
Abstract
This study aimed to identify changes in clusters of lifestyle behaviours (physical activity, screen time and diet) between the ages of 7 and 14 years, and to examine socio-demographic determinants of changes. Longitudinal analyses were performed on a sample of 9339 children from the UK Millennium Cohort Study (MCS) who had complete data on behaviours of interest at age 7 (wave 4) and 14 years (wave 6). Joint Correspondence Analysis (JCA) and k-means cluster analysis were used to identify clusters of lifestyle behaviours at both time waves. Multinomial logistic regressions were used to examine the associations between socio-economic variables and changes in cluster membership. Analyses were conducted separately for boys and girls. Clusters of behaviours at age 7 and 14 years were identified as healthy, mixed or unhealthy respectively. Compared to girls, a higher proportion of boys remained in the healthier cluster over time (19.1% vs. 13.1%) or became healthier (26.4% vs. 9.36%). A higher proportion of girls changed to an unhealthier cluster (57.2% vs. 33.9%). Indicators of lower socio-economic status, such as low family income, low parental education, and not living with both parents at age 7 were associated with unhealthier changes in cluster membership. Conclusion Lifestyle behaviours cluster in children and are susceptible to change over a 7-year period, with a high proportion of boys becoming healthier and a higher proportion of girls became unhealthier. Indicators of socio-economic status appear to be important in determining changes in clusters.
What is Known: • Poor lifestyle behaviours (i.e. unhealthy dietary habits, low physical activity, and sedentary behaviours) tend to cluster in children and adolescents. |
What is New: • Lifestyle behaviours cluster in children and are susceptible to changes between childhood and adolescence. Changes occur differently in boys and girls. Indicators of low socio-economic status are associated with unhealthier changes in behavioural clusters. |
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Lifestyle behaviours such as diet, physical activity, and sedentary behaviour have a significant impact on the health and wellbeing of children and young people [1, 2]. Previous studies suggest that the transition from childhood to adolescence is a critical period for behaviour formation [3, 4]. Adolescence is often accompanied by increases in screen time, decreases in physical activity, and poorer dietary behaviours, characterised by low consumption of fruit and vegetables, higher consumption of snacks and sugar-sweetened beverages, and breakfast skipping [3, 5,6,7,8]. The acquisition of poor lifestyle behaviours during adolescence can result in higher adiposity and cardiometabolic risk [9,10,11], lower cardio-respiratory fitness [9, 11], poorer self-rated health [12], poorer mental and emotional health [9, 11, 13], and lower quality of life [10].
Much of the evidence on health behaviours of adolescents comes from studies looking at individual health behaviours in isolation. However, lifestyle behaviours are likely to co-occur within groups of young people [9, 14]. For example, it has been shown that high screen time and high energy-dense snack consumption tend to cluster in young people, as does low fruit consumption and low physical activity [9, 14]. The effect of clusters of behaviours on health is likely to be greater than the effect of individual behaviours [15, 16]. A better understanding of how, and in whom lifestyle behaviours cluster, and how clusters of behaviours evolve over critical life periods of childhood is essential for the development of targeted interventions. However, to date, much of the evidence on clustering of health behaviours has come from cross-sectional studies [9, 17] or research that has not examined changes in clusters from childhood to adolescence [9]. Previous research has shown that a high proportion of 5–6 years old children belonged to an unhealthy behavioural cluster (high sedentary and low physical activity, or high TV and high energy-dense snack consumption) and tended to remain in the same cluster or move to the other unhealthy cluster by age 9 years [18]. Furthermore, in a study of adolescents aged 14–16 years at baseline, there was a high stability in clusters of lifestyle behaviours (healthy and unhealthy) over a 2-year period [19]. However, it is unknown how clusters of lifestyle behaviours change as children become adolescents. Given the significant social, environmental, and interpersonal changes that go alongside this transition [3, 20], it is imperative to understand in whom and how clusters of behaviours change during this period to help inform public health interventions.
An understanding of the determinants of behavioural clusters is required to underpin public health interventions aimed at promoting positive changes in health behaviours [17]. Given that behaviour change interventions that are theoretically based have been shown to be more effective than those without a theoretical underpinning [21, 22], it is useful to utilise behavioural theories to provide a framework for studying determinants of behavioural clusters. There is support for the use of socio-ecological models for understanding key determinants of health behaviours [23]. The socio-ecological model acknowledges that children are embedded within larger social systems and that characteristics of children interact with environments that underlie health behaviours [24].
Previous research has identified that indicators of socio-economic position, factors from a most pertinent level of the socio-ecological model, are important influences on children’s behavioural clusters, partly because they influence children’s attitudes, experiences, behaviours, and exposures to health risk factors [25]. For example, cross-sectional studies have shown that higher parental education is associated with behavioural clusters including high physical activity in schoolchildren [26], while girls and children from lower-educated parents have a higher prevalence of unhealthier clusters (for example, clusters including high consumption of sugar-sweetened beverages, high screen time, and low sleep duration) [26, 27]. However, wider socio-economic determinants of changes in clusters of lifestyle behaviours are poorly understood.
The results from this study provide support for intervening on multiple behaviours during childhood and adolescence, and to focus on gender differences and parental characteristics related to socio-economic disparities. More longitudinal analyses in different countries that help to better understand how young boys and girls from different socio-economic positions change their lifestyle behaviours over time may guide research to develop more specific and targeted interventions that better consider the needs of different subgroups of young people.
Methods
Study design and participants
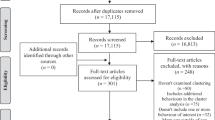
Data from the UK Millennium Cohort Study (MCS) (https://cls.ucl.ac.uk/cls-studies/millennium-cohort-study/) were used for the present analyses. Details of the design and sampling of MCS have been published elsewhere [28]. In brief, the MCS is an observational nationally representative longitudinal birth cohort study, which examines socio-economic, and health-related circumstances of children born in the UK between September 2000 and January 2002. At baseline (Wave 1), 18,818 children were first assessed when they were 9 months of age. For the present analyses, data when participants were aged 7 years (MCS4: January–December 2008; n = 14,043) and aged 14 years (MCS6: January 2015–March 2016; n = 11,872) were used (Fig. 1).

Sample selection flow-chart
Measures
All assessments of behaviours (physical activity, screen time, and dietary behaviours) were collected via parent report when participants were aged 7 years and via self-report when participants were aged 14 years. For the present analyses, variables were dichotomized considering the values which were closer to the guideline recommendations [29, 30] and the sample distribution.
Physical activity
Physical activity was reported as the number of days per week that the cohort member (child participant) took part in moderate-to-vigorous physical activity (MVPA). For the present analysis, MVPA was classified as ‘ < 5 days/week’ and ‘ ≥ 5 days/week’.
Screen time
The number of hours spent watching television (TV) and playing electronic games on a typical weekday was reported. Time spent TV viewing was dichotomized into ‘ < 3 h/day’ and ‘ ≥ 3 h/day’, and time spent using electronic games was dichotomized into ‘ < 1 h/day’ and ‘ ≥ 1 h/day’.
Dietary behaviours
Participants reported the servings of fruit eaten per day and the number of days per week breakfast was eaten. Fruit consumption was dichotomized into ‘ < 2 servings/day’ and ‘ ≥ 2 servings/day’, and the frequency of eating breakfast was dichotomized into ‘not every day’ and ‘everyday’.
Socio-economic variables at age 7 years
When participants were aged 7 years, parents reported their child’s sex, ethnicity, and their weekly household income according to the Organisation for Economic Co-operation and Development (OECD), participants whose OECD was below 60% of the median were considered in situations of poverty. Parents also reported their highest National Vocational Qualification (NVQ) level achieved and who the child lived with at home.
Statistical analyses
Analyses were conducted using Stata software version 14 (Stata, College Station, TX). Baseline sample characteristics were computed by sex and summarized as median and interquartile range (IQR) for continuous variables and frequencies and percentages for categorical variables. Kolmogorov–Smirnov test and histograms were used to assess the variable distribution. Mann–Whitney U tests were used for sex differences in continuous non-parametrical variables, and chi-square tests were used for sex differences in proportions.
At both time points, Joint Correspondence Analysis (JCA), which is an extension of the Multiple Correspondence Analysis (MCA), was conducted to explore the patterns in the categorical lifestyle variables. The analysis included five variables (physical activity, TV viewing, electronic games playing, breakfast eating, and fruit consumption). Analyses were carried out for boys and girls separately, as significant sex differences were shown in the lifestyle behaviours at baseline (Table 1). The dimensions revealed from the JCA that contained most of the data variability were used to inform the cluster analysis. The Calinski-Harabasz rule [31] was used to determine the optimal number of cluster solutions. The final number of clusters was decided based on interpretability and Calinski-Harabasz indexes at both time points and for both sexes. So, the number of clusters less or equal to five, with a higher Calinski-Harabasz index at both time points and for both sexes were selected. K-means cluster analysis was used to create three clusters of behaviours using the coordinates obtained from the JCA at both waves of assessment independently and for boys and girls separately. The stability (tracking) of cluster membership between ages 7 years and 14 years was examined using Kappa (K) statistics. The degree of tracking was evaluated using the cut-offs suggested by Landis and Koch [32]: < 0.2, poor; 0.2–0.4, fair; 0.41–0.6, moderate; 0.61–0.8, good; > 0.81, very good. The K value for the stability of cluster membership between 7 and 14 years was 0.254 for girls and 0.265 for boys, which shows fair agreement between baseline and follow-up cluster membership.
As the tracking of clusters was fair, we determined the profile of changes in behavioural clusters. Participants were classified depending on their continuity in the same cluster over time or by their change from one cluster to another. The categories to represent change between age 7 and 14 years were ‘remained in healthy cluster’, ‘remained in mixed cluster’, ‘remained in unhealthy cluster’, ‘changed to an unhealthier cluster (i.e. moved from healthy at age 7 to mixed or unhealthy at age 14; or from mixed at age 7 to unhealthy at age 14)’, and ‘changed to a healthier cluster (i.e. moved from unhealthy at age 7 to mixed or healthy at age 14; or from mixed at age 7 to healthy at age 14)’. Multinomial logistic regressions and the calculation of the corresponding odds ratios (OR) were used to examine the associations between socio-economic variables at baseline and the changes in cluster membership between ages 7 and 14 years. These models were performed for boys and girls separately and were adjusted for weight status and body fat percentage. Anthropometric covariates were collected by trained researchers during home visits when children were aged 7 years (MCS 4).
Results
From the initial MCS sample of 18,818 children, a final sample analytical sample of 9339 children (4660 girls and 4679 boys; 49.6% of the initial sample) had complete data on all variables of interest and were included in the present analyses (Fig. 1).
Characteristics of participants at age 7 years
Parents of boys had a high education level (NVQ above 3) (40.27% vs. 38.65%; p = 0.035) and had higher weekly family income (£405.27 ± 232.47 vs. £397.99 ± 234.50; p = 0.038) compared to girls (Table 1).
At age 7, girls participated in MVPA less frequently and skipped breakfast more frequently than boys. Boys consumed less servings of fruit and spent more time watching TV and playing electronic games than girls (Table 1).
Characteristics of behavioural clusters
For boys, the two dimensions (x and y) revealed by the JCA analyses explained 76.1% and 26.1% of the variability in the data at baseline, and the 89.4% and 10.4% variability in the data at follow-up. For girls, the two dimensions revealed by the JCA analyses explained 82.4% and 17.5% of the variability in the data at baseline, and the 86.5% and 13.4% variability in the data at follow-up (SF 1).
Three behavioural cluster solutions were produced: a healthy cluster (HC), a mixed cluster (MC), and an unhealthy cluster (UC) (Table 2). At baseline, 41.6% of boys and 52.6% of girls were in the HC, 36.5% of boys and 31.2% of girls were in the MC, and 21.9% of boys and 16.2% of girls were in the UC.
Among boys and girls at baseline, the HC was characterised by no breakfast skipping, lower TV viewing, higher MVPA, higher fruit consumption, and lower e-games playing than in the MC and UC (Table 2). The UC was characterised by lower MVPA, higher breakfast skipping, lower fruit consumption (especially in boys), higher TV viewing, and higher e-games playing than HC and MC. The MC was characterised by lower MVPA, low breakfast skipping, low TV watching higher, high electronic games playing, and fruit consumption lower than HC, but higher than UC (Table 2).
At follow up, there were differences in the behaviours that characterised each cluster, and clusters differed more between boys and girls than at baseline (Table 2). In boys, the three clusters had a similar percentage of high e-games playing (between 28.8 and 37.4%), while 76% of the girls with high e-games playing were in the UC. In girls, the MC was characterised by high fruit consumption (similar to HC), while in boys the MC was characterised by low fruit consumption (Table 2).
Changes in behavioural clusters between ages 7 and 14 years
Almost a fifth of boys (19.1%) who were in the HC at baseline remained in the HC at age 14 compared with 13.1% of girls (Table 3). A similar proportion of boys and girls who were in the MC at age 7 remained in the MC at age 14 years (11.2% and 9.1%), and a higher proportion of boys (7%) who were in the UC at age 7 remained in the UC at age 14 years compared to girls (3.4%). A high percentage of boys (26.4%) became healthier compared to girls (9.4%). A higher proportion of girls became unhealthier compared to boys (57.2% vs. 33.9%).
Associations between indicators of socio-economic and change in behavioural cluster profiles
After controlling for socio-economic indicators and anthropometric factors, compared to the boys who remained in HC, boys from low-income households were more likely to change to a healthier cluster than those from a higher-income household (OR (95% CI) = 1.43 (1.10, 1.84)) (Table 4). Boys with parents of higher education were less likely to remain in the MC, remain in the UC, and change to an unhealthier cluster, but also less likely to change to a healthier cluster than those of less educated parents (NVQ below 3 or other qualifications). Boys living with a single parent or other guardian were more likely to remain in MC, remain in UC, and change to an unhealthier cluster, but also less likely to change to a healthier cluster compared to those living with both parents.
Compared to the girls who remained in HC, girls from lower-income households were more likely to remain in UC and change to an unhealthier cluster (Table 5). Girls with higher educated parents were less likely to remain in MC, remain in UC, and change to an unhealthier cluster, but also less likely to change to a healthier cluster than those with lower parental education. Girls whose parents had other qualifications were two times more likely to remain in UC (OR (95% CI) = 2.25 (1.40, 3.62)), and two times more likely to change to a healthier cluster (OR (95% CI) = 2.14 (1.30, 3.52)) compared to girls who parents have lower education levels. Girls from White ethnic groups were less likely to remain in MC and less likely to change to a healthier cluster compared to girls from other ethnic groups. Girls living with a single parent or other guardian were more likely to remain in UC and change to an unhealthier cluster compared to those living with both parents.
Discussion
The aims of this study were to identify the changes in behavioural clusters from childhood to adolescence and to examine the associations between indicators of socio-economic status and changes in behavioural clusters over time. To the best of our knowledge, these are the first analyses to have examined changes in clusters of health behaviours over 7 years, to have considered the transition from childhood to adolescence, and to associate these changes to socio-economic indicators. Findings show low consistency in behavioural clusters over the 7 years ages 7 and 14 years with clear sex differences, as girls tend to change to unhealthier clusters, while boys tend to remain in healthier clusters. Indicators of socio-economic status during childhood appear to be important determinants of changes in behavioural clusters over the 7-year period.
The present study found that behavioural clusters are susceptible to changes over a 7-year period. At age 7 years, boys and girls had similar cluster prevalences, being in the HC was the most prevalent and in the UC was the least prevalent. This changed in boys to an almost equal prevalence across the three clusters, whereas among girls, the UC became the most prevalent and the HC the least prevalent at age 14 years. Previous studies have also shown that clusters of health behaviours have low to moderate tracking rates from ages 5–11 to 9–14 years [18]. Within the clusters in the present study, the number of boys with high e-games playing increased over time and was similarly distributed among the three clusters, and the number of boys and girls with high TV watching increased, especially in the UC. These results are in line with other studies reporting an increase in screen time from childhood to early adolescence, with differences in media used among boys and girls [33], and such increases in screen time could be driving the changes seen in certain clusters.
Results also showed that girls tended to change to unhealthier clusters, while boys tended to remain in HC or change to healthier clusters during the transition from childhood to adolescence. Previous literature has shown evidence of sex differences in lifestyle behavioural patterns over time. Research has shown that girls are more likely to become unhealthier in terms of lifestyle patterns of physical activity and sedentary behaviour [34, 35], especially when they came from lower socio-economic backgrounds [34]. Furthermore, a study by Daking et al. [19] found that boys were more likely to show unfavourable changes in lifestyle behavioural clusters (including diet, physical activity, and sedentary behaviour) across the transition from middle to late adolescence compared to girls. These findings show that variability in behaviours included in cluster analyses may influence the direction of sex differences regarding lifestyle patterns. Further research is needed examining the same behavioural clusters over critical time periods to be able to compare and unpack the sex differences in changes over time to inform interventions.
In addition to the gender differences seen in changes in clusters over time, indicators of socio-economic status appeared to impact changes in cluster membership. Among both boys and girls, living with a single parent (or another person different from the parents) was associated with a higher chance of remaining in UC or changing to unhealthier clusters, while higher parental education was associated with a higher likelihood of remaining in HC. For girls, lower family income was also associated with a higher probability of remaining in UC or changing to unhealthier clusters. Lower socio-economic status has been previously examined in association with lifestyle clusters in young people in cross-sectional studies [9]. For example, low parental education [36,37,38], low household income [36], and living in a deprived neighbourhood [39] have been associated with unhealthier lifestyle clusters, which may be related to a higher food insecurity/access to healthy foods [40], and/or lower access to a safe built environment that facilitate the physical activity practice. [41, 42]. Contrastingly, we also found that children with low socio-economic status had higher probabilities of transitioning to healthier clusters. These results may be partially explained by our reference group in the multinomial logistic regression analyses which was ‘remaining in HC’. Most of the children from high-socio-economic environments were in the healthier cluster at baseline (SF 2); therefore, these children had less probability of changing to healthier clusters than children from lower socio-economic groups. The results from this study provide support for intervening on multiple behaviours during childhood and adolescence, and to focus on gender differences and parental characteristics related to socio-economic disparities. More longitudinal analyses in different countries that help to better understand how young boys and girls from different socio-economic positions change their lifestyle behaviours over time may guide research to develop more specific and targeted interventions that better consider the needs of different subgroups of young people.
Strengths and limitations
Strengths of the study include the longitudinal study design, which includes a large nationally representative sample of British children, the inclusion of multiple health behaviours, and a thorough analysis of clustering. However, conclusions must be made in light of the limitations. Participants (12%) were excluded from the original sample due to missing data (SF 3), potentially limiting the generalisability of our findings. The outcome variables (physical activity, screen time, and dietetic variables) and socio-demographic variables were all assessed via questionnaires, which could lead to errors in the measurement due to socially desirable responses and/or inaccurate recall [43,44,45]. Furthermore, parents reported during the first wave of data collection and adolescents during the second wave which could change reporting bias [46].
Conclusions
Lifestyle behaviours cluster in children and are susceptible to change over a 7-year period with a high proportion of boys changing to healthier clusters compared to girls, and a higher proportion of girls changing to unhealthier clusters compared to boys. Children from lower socio-economic status backgrounds including low household income, low parental education, or not living with both parents were not only more likely to change to unhealthier clusters over this period but also more likely to change to healthier clusters. More longitudinal analyses in different countries are needed for a better understanding of the key drivers of change in clusters among subgroups of children, which is essential for the development of interventions targeting multiple health behaviours.
Data availability
Anonymised data from the MCS are accessible for academic use through the UK Data Service (https://ukdataservice.ac.uk/).
Abbreviations
- HC:
-
Healthy Cluster
- IQR:
-
Interquartile range
- JCA:
-
Joint Correspondence Analysis
- OECD:
-
Organisation for Economic Co-operation and Development
- MC:
-
Mixed cluster
- MCA:
-
Multiple Correspondence Analysis
- MCS:
-
Millenium Cohort Study
- MVPA:
-
Moderate-to-vigorous physical activity
- NVQ:
-
National Vocational Qualification
- OR:
-
Odds ratio
- TV:
-
Television
- UC:
-
Unhealthy Cluster
References
Liberali R, Del Castanhel F, Kupek E, de Assis MAA (2021) Latent class analysis of lifestyle risk factors and association with overweight and/or obesity in children and adolescents: systematic review. Child Obes 17:2–15. https://doi.org/10.1089/chi.2020.0115
Saunders TJ, Gray CE, Poitras VJ et al (2016) Combinations of physical activity, sedentary behaviour and sleep: relationships with health indicators in school-aged children and youth. Appl Physiol Nutr Metab 41:S283–S293. https://doi.org/10.1139/apnm-2015-0626
Haerens L, Vereecken C, Maes L, De Bourdeaudhuij I (2010) Relationship of physical activity and dietary habits with body mass index in the transition from childhood to adolescence: a 4-year longitudinal study. Public Health Nutr 13:1722–1728. https://doi.org/10.1017/S1368980010002284
Lommi S, Engberg E, Tuorila H et al (2021) Sex- and weight-specific changes in the frequency of sweet treat consumption during early adolescence: a longitudinal study. Br J Nutr 126:1592–1600. https://doi.org/10.1017/S0007114521001112
Rubín L, Gába A, Pelclová J et al (2022) Changes in sedentary behavior patterns during the transition from childhood to adolescence and their association with adiposity: a prospective study based on compositional data analysis. Archives of Public Health 80:1. https://doi.org/10.1186/s13690-021-00755-5
Kemp BJ, Parrish A-M, Cliff DP (2020) ‘Social screens’ and ‘the mainstream’: longitudinal competitors of non-organized physical activity in the transition from childhood to adolescence. Int J Behav Nutr Phys Act 17:5. https://doi.org/10.1186/s12966-019-0908-0
Júdice PB, Hetherington-Rauth M, Northstone K et al (2020) Changes in physical activity and sedentary patterns on cardiometabolic outcomes in the transition to adolescence: International Children’s Accelerometry Database 2.0. J Pediatr 225:166-173.e1. https://doi.org/10.1016/j.jpeds.2020.06.018
Gebremariam MK, Bergh IH, Andersen LF et al (2013) Are screen-based sedentary behaviors longitudinally associated with dietary behaviors and leisure-time physical activity in the transition into adolescence?. Int J Behav Nutr Phys Act 10. https://doi.org/10.1186/1479-5868-10-9
Alosaimi N, Sherar LB, Griffiths P, Pearson N (2023) Clustering of diet, physical activity and sedentary behaviour and related physical and mental health outcomes: a systematic review. BMC Public Health 23:1572. https://doi.org/10.1186/s12889-023-16372-6
Dalwood P, Marshall S, Burrows TL et al (2020) Diet quality indices and their associations with health-related outcomes in children and adolescents: an updated systematic review. Nutr J 19:118. https://doi.org/10.1186/s12937-020-00632-x
Rollo S, Antsygina O, Tremblay MS (2020) The whole day matters: understanding 24-hour movement guideline adherence and relationships with health indicators across the lifespan. J Sport Health Sci 9:493–510. https://doi.org/10.1016/j.jshs.2020.07.004
Zhang T, Lu G, Wu XY (2020) Associations between physical activity, sedentary behaviour and self-rated health among the general population of children and adolescents: a systematic review and meta-analysis. BMC Public Health 20:1343. https://doi.org/10.1186/s12889-020-09447-1
Rodriguez-Ayllon M, Cadenas-Sánchez C, Estévez-López F et al (2019) Role of physical activity and sedentary behavior in the mental health of preschoolers, children and adolescents: a systematic review and meta-analysis. Sports Med 49:1383–1410. https://doi.org/10.1007/s40279-019-01099-5
Pearson N, Griffiths P, Biddle SJ et al (2017) Clustering and correlates of screen-time and eating behaviours among young adolescents. BMC Public Health 17:533. https://doi.org/10.1186/s12889-017-4441-2
Poortinga W (2007) The prevalence and clustering of four major lifestyle risk factors in an English adult population. Prev Med (Baltim) 44:124–128. https://doi.org/10.1016/j.ypmed.2006.10.006
Slattery ML, Potter JD (2002) Physical activity and colon cancer: confounding or interaction? Med Sci Sports Exerc 34:913–919. https://doi.org/10.1097/00005768-200206000-00002
D’Souza NJ, Kuswara K, Zheng M et al (2020) A systematic review of lifestyle patterns and their association with adiposity in children aged 5–12 years. Obes Rev 21:e13029. https://doi.org/10.1111/obr.13029
Leech RM, McNaughton SA, Timperio A (2015) Clustering of diet, physical activity and sedentary behaviour among Australian children: cross-sectional and longitudinal associations with overweight and obesity. Int J Obes 39:1079–1085. https://doi.org/10.1038/ijo.2015.66
Dakin M, Manneville F, Langlois J et al (2021) Longitudinal patterns of lifestyle behaviours in adolescence: a latent transition analysis. Br J Nutr 126:621–631. https://doi.org/10.1017/S0007114520004316
Neufeld LM, Andrade EB, Ballonoff Suleiman A et al (2022) Food choice in transition: adolescent autonomy, agency, and the food environment. The Lancet 399:185–197. https://doi.org/10.1016/S0140-6736(21)01687-1
Hargreaves D, Mates E, Menon P et al (2022) Strategies and interventions for healthy adolescent growth, nutrition, and development. The Lancet 399:198–210. https://doi.org/10.1016/S0140-6736(21)01593-2
van Sluijs EMF, Ekelund U, Crochemore-Silva I et al (2021) Physical activity behaviours in adolescence: current evidence and opportunities for intervention. The Lancet 398:429–442. https://doi.org/10.1016/S0140-6736(21)01259-9
Golden SD, Earp JAL (2012) Social ecological approaches to individuals and their contexts. Health Educ Behav 39:364–372. https://doi.org/10.1177/1090198111418634
Sallis JF, Owen N, Fisher EB (2008) Ecological models of health behavior. In: Glanz K, Rimer BK, Viswanath K (eds) Health behavior and health education: theory, research, and practice. Jossey-Bass, San Francisco, CA, pp 465–486
Mahase E (2019) A decade on from Marmot, why are health inequalities widening? BMJ l4251. https://doi.org/10.1136/bmj.l4251
Fernández-Alvira JM, De Bourdeaudhuij I, Singh AS et al (2013) Clustering of energy balance-related behaviors and parental education in European children: the ENERGY-project. Int J Behav Nutr Phys Act 10:5. https://doi.org/10.1186/1479-5868-10-5
Pérez-Rodrigo C, Gil Á, González-Gross M et al (2015) Clustering of dietary patterns, lifestyles, and overweight among Spanish children and adolescents in the ANIBES study. Nutrients 8:11. https://doi.org/10.3390/nu8010011
Connelly R, Platt L (2014) Cohort profile: UK Millennium Cohort Study (MCS). Int J Epidemiol 43:1719–1725. https://doi.org/10.1093/ije/dyu001
World Health Organization (2020) WHO guidelines on physical activity and sedentary behaviour. Switzerland, Geneva
Public Health England (2016) The Eatwell Guide. https://www.gov.uk/government/publications/the-eatwell-guide. Accessed 29 Jul 2024
Calinski T, Harabasz J (1974) A dendrite method for cluster analysis. Commun Stat Theory Methods 3:1–27. https://doi.org/10.1080/03610927408827101
Landis J, Koch G (1979) The analysis of categorical data in longitudinal studies of behavioral development. In: Nesselroade J, Baltes P (eds) Longitudinal research in the study of behavior and development. Academic Press, New York, pp 233–261
Gebremariam MK, Totland TH, Andersen LF et al (2012) Stability and change in screen-based sedentary behaviours and associated factors among Norwegian children in the transition between childhood and adolescence. BMC Public Health 12:104. https://doi.org/10.1186/1471-2458-12-104
Wilhite K, del Pozo CB, Noetel M et al (2023) Socioeconomic position as a predictor of youth’s movement trajectory profiles between ages 10 and 14 years. Int J Behav Nutr Phys Act 20:88. https://doi.org/10.1186/s12966-023-01491-5
Farooq A, Basterfield L, Adamson AJ et al (2021) Moderate-to-vigorous intensity physical activity and sedentary behaviour across childhood and adolescence, and their combined relationship with obesity risk: a multi-trajectory analysis. Int J Environ Res Public Health 18:7421. https://doi.org/10.3390/ijerph18147421
Hardy LL, Grunseit A, Khambalia A et al (2012) Co-occurrence of obesogenic risk factors among adolescents. J Adolesc Health 51:265–271. https://doi.org/10.1016/j.jadohealth.2011.12.017
Matias TS, Silva KS, da Silva JA et al (2018) Clustering of diet, physical activity and sedentary behavior among Brazilian adolescents in the national school-based health survey (PeNSE 2015). BMC Public Health 18:1283. https://doi.org/10.1186/s12889-018-6203-1
Leech RM, McNaughton SA, Timperio A (2014) Clustering of children’s obesity-related behaviours: associations with sociodemographic indicators. Eur J Clin Nutr 68:623–628. https://doi.org/10.1038/ejcn.2013.295
Mandic S, Bengoechea EG, KirstenJ C, JohnC S (2017) Clustering of (un)healthy behaviors in adolescents from Dunedin, New Zealand. Am J Health Behav 41:266–275. https://doi.org/10.5993/AJHB.41.3.6
Barreiro-Álvarez MF, Latorre-Millán M, Bach-Faig A et al (2024) Family meals and food insecurity in Spanish adolescents. Appetite 195:107214. https://doi.org/10.1016/j.appet.2024.107214
Gu X, Keller J, Zhang T et al (2023) Disparity in built environment and its impacts on youths’ physical activity behaviors during COVID-19 pandemic restrictions. J Racial Ethn Health Disparities 10:1549–1559. https://doi.org/10.1007/s40615-022-01341-3
Gutiérrez-González E, Sánchez Arenas F, López-Sobaler AM et al (2023) Socioeconomic and gender inequalities in childhood obesity in Spain. Anales de Pediatría (English Edition) 99:111–121. https://doi.org/10.1016/j.anpede.2023.05.008
Quinlan C, Rattray B, Pryor D et al (2021) The accuracy of self-reported physical activity questionnaires varies with sex and body mass index. PLoS ONE 16:e0256008. https://doi.org/10.1371/journal.pone.0256008
Ravelli MN, Schoeller DA (2020) Traditional self-reported dietary instruments are prone to inaccuracies and new approaches are needed. Front Nutr 7. https://doi.org/10.3389/fnut.2020.00090
Svedberg P, Nygren JM, Staland-Nyman C, Nyholm M (2016) The validity of socioeconomic status measures among adolescents based on self-reported information about parents occupations, FAS and perceived SES; implication for health related quality of life studies. BMC Med Res Methodol 16:48. https://doi.org/10.1186/s12874-016-0148-9
Mak HW, Fancourt D (2020) Reading for pleasure in childhood and adolescent healthy behaviours: longitudinal associations using the Millennium Cohort Study. Prev Med (Baltim) 130:105889. https://doi.org/10.1016/j.ypmed.2019.105889
Acknowledgements
We would like to thank the families who voluntarily participated in the Millenium Cohort Study, as well as the Millennium Cohort Study team at the Centre for Longitudinal Studies who were involved in data collection and management of the study.
Funding
APS has a Ministerio de Universidades-Margarita Salas fellowship funded by the European Union–NextGenerationEU (Grant number: CT18/22). The Millennium Cohort Study is supported primarily by the UK Economic and Social Research Council with co-funding from a consortium of UK government departments.
Author information
Authors and Affiliations
Contributions
APS and NP participated in the conceptualization; APS, NP and NA participated in the methodology and performed the formal analysis; APS, NP, LBS and APK wrote the original draft; All authors contributed to the review and editing and the visualization of the paper, as well as all authors read and approved the final draft.
Corresponding author
Ethics declarations
Ethics approval
All procedures performed for each MCS wave were carried out in accordance with the Declaration of Helsinki and have received ethical approval from the National Research Ethics Service (NRES) Research Ethics Committee (REC) London–Central (REC ref: 13/LO/1786).
Consent to participate
Parents and participants provided written informed consent prior to completing all assessments.
Competing interests
The authors declare no competing interests.
Additional information
Communicated by Peter de Winter
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Peral-Suárez, Á., Sherar, L.B., Alosaimi, N. et al. Change in clusters of lifestyle behaviours from childhood to adolescence: a longitudinal analysis. Eur J Pediatr 183, 4507–4518 (2024). https://doi.org/10.1007/s00431-024-05729-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00431-024-05729-7