each city and subgroup were calculated by applying the “forward perspective” within the framework of DLNM. Monte Carlo simulation was applied to calculate the 95% empirical confidence interval (eCI) as an evaluation indicator of attributable risk (Gasparrini and Leone 2014).
To identify vulnerable groups (defined by the largest AF), the whole population was stratified by gender (males and females), age (0–5, 6–19, and ≥ 20 years), and occupation (scattered and nursery children, housekeeping and unemployed, students, farmers, workers, and others consisting of teachers, herders, medical staffs, and so on). Furthermore, defining temperatures below the 5th as low temperature and higher than the 95th as high temperature in this study will be conducive to better identifying sensitive subgroups and cities.
The robustness of the model was evaluated by changing the maximum lag days (25, 30, 35, and 40), altering the 3–5 df for meteorological factors and 7–10 df for time variable, and controlling the first-order lagged residual errors or not. R 4.0.3 with packages of “dlnm” and “mvmeta” was conducted for all analyses. P < 0.05 (two-sided) was considered statistically significant.
Results
Description of meteorological and OID data
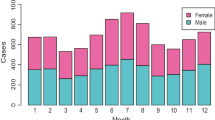
From 2014 to 2016, a total of 353,061 OID cases were notified in the 21 cities of Guangdong Province, of which 58.28% were males and 41.72% were females, with a sex ratio of 1.40:1 (Table 1). In terms of age, people under 5 years accounted for 72.70% of cases. Scattered and nursery children were the main group for occupation patients, with a proportion of 74.10%.
The OID case counts varied across the 21 cities in Guangdong. Shenzhen, Guangzhou, and Jiangmen ranked in the top three, reaching approximately 40% of the total number of cases (Fig. 1, Table A2). The time-series curves of OID and temperature showed opposite trends (Fig. 2). During the study period, the average daily mean temperature, relative humidity, precipitation, and wind speed were 22.70 °C, 79.14%, 5.38 mm, and 2.12 m/s, respectively. More descriptive information was presented in Table A2.

Time series curves of daily other infectious diarrhea (OID) and mean temperature in Guangdong, 2014–2016
Cumulative effects and lag effects of temperature on OID
Figure 3 showed the cumulative effects of temperature-OID, with an approximate L-shaped exposure–response curve over 35 lag days. The adverse effect on the whole population emerged when the temperature was lower than 12.27 ℃. An inverted V-shaped curve was presented for the lag effect of low temperature, with RR starting to be larger than 1 at lag 9 and reaching the maximum at lag 20 (RR = 1.046, 95% CI: 1.035–1.058) (Fig. A1).

Pooled cumulative effects of daily mean temperature on other infectious diarrhea (OID) in whole population and gender (males and females), age (0–5, 6–19, and ≥ 20 years), and occupation (scattered and nursery children, housekeeping and unemployed, students, farmers, workers, and others consisting of teachers, herders, medical staffs, and so on) subgroups
The accumulative risks of different subgroups were presented in Fig. 3. Compared with the total population, males and females showed similar risks under low temperatures. In terms of age, the cumulative RR of low temperature for people aged 6–19 years was higher than that for people under 5 years (RR = 1.073, 95% CI: 1.044–1.103 versus RR = 1.026, 95% CI: 1.014–1.038). For patients with different occupations, the effects of scattered and nursery children and students were significant in low temperatures, with cumulative RRs of 1.026 (95% CI: 1.015–1.038) and 1.093 (95% CI: 1.045–1.143), respectively. Furthermore, the results showed that high temperature only had adverse effects on people under 5 years and scattered and nursery children. More details were given in Table A3.
Analysis of multivariate meta-regression
The results of multivariate meta-regression (intercept-only model) displayed that the residual heterogeneity was significant (Q = 2,574.5, p < 0.001), but the heterogeneity attributed to the actual difference among 21 cities was high, with I2 statistics of 97.67% (Table 2). Several city-specific characteristics could explain partial residual heterogeneity, including longitude, population density, urbanization rate, disposable income per capita, and the number of medical technicians and beds per thousand persons.
Based on the significant city-specific characteristics in Table 2, the temperature-OID associations were predicted and reported for the 5th and 95th percentiles of modifiers in Fig. 4. In high-longitude cities, the effects of medium–low temperature (7 to 24 ℃) on OID were significantly enhanced. High temperature was associated with greater effects on OID among cities with a high urbanization rate, high population density, and high disposable income per capita. Besides, we found that cities equipped with better health resources (i.e., more medical technicians and beds) had higher risks of OID at low temperatures.

Predicted temperature-other infectious diarrhea (OID) relationships for the 5th (yellow line) and 95th (blue line) percentiles longitude, urbanization rate, population density, disposable income per capita, and the number of medical technicians and beds per thousand persons. Reference: the 50th percentile of temperature
Attributable risk assessment
During the study period, 60,505 OID cases (17.14% of the total OID case counts) were attributable to daily mean temperature, and the AF of low temperature (4.23%, 95% eCI: 1.79–5.71%) was higher than that of high temperature (1.34%, 95% eCI: 0.86–1.64%) (Table 3). The attributable risk varied substantially at the city level; Shenzhen and Dongguan had fairly high AN, with numbers of 27,133 and 8,783, respectively. The AF ranked first in low temperature was Shaoguan (9.58%, 95% eCI: 8.36–10.09%), and in high temperature, it was Shenzhen (3.16%, 95% eCI: 2.70–3.51%).
Figure 5 illustrated the AF of temperature (low and high) in different subgroups. Males, people under 5 years, and workers appeared to be more vulnerable to temperature, with AFs of 29.40%, 19.25%, and 21.49%, respectively. There were some variations for vulnerable groups under different temperature conditions: males, people under 5 years, and scattered and nursery children in low temperature while males, people under 5 years, and workers in high temperature (Table A4).

The estimated attributable risks of other infectious diarrhea (OID) due to temperature for whole population and gender (males and females), age (0–5, 6–19, and ≥ 20 years), and occupation (scattered and nursery children, housekeeping and unemployed, students, farmers, workers, and others consisting of teachers, herders, medical staffs, and so on) subgroups. Low temperature was defined as temperature below the 5th percentile of the temperature, and high temperature was defined as temperature higher than the 95th percentile of the temperature
Sensitivity analyses
After changing the df for meteorological factors and time variables, the maximum lag days, and controlling the autocorrelation or not, the pooled temperature-OID curves changed little, indicating that the model had good robustness (Figs. A2-A8).
Discussion
Climate change can change the pattern of temperature, relative humidity, and precipitation, which can directly or indirectly lead to the emergence and re-emergence of sensitive infectious diseases through the impact on pathogens, disease vectors or hosts, and the mode of transmission (Cox et al. 2012). Previous studies have found temperature changes have significantly and severely increased the prevalence of diarrheal diseases worldwide (El-Sayed and Kamel 2020). In China, the incidence of OID is increasing at an annual rate of 6.6% (Yang et al. 2017). Therefore, it is essential to explore the temperature-OID relationships and search for modifiable risk factors (i.e., modifiers among cities) within this association. In this study, the relationships and attributable risks were analyzed between daily mean temperature and OID in Guangdong, and potential effect modifiers were identified among 21 cities. To our knowledge, this is the first study that conducted a comprehensive attributable risk assessment to identify vulnerable groups and regions for OID and explored potential effect modifiers in Guangdong Province. Our research will provide decision-makers with valuable information to formulate and improve prevention strategies for targeted populations and regions.
This study detected that low temperature had an adverse effect on OID incidence, which is similar to the findings in Guangzhou, the capital of Guangdong Province (Wang et al. 2019). The mechanism by which low temperature exerted adverse effects may involve both pathogens and hosts. From the perspective of pathogens, according to the seasonal characteristics of different pathogens, OID can be classified into two main categories, including viral diarrhea (rotavirus and norovirus) prevalent in winter and bacterial diarrhea (Campylobacter jejuni, Escherichia coli, Salmonella, Vibrio parahaemolyticus) prevalent in summer and autumn (Fang et al. 2019). We found that viral diarrhea accounted for 91.64% of all biology-tested OID cases according to Guangdong data reported from 2014 to 2016. Rotavirus and norovirus are more suitable for growth and reproduction in a low-temperature environment (Carlton et al. 2016). For example, a study pointed out that norovirus presents the strongest transmission ability at 8 °C (Gao et al. 2020). Besides, a meta-analysis found that the annual incidence of rotavirus infection increases by 1.3% when the monthly average temperature decreases by 1 ℃ (Jagai et al. 2012). Furthermore, evidence from laboratory studies showed that low temperature could increase the reproduction of viruses and reduce the decay rate in the environment, thereby prolonging the survival time of viruses on the surface of contaminated objects and aquatic environments (Bozkurt et al. 2015). From the perspective of the host, people who live in subtropical zones are more vulnerable to cold and prefer to stay indoors during cold weather, which increases the probability of contacting infected people and contaminated objects (Wang et al. 2018).
It is noteworthy that high temperature caused adverse effects only in people under 5 years, and scattered and nursery children. Several studies have shown that a relatively smaller peak often appears in summer (Fang et al. 2019). This is mainly caused by bacteria because high temperature may promote the regeneration of bacteria and then increase the intake of food contaminated by bacteria (Kovats et al. 2004; Liu et al. 2020). Therefore, the mechanism of susceptibility for people under 5 years and scattered and nursery children may involve an immature immune system and bad hygiene habits, which can promote bacterial infection (Xu et al. 2013).
The results of multivariate meta-regression showed that some modifiers could explain partial residual heterogeneity among 21 cities. We found that high longitude strengthened the association between medium–low temperature and OID. To explore the mechanism of the modification effect of longitude, we further studied the topography of Guangdong. Since the mountains in southeastern Meizhou block a lot of water vapor from the South China Sea, it appears that high-longitude regions have a lower relative humidity (77.5% in Meizhou to 82.7% in Zhanjiang) (Liao et al. 2014). Lower relative humidity improves the survival rate and survival time of rotavirus, and the infectivity of rotavirus will rapidly lose when relative humidity reaches 80% (Hashizume et al. 2008).
In cities with a high urbanization rate and high population density, the relative risk of high temperature on OID was significantly increased. In the past decades, a substantial proportion of rural people and migrant workers have entered cities, leading to increases in urbanization rates and population densities. Crowded populations will increase disease transmission via direct or indirect contact (Hao et al. 2019). Moreover, people living in urban villages with poor sanitary conditions were more likely to be infected with OID (Zhang et al. 2016).
The result of effect modification analysis for disposable income per capita showed that residents of cities with high disposable income have a higher OID risk in high temperature. This may be due to the higher outpatient rate at a greater level of economic development (Qian et al. 2017). In addition, we also found that low temperature could amplify the risks of OID in cities with better medical resources. This is likely because people living in these areas tend to have a higher level of hygiene awareness, and they might incline to seek medical treatment when they had symptoms of OID.
In this study, attributable risk of the males was much greater than that of females, which might be due to the gender differences in immune levels, behavioral patterns, and occupational exposures (Anteneh et al. 2017; Sevilimedu et al. 2016). The exact mechanisms are not clear and require further research. For age subgroups, the OID burden of people under 5 years was higher, which further confirms that this age group suffers most from diarrhea worldwide (Das et al. 2014; Heaney et al. 2019). For occupation subgroups, the burden of workers far exceeded that of other subpopulations, and this susceptibility to OID is likely due to poor living and sanitary conditions. We also found that the cumulative effects of temperature-OID in low temperature and high temperature for students, farmers, workers, and others were not significant, but the AFs were significant. The possible speculation of these results may be due to the relatively small dataset, which led to the unstable fit of the effect estimates (Gasparrini et al. 2015).
The RR of temperature-OID we explored was small because the exposure of the population to temperature is broad and inconspicuous; therefore, it may not be a priority when formulating prevention strategies. However, attributable risk assessment can take into account both the adverse effect of temperature and the exposure level of the population, so it could show the actual adverse effect of temperature and identify vulnerable populations (Yang et al. 2016). For instance, although the effect of temperature-OID for males was not prominent in our study, we found that they have higher attributable risks from a public health perspective.
Several limitations should be acknowledged. First, our research was limited to Guangdong Province, so the conclusions we reached might not be applicable to other geographic regions. Second, due to the lack of information on the pathogenic composition, we could not explore the effect of temperature on different types of pathogens of OID. Third, our meteorological data were collected from fixed weather monitoring stations, which may lead to measurement biases of actual exposure levels of individuals.
Conclusions
In conclusion, this study demonstrated that low temperature could increase the incidence of OID and the associations varied slightly in subgroups. City-specific characteristics can explain partial heterogeneity among different cities. Furthermore, we found that males, people under 5 years, and workers were vulnerable groups. Therefore, corresponding prevention strategies should be actively taken to reduce the burden of OID.
References
Anteneh ZA, Andargie K, Tarekegn M (2017) Prevalence and determinants of acute diarrhea among children younger than five years old in Jabithennan District, Northwest Ethiopia, 2014. BMC Public Health 17:99. https://doi.org/10.1186/s12889-017-4021-5
Barrett B, Charles JW, Temte JL (2015) Climate change, human health, and epidemiological transition. Prev Med 70:69–75. https://doi.org/10.1016/j.ypmed.2014.11.013
Bozkurt H, D’Souza DH, Davidson PM (2015) Thermal inactivation of foodborne enteric viruses and their viral surrogates in foods. J Food Prot 78:1597–1617. https://doi.org/10.4315/0362-028X.JFP-14-487
Carlton EJ, Woster AP, DeWitt P, Goldstein RS, Levy K (2016) A systematic review and meta-analysis of ambient temperature and diarrhoeal diseases. Int J Epidemiol 45:117–130. https://doi.org/10.1093/ije/dyv296
Cheng J, Xie M, Zhao K, Wu J, Xu Z, Song J, Zhao D, Li K, Wang X, Yang H (2017) Impacts of ambient temperature on the burden of bacillary dysentery in urban and rural Hefei, China. Epidemiol Infect 145:1567–1576. https://doi.org/10.1017/S0950268817000280
Cox R, Revie CW, Sanchez J (2012) The use of expert opinion to assess the risk of emergence or re-emergence of infectious diseases in Canada associated with climate change. PLoS ONE 7:e41590. https://doi.org/10.1371/journal.pone.0041590
Das JK, Salam RA, Bhutta ZA (2014) Global burden of childhood diarrhea and interventions. Curr Opin Infect Dis 27:451–458. https://doi.org/10.1097/QCO.0000000000000096
Deng Z, Xun H, Zhou M, Jiang B, Wang S, Guo Q, Wang W, Kang R, Wang X, Marley G, Ma W (2015) Impacts of tropical cyclones and accompanying precipitation on infectious diarrhea in cyclone landing areas of Zhejiang Province, China. Int J Environ Res Public Health 12:1054–1068. https://doi.org/10.3390/ijerph120201054
El-Sayed A, Kamel M (2020) Climatic changes and their role in emergence and re-emergence of diseases. Environ Sci Pollut Res Int 27:22336–22352. https://doi.org/10.1007/s11356-020-08896-w
Fang X, Ai J, Liu W, Ji H, Zhang X, Peng Z, Wu Y, Shi Y, Shen W, Bao C (2019) Epidemiology of infectious diarrhoea and the relationship with etiological and meteorological factors in Jiangsu Province. China Scientific Reports 9:19571. https://doi.org/10.1038/s41598-019-56207-2
Fu S, Wang B, Zhou J, Xu X, Liu J, Ma Y, Li L, He X, Li S, Niu J (2021) Meteorological factors, governmental responses and COVID-19: Evidence from four European countries. Environ Res 194:110596. https://doi.org/10.1016/j.envres.2020.110596
Gao Y, Chen Y, Shi P, Zhang Q, Qian C, Xiao Y, Feng W, Shen Y, Shi C (2020) The effect of ambient temperature on infectious diarrhea and diarrhea-like illness in Wuxi, China. Disaster Med. Public Health Prep., 1-7. https://doi.org/10.1017/dmp.2020.340
Gasparrini A, Armstrong B, Kenward MG (2012) Multivariate meta-analysis for non-linear and other multi-parameter associations. Stat Med 31:3821–3839. https://doi.org/10.1002/sim.5471
Gasparrini A, Armstrong B (2013) Reducing and meta-analysing estimates from distributed lag non-linear models. BMC Med Res Methodol 13:1–10. https://doi.org/10.1186/1471-2288-13-1
Gasparrini A, Leone M (2014) Attributable risk from distributed lag models. BMC Med Res Methodol 14:1–8. https://doi.org/10.1186/1471-2288-14-55
Gasparrini A, Guo Y, Hashizume M, Lavigne E, Zanobetti A, Schwartz J, Tobias A, Tong S, Rocklöv J, Forsberg B (2015) Mortality risk attributable to high and low ambient temperature: a multicountry observational study. Lancet (london, England) 386:369–375. https://doi.org/10.1016/S0140-6736(14)62114-0
Hao Y, Liao W, Ma W, Zhang J, Zhang N, Zhong S, Wang Z, Yang L, Huang C (2019) Effects of ambient temperature on bacillary dysentery: a multi-city analysis in Anhui Province, China. The Science of the Total Environment 671:1206–1213. https://doi.org/10.1016/j.scitotenv.2019.03.443
Hashizume M, Armstrong B, Wagatsuma Y, Faruque AS, Hayashi T, Sack DA (2008) Rotavirus infections and climate variability in Dhaka, Bangladesh: a time-series analysis. Epidemiol Infect 136:1281–1289. https://doi.org/10.1017/S0950268807009776
Heaney AK, Shaman J, Alexander KA (2019) El Niño-Southern oscillation and under-5 diarrhea in Botswana. Nat Commun 10:5798. https://doi.org/10.1038/s41467-019-13584-6
Huang Z, Lin H, Liu Y, Zhou M, Liu T, Xiao J, Zeng W, Li X, Zhang Y, Ebi KL (2015) Individual-level and community-level effect modifiers of the temperature–mortality relationship in 66 Chinese communities. BMJ Open 5:e009172. https://doi.org/10.1136/bmjopen-2015-009172
Jagai JS, Sarkar R, Castronovo D, Kattula D, McEntee J, Ward H, Kang G, Naumova EN (2012) Seasonality of rotavirus in South Asia: a meta-analysis approach assessing associations with temperature, precipitation, and vegetation index. PLoS ONE 7:e38168. https://doi.org/10.1371/journal.pone.0038168
Kelly P (2019) Infectious Diarrhoea Medicine 47:341–346. https://doi.org/10.1016/j.mpmed.2019.03.004
Khan MD, Thi Vu HH, Lai QT, Ahn JW (2019): Aggravation of human diseases and climate change nexus. Int J Environ Res Public Health 16 https://doi.org/10.3390/ijerph16152799
Kovats RS, Edwards SJ, Hajat S, Armstrong BG, Ebi KL, Menne B (2004) The effect of temperature on food poisoning: a time-series analysis of salmonellosis in ten European countries. Epidemiol Infect 132:443–453. https://doi.org/10.1017/s0950268804001992
Leung DT, Chisti MJ, Pavia AT (2016) Prevention and control of childhood pneumonia and diarrhea. Pediatr Clin North Am 63:67–79. https://doi.org/10.1016/j.pcl.2015.08.003
Levy K, Woster AP, Goldstein RS, Carlton EJ (2016) Untangling the impacts of climate change on waterborne diseases: a systematic review of relationships between diarrheal diseases and temperature, rainfall, flooding, and drought. Environ Sci Technol 50:4905–4922. https://doi.org/10.1021/acs.est.5b06186
Liao Y, Li D, Zhuo M, Wei G (2014) Spatio-temporal variation and tendency of rainfall in Guangdong province during past 50 years. (in Chinese). Ecology and Environment Sciences 2:223–228. https://doi.org/10.3969/j.issn.1674-5906.2014.02.007
Liu Z, Zhang F, Zhang Y, Li J, Liu X, Ding G, Zhang C, Liu Q, Jiang B (2018) Association between floods and infectious diarrhea and their effect modifiers in Hunan province, China: a two-stage model. The Science of the Total Environment 626:630–637. https://doi.org/10.1016/j.scitotenv.2018.01.130
Liu Z, Liu Y, Zhang Y, Lao J, Zhang J, Wang H, Jiang B (2019) Effect of ambient temperature and its effect modifiers on bacillary dysentery in Jinan, China. The Science of the Total Environment 650:2980–2986. https://doi.org/10.1016/j.scitotenv.2018.10.053
Liu Z, Tong MX, Xiang J, Dear K, Wang C, Ma W, Lu L, Liu Q, Jiang B, Bi P (2020) Daily temperature and bacillary dysentery: estimated effects, attributable risks, and future disease burden in 316 Chinese cities. Environ Health Perspect 128:057008. https://doi.org/10.1289/EHP5779
Mertens A, Balakrishnan K, Ramaswamy P, Rajkumar P, Ramaprabha P, Durairaj N, Hubbard AE, Khush R, Colford JM Jr, Arnold BF (2019) Associations between high temperature, heavy rainfall, and diarrhea among young children in rural Tamil Nadu, India: a prospective cohort study. Environ Health Perspect 127:047004. https://doi.org/10.1289/EHP3711
Musengimana G, Mukinda FK, Machekano R, Mahomed H (2016) Temperature variability and occurrence of diarrhoea in children under five-years-old in Cape Town metropolitan sub-districts. Int J Environ Res Public Health 13:859. https://doi.org/10.3390/ijerph13090859
Northridge ME (1995) Public health methods–attributable risk as a link between causality and public health action. Am J Public Health 85:1202–1204. https://doi.org/10.2105/ajph.85.9.1202
Qian Y, Zhou Z, Yan J, Gao J, Wang Y, Yang X, Xu Y, Li Y (2017) An economy-ralated equity analysis of health service utilization by women in economically underdeveloped regions of western China. International Journal for Equity in Health 16:186. https://doi.org/10.1186/s12939-017-0667-y
Qu M, Deng Y, Zhang X, Liu G, Huang Y, Lin C, Li J, Yan H, Li X, Jia L, Kan B, Huang F, Wang Q (2012) Etiology of acute diarrhea due to enteropathogenic bacteria in Beijing. China J Infect 65:214–222. https://doi.org/10.1016/j.jinf.2012.04.010
Sevilimedu V, Pressley KD, Snook KR, Hogges JV, Politis MD, Sexton JK, Duke CH, Smith BA, Swander LC, Baker KK, Gambhir M, Fung IC (2016) Gender-based differences in water, sanitation and hygiene-related diarrheal disease and helminthic infections: a systematic review and meta-analysis. Trans R Soc Trop Med Hyg 110:637–648. https://doi.org/10.1093/trstmh/trw080
Tao LZ, Mi S, J S, (2015) Effects of meteorological factors on other types of infectious diarrhea. (in Chinese). Journal of Lanzhou University (natural Sciences) 51:646–651
Wang H, Di B, Zhang T, Lu Y, Chen C, Wang D, Li T, Zhang Z, Yang Z (2019) Association of meteorological factors with infectious diarrhea incidence in Guangzhou, southern China: a time-series study (2006–2017). The Science of the Total Environment 672:7–15. https://doi.org/10.1016/j.scitotenv.2019.03.330
Wang H, Liu Z, Xiang J, Tong MX, Lao J, Liu Y, Zhang J, Zhao Z, Gao Q, Jiang B (2021) Effect of ambient temperatures on category C notifiable infectious diarrhea in China: an analysis of national surveillance data. The Science of the Total Environment 759:143557. https://doi.org/10.1016/j.scitotenv.2020.143557
Wang P, Goggins WB, Chan EYY (2018) A time-series study of the association of rainfall, relative humidity and ambient temperature with hospitalizations for rotavirus and norovirus infection among children in Hong Kong. The Science of the Total Environment 643:414–422. https://doi.org/10.1016/j.scitotenv.2018.06.189
Wei J, Hansen A, Zhang Y, Li H, Liu Q, Sun Y, Xue S, Zhao S, Bi P (2014) The impact of climate change on infectious disease transmission: perceptions of CDC health professionals in Shanxi Province. China Plos One 9:e109476. https://doi.org/10.1371/journal.pone.0109476
WHO (2018) COP24 special report: health and climate change. https://www.who.int/publications/i/item/cop24-special-report-health-climate-change. Accessed 26 July 2021
Xu Z, Huang C, Turner LR, Su H, Qiao Z, Tong S (2013) Is diurnal temperature range a risk factor for childhood diarrhea? PLoS ONE 8:e64713. https://doi.org/10.1371/journal.pone.0064713
Yang J, Yin P, Zhou M, Ou C-Q, Li M, Li J, Liu X, Gao J, Liu Y, Qin R (2016) The burden of stroke mortality attributable to cold and hot ambient temperatures: epidemiological evidence from China. Environ Int 92:232–238. https://doi.org/10.1016/j.envint.2016.04.001
Yang S, Wu J, Ding C, Cui Y, Zhou Y, Li Y, Deng M, Wang C, Xu K, Ren J, Ruan B, Li L (2017) Epidemiological features of and changes in incidence of infectious diseases in China in the first decade after the SARS outbreak: an observational trend study. Lancet Infect Dis 17:716–725. https://doi.org/10.1016/S1473-3099(17)30227-X
Zhang H, Si Y, Wang X, Gong P (2016) Patterns of Bacillary Dysentery in China, 2005–2010. Int J Environ Res Public Health 13:164. https://doi.org/10.3390/ijerph13020164
Zhang P, Zhang J (2017) Surveillance on other infectious diarrheal diseases in China from 2014 to 2015. (in Chinese). Chin J Epidemiol 38:424–430. https://doi.org/10.3760/cma.j.issn.0254-6450.2017.04.003
Zhao Q, Li S, Cao W, Liu D-L, Qian Q, Ren H, Ding F, Williams G, Huxley R, Zhang W (2018) Modeling the present and future incidence of pediatric hand, foot, and mouth disease associated with ambient temperature in mainland China. Environ Health Perspect 126:047010. https://doi.org/10.1289/EHP3062
Zhao R, Gao Q, Hao Q, Wang S, Zhang Y, Li H, Jiang B (2021) The exposure-response association between humidex and bacillary dysentery: a two-stage time series analysis of 316 cities in mainland China. The Science of the total environment, 148840. https://doi.org/10.1016/j.scitotenv.2021.148840
Acknowledgements
We thank the Chinese Center for Disease Control and Prevention, National Meteorological Information Center of China for sharing the data.
Funding
This study was supported by the Special Foundation of Basic Science and Technology Resources Survey of Chinese Ministry of Science and Technology (No. 2017FY101202).
Author information
Authors and Affiliations
Contributions
HQ: Conceptualization; Methodology; Software; Formal analysis; Data curation; Writing, original draft; Visualization. GQ: Methodology; Writing, review and editing. ZR: Methodology; Data curation; Writing, review and editing. WHT: Resources; Writing, review and editing. LH: Writing, review and editing. JBF: Conceptualization; Validation; Resources; Writing, review and editing; Supervision; Project administration; Funding acquisition. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval for analysis of this de-identified data was granted by the Ethics Review Committee, School of Public Health, Shandong University (20120501).
Competing interests
The authors declare no competing interests.
Additional information
Responsible Editor: Lotfi Aleya
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Hao, Q., Gao, Q., Zhao, R. et al. The effect and attributable risk of daily temperature on category C infectious diarrhea in Guangdong Province, China. Environ Sci Pollut Res 29, 23963–23974 (2022). https://doi.org/10.1007/s11356-021-17132-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11356-021-17132-y