
Abstract
Background
Transanal endoscopic microsurgery (TEM) is the treatment of choice for benign rectal tumors and select early rectal cancers. This surgical approach has become ubiquitous and surgeons are seeing recurrent lesions after TEM resection. This study aims to outline the safety and outcomes of repeat TEM when compared to primary TEM procedures.
Methods
At St. Paul’s Hospital, demographic, surgical, pathologic, and follow-up data for patients treated by TEM are maintained in a prospectively populated database. Two groups were established for comparison: patients undergoing first TEM procedure (TEM-P) and patients undergoing repeat TEM procedure (TEM-R).
Results
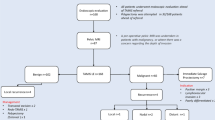
Between 2007 and 2017, 669 patients had their first TEM procedure. Over this time frame, 57 of these patients required repeat TEM procedures, including 15 of these patients treated by 3 or more TEMs. Indications for repeat TEM included recurrence (78%), positive margins (15%), and metachronous lesions (7%). There were no differences between the groups in patient age, gender, or tumor histology. Compared to TEM-P, TEM-R had shorter operative times (38 vs. 52 min, p < 0.001), more distal lesions (5 vs. 7 cm, p < 0.004), and smaller lesions (3 vs. 4 cm, p < 0.0003). The TEM-R group had similar length of hospital stay (0.45 vs. 0.56 days, p = 0.65), rates of clear margins on pathology (81% vs. 88%, p = 0.09), and 30-day readmission rates (7% vs. 4%, p = 0.27) when compared to TEM-P group. TEM-R was more likely to be managed without suturing the surgical defect (72% vs. 32%, p < 0.0001). Repeat TEM was associated with similar post-operative complications as primary TEM graded on the Clavien–Dindo classification scale (Grade 1: 5% vs. 5%, Grade 2: 5% vs. 4%, Grade 3: 5% vs. 1%, p = 0.53). No 30-day mortality occurred in either group.
Conclusions
The St. Paul’s Hospital TEM experience suggests repeat TEM is a safe and feasible procedure with similar outcomes as patients undergoing first TEM.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Transanal endoscopic microsurgery (TEM) is a minimally invasive technique that has established itself as the standard of care for benign rectal tumors and select early rectal cancers [1,2,3]. Since its introduction by Buess in 1983, it has replaced conventional transanal surgery as it is associated with better R0 resection rates, specimen integrity, and fewer recurrences [4,5,6]. The technical advantage of TEM facilitates expanded indications for resection, particularly in the mid to upper rectum, avoiding radical transabdominal rectal surgery and its significant morbidity [7]. When compared to endoscopic mucosal and submucosal resection, TEM surgeons can resect larger lesions, complete full thickness excisions (including some mesorectum when indicated), and direct view suture closure [8]. As a low impact procedure, TEM offers another surgical option for patients who are poor operative candidates for the transabdominal approach [9].
With its growing usage, there is the inevitable situation where patients present with recurrent lesions, positive margins, or metachronous lesions that require management. While repeat TEM may be an option for these patients, there are some possible limitations; theoretical concerns include decreased rectal wall compliance, reduced luminal diameter, inability to close the rectal wall defect, and increased post-operative complications. However, few studies have investigated the feasibility, safety, and outcomes of repeat TEM operations [10, 11].
The aim of our study is to analyze the feasibility, morbidity, and outcomes of repeat TEM procedures (TEM-R) compared to primary TEM procedure (TEM-P) in a single tertiary care center.
Materials and methods
Between March 2007 and August 2017, demographic, operative, pathologic, and outcomes data were collected and maintained prospectively for all patients undergoing TEM treated by 4 subspecialty colorectal surgeons at St. Paul’s Hospital in Vancouver, Canada. This was a retrospective review of this database. This study was submitted and approved by the Providence Health Care Research Ethics Board.
Surgical approach
All patients were evaluated preoperatively with colonoscopy, lesion biopsy, and, in cases of suspected cancer, endorectal ultrasound or pelvic magnetic resonance imaging. Rigid rectoscopy was performed in most patients to confirm the height and location of the lesion. The TEM procedure was performed with patients in a lithotomy, lateral decubitus or prone position, depending on the location of the lesion. For the procedure, we utilized the Richard Wolf Medical Instrument Corporation TEM instrument system and the KARL STORTZ GmbH & Co. insufflator with pressures set to 15 mm Hg. The conventional laparoscopic camera (Storz Medical Ag, Tagerwilen, Switzerland) and high-definition video tower was used. Full thickness rectal wall excision was performed for all malignant lesions and selectively for adenomas. In all patients, the rectal vault was irrigated with saline prior to completion of the procedure.
Post-operative care
There was no standard post-operative and imaging protocol used for this study. Discharge for all patients was at the surgeon’s discretion, with the plan for same-day discharge the prevailing institutional norm. Hospital day care surgery discharge criteria were applied, and include return to preoperative baseline orientation and activity level, vital signs within 20% of preoperative value, pain, nausea, and vomiting controlled with oral medications and minimal to no rectal bleeding. Elderly males aged 65 years or older had a planned urinary catheter removal 24–48 h after surgery to reduce incidence of urinary retention. This practice method was introduced early in our study within 2 years of data collection.
Data collection
All patient demographics, operative details, pathology, post-operative complications, and follow-up information were prospectively collected and maintained in the secure St. Paul’s Hospital TEM Database. Post-operative complications were classified using Clavien–Dindo methodology [12]. Patients were followed up at 30 days either in person or by telephone. Patients were excluded if they failed to follow-up or if their operation was abandoned and did not undergo a resection. We performed statistical analysis using student’s T test or chi-squared test, where appropriate.
Outcomes
The primary outcome of interest was post-operative complication (bleeding, infection, urinary retention) within 30 days of surgery. Bleeding was defined as clinic presentation of bright red blood per rectum (in- or outpatient) associated with at least one of hemoglobin drop of 20 g/L from preoperative, blood transfusion, readmission to hospital and/or surgical/endoscopic intervention. Infection was defined as peritonitis or pelvic pain and either fever > 37.9 °C or WBC > 11 × 109 c/L or clinician diagnosed post-operative infection. Urinary retention was defined as either catheter reinsertion after surgery because of failure to void or catheter reinsertion within 30 days of surgery.
All patients diagnosed with infection and discharged from hospital were treated with oral ciprofloxacin 500 mg PO BID and metronidazole 500 mg PO BID for 7 days. Conversely, patients admitted to hospital for infection were treated with piperacillin/tazobactam 3.375 g IV q6H and transitioned to ciprofloxacin and metronidazole by the time of discharge, completing a 7-day course of antibiotics.
Results
A total of 669 patients from the TEM database were included in the study in the TEM-P group. There were 57 repeat TEM procedures recorded in the TEM-R group. Some patients required more than two TEM operations. Forty-two procedures were patients’ 2nd TEM, ten procedures were patients’ 3rd TEM, four procedures were patients’ 4th TEM, and one procedure was patents’ 5th TEM. The indications for the TEM-R group included recurrence (78%), positive margins (15%), and metachronous lesions (7%).
In analyzing the TEM-R group compared to TEM-P, no significant differences were found in terms of patient age (67.1 vs. 68.8 years, p = 0.23), male:female ratio (p = 0.22), or tumor histology (p = 0.16) (Table 1). Lesions in the TEM-P group included 362 adenomas, 245 adenocarcinomas, 32 neuroendocrine tumors, 7 GISTs, and 23 other lesions which included rectal polyp, normal rectal tissue, melanoma, and anal squamous cell carcinoma. Lesions in the TEM-R group included 49 adenomas, 6 adenocarcinomas, and 2 GISTs.
Repeat TEM had shorter operative times (38 vs. 52 min, p < 0.001), more distal lesions (5 vs. 7 cm, p < 0.004), and smaller lesions (3 vs. 4 cm, p < 0.0003) compared to patients undergoing first TEM. Patients undergoing repeat TEM were more likely to have unsutured rectal defects (72% vs. 32%, p < 0.0001). Of the TEM-R group, 74% of these patients had their original defect left open during their initial procedure. In assessing pathologic data, TEM-R had similar rates of clear margins on pathology (81% vs. 88%, p = 0.09) compared to TEM-P.
Post-operatively, the TEM-R group had similar length of hospital stay (0.45 vs. 0.56 days, p = 0.65), and 30-day readmission rates (7% vs. 4%, p = 0.28) (Table 2). In addition, 81% of the repeat TEM patients were safely discharged same day of surgery. Similar post-operative complications were found between TEM-R and TEM-P (15% vs. 10%, p = 0.15). No difference was found between TEM-R and TEM-P on the Clavien–Dindo classification scale (Grade 1: 5% vs. 5%, Grade 2: 5% vs. 4%, Grade 3: 5% vs. 1%, p = 0.53). No 30-day mortality occurred in either group.
Further classifying complications, repeat TEM was associated similar rates of post-operative bleeding (5% vs. 2%, p = 0.10), infection (5% vs. 4%, p = 0.73), and urinary retention (2% vs. 3%, p = 0.56) when compared to TEM-P. Three patients had Clavien–Dindo grade 3 complications and required reoperations in the TEM-R group. One patient had a post-operative bleed on day five from a resection of a 1.5-cm adenoma and required endoscopic argon beam cauterization for hemostasis. Another patient who had a 3.5-cm adenoma resected had persistent perianal pain 2 weeks after procedure. This patient was brought to surgery for examination under anesthesia, and it was found that the dissection extended distal to the dentate line causing the discomfort. Local anesthetic was used and patient’s pain resolved. Finally, one patient required reoperation same day for a missed peritoneal perforation after removing a circumferential 3-cm adenoma. The patient required a repeat TEM for endoscopic suture closure of the defect and was discharged safely on post-operative day 2.
There were two non-operative readmissions within 30 days for the TEM-R group. One patient had a post-operative bleed on post day 2 and required two units of packed RBC transfusion after resection of a 3.5-cm adenocarcinoma. Another patient, who had a GIST removed, returned 2 weeks after his procedure with a small 2-cm periprostatic abscess that was treated conservatively with antibiotics.
Discussion
TEM is a modern approach to certain types of rectal lesions. Due to a high volume, our group has started to encounter patient candidates for repeat TEM for recurrence, positive margins, or metachronous lesions. There are very few studies focused on the safety and outcomes of repeat TEM [10, 11]. To our current knowledge, this is the largest TEM study solely looking at the feasibility and outcomes of repeat TEM. Khoury et al. found similar results with no significant difference in terms of overall morbidity and length of hospital stay in repeat TEM [10]. From our database, we were able to identify 57 patients who had repeat TEM procedures. Fifteen of these were patient’s third surgery or greater, whereas one patient underwent a total of 5 TEM procedures over a span of 4 years.
The main indication for repeat TEM was recurrence. Studies have shown the recurrence rate for adenomas to range from 0 to 16% [13,14,15]. In our study, repeat TEM was associated with more distal lesions, and an association between recurrence and tumor location has not been shown in the literature [16]. It is important to note that not all adenoma recurrences are managed by TEM; both endoscopic removal and abdominal surgery were used for these patients, and TEM was preferred with low lesions not amenable to these approaches.
It has been theorized that repeat TEM would be technically difficult, possibly due to poor insufflation related to scar tissue from previous resection [10]. In the 57 patients who underwent repeat TEM, including 15 operations where it was a third attempt at TEM, no surgery had to be abandoned for this reason. In fact, the operative times for repeat surgery were significantly shorter than the original TEM surgery. As previous studies have shown that surgeon’s case volume and experience is associated with better outcomes, these findings might be biased in favor of the more recently performed repeat TEMS [17, 18]. In addition, patients treated by repeat TEM were more likely to have unsutured defects which would contribute to the shorter operating time.
The propensity toward unsutured rectal defects after repeat TEM warrants some exploration. The surgeons within our study describe scar tissue creating rectal fixation and a lack of pliability creating areas of high tension where the sutures would tear through the tissue when trying to reapproximate the edges. In addition, 74% of these TEM-R patients had their rectal defect left open during their first TEM surgery, owing to the large size and distal location of the lesions. Despite the difference in open rectal defects, the ability to achieve clear pathologic margins was similar between the groups. Also, there was no significant difference in post-operative bleeding, which has been associated with leaving the defect open [19].
In our study, we found that short-term outcomes after repeat TEM were acceptable. The length of post-operative hospital stay was similar between the two groups. In 81% of repeat TEM patients, safe same-day discharge was achieved. Day surgery has many benefits including health care financial benefits, higher patient satisfaction, and lower complications rates [20, 21]. Similarly, there was no significant difference between the two groups in terms of post-operative complications, including bleeding, infection, and urinary retention rates. Our group has similar post-op morbidity rates as other TEM studies [22, 23]. However, our study reports lower rates of urinary retention for both groups post TEM compared to the literature [22,23,24]. Our group initiated a protocol of discharging elderly male patients aged 65 years and over with a catheter for planned removal 24–48 h after surgery. This has helped significantly reduce this common post-operative issue after TEM.
Only one patient required reoperation during the same admission. There was a missed peritoneal perforation which was amenable to TEM endoscopic suturing despite being a repeat procedure. Only two other patients in repeat TEM required additional intervention post procedure. One had post-op bleed that was cauterized with argon beam and the other had an anesthetic injection, as the dissection was distal to the dentate line and the patient experienced much pain in the early post-op period. All three of these patients with Grade 3 Clavien–Dindo post-operative complications had their defects left unsutured. Despite the scar tissue related to repeat TEM, our recommendation would be to close these defects if technically feasible to help reduce the morbidity risk. However, studies have shown open defects as a safe alternative [19, 25, 26]. Overall, repeat TEM patients had a similar post-operative complication rate as patients undergoing first TEM. Repeat TEM should be considered before proceeding with conventional radical resection which has higher morbidity rate [4, 5, 27].
The small size of our repeat TEM group is a limitation. Larger studies including long-term outcomes would help verify the feasibility of repeat TEM. The prospective collection of data reduces some of the inherit biases associated with retrospective studies.
In conclusion, our study represents the largest single study describing repeat TEM showing it is a feasible and safe option for select patients. Repeat TEM had similar day surgery rate, post-operative complications, and readmission rates as patients undergoing primary TEM.
References
Lezoche E, Guerrieri M, Paganini A, Feliciotti F, Di Pietrantonj F (1996) Is transanal endoscopic microsurgery (TEM) a valid treatment for rectal tumors? Surg Endosc 7:736–741
Middleton PF, Sutherland LM, Maddern GJ (2005) Transanal endoscopic microsurgery: a systematic review. Dis Colon Rectum 48:270–284
Saclarides TJ (1997) Transanal endoscopic microsurgery. Surg Clin North Am 1:229–239
Winde G, Nottberg H, Keller R, Schmid KW, Bünte H (1996) Surgical cure for early rectal carcinomas (T1). Transanal endoscopic microsurgery vs. anterior resection. Dis Colon Rectum 9:969–976
Lezoche G, Baldarelli M, Guerrieri M, Paganini AM, De Sanctis A, Bartolaccis S, Lezoche E (2008) A prospective randomized study with a 5-year minimum followup evaluation of transanal endoscopic microsurgery versus laparoscopic total mesorectal excision after neoadjuvant therapy. Surg Endosc 22:352
Behrouz H, Phang TP, Raval MJ, Brown CJ (2013) Transanal endoscopic microsurgery: a review. Can J Surg 57:127–138
Buess G, Theiss R, Gunther M, Hutterer F, Pichlmaier H (1985) Endoscopic surgery in the rectum. Endoscopy 17:31–35
Barendse RM, van den Broek FJC, Dekker E, Bemelman WA, de Graaf EJR, Foceksn P, Reitsma JB (2011) Systematic review of endoscopic mucosal resection versus transanal endoscopic microsurgery for large rectal adenomas. Endoscopy 43:941–955
Perrotta S, Quarto G, Desiato V, Benassai G, Amato B, Benassai G (2013) TEM in the treatment of recurrent rectal cancer in elderly. BMC Surg 13:S56
Khoury W, Gilshtein H, Nordkin D, Kluger Y, Duek SD (2013) Repeated transanal endoscopic microsurgery is feasible and safe. J Laparoendosc Adv Surg Tech 23:216–219
Zhang HW, Han XD, Wang Y, Zhang P, Jin ZM (2012) Anorectal functional outcome after repeated transanal endoscopic microsurgery. World J Gastroenterol 18:5807–5811
Dindo D, Demartines N, Clavien PA (2004) Classification of surgical complications. Ann Surg 240:205–213
Guerrieri M, Baldarelli M, Morino M, Trompetto M, Da Rold A, Selmi I, Allaix ME, Lezoche G, Lezoche E (2006) Transanal endoscopic microsurgery in rectal adenomas: experience of six Italian centres. Dig Liver Dis 38:202–207
Middleton PF, Sutherland LM, Maddern G (2005) Transanal endoscopic micro-surgery: a systematic review. Dis Colon Rectum 48:270–284
Kunitake H, Abbas MA (2012) Transanal endoscopic microsurgery for rectal tumors: a review. Perm J 16:45–50
McCloud JM, Waymont N, Pahwa N, Varghese P, Richards C, Jameson JS, Scott AN (2006) Factors predicting early recurrence after transanal endoscopic microsurgery excision for rectal adenoma. Colorectal Dis 8:581–585
Maya A, Vorenberg A, Oviedo M, da Silva G, Wexner SD, Sands D (2013) Learning curve for transanal endoscopic microsurgery: a single-center experience. Surg Endosc 28:1407–1412
Barendse RM, Dijkgraaf MG, Rolf UR, Bijnen AB, Consten ECJ, Hoff C, Dekker E, Fockens P, Bemelman WA, De Graaf EJR (2013) Colorectal surgeons’ learning curve of transanal endoscopic microsurgery. Surg Endosc 27:3591–3602
Lee L, Althoff A, Edwards K, Albert MR, Atallah SB, Hunter IA, Hill J, Monson JRT (2018) Outcomes of closed versus open defects after local excision of rectal neoplasms: a multi-institutional matched analysis. Dis Colon Rectum 61:172–178
Lemos P, Pinto A, Morais G, Pereira J, Loureiro R, Teixeira S, Nunes CS (2009) Patient satisfaction following day surgery. J Clin Anesth 21:200–205
Sturniolo G, Bonanno L, Lo Schiavo MG, Tonante A, Taranto F, Gagliano E, Sturniolo G (2007) Day surgery as a factor in reducing hospital stay. Chir Italy 59:41–52
Bignell MB, Ramwell A, Evans JR, Dastur N, Simson JNL (2009) Complications of transanal endoscopic microsurgery (TEMS): a prospective audit. Colorectal Dis 12:e99–e103
Kumar A, Coralic J, Kelleher D, Sidani S, Kolli K, Smith L (2013) Complications of transanal endoscopic microsurgery are rare and minor: a single institution’s analysis and comparison to existing data. Dis Colon Rectum 56:295–300
Laliberte AS, Lebrun A, Drolet S, Bouchard P, Bouchard A (2014) Transanal endoscopic microsurgery as an outpatient procedure is feasible and safe. Surg Endosc 29:3454–3459
Brown C, Raval MJ, Phang PT, Karimuddin K (2017) The surgical defect after transanal endoscopic microsurgery: open versus closed management. Surg Endosc 31:1078–1082
Ramirez JM, Aguilella V, Arribas D, Martinez M (2002) Transanal-full thickness excision of rectal tumours: should the defect be sutured? a randomized controlled trial. Colorectal Dis 4:51–55
Morino M, Allaix ME (2013) Transanal endoscopic microsurgery: what indications in 2013? Gastroenterol Rep 1:75–84
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Drs. Jonathan Ramkumar, Francois Letarte, Ahmer A. Karimuddin, P. Terry Phang, Manoj J. Raval, and Carl J. Brown have no conflicts of interest or financial ties to disclose.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Ramkumar, J., Letarte, F., Karimuddin, A.A. et al. Assessing the safety and outcomes of repeat transanal endoscopic microsurgery. Surg Endosc 33, 1976–1980 (2019). https://doi.org/10.1007/s00464-018-6501-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-018-6501-9