
Abstract
Background
Recently, several new imaging technologies, such as three-dimensional (3D)/high-definition (HD) stereovision and high-resolution two-dimensional (2D)/4K monitors, have been introduced in laparoscopic surgery. However, it is still unclear whether these technologies actually improve surgical performance.
Methods
Participants were 11 expert laparoscopic surgeons. We designed three laparoscopic suturing tasks (task 1: simple suturing, task 2: knotting thread in a small box, and task 3: suturing in a narrow space) in training boxes. Performances were recorded by an optical position tracker. All participants first performed each task five times consecutively using a conventional 2D/HD monitor. Then they were randomly divided into two groups: six participants performed the tasks using 3D/HD before using 2D/4K; the other five participants performed the tasks using a 2D/4K monitor before the 3D/HD monitor. After the trials, we evaluated the performance scores (operative time, path length of forceps, and technical errors) and compared performance scores across all monitors.
Results
Surgical performances of participants were ranked in decreasing order: 3D/HD, 2D/4K, and 2D/HD using the total scores for each task. In task 1 (simple suturing), some surgical performances using 3D/HD were significantly better than those using 2D/4K (P = 0.017, P = 0.033, P = 0.492 for operative time, path length, and technical errors, respectively). On the other hand, with operation in narrow spaces such as in tasks 2 and 3, performances using 2D/4K were not inferior to 3D/HD performances. The high-resolution images from the 2D/4K monitor may enhance depth perception in narrow spaces and may complement stereoscopic vision almost as well as using 3D/HD.
Conclusions
Compared to a 2D/HD monitor, a 3D/HD monitor improved the laparoscopic surgical technique of expert surgeons more than a 2D/4K monitor. However, the advantage of 2D/4K high-resolution images may be comparable to a 3D/HD monitor especially in narrow spaces.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
High-definition video (HD) systems for laparoscopic surgery can provide clear images of fine anatomical structure and are in widespread clinical use today. Recently, several new imaging technologies, such as three-dimensional (3D)/HD stereovision and ultra-high-resolution image two-dimensional (2D)/4K monitors, have been introduced in laparoscopic surgery. These new camera systems for laparoscopic surgery were expected to overcome a lack of depth perception and improve surgical performance with respect to superior accuracy and dexterity compared with a conventional 2D/HD monitor. Several reports indicate that a 3D/HD monitor improves surgical performance and reduces operative time and technical errors in tasks with training boxes or in actual surgery compared with a 2D/HD monitor [1,2,3,4,5,6,7,8,9]. However, no report has evaluated the usefulness of a 2D/4K resolution monitor for laparoscopic surgical performance.
In previous studies, we reveal that a 3D/HD system significantly improves the laparoscopic surgical performance in training boxes for moderately experienced surgeons and novices compared with a 2D/HD monitor [10, 11]. However, the negative or positive effects of laparoscopic training for expert surgeons using a 3D/HD monitor are still unknown.
In this study, we analyzed operative data performed under three different systems (2D/HD, 3D/HD, and 2D/4K resolution monitors) using an optical tracking systems in laparoscopic training boxes to compare the performances between monitors and evaluate the advantages of 3D/HD and 2D/4K monitors for the laparoscopic performance of expert surgeons.
Materials and methods
Trial equipment
Figure 1A shows the trial setup. Devices used were a 3D/HD laparoscopy system and a 2D/4K laparoscopy system (Olympus Medical Systems, Tokyo, Japan). Each setting closely simulated the usual position of the surgeon and monitor in actual laparoscopic surgery in our institution. With a 3D/HD laparoscope system, two charge-coupled device (CCD) image sensors are located at the distal end of the laparoscope to provide left and right images. These two image signals are processed by a special-purpose video system to generate a high-resolution 3D image that is then displayed on a 3D monitor and viewed through 3D glasses to provide realistic 3D images. This system can be switched from 3D images to 2D images by pressing a switch on the scope for performing under 2D/HD vision. The distance between the tip of the endoscope and the object of the operation was fixed at 15 cm. For the trial, we set the monitor so the subject directly faced the display with viewing distance range of about 1.2 m, and the viewer’s eye level is at the middle of the display (Fig. 2A).

Schema for recording performance in the training box. A The apparatus consisted of a monitor, position tracker, and training box including a phantom task. B Device for task 1 (simple suturing). C Device for task 2 (knotting thread around two rubber bands in a small box). D Device for task 3 (suturing in a tiny space)

Setup of the participant, devices, and monitor. A 2D/HD and 3D/HD laparoscope system. B 2D/4K laparoscope system
With a 2D/4K laparoscope system, the main monitor has 1264.6 width and 771.5 height (55 inch LMD), and we set the monitor so that the subject directly faced the display with a viewing distance of about 1.5 m, and the viewer’s eye level is at the middle of the display. The distance between the tip of the endoscope and the object of the operation was fixed at 15 cm which is similar to the setting of the trial of a 3D/HD system (Fig. 2B).
The micron tracker (Claron Technology, Toronto, Canada) consists of charge-coupled device (CCD) image sensors. This system enables the tracking and recording of 3D coordinates and rotation of forceps with an optical marker (Fig. 1A). Data are obtained as text data and can be analyzed by statistical software.
Study design
Study participants were 11 expert surgeon volunteers who were rigorously certified by Japan Society for Endoscopic Surgery (JSES) with the Endoscopic Surgical Skill Qualification System of “qualified surgeon.” Their laparoscopic surgical skills are guaranteed by the most rigorous examination (including suturing technique test) in Japan, and the acceptance rate is about 20–30%. All participants had performed at least 100 laparoscopic surgeries.
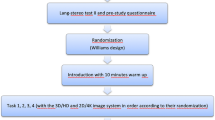
Participants performed three different laparoscopic phantom tasks in training boxes five times each using three different monitors. All participants performed the tasks initially using a 2D/HD monitor. After performing the initial 2D/HD monitor tasks, participants were randomly divided into two groups: 6 participants performed the tasks using a 3D/HD monitor before the 2D/4K monitor, and the other 5 participants performed the tasks using a 2D/4K monitor before the 3D/HD monitor (Fig. 3). At least 24 h elapsed between switching monitors. Performances were recorded by the optical position tracker to analyze the motion of the forceps in 3D space. We compared operative times, path lengths of the forceps, and counted technical errors between each monitor system after participants completed each trial. The purpose of the study was explained to all participants, and consent was obtained from all participants of this study before the first trial.

Diagram of study design
Tasks
Task 1: Simple suturing (Fig. 1B)
This task was performed by both hands. Initially, a 12 cm length of 3-0 vicryl thread (Ethicon, Inc., Somerville, New Jersey, USA) was set in the field. A needle with thread had to be grasped with a lockable endoscopic needle holder by both hands, and then used to pierce dots on a sheet of paper. Finally, the thread had to be tied three times using a throw knot. After the task was completed, both forceps were set back in their original positions. Skipping the dots and not grasping the tail of the thread were counted as errors.
Task 2: Knotting thread around two rubber bands in a small box (Fig. 1C)
In this task, a 12 cm length of 3-0 vicryl thread grasped by an endoscopic needle holder had to be turned around two parallel rubber bands in a small metal box. The thread then had to be tied three times with a throw knot. After the task was completed, both forceps were set back in their original positions. The metal box was 4 cm wide, 4 cm tall, and 2.5 cm deep. Participants were instructed to avoid touching the metal box with either the needle or forceps. A small light bulb was wired to the metal box and was lit by accidental touching, and the number of lightings was counted as errors.
Task 3: Suturing in a narrow space (Fig. 1D)
This task was performed by both hands. Initially, a 12 cm length of 3-0 vicryl thread was set in the field. A needle with thread had to be grasped with a lockable endoscopic needle holder by both hands, and then used to pierce dots on a sheet of paper. Finally, the thread had to be tied three times with throw knots. After the task was completed, both forceps were set back in their original positions. This task was performed in a metal box which became narrower with increasing length, and participants were instructed to avoid touching the metal box with either the needle or forceps. The front side of the metal box was 10 cm wide and 6 cm tall, the back side was 1 cm wide and 2 cm tall, and the lateral side was 6 cm deep. A small light bulb was wired to the metal box and would light up with accidental touching, and the number of lightings was counted as errors.
Statistical analysis
Measured data were recorded and assessed by a single investigator. Forceps path lengths were calculated as follows:
where P1, P2, …, Pn represent tip positions of the forceps at each time frame (one time frame = 0.05 s).
Statistical analysis of the data was performed using JMP ver.8.0 software (SAS Institute Inc., Cary, NC, USA). All data are presented as median values and the mean ± standard error of the mean (SEM). Comparisons between groups were performed by the Wilcoxon signed-rank test with P < 0.05 considered significant.
Results
Tables 1 and 2 and Fig. 4 show comparisons of the scores of all participants for each task between each monitor.

Comparison between 2D/HD, 2D/4K, and 3D systems regarding median scores (operative times, path length of forceps, technical errors) of all participants with the scores for each task and with total scores from all tasks
Task 1
Median operative times (2D/4K vs. 3D/HD) were 55.7 and 48.2 s, respectively (P = 0.017). Median path lengths (2D/4K vs. 3D/HD) were 3845 and 3307 mm, respectively (P = 0.033). The median technical errors were 0 for this task for all monitors, and there are no significant differences in error rates between monitors.
Table 2 and Fig. 4 show that performances using 2D/HD and 2D/4K monitors did not differ significantly. However, performances using a 3D/HD monitor were significantly better than when using 2D/HD and 2D/4K monitors.
Task 2
Median operative times (2D/4K vs. 3D/HD) were 60.6 and 56.7 s, respectively (P = 0.380). Median path lengths (2D/4K vs. 3D/HD) were 3617 and 3832 mm, respectively (P = 0.838). Median technical errors were 1 and 0, respectively (P = 0.002).
Table 2 and Fig. 4 show that performances using the 3D/HD and 2D/4K monitors were both significantly better than from the 2D/HD monitor. However, performances from the 2D/4K and 3D/HD monitors did not differ significantly from each other.
Task 3
Median operative times (2D/4K vs. 3D/HD) were 77.0 and 66.6 s, respectively (P = 0.158). Median path lengths (2D/4K vs. 3D/HD) were 4058 and 3911 mm, respectively (P = 0.654). The median technical errors were 2 and 1 for 2D/4K and 3D/HD, respectively (P = 0.592).
Table 2 and Fig. 4 show that, though there were no significant difference between 2D/4K and 3D/HD monitors with respect to operative time and path length, performances using 3D/HD and 2D/4K monitors are both significantly better than from the 2D/HD monitor with respect to technical errors.
Total tasks
We also evaluated the median of all scores tasks from all participants for all tasks. Median operative times were 71.2, 62.4, and 55.6 s with 2D/HD, 2D/4K, and 3D/HD, respectively. Median path lengths for total tasks were 4431, 3821, and 3693 mm with 2D/HD, 2D/4K, and 3D/HD, respectively. Median technical errors for all tasks were 1, 1, and 0 with 2D/HD, 2D/4K, and 3D/HD, respectively.
As shown in Fig. 4, the surgical performances of participants were ranked in decreasing order: 3D/HD, 2D/4K, 2D/HD.
Discussion
A 3D monitor is expected to correct deficiencies in depth perception for improvement of laparoscopic surgical performance. In this study, we showed that the performance using a 3D/HD monitor was better than using 2D/HD and 2D/4K monitors for the median scores of all tasks. However, for each individual task, there were differences in the advantages conferred by a 3D/HD system compared with a 2D/4K system depending on the task design.
It is often considered that greatly experienced laparoscopic surgeons are capable of perceiving depth of surgical fields from binocular disparity as well as from even conventional 2D vision. Therefore, for basic tasks such as simple suturing which experts had already mastered under 2D vision, we initially hypothesized that the performance might not show significant differences compared with 4K/2D and 3D vision systems. However, with simple suturing (task 1), though no errors were observed for each monitor, the surgical performance of expert surgeons was significantly improved with respect to operative time and path length using a 3D/HD system. A 3D/HD monitor makes experts more efficient and dexterous even in simple suturing. On the other hand, we initially presumed that performances using 3D/HD would be better than 2D/4K in complex tasks even for experts. However, with complex tasks (tasks 2 and 3), performances under 2D/4K were actually comparable to those using 3D/HD.
According to this study, the performance using 2D/4K was obviously inferior to that under 3D/HD in a simple task, but using a 2D/4K monitor was not inferior to a 3D/HD monitor in complex tasks. A previous report showed that human stereopsis can recognize depth perception from 2D images [12] meaning surrounding objects can confer contrast between the target and the background and emphasize depth perception signs such as shading or motion parallax of objects. We hypothesized that a 4K resolution video would improve laparoscopic surgical performance by emphasizing these depth perception signs and making them clearer than a conventional 2D/HD monitor. We extrapolated that, in such a narrow space such as used in tasks 2 and 3, the shading of target objects and surroundings might be enhanced by high-resolution vision from a 2D/4K monitor compared with a conventional 2D/HD monitor. On the other hand, the operating field of task 1 was free of obstruction and, therefore, it was relatively difficult to recognize depth perception signs such as shading of target objects. This result suggests that a 2D/4K resolution monitor has the potential to be just as good as a 3D/HD monitor especially in narrow surgical fields such as digestive tract reconstruction or lymphadenectomy around the esophagogastric junction or in the pelvic cavity.
There are several limitations in this study. First, the performance using a 2D/HD monitor might have been reduced by an unfamiliarity with the assessment system since this trial occurred before the 2D/4K or 3D/HD trials. However, all participants were experts at basic laparoscopic surgical techniques, and the lack of technical errors in trial 1 supported their expertise. Therefore, we consider the learning effects were minimal for our experts. Second, the sample size was small. It was difficult to enroll a large sample in this study because the number of surgeons qualified by JSES is about 3000 and is less than 10% of all surgeons in Japan.
In conclusion, a 3D/HD monitor improved the laparoscopic surgical technique of expert surgeons better than a 2D/4K monitor in open spaces. However, 2D/4K high-resolution images may be not inferior to a 3D/HD monitor especially in narrow spaces.
References
Currò G, La Malfa G, Caizzone A, Rampulla V, Navarra G (2015) Three-dimensional (3D) versus two-dimensional (2D) laparoscopic bariatric surgery: a single-surgeon prospective randomized comparative study. Obes Surg 25:2120–2124
Kanaji S, Suzuki S, Harada H, Nishi M, Yamamoto M, Matsuda T, Oshikiri T, Nakamura T, Fujino Y, Tominaga M, Kakeji Y (2017) Comparison of two- and three-dimensional display for performance of laparoscopic total gastrectomy for gastric cancer. Langenbecks Arch Surg 402:493–500
Mashiach R, Mezhybovsky V, Nevler A, Gutman M, Ziv A, Khaikin M (2014) Three-dimensional imaging improves surgical skill performance in a laparoscopic test model for both experienced and novice laparoscopic surgeons. Surg Endosc 28:3489–3493
Ashraf A, Collins D, Whelan M, O’Sullivan R, Balfe P (2015) Three-dimensional (3D) simulation versus two-dimensional (2D) enhances surgical skills acquisition in standardised laparoscopic tasks: a before and after study. Int J Surg 14:12–16
Chiu CJ, Lobo Prabhu K, Tan-Tam CC, Panton ON, Meneghetti A (2015) Using three-dimensional laparoscopy as a novel training tool for novice trainees compared with two-dimensional laparoscopy. Am J Surg 209:824–827
Rodrigues SP, Horeman T, Blomjous MS, Hiemstra E, van den Dobbelsteen JJ, Jansen FW (2016) Laparoscopic suturing learning curve in an open versus closed box trainer. Surg Endosc 1:315–322
Egi H, Hattori M, Suzuki T, Sawada H, Kurita Y, Ohdan H (2016) The usefulness of 3-dimensional endoscope systems in endoscopic surgery. Surg Endosc 30:4562–4568
Blavier A, Gaudissart Q, Cadiere GB, Nyssen AS (2007) Comparison of learning curves and skill transfer between classical and robotic laparoscopy according to the viewing conditions: implications for training. Am J Surg 194:115–121
Poudel S, Kurashima Y, Watanabe Y, Ebihara Y, Tamoto E, Murakami S, Nakamura T, Tsuchikawa T, Okamura K, Shichinohe T, Hirano S (2017) Impact of 3D in the training of basic laparoscopic skills and its transferability to 2D environment: a prospective randomized controlled trial. Surg Endosc 31:1111–1118
Nishi M, Kanaji S, Otake Y, Harada H, Yamamoto M, Oshikiri T, Nakamura T, Suzuki S, Suzuki Y, Hiasa Y, Sato Y, Kakeji Y (2016) Quantitative comparison of operative skill using two- and three-dimensional monitors during laparoscopic phantom tasks. Surgery 161:1334–1340
Harada H, Kanaji S, Nishi M, Otake Y, Hasegawa H, Yamamoto M, Matsuda Y, Yamashita K, Matsuda T, Oshikiri T, Sumi Y, Nakamura T, Suzuki S, Sato Y, Kakeji Y (2017) The learning effect of using stereoscopic vision in the early phase of laparoscopic surgical training for novices. Surg Endosc. https://doi.org/10.1007/s00464-017-5654-2
Fergo C, Burcharth J, Pommergaard HC, Rosenberg J (2016) Age is highly associated with stereo blindness among surgeons: a cross-sectional study. Surg Endosc 30:4889–4894
Acknowledgements
This work is supported by JSPS KAKENHI Grant Number JP16K12911. Participating investigators Endoscopic surgical skill qualification system: qualified surgeons; Goto H, Oyama M, Yasuda T (Hyogo Cancer Center, Akashi, Hyogo, Japan), and Kanemitsu K (Yodogawa Christian Hospital, Osaka, Osaka, Japan) significantly contributed as participants in this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Drs. Hitoshi Harada, Shingo Kanaji, Hiroshi Hasegawa, Masashi Yamamoto, Yoshiko Matsuda, Kimihiro Yamashita, Takeru Matsuda, Taro Oshikiri, Yasuo Sumi, Tetsu Nakamura, Satoshi Suzuki, and Yoshihiro Kakeji have no conflicts of interest or financial ties to disclose.
Rights and permissions
About this article

Cite this article
Harada, H., Kanaji, S., Hasegawa, H. et al. The effect on surgical skills of expert surgeons using 3D/HD and 2D/4K resolution monitors in laparoscopic phantom tasks. Surg Endosc 32, 4228–4234 (2018). https://doi.org/10.1007/s00464-018-6169-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-018-6169-1