
Abstract
Videofluoroscopic swallow studies are widely used in clinical and research settings to assess swallow function and to determine physiological impairments, diet recommendations, and treatment goals for people with dysphagia. Videofluoroscopy can be used to analyze biomechanical events of swallowing, including hyoid bone displacement, to differentiate between normal and disordered swallow functions. Previous research has found significant associations between hyoid bone displacement and penetration/aspiration during swallowing, but the predictive value of hyoid bone displacement during swallowing has not been explored. The primary objective of this study was to build a model based on aspects of hyoid bone displacement during swallowing to predict the extent of airway penetration or aspiration during swallowing. Aspects of hyoid bone displacement from 1433 swallows from patients referred for videofluoroscopy were analyzed to determine which aspects predicted risk of penetration and aspiration according to the Penetration–Aspiration Scale. A generalized estimating equation incorporating components of hyoid bone displacement and variables shown to impact penetration and aspiration (such as age, bolus volume, and viscosity) was used to evaluate penetration and aspiration risk. Results indicated that anterior-horizontal hyoid bone displacement was the only aspect of hyoid bone displacement predictive of penetration and aspiration risk. Further research should focus on improving the model performance by identifying additional physiological swallowing events that predict penetration and aspiration risk. The model built for this study, and future modified models, will be beneficial for clinicians to use in the assessment and treatment of people with dysphagia, and for potentially tracking improvement in hyolaryngeal excursion resulting from dysphagia treatment, thus mitigating adverse outcomes that can occur secondary to dysphagia.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Dysphagia affects approximately one in 25 adults in the United States annually [1,2,3,4,5]. It can occur in patients secondary to a variety of etiologies such as stroke, Parkinson's disease [6], head and neck cancer, and brain injuries [7], as well as many other neurological, iatrogenic, and developmental conditions. Aspiration may occur because of dysphagia, which can lead to adverse outcomes including aspiration pneumonia, malnutrition, and dehydration [8,9,10,11]. Additionally, dysphagia and secondary medical complications often result in reduced quality of life for patients. Because of this, it is necessary to rapidly identify dysphagia and determine aspiration risk of patients through timely diagnosis and management.
Videofluoroscopy (VF) is one of the instrumental evaluation tools used to assess physiological impairments of swallowing and reduced airway protection [12, 13]. Clinicians rely on subjective interpretation of the biomechanical events of swallowing observed during VF to determine patient risk of penetration and aspiration. Standardized tools exist for categorizing swallow events during VF, such as the Modified Barium Swallow Impairment Profile (MBSImP) and the Penetration–Aspiration Scale (PAS). The MBSImP is a widely used clinical tool that allows clinicians to evaluate 17 physiological components of swallowing using a subjective ordinal scale. The PAS is an 8-point interval rating scale used to determine the severity of penetration and aspiration. The PAS is used to determine how far material enters the airway and whether or not patients are able to clear penetrated or aspirated material from the airway. While these tools are useful in identifying gross impairments in swallowing function, they involve subjectivity to quantify the degree of swallowing impairment. Swallow kinematic analysis is an objective way to quantify biomechanical events of swallowing; however, it requires standardized training and experience to perform with high levels of intra- and interrater reliability and is not used in most settings.
VF exposes patients to radiation, which forces clinicians to conduct swallowing evaluations in a short period of time. Because of these time constraints, swallowing evaluations may not fully capture a patient's risk of penetration and aspiration. For this reason, clinicians would benefit from having a tool that objectively and automatically measures physiological events that occur during swallowing, such as hyoid bone displacement, to more accurately quantify patient's risk of penetration or aspiration.
While differences in hyoid bone displacement are known to exist among healthy, especially aging individuals [14,15,16], it is known to be associated with an increased risk of penetration and aspiration [17] and can be measured in both horizontal and vertical planes, as described in previous research [18]. However, the exact relationship between hyoid bone displacement and penetration and aspiration risk remains unknown due to conflicting research [19,20,21,22,23].
We previously investigated six aspects of hyoid bone displacement using coordinates based on anatomical landmarks of the vertebral column. Results revealed that reduced anterior-horizontal displacement was the only aspect of hyoid bone displacement associated with higher scores on the PAS [24]. The primary aim of the current study was to determine which aspects of hyoid bone displacement predict the risk of penetration and aspiration. We also investigated the effects of patient’s demography and clinical variables in the model. We hypothesized that a predictive model would reasonably predict penetration and aspiration risk using aspects of hyoid bone displacement and important clinical variables that are associated with penetration and aspiration risk. To test this hypothesis, we built a generalized estimating equation (GEE) model by extracting aspects of hyoid bone displacement data from VF images.
Methods
Data Acquisition
Two hundred and sixty-five patients with suspected dysphagia were enrolled in this prospective study and underwent VF at the University of Pittsburgh Medical Center Presbyterian Hospital. The protocol for the study was approved by the Institutional Review Board at the University of Pittsburgh, and all participants provided informed consent. Patients with tracheostomies or anatomical abnormalities of the head and neck were excluded from the study.
The data for this study were collected in the course of standard clinical care rather than solely for research purposes. We intentionally did not interfere with clinical decision-making in the conduct of the VF examinations. Clinicians who conducted VF modified the protocol for the administration of boluses (e.g., number of swallows, bolus consistencies, head positions, etc.) based on clinical hypotheses and the patients' clinical presentation of dysphagia. The following consistencies were used: E-Z-EM Canada, Inc. Varibar thin (Bracco Diagnostics, Inc.) (< 5 cPs viscosity), Varibar nectar (300 cPs viscosity), Varibar pudding (5000 cPs viscosity), and Keebler Sandies Mini Simply Shortbread Cookies (Kellogg Sales Company). Clinicians administered boluses by spoon (3–5mL) or had participants self-administer a comfortable volume by cup. Head positions included neutral and chin down. Participant characteristics and methods for VF data collection can be found in Table 1.
VF was conducted in the lateral plane using a 30PPS pulse rate and recorded at 60FPS by a video card (AccuStream Express HD, Foresight Imaging, Chelmsford, MA) and recorded onto a hard drive with a LabVIEW program. Videos were converted into digital movie clips of 720 × 1080 resolution and then downsampled to 30 frames per second to eliminate duplicate frames.
Image Analysis
Over 3000 video clips were obtained from VF swallow evaluations. The final dataset used for analysis included 1434 video clips because over half of the original clips were unacceptable for tracking hyoid bone displacement due to poor image quality or obstruction of hyoid bone landmarks by the shoulder or other medical equipment such as cardiac monitor lines, pacemaker leads, etc. Videos were segmented into individual swallow events based on the frame in which the head of the bolus reached the ramus of the mandible (onset), and the frame in which the bolus tail passed the upper esophageal sphincter (UES) (offset) [25]. Swallows were categorized into single (one swallow per bolus), multiple 1 (two swallows per bolus), and multiple 2 (more than two swallows per bolus).
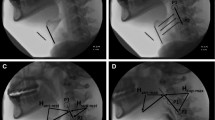
As shown in Fig. 1, an expert judge, trained in swallow kinematic rating, initially identified the following points of interest in each video frame: (1) anterior–inferior corner of C2 vertebral body; (2) anterior–inferior corner of the C4 vertebral body; (3) anterior–inferior corner of the body of the hyoid bone; (4) posterior–superior corner of the body of the hyoid bone; (5) anterior–inferior corner of C3 vertebral body; and (6) anterior–superior corner of C3 vertebral body. The anterior–inferior corner of the C4 vertebral body (2) was defined as the origin. The straight line connecting (2) and (1) was defined as the y-axis. The x-axis was defined as the horizontal line perpendicular to the y-axis and intersecting with (2). To normalize patients with different heights to a common anatomical referent, the anatomical scaling factor for displacement measures was defined as the length between (5) and (6) (i.e., the height of the C3 vertebral body). Image pixels were used to measure distance.
Three raters trained in swallow kinematic analysis identified anatomical points of interest in each of the 1434 swallows, and tracked hyoid displacement using frame-by-frame analysis in MATLAB (R2015b, The MathWorks, Inc., Natick, MA, USA). Reliability was established on 10% of the videos with ICCs of over 0.99 and intrarater reliability was maintained throughout testing to avoid judgment drift. Two clinicians trained in PAS analysis established a priori inter- and intrarater reliability with ICCs of 0.99. All raters were blinded to participant age, sex, and diagnosis.

The landmarks for hyoid bone, C2, C3, C4, and established coordinate
Statistical Analysis
SAS® version 9.3 (SAS Institute, Inc., Cary, North Carolina) was used for all statistical analyses with the GENMOD procedure for obtaining the main results. A dichotomous (normal; disordered) operational definition of PAS scores (1–2; and 3–8, respectively) was used for analyses, because there was a skewed distribution of PAS scores. Logistic regression models that are typically used with dichotomous data could not be used, because the independence criterion was not met due to having multiple swallows in the dataset from each patient. Therefore, a GEE model [26] with a binomial distribution, a logit link function, and an exchangeable working correlation structure (which is an extension of a logistic regression model suitable for analyzing correlated data) was used. Age, gender, swallow type (single/multiple 1/multiple 2), viscosity (thin/nectar/pudding/cookie), utensil (cup/spoon), head position (neutral/chin down), and swallow duration were used as forced-in independent variables based on face validity and prior knowledge of their dependence on PAS scores. In addition to these independent variables, we examined various aspects of hyoid bone displacement using a forward selection strategy with an entry criterion of p < 0.05. The measurement of these landmarks (superior hyoid hone and anterior hyoid bone) includes maximal displacement, maximal peak position, velocity, acceleration, and duration in horizontal and vertical direction. To assess the predicted and observed disordered PAS scores, we created a contingency table based on the predicted probability deciles. The deciles were formed by sorting and separating the predicted probabilities into ten subgroups based on each patient's risk profile, from the lowest to highest risk (1–10). We examined the observed percentage of disordered PAS swallows (3–8) within each decile compared to the predicted percentage according to the model. See Appendix for the predictive model.
Results
Table 1 illustrates the descriptive statistics and participant characteristics. The swallow analysis data were presented in this study for 1433 swallows from 265 distinct patients. Ninety-one swallows were excluded from the analysis due to missing information or incorrect recording. The age range of the subjects was from 19 to 94, and the average ± standard variation age was \(64.8 \pm 13.6\) years. 1129 swallows had PA scores of 1 or 2, and 304 swallows had PA scores greater or equal to 3.
Table 2 illustrates the statistical results of focused-in clinical variables and aspects of hyoid bone displacement that met the 0.05 entry criterion for the model. Clinical variables shown in Table 2 were forced-in to the model with forward selection. Maximum anterior-horizontal hyoid bone displacement was the only aspect of hyoid bone displacement that was significantly predictive of normal versus disordered PAS scores and included in the model. Patient age was significantly predictive of normal versus disordered PAS scores, although the confidence interval included \(\hbox {OR} \,\, 1.00\). For each additional year of age, the odds of a disordered PAS score increased by 3% (\(\hbox {OR}\,\, 1.03\), 95% \(\hbox {CI} \,\, 1.00\) 1.05; \(\hbox {p} = 0.0178\)). There was a trend toward a single swallow being less likely (36%) to have a disordered PAS score compared to multiple swallows, (\(\hbox {OR} \,\,0.64\), 95% \(\hbox {CI} \,\,0.40- 1.04\); \(\hbox {p} = 0.0708\)). Two swallows per bolus (multiple 1) were significantly more likely to have a disordered PAS score (\(\hbox {OR} \,\,1.58\), 95% \(\hbox {CI} \,\,1.16\) 2.15; \(\hbox {p} = 0.0040\)) than more than two swallows per bolus (multiple 2). There was strong evidence that swallows of thin liquid had significantly greater odds of a disordered PAS score than a cookie swallow (\(\hbox {OR} \,\,3.62\), 95% \(\hbox {CI} \,\,1.37\) 9.58; \(\hbox {p}=0.0096\)). The model predicted the risk of penetration and aspiration for each patient based on the variables included in the model. Table 3 shows the predicted probability of having a disordered PAS score in each decile compared to the observed percentage of disordered PAS scores in each decile. For instance, as shown in the table, the predicted probability for decile 1 indicates that 0–7% of the swallows will be disordered. The predictive model effectively captured patient risk profiles for this decile because 6.72% of the swallows had a disordered PAS score. Similar observations can be made for deciles 2, 4, 8, and 9. Deciles 3, 5, 6, 7, and 10 captured the increasing probability trends of penetration and aspiration, although the observed percentage of swallows with disordered PAS scores were slightly outside of the predicted ranges.
Discussion
This study found that a predictive model that included maximum anterior-horizontal hyoid bone displacement and other variables known to affect penetration and aspiration risk can reasonably predict the risk of penetration and aspiration in patients with dysphagia. While this predictive model accurately captured the increasing probability trends of penetration and aspiration risk of patients, the predicted and observed probabilities did not always match. Current clinical practice is for clinicians to assess physiological impairments of swallowing and reduced airway protection by subjectively interpreting VF images. However, one limitation of using VF as an assessment tool is that aspiration may not be observed during VF due to the time constraints of the examination to minimize radiation exposure. Creating a predictive model based on objective measurements of physiological swallowing events, such as the measurements of hyoid bone displacement, which were used in this study, would allow clinicians to more accurately capture patient risk profiles of penetration and aspiration. This model could be used to improve assessment of swallow function, effectively track progress in therapy, and to proactively and objectively identify physiologic markers of elevated risk of adverse events that occur secondary to dysphagia, such as aspiration pneumonia.
Limitations
The GEE model in this study used anterior-horizontal hyoid bone displacement and other independent variables to reasonably predict penetration and aspiration risk for patients with dysphagia. However, swallowing and airway protection are complex, multifactorial processes. It is probable that the variables included in this model are not the only predictors of aspiration. One limitation of the current predictive model is that it underestimates the risk of penetration and aspiration for patients with disordered PAS scores. The predictive model will likely be improved by including other swallow kinematic measurements.
Conclusion
This research work developed a preliminary GEE model that can reasonably predict penetration and aspiration risk for patients with dysphagia. This is an important and necessary first step toward developing a more sophisticated and accurate predictive model that can be used in clinical settings. In the future, clinicians could use a predictive model based on physiological aspects of swallow function to calculate penetration and aspiration risk profiles for patients by entering patient specific information into the equation. By objectively determining patient risk profiles, clinicians could develop individualized treatment plans to prevent adverse outcomes (i.e., dehydration, malnutrition, and aspiration pneumonia) based on risk severity level, and objectively track the effectiveness of dysphagia treatment on functional patient outcome measures. Future research should examine the predictive ability of additional swallow kinematic measures on penetration and aspiration risk in patients with dysphagia. Variables such as hyoid bone velocity, initiation of the pharyngeal swallow, laryngeal elevation, laryngeal vestibular closure, UES duration, and other physiological parameters related to swallow function should be investigated. Including these kinematic events in the predictive model may increase the model’s predictive value, which would further improve its clinical application.
References
Clavé P, Shaker R. Dysphagia: current reality and scope of the problem. Nat Rev Gastroenterol Hepatol. 2015;12(5):259–70.
Dudik JM, Coyle JL, El-Jaroudi A, Sun M, Sejdić E. A matched dual-tree wavelet denoising for tri-axial swallowing vibrations. Biomed Signal Process Control. 2016;27:112–21.
Miller AJ. The neurobiology of swallowing and dysphagia. Dev Disabil Res Rev. 2008;14(2):77–86.
Movahedi F, Kurosu A, Coyle JL, Perera S, Sejdić E. Anatomical directional dissimilarities in tri-axial swallowing accelerometry signals. IEEE Trans Neural Syst Rehabilit Eng. 2017;25(5):447–58.
Bhattacharyya N. The prevalence of dysphagia among adults in the United States. Otolaryngol Head Neck Surg. 2014;151(5):765–9.
Murray J. Manual of dysphagia assessment in adults. Boston: Cengage Learning; 1999.
Lazarus C, Logemann A. Swallowing disorders in closed head trauma patients. Arch Phys Med Rehabil. 1987;68(2):79–84.
Cook IJ, Kahrilas PJ. AGA technical review on management of oropharyngeal dysphagia. Gastroenterology. 1999;116(2):455–78.
Gordon C, Hewer RL, Wade DT. Dysphagia in acute stroke. Br Med J. 1987;295(6595):411–4.
Humbert IA, Robbins J. Dysphagia in the elderly. Phys Med Rehabil Clin N Am. 2008;19(4):853–66.
Gorell JM, Johnson CC, Rybicki BA. Parkinson’s disease and its comorbid disorders An analysis of Michigan mortality data, 1970 to 1990. Neurology. 1994;44(10):1865–1865.
Coyle JL, Davis LA, Easterling C, Graner DE, Langmore S, Leder SB, Lefton-Greif MA, Leslie P, Logemann JA, Mackay L, Martin-Harris B, Murray JT, Sonies B, Steele CM. Oropharyngeal dysphagia assessment and treatment efficacy: setting the record straight (response to Campbell–Taylor). J Am Med Directors Assoc. 2009;10(1):62–6.
Rugiu M. Role of videofluoroscopy in evaluation of neurologic dysphagia. Acta Otorhinolaryngol Ital. 2007;27(6):306.
Molfenter SM, Steele CM. Physiological variability in the deglutition literature: hyoid and laryngeal kinematics. Dysphagia. 2011;26(1):67–74.
Kim Y, McCullough GH. Maximum hyoid displacement in normal swallowing. Dysphagia. 2008;23(3):274–9.
Kang B-S, Oh B-M, Kim IS, Chung SG, Kim SJ, Han TR. Influence of aging on movement of the hyoid bone and epiglottis during normal swallowing: a motion analysis. Gerontology. 2010;56(5):474–82.
Martin-Harris B, Jones B. The videofluorographic swallowing study. Phys Med Rehabil Clin N Am. 2008;19(4):769–85.
Zhang Z, Kurosu A, Coyle J, Perera S, Sejdić E. Hyoid displacement during swallowing is related to penetration–aspiration scores. Under Review.
Kendall KA, Leonard RJ. Hyoid movement during swallowing in older patients with dysphagia. Arch Otolaryngol Head Neck Surg. 2001;127(10):1224–9.
Perlman AL, Booth B, Grayhack J. Videofluoroscopic predictors of aspiration in patients with oropharyngeal dysphagia. Dysphagia. 1994;9(2):90–5.
Su J, Yuan C, Shu K. Hyoid bone displacement during swallowing have no association with penetration/aspiration severity in dysphagic stroke patients. Arch Phys Med Rehabil. 2014;95(10):e16.
Molfenter SM, Steele CM. Kinematic and temporal factors associated with penetration–aspiration in swallowing liquids. Dysphagia. 2014;29(2):269–76.
Seo HG, Oh B-M, Han TR. Swallowing kinematics and factors associated with laryngeal penetration and aspiration in stroke survivors with dysphagia. Dysphagia. 2016;31(2):160–8.
Rosenbek JC, Robbins JA, Roecker EB, Coyle JL, Wood JL. A penetration–aspiration scale. Dysphagia. 1996;11(2):93–8.
Lof GL, Robbins J. Test–retest variability in normal swallowing. Dysphagia. 1990;4(4):236–42.
Wang M. Generalized estimating equations in longitudinal data analysis: a review and recent developments. Adv Stat. 2014. https://doi.org/10.1155/2014/303728.
Acknowledgement
The authors acknowledge Dr. Aliaa Elbahnasy Sabry for her critical review and suggestions on the final manuscript.
Funding
This study was funded by two grants from the Eunice Kennedy Shriver National Institute of Child Health & Human Development of the National Institutes of Health under Award Number R01HD092239, while the data was collected under Award Number R01HD074819. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
We have no conflict of interest to declare.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendix
Appendix
Prediction equation steps:
- 1.
Let \(XB=-3.479-0.0583\times (x1_min2max_distance)+ 0.0265\times (age)-0.0004\times (duration)\)
- 2.
Subtract from XB 0.4435 if the swallow is single, add to XB 0.4545 if the swallow is multiple 1, or do nothing if multiple 2.
- 3.
Subtract from XB 0.1398 if the \(\hbox {sex}=2(\hbox {female}?)\), or do nothing if \(\hbox {sex}=1(\hbox {male}?)\).
- 4.
Add 1.2862 to XB if \(\hbox {viscosity}=\hbox {thin}\), add 0.7049 if nectar, subtract 0.5334 if pudding, and do nothing if cookie.
- 5.
Add to XB 0.1622 if spoon, or do nothing if cup.
- 6.
Add to XB 0.0994 if chin down, or do nothing if head position is neutral.
- 7.
Compute the probability of a high PA swallow as \(exp(XB)/(1+exp(XB))\).
Rights and permissions
About this article

Cite this article
Zhang, Z., Perera, S., Donohue, C. et al. The Prediction of Risk of Penetration–Aspiration Via Hyoid Bone Displacement Features. Dysphagia 35, 66–72 (2020). https://doi.org/10.1007/s00455-019-10000-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00455-019-10000-5