
Abstract
Background
Evidence suggests that participation in physical activity may support young people’s current and future mental health. Although previous reviews have examined the relationship between physical activity and a range of mental health outcomes in children and adolescents, due to the large increase in published studies there is a need for an update and quantitative synthesis of effects.
Objectives
The objectives of this study were to determine the effect of physical activity interventions on mental health outcomes by conducting a systematic review and meta-analysis, and to systematically synthesize the observational evidence (both longitudinal and cross-sectional studies) regarding the associations between physical activity and sedentary behavior and mental health in preschoolers (2–5 years of age), children (6–11 years of age) and adolescents (12–18 years of age).
Methods
A systematic search of the PubMed and Web of Science electronic databases was performed from January 2013 to April 2018, by two independent researchers. Meta-analyses were performed to examine the effect of physical activity on mental health outcomes in randomized controlled trials (RCTs) and non-RCTs (i.e. quasi-experimental studies). A narrative synthesis of observational studies was conducted. Studies were included if they included physical activity or sedentary behavior data and at least one psychological ill-being (i.e. depression, anxiety, stress or negative affect) or psychological well-being (i.e. self-esteem, self-concept, self-efficacy, self-image, positive affect, optimism, happiness and satisfaction with life) outcome in preschoolers, children or adolescents.
Results
A total of 114 original articles met all the eligibility criteria and were included in the review (4 RCTs, 14 non-RCTs, 28 prospective longitudinal studies and 68 cross-sectional studies). Of the 18 intervention studies, 12 (3 RCTs and 9 non-RCTs) were included in the meta-analysis. There was a small but significant overall effect of physical activity on mental health in children and adolescents aged 6–18 years (effect size 0.173, 95% confidence interval 0.106–0.239, p < 0.001, percentage of total variability attributed to between-study heterogeneity [I2] = 11.3%). When the analyses were performed separately for children and adolescents, the results were significant for adolescents but not for children. Longitudinal and cross-sectional studies demonstrated significant associations between physical activity and lower levels of psychological ill-being (i.e. depression, stress, negative affect, and total psychological distress) and greater psychological well-being (i.e. self-image, satisfaction with life and happiness, and psychological well-being). Furthermore, significant associations were found between greater amounts of sedentary behavior and both increased psychological ill-being (i.e. depression) and lower psychological well-being (i.e. satisfaction with life and happiness) in children and adolescents. Evidence on preschoolers was nearly non-existent.
Conclusions
Findings from the meta-analysis suggest that physical activity interventions can improve adolescents’ mental health, but additional studies are needed to confirm the effects of physical activity on children’s mental health. Findings from observational studies suggest that promoting physical activity and decreasing sedentary behavior might protect mental health in children and adolescents. PROSPERO Registration Number: CRD42017060373.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Physical activity interventions have a small positive effect on mental health in adolescents; however, well-designed intervention studies are needed to confirm these findings. |
The majority of studies in this review involved adolescent populations; therefore, future research should focus on preschoolers and children. |
Observational evidence suggests that promoting physical activity and decreasing sedentary behavior might support mental health in children and adolescents. Additional studies answering the questions when, where, what, how much and with whom are needed to better understand the relationship between physical activity, sedentary behavior and mental health in young people. |
1 Introduction
Mental disorders are expected to be one of the main causes of disability in developed countries by 2020 [1]. Prevention of mental disorders not only depends on the absence of psychological ill-being but also on the presence of psychological well-being. For the purpose of this review, the term psychological ill-being will be used to represent unpleasant feelings or emotions that impact the level of functioning, as well as preclinical and clinically diagnosed psychological disorders (e.g. depression and anxiety) [2, 3]. Conversely, psychological well-being is the combination of positive affective states and functioning with optimal effectiveness in personal and social life [2, 3]. Childhood and adolescence represent periods of rapid growth and development characterized by neuronal plasticity [4, 5], development of identity [6], and the establishment of behavioral patterns that may enhance or diminish mental health [7]. Thus, it is of interest to identify environmental exposures during these ages that may decrease the development of mental health disorders later in life [8].
Physical activity and sedentary behavior are two independent but related lifestyle behaviors that occupy all waking hours of a day. Physical activity is defined as any bodily movement that increases energy expenditure above resting energy expenditure [9]. Exercise is a subset of physical activity that is planned, structured, repetitive and purposeful that might have a different effect on mental health depending on the constituent elements (e.g. competitive vs. non-competitive) [10]. Sedentary behavior is defined as any waking behavior characterized by an energy expenditure ≤ 1.5 metabolic equivalents (METs), while in a sitting, reclining or lying posture [11].
The underlying mechanisms responsible for the effects of physical activity and sedentary behavior on mental health are unclear; however, several hypotheses have been proposed. For instance, it seems that participation in physical activity might enhance mental health via the release of endorphins [12], increases in brain-derived neurotrophic factor [13] and growth of new capillaries [14], which in turn might enhance the structural and functional composition of the brain. Other theoretical frameworks propose that increased levels of physical activity and reduced sedentary behavior might help to satisfy basic psychological needs (e.g. social connectedness, self-acceptance, and purpose in life), and consequently improve overall mental health in young people [15].
The recently published second edition of the Physical Activity Guidelines for Americans highlights that moving more and sitting less have enormous benefits for everyone [16]. However, the benefits of physical activity for mental health has received less attention in comparison to the physical health benefits. A previous review of reviews, published in 2011, showed that physical activity has beneficial effects on mental health in children and adolescents [17]. Nevertheless, the majority of included reviews were considered to be of low quality [17]. From 2010 to 2017, several systematic reviews and meta-analyses on this topic were published [18]. Most of the studies concluded there was a small significant overall association between physical activity and indicators of mental health [10, 19,20,21,22,23,24]; however, these systematic reviews and meta-analyses were focused on specific mental health outcomes (e.g. depression) [19,20,21, 24, 25], specific activities [26], mechanisms (i.e. neurobiological, psychosocial, and behavioral) [15] or specific age ranges (e.g. adolescents) [10]. Therefore, it is important to examine the overall effect of physical activity on the mental health of young people in order to guide health policies for this population.
Sedentary time has become a central component of our daily lives [27]. A review of reviews demonstrated that screen time was negatively associated with young people’s mental health in cross-sectional studies [17]. A recent systematic review in adolescents showed that leisure screen-based sedentary behaviors were related to higher psychological distress and lower self-esteem [28]. However, time spent in leisure screen-based activities is only a small part of the total sedentary time, and each sedentary activity may have a different effect on mental health [29]. For example, playing an instrument or reading a book may positively influence mental health, while excessive television viewing may diminish mental health. A previous systematic review concluded that, due to the low quality of the research conducted, the relationship between sedentary behavior and indicators of mental health in school-aged children and adolescents was indeterminate [30].
In summary, systematic reviews and meta-analyses have focused on specific lifestyle behaviors, mental health outcomes or a narrow age range, which dramatically limits their conclusions [31]. Therefore, it is imperative to extend and update all relevant literature, mapping the links between physical activity, sedentary behavior and mental health in preschoolers, children and adolescents. Although intervention studies can provide evidence for cause and effect, observational longitudinal studies provide complementary information, particularly about the longer-term effects of physical activity and sedentary behavior. Therefore, an integrated review of both intervention and observational studies is needed.
The aims of this review were to (1) determine the overall effect of physical activity on mental health in preschoolers, children and adolescents by conducting a systematic review and meta-analysis of available intervention studies; and (2) systematically synthesize recent observational evidence (both longitudinal and cross-sectional) on the association between physical activity and sedentary behavior with mental health in various pediatric age groups.
2 Methods
This study follows the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines [32]. Inclusion and exclusion criteria, as well as analytical methods, were specified in advance and registered in the PROSPERO (http://www.crd.york.ac.uk/PROSPERO) database, an international database of systematic reviews (PROSPERO reference number, CRD42017060373).
2.1 Search Strategy and Inclusion Criteria
The search was conducted in the PubMed and Web of Science electronic databases, and the dates of the published articles included in the search were from 1 January 2013 to 9 April 2018. Search terms were selected based on the eligibility criteria and outcomes of interest described in the following paragraph (see electronic supplementary Table S1). Two researchers (MRA and NEM) independently identified relevant articles by screening the titles and reviewing the abstracts. Full-text articles deemed eligible for review were examined to determine final eligibility; this process was conducted by the same two individuals (MRA and NEM).
Inclusion criteria were (1) design: intervention studies (randomized controlled trials [RCT], non-RCTs), and prospective longitudinal and cross-sectional studies focused on physical activity, sedentary behavior and mental health; (2) language criterion: articles only published in English or Spanish; (3) age criterion: preschoolers (2–5 years of age), children (6–11 years of age) and adolescents (12–18 years of age); and (4) topic criterion: articles examining the association between physical activity and/or sedentary behavior and at least one psychological ill-being (i.e. depression, anxiety, stress or negative affect) and/or psychological well-being (i.e. self-esteem, self-concept, self-efficacy, self-image, positive affect, optimism, happiness and satisfaction with life) outcome. With regard to exclusion criteria, we did not include conference proceedings and other types of grey literature because of the feasibility and limitations in the quality of reporting in conference abstracts [33]. Studies including individuals with physical or psychological disorders diagnosed by medical records, elite athletes, and animals were also excluded. Lastly, multiple health behavior intervention studies were excluded (e.g. co-interventions such as a dietary program combined with physical activity) because they preclude drawing conclusions on the isolated effect of physical activity or sedentary behavior on mental health outcomes.
2.2 Data Extraction
One author (MRA) extracted the following information from each eligible study: study background (name of the first author, year, and study location), sample characteristics (number of participants, age of participants, and number of girls and boys), design (intervention [RCT or non-RCT], or observational [cross-sectional or longitudinal]), and instruments used to assess physical activity and/or sedentary behavior and mental health outcomes. For intervention studies (RCTs and non-RCTs), we also extracted weeks of intervention, description of the program, intensity, duration and frequency. For longitudinal studies, we also extracted years of follow-up.
To reduce heterogeneity, sedentary behavior data were combined into three groups: recreational screen time (i.e. viewing television, using computer games, playing video games, using a mobile phone, using the internet), non-recreational screen time (i.e. homework using a screen) and non-screen time (i.e. music, passive transport, homework, reading, creative hobbies, talking). In regard to physical activity, data from general physical activity, outdoor play and sport participation were combined.
2.3 Meta-Analysis of Intervention Studies
All statistical analyses were performed using the Comprehensive Meta-Analysis software (version 3; Biostat Inc., Englewood, NJ, USA). A p value < 0.05 was accepted to indicate statistical significance. The meta-analysis of the intervention studies (RCTs and non-RCTs) was performed comparing the intervention versus control groups. Mean difference (post-test minus baseline values) and standardized mean difference were calculated for each group.
We also calculated the effect size (ES) using Cohen’s d and 95% confidence intervals (CIs) for standardized mean difference (post minus pre) on overall mental health (i.e. psychological ill-being and psychological well-being outcomes). For overall analyses, we reversed the ES obtained in studies focused on psychological ill-being in order to present results in the same direction (the higher the ES, the better the effect, as occurs with psychological well-being outcomes). Pooled ES of the effect of physical activity on psychological ill-being and psychological well-being was obtained using random-effects models. Heterogeneity was measured using the I2 statistic (total variability attributed to between-study heterogeneity, i.e. I2 < 25%, 50% and 75% was considered as low, moderate and high heterogeneity, respectively) [34]. In addition, we examined how the duration of the physical activity interventions (grouped as < 60 or ≥ 60 min) could influence mental health. Funnel plots were calculated and the Egger’s test was conducted to assess risk of publication bias. The trim and fill procedure was also performed to adjust for the suspected publication bias where the pooled ES was recalculated to incorporate hypothetical missing studies if necessary.
Subgroup analyses were performed comparing the RCT and non-RCT studies. In addition, we performed a sensitivity analysis excluding those studies categorized as high risk of bias. As secondary analysis, we performed one meta-analysis of only those studies that measured psychological ill-being outcomes and another meta-analysis of only those studies that measured psychological well-being outcomes. Lastly, we performed a subgroup analysis examining preschoolers, children and adolescents, separately.
2.4 Data Synthesis of Observational Studies
Findings from observational studies were rated using the method first employed by Sallis et al. [35], and more recently used by Lubans et al. [36] and Smith et al. [37]. If 0–33% of studies reported a statistically significant association for the outcome of interest, the result was classified as no association (Ø); if 34–59% of studies reported a significant association, or if fewer than four studies reported on the outcome, the result was classified as being inconsistent/uncertain (?); and if ≥ 60% of studies found a statistically significant association, the result was classified as positive (+) or negative (−), depending on the direction of the association. When the association was examined only in girls or boys, we specified it as ‘♀’ or ‘♂’, respectively. If the association between independent and dependent variables was tested or was significant in only one sex (girls or boys), we quantified it with a 0.5 score instead of 1.
2.5 Criteria for Risk of Bias Assessment
Risk of bias was individually assessed for each eligible study by two researchers (MRA and FEL) and disagreements were solved in a consensus meeting. Inter-rater agreement for the risk of bias assessment was determined by the percentage agreement between evaluators (MRA and FEL). Furthermore, an intraclass correlation coefficient (ICC) analysis was conducted using SPSS software, version 21.0 (IBM Corporation, Armonk, NY, USA).
Different checklists, depending on the study design, were used to assess the risk of bias. First, the Cochrane Collaboration’s tool was used for assessing risk of bias in RCTs. The scores for each criterion were summed to provide a total score out of 7, using the following categories: 1–2 ‘low risk’, 3–4 ‘medium risk’, and 5–7 ‘high risk’ [38]. The criteria for assessing risk of bias in non-RCTs, prospective longitudinal studies and cross-sectional studies were created based on the STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) criteria [39] and the Effective Public Health Practice Project (EPHPP) [40]. A risk of bias score was calculated based on the following five criteria, first employed by Smith and Madden [41]: (1) adequate description of the study sample (i.e. number of participants, mean age and sex); (2) adequate assessment/reporting of physical activity (i.e. validity/reliability of physical activity measurement reported and/or detailed description of the testing protocol); (3) adequate assessment of the mental health outcomes (i.e. validity/reliability of the outcome measure reported and/or measurement procedure adequately described); (4) adequate adjustment of confounders (i.e. age and sex); and (5) description of both the numbers and reasons for withdrawals and dropouts. Based on previous methodology, the scores were summed to provide a total score out of 5, using the following categories: 0–2 ‘low risk’, 3 ‘medium risk’, and 4–5 ‘high risk’.
3 Results
3.1 Selection Process
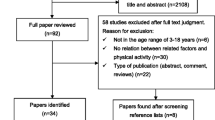
The search yielded 4624 original articles, from which 282 were screened in full-text (see Fig. 1 for full search details). Finally, a total of 114 original articles were included in the systematic review: 4 RCTs, 14 non-RCTs, 28 prospective longitudinal studies and 68 cross-sectional studies. Of the 18 intervention studies, 12 (3 RCTs [42,43,44] and 9 non-RCTs [45,46,47,48,49,50,51,52,53]) were included in the meta-analysis and 6 were excluded (3 did not report the ES data needed [54,55,56], 2 included an active control group performing other types of physical activity [57, 58] (i.e. yoga vs. combined exercise [57] and Tai-Chi vs. gymnastics [58]) and 1 did not include a control group [59]). The list of excluded articles categorized based on the exclusion criteria can be seen in electronic supplementary Table S2.

Results of the study selection process. RCT randomized controlled trial
3.2 Summary of Included Studies
A detailed description of the intervention studies (RCTs and non-RCTs) is provided in Table 1. We conducted a meta-analysis of the RCT and non-RCT studies (see Fig. 2) to determine the overall effect of physical activity on mental health in different pediatric age groups. A summary of the associations of different types of physical activities (i.e. physical activity, sport participation and outdoor play) and different types of sedentary behaviors (i.e. recreational screen time, non-recreational screen time and non-screen time) with psychological ill-being and psychological well-being in the different pediatric age groups is reported in Tables 2 and 3, respectively. Further details on the study characteristics of prospective longitudinal studies and cross-sectional studies are presented in electronic supplementary Tables S3 and S4, respectively. Moreover, the results of the risk of bias assessment can be found in electronic supplementary Tables S5–S8.

Forest plot of the pooled effect size and confidence intervals of exercise on overall mental health. RCT randomized controlled trial, Std Diff standard difference, CI confidence interval
3.3 Characteristics of Intervention Studies (Randomized Controlled Trials [RCTs] and Non-RCTs)
3.3.1 Sample Characteristics
Sample sizes of intervention studies (n = 18) ranged from 20 [48] to 420 [50]. One study did not have a control group [59], while two studies included an active control group performing other types of physical activity [57, 58] (i.e. yoga vs. combined exercise [57] and Tai-Chi vs. gymnastics [58]). Lastly, 10 studies included adolescents [42,43,44,45,46, 49,50,51,52, 58], while 8 studies included children [47, 48, 53,54,55,56,57, 59], of whom 4 were focused on overweight/obese adolescents [43, 46] or children [48, 55]. We did not find any studies focused on preschoolers (2–5 years of age).
3.3.2 Outcome Characteristics
Of the 18 studies included in the systematic review, 8 provided data on psychological ill-being [44, 45, 47, 49, 51, 54, 55, 58]. Specifically, 5 studies provided data on generic psychological ill-being [44, 47, 49, 51, 54], 2 on depression [49, 55], 3 on anxiety [49, 55, 58] and 1 on stress [45]. On the other hand, 13 studies provided data on psychological well-being [42,43,44, 46, 48, 50,51,52,53, 56,57,58,59]. Specifically, 1 study focused on a total score of psychological well-being [44], 7 on self-esteem [42, 43, 46, 48, 51, 53, 57], 6 on self-image [43, 44, 48, 52, 58, 59], 1 on self-concept [56], 1 on self-efficacy [50, 56], 2 on happiness [53, 58] and 2 on positive emotions [43, 44].
3.3.3 Exposures and Comparison Conditions
Most of the study interventions ranged from 8 to 28 weeks [42,43,44,45,46, 48, 49, 51,52,53,54,55,56,57, 59]; however, two studies lasted for more than 28 weeks [47, 58] and one study lasted for < 8 weeks [50]. Of note, our search also included physical activity and sedentary behavior interventions, yet only exercise and sport interventions were available: mind-body exercise programs [45, 50, 52, 53, 57, 58], aerobic exercise programs [43, 44, 55], resistance exercise programs [43], combined exercise programs (aerobic + resistance) [42,43,44, 47, 49, 56], football [48, 59], exergames [46, 54] and CrossFit [51]. The majority of the studies (80%) implemented exercise sessions for 60 min [42, 46, 48, 51, 52, 55, 58], two to three times per week (80%) [42,43,44, 46,47,48,49, 51,52,53, 56, 59]. Finally, only five studies reported the intensity during the program (50–80% maximum heart rate) [42, 44, 48, 49, 51]; however, none of them controlled individual intensity, for instance by heart rate monitors, to estimate the time spent in 50–80% of their maximum heart rates.
3.4 Synthesis of Findings
3.4.1 Meta-Analysis of Intervention Studies
Figure 2 presents the meta-analysis of the exercise versus control effects, showing a small significant pooled ES for the efficacy of the exercise on overall mental health (ES = 0.173, 95% CI 0.106–0.239; p < 0.001, I2 = 11.3%). No significant publication bias was detected based on Egger’s test (p = 0.139) and visual inspection of the funnel plot (Fig. 3). Moreover, the trim and fill procedure showed that the ES estimate was not changed, and thus no correction for potential publication bias was needed. The analysis conducted by meeting the physical activity recommendations during the exercise program (< 60 or ≥ 60 min) showed that those programs with ≥ 60 min of exercise activities significantly improved the overall mental health compared with those peers who engaged in an exercise program of < 60 min (ES = 0.277, 95% CI 0.138–0.415; p < 0.001, I2 = 37.22%) (Fig. 4).

Funnel plot to assess publication bias in the effects of exercise on overall mental health. Diagonal lines represent pseudo-95% confidence intervals. The y-axis represents the standard error (weight in the pooled analysis), and the x-axis shows the effect size; thus, the vertical line represents the calculated estimated effect of overall mental health

Grouping analysis of not meeting (< 60 min) and meeting (≥ 60 min) the physical activity recommendations against the effect size on overall mental health. The more positive the effect size, the better the changes in overall mental health. Overall effect size for each group (meeting or not meeting the recommendations) is shown in grey. RCT randomized controlled trial, Std Diff standard difference, CI confidence interval
When the analyses were performed separately for RCTs and non-RCTs, the results were ES = 0.094, 95% CI 0.017–0.172; p = 0.017, I2 = 0% for RCTs, and ES = 0.269, 95% CI 0.137–0.400; p < 0.001, I2 = 31.8% for non-RCTs. Furthermore, after removing the studies with a high risk of bias, the result was similar (ES = 0.165, 95% CI 0.098–0.232; p < 0.001, I2 = 10.3%) [data not shown].
Secondary analyses showed that exercise improved psychological ill-being (ES = 0.130, 95% CI 0.036–0.224; p = 0.007, I2 = 0%) and psychological well-being (ES = 0.189, 95% CI 0.084–0.294; p < 0.001, I2 = 32.3%) when they were considered as two independent constructs (electronic supplementary Figs. S1a and b, respectively). No significant publication bias was observed for either psychological ill-being or psychological well-being (Egger’s test, p = 0.906 and 0.138, respectively). Funnel plots are shown in electronic supplementary Fig. S2a and b. Therefore, the trim and fill procedure showed no correction for potential publication bias for psychological ill-being and psychological well-being, respectively.
Lastly, when the analyses were performed separately for children and adolescents (no studies were found in preschoolers), the results were similar for adolescents (ES = 0.181, p ≤ 0.001; I2 = 15.7%) and children (ES = 0.209, p = 0.141; I2 = 0%); however, the summary effect for children was not statistically significant.
3.4.2 Summary of Findings from Observational Studies: Prospective Longitudinal and Cross-Sectional Studies
3.4.2.1 Association Between Physical Activity and Mental Health
The association between physical activity and psychological ill-being components (i.e. depression, anxiety, stress, negative affect, total psychological distress) was investigated in 52 studies, of which 13 studies were longitudinal, 35 were cross-sectional, and 4 studies reported both longitudinal and cross-sectional data. Furthermore, the association between physical activity and psychological well-being components (i.e. self-esteem, self-concept, self-efficacy, self-image, positive affect, satisfaction with life and optimism) was investigated in 39 studies, of which 8 were longitudinal and 31 were cross-sectional.
No studies were conducted on preschoolers, while 11 studies were conducted on children, 63 studies were conducted on adolescents, and three studies were conducted on children and adolescents together. Only five studies evaluated objectively measured physical activity by accelerometry [60,61,62,63]. Depression was the most studied psychological ill-being outcome (80%), while self-esteem, self-image and satisfaction with life were the most studied psychological well-being outcomes (28%, 23%, and 30%, respectively).
There was evidence for a statistically significant association between physical activity and depression (28.5 of 43 studies, 66.3%), stress (6 of 6 studies, 100%), negative affect (3 of 4 studies, 75%) and a total psychological distress (5 of 8 studies, 62.5%). There was an unclear association between physical activity and anxiety (7 of 12 studies, 58.3%) in children and adolescents. Regarding psychological well-being outcomes, there was evidence for a statistically significant association between physical activity and self-image (6.5 of 9 studies, 72.2%), satisfaction with life (10 of 12 studies, 83.3%) and total psychological well-being (7 of 7 studies, 100%). There was also an unclear association between physical activity and self-esteem (5 of 11.5 studies, 43.5%). Lastly, there were insufficient studies (< 4 studies) to determine the association between physical activity and self-concept, self-efficacy, positive affect and optimism in children and adolescents.
3.4.2.2 Association Between Sedentary Behavior and Mental Health
The association between sedentary behavior and psychological ill-being outcomes (i.e. depression, anxiety, stress, negative affect) was investigated in 32 studies, of which 8 were longitudinal, 19 were cross-sectional, and 5 reported both longitudinal and cross-sectional data. The association between sedentary behavior and psychological well-being outcomes (i.e. self-esteem, self-concept, self-efficacy, self-image, positive affect, satisfaction with life and optimism) was investigated in 16 studies, of which 3 were longitudinal and 13 were cross-sectional.
Only 3 studies were conducted on preschoolers, 8 studies were conducted on children, 28 studies were conducted on adolescents, and 3 studies were conducted on children and adolescents. Only 3 studies evaluated objectively sedentary behavior by accelerometry [64,65,66]. Depression was the most studied psychological ill-being outcome examined (65%), while self-esteem and self-image were the most studied psychological well-being outcomes (35% and 32%, respectively).
There was only evidence for a statistically significant positive association between sedentary behavior and depression (35 of 21.5 studies, 61.4%). However, the associations between sedentary behavior and anxiety (4.5 of 10 studies, 45%) and total psychological distress (7 of 17 studies, 41.1%) were considered to be unclear. Insufficient studies were found testing the association between sedentary behavior and stress [67] and negative affect [68] in children and adolescents. Regarding psychological well-being, there was evidence for a statistically significant inverse association between sedentary behavior and satisfaction with life (4 of 5 studies, 80%). There was an unclear association between sedentary behavior and self-esteem (7 of 14.5 studies, 48%), self-image (5 of 13.5 studies, 37%) and total psychological well-being score (4 of 9 studies, 44.4%). There were insufficient studies (< 4 studies) testing the association between sedentary behavior and self-concept, self-efficacy, and positive affect, and optimism in children and adolescents.
3.5 Risk of Bias Assessment
There was a strong agreement among researchers in the risk of bias assessment (ICC 0.80). Overall, three RCTs showed medium risk of bias [43, 44, 57], while only one RCT showed a high risk of bias [42]. Furthermore, eight non-RCTs showed low risk of bias [45, 46, 48, 49, 51, 52, 54, 58], three showed medium risk of bias [50, 53, 55] and three showed high risk of bias [47, 56, 59]. Most studies included an adequate description of the study sample (95%), as well as an adequate assessment of outcome measures (93%).
In addition, 20 prospective longitudinal studies showed a low risk of bias (71.4%), and 8 studies showed a medium risk of bias (28.6%). Additionally, 33 cross-sectional studies showed a low risk of bias (48.5%), 19 cross-sectional studies showed a medium risk of bias (28%) and 16 cross-sectional studies showed a high risk of bias (23.5%). Only 46.5% of longitudinal cohort studies used a validated and/or reliable tool to evaluate physical activity or sedentary behavior, while 44% of cross-sectional studies used a validated and/or reliable tool to evaluate physical activity or sedentary behavior.
4 Discussion
The aims of this review were to (1) determine the overall effect of physical activity on mental health in preschoolers, children and adolescents; and (2) synthesize recent observational evidence (both longitudinal and cross-sectional studies) examining the association between physical activity, sedentary behavior and mental health in these pediatric age groups. The main findings of this review are as follows: (1) there was a small positive effect of exercise interventions on mental health outcomes (i.e. psychological ill-being and psychological well-being) in adolescents; (2) physical activity was inversely associated with psychological ill-being (i.e. depression, stress, negative affect, total physiological distress) and positively associated with psychological well-being (i.e. self-image, satisfaction with life and happiness, and psychological well-being); and (3) there was a positive association between sedentary behavior and depression, and an inverse association between sedentary behavior and satisfaction with life and happiness in children and adolescents. Therefore, findings from the present research suggest that increased physical activity and decreased sedentary behavior may enhance mental health in children and adolescents.
4.1 Effects of Intervention Studies on Mental Health
Our meta-analytical approach allowed us to determine the overall effect of exercise interventions on mental health in children and adolescents. The results suggest that there are small significant effects of exercise on reducing psychological ill-being and improving psychological well-being, as separate effects. Larger effects may not be expected due to the good levels of mental health experienced by the majority of young people. Future interventions are warranted to determine if physical activity effects are consistent in youth with poor mental health. It is important to note that not all young people will experience increased physical competence or improved perceived appearance after completing a physical activity regimen (e.g. by not gaining strength, not experiencing weight loss, or losing games all the time). Indeed, poorly designed physical activity interventions may thwart the satisfaction of young people’s needs and lead to decreases in perceived competence and global self-esteem [71]. Therefore, future intervention studies might consider the use of evidence-based physical activity strategies to maximize the positive effect of physical activity on mental health outcomes, e.g. the Supportive, Active, Autonomous, Fair, Enjoyable (SAAFE) principles and practical strategies designed by Lubans et al. [72].
Of note, when the analyses were performed separately for children and adolescents (no studies were found in preschoolers), the results were similar. However, the summary effect was not statistically significant for children. This finding is likely due to the small number of studies including children (only three studies). As such, more studies are needed in preschoolers (2–5 years of age) and children (6–11 years of age) to test the effect of physical activity on mental health.
The relationship between interventions and overall mental health (i.e. both psychological ill-being and psychological well-being) has not been previously studied using meta-analyses. As such, this work complements previous meta-analyses and reviews focused on specific mental health components. For instance, our findings are consistent with the meta-analysis published by Brown et al. [19], who found a small positive effect of exercise on depression. Similarly, our findings are in accord with the review conducted by Larun et al. [69], who found a significant moderate effect of exercise on depressive symptoms. The larger ESs observed in the review by Larun et al. [69] may be explained by their inclusion of children and adolescents with major depression symptoms, who were not included in this review. This hypothesis is consistent with the findings of Carter et al. [70], who found that exercise appears to improve depressive symptoms in adolescents, especially in clinical samples diagnosed with major psychological disorders.
In the present review, we found that compared with those peers who engaged in exercise activities for < 60 min/day, participants who met the physical activity recommendations significantly improved their overall mental health. In the context of the literature, this review expands on the compelling evidence of general cardiometabolic health benefits of physical activity recommendations by providing further evidence for the mental health benefits for children and adolescents [73]. However, it is important to note that most of the intervention studies were non-RCTs (9 of 13 studies, 70%) and none had a low risk of bias. Moreover, most of the intervention studies included adolescents (11 of 13 studies, 85%). Therefore, well-designed intervention studies are needed to confirm our findings, especially in preschoolers and children.
4.2 Observational Studies on the Association Between Physical Activity and Mental Health
Physical activity was inversely associated with psychological ill-being (i.e. depression, stress, negative affect, overall physiological distress) and positively associated with psychological well-being (i.e. self-image, satisfaction with life and happiness, and overall psychological well-being) in children and adolescents. Therefore, findings from the present systematic review suggest that increased levels of physical activity may have a positive effect on mental health in children and adolescents.
Each type of physical activity (e.g. sports participation, outdoor play or active commuting) may contribute in distinct ways to mental health in children and adolescents. For instance, Schneider et al. [74] found that adolescents who participated in non-aesthetic sports (e.g. swimming, horseback, judo or hockey) were satisfied with their physical appearance, while participation in aesthetic activities such as ballet and rhythmic gymnastics was significantly correlated with body dissatisfaction [74]. This is perhaps not surprising considering the strong focus on physical appearance inherent in aesthetic activities. In addition, it seems that adolescents who continue to participate in team sports during high school report lower levels of depression in early adulthood [75, 76]. In contrast, number of years participating in individual sports was not significantly associated with depressive symptoms in early adulthood [76, 77]. Moreover, Brunet et al. [78] found that sport participation during adolescence, but not overall physical activity, was associated with decreased levels of depression in adulthood. Therefore, it seems that sport participation, especially team sports without any aesthetic implication, is the type of physical activity most strongly associated with mental health in young people. This result may be explained by the fact that team sports provide important peer support during childhood and adolescence, which might help to buffer the effects of stressful life events that occur during adolescence [79]. Of note, the relationship between sport and mental health might be potentially bidirectional [80]. Specifically, it seems that young people who experience greater levels of psychological ill-being have lower subsequent levels of sport participation [80]. Therefore, experimental studies on sport participation and mental health are required to draw conclusions about the causality of our findings.
Interestingly, the relation between physical activity and mental health may be influenced by several potential moderators and mediators. For instance, Adachi and Willoughby [81] suggested that enjoyment of physical activity positively influences self-esteem, while Wagnsson et al. [82] demonstrated that perceived sport competence plays an important mediating role in the relationship between sport participation and self-esteem. In addition, Reigal et al. revealed that the association between physical activity and satisfaction with life may be influenced by the social context [83]. Moreover, Ho et al. [84] found that resilience was a significant mediator of the association between physical activity and psychological well-being in young people.
In the present review, we observed a paucity of studies analyzing the relationship between physical activity and anxiety, self-esteem, self-concept, self-efficacy, positive affect and optimism. Although experimental studies are considered to provide the highest level of evidence, observational studies may be useful for determining the relationship between physical activity and less-studied mental health outcomes. Of note, type of physical activity (e.g. sports participation, outdoor play or active commuting) might be considered when studying the relationship between physical activity and mental health in young people. Lastly, further studies might consider the interrelationship between other environmental factors, such as enjoyment or perceived sport competence, that could differently influence the mental health of children and adolescents.
4.3 Possible Mechanisms for the Role of Physical Activity in Mental Health
While the evidence examining the relationship between physical activity and mental health is growing, the underlying plausible mechanisms of this association cannot be elucidated in our review. In this context, a range of neurobiological, psychosocial and behavioral mechanisms have been previously proposed by Lubans et al. [15].
First, physical activity may have a positive effect on the structure and function of the brain, which is now quantifiable as a result of technological advancement (e.g. magnetic resonance imaging [MRI]). Using this technology, for instance, a recent RCT in children showed that a 9-month physical exercise intervention improved the structure and function of brain networks related to cognitive function [85]. Therefore, it is possible that physical activity changes brain structure and function, which in turn has a positive effect on mental health. Regarding the cellular and molecular bases of mental health, it is well-known that decreased levels of brain-derived neurotrophic factor (BDNF), which plays a crucial role in the growth and healthy maintenance of neurons [86], is associated with increased levels of anxiety and depression [87]. Exercise is known to increase BDNF levels in the central nervous system, which may improve anxiety and depressive symptoms [13]. Another explanation might be that exercise, by increasing brain dopamine, serotonin, and noradrenaline concentrations, might not only improve mood but also protect against the onset of mental disorders [88]. More research is needed to understand the neurobiological mechanisms that elicit the positive effects of physical activity on mental health in young people.
Second, evidence suggests a causal link between physical self-concept (i.e. perceived appearance, perceived fitness and perceived competence) and mental health (e.g. global self-concept, self-esteem) [15]. Social support and autonomy are also plausible psychosocial contributors to mental health in young people [89]. Therefore, the effects of physical activity on mental health in young people might be mediated by several psychosocial paths.
Finally, a range of potential behavioral mechanisms might explain the effect of physical activity on mental health outcomes, including sleep duration, sleep efficiency, sleep onset latency, and reduced sleepiness [15]. However, there are insufficient studies to draw firm conclusions about any of these behavioral mechanisms.
4.4 Observational Studies on the Association Between Sedentary Behavior and Mental Health
Significant associations were found between higher time spent in sedentary behaviors and higher depression, lower satisfaction with life and lower happiness in children and adolescents, while other psychological ill-being and psychological well-being outcomes (i.e. stress, anxiety, negative affect, self-esteem, self-concept, self-efficacy, positive affect and optimism) have not been studied. Therefore, the present research suggests that decreasing sedentary behavior may have a positive effect on depression, satisfaction with life and happiness in children and adolescents [67, 90, 91]. There is a lack of data for preschoolers (2–5 years of age). Given that there are a variety of developmental changes happening in the brain during the early stages of human life [5], more studies involving preschoolers are warranted.
The findings of this systematic review are consistent with those from Hoare et al. [28], who provided strong evidence for the positive relationship between sedentary behavior and depressive symptoms among adolescents [28]. These findings were also reported by Liu et al. [92] in a meta-analysis of observational studies in children and adolescents. However, these investigators found that compared with the reference group who had no sedentary behavior, there was a non-linear dose–response association of screen time-based sedentary behavior (i.e. watching television, computer/internet use, and video gaming) with a decreasing risk of depression at sedentary time < 2 h/day, with the lowest risk being observed for 1 h/day. These findings suggest that recreational screen time in moderation is not harmful. On the other hand, a number of longitudinal studies suggested that lower levels of sedentary behavior were weakly associated or not associated with lower levels of anxiety [67, 93], stress [67] and total psychological distress [94]. A stronger association between sedentary behavior and anxiety [93, 95] and total psychological distress [96, 97] was found in cross-sectional studies. Moreover, as discussed for physical activity, the association between sedentary behavior and psychological distress may be bidirectional. Therefore, experimental studies on sedentary behavior and mental health are required to elucidate the causality of these associations.
While the eligibility criteria allowed for a broad range of sedentary behaviors, the most frequently examined behavior in children and adolescents was a measure of total recreational screen time (i.e. recreational use of computer and television viewing) [76, 91, 97,98,99]. It is widely known that prolonged television viewing is the most prevalent and pervasive sedentary behavior in developed countries and has been associated with morbidity and mortality [100]. This finding is consistent with that of Bickham et al. [101] who found that television viewing, and not recreational use of computers during adolescence, was associated with depressive symptoms over time. In addition, similar findings were reported by Grøntved et al. [102] for children. However, this finding is contrary to other studies that have suggested that recreational use of computers was more strongly associated with poorer mental health than television viewing in children and adolescents [95, 103]. In addition, social media technology commonly used by young people on tablets/mobile phone (e.g. Facebook, Instagram and Snapchat) may encourage adolescents to compare themselves with their peers [104], and consequently increase their body dissatisfaction when discrepancies are found between perceived and ideal body shape. Therefore, research is required to examine if the type (e.g. watching television, using the computer/internet, or playing video games) of sedentary behavior versus sedentariness itself explains the association between sedentary behavior and mental health in young people.
Due to the lack of research, it was not possible to determine the strength of association between sedentary behavior and stress, anxiety, negative affect, self-esteem, self-concept, self-efficacy, positive affect and optimism; more research (including observational studies) is warranted. As such, experimental research is needed to elucidate the effect of reducing sedentary behavior on young people’s mental health. Future studies are encouraged to explore the following: (1) how much screen time is acceptable for young people (e.g. > 2 h vs. < 2 h); (2) to what extent does screen-time content influence young people’s mental health (e.g. violence vs. non-violence); and (3) are the effects of screen time consistent if young people are watching or playing with others (e.g. gaming alone vs. gaming with friends).
4.5 Possible Mechanisms for the Role of Sedentary Behavior in Mental Health
Although the underlying mechanisms responsible for the effects of sedentary behavior on mental health in children and adolescents are still unclear, several hypotheses have been proposed. First, given that it often takes place alone, sedentary behavior may elicit feelings of loneliness and, consequently, negatively impacts on mental health [105]. Thus, it seems that higher levels of screen time (e.g. time spent watching television and using the internet) may lead to social isolation, and hence to mental health problems [107]. Second, cultural messages transmitted through media may affect other behaviors related to mental health (e.g. eating disorders and aggressive behavior) [106]. Third, excessive media exposure often occurs at day or night. During the day, time spent on screen-based activities may replace time participating in more productive and/or active activities, especially activities involving physical activity [107] and interpersonal communication [108]. At night, screen-based activities can displace sleep, which is crucial for normal cognitive and emotional development [106]. In both scenarios, the replacement of healthy with unhealthy behaviors may have negative consequences on the mental health of young people. Given the limited evidence, more studies focused on potential mechanisms explaining the relationship between sedentary behavior and mental health are needed to confirm these hypotheses. Since nothing is known about them, studies focusing on neurobiological mechanisms are of particular interest.
4.6 Literature Gaps and Future Research
-
Most of the studies included in this review were focused on adolescents. Therefore, future research is required, especially in preschoolers and children.
-
Well-designed physical activity interventions are needed to confirm our findings. In addition, experimental studies on sedentary behavior and mental health are required to draw conclusions in regard to cause and effect.
-
Mediation models are needed to identify the mechanisms (i.e. neurobiological, psychological and behavioral) responsible for any changes in mental health resulting from physical activity and sedentary behavior.
-
Type of physical activity (e.g. sports participation, outdoor play or active commuting) and type of sedentary behavior (e.g. television viewing, playing video games, social media technology) might be considered when the relationship between physical activity, sedentary behavior and mental health is studied in young people.
-
More studies focused on the relationship between physical activity and mental health (i.e. anxiety, self-esteem, self-concept, self-efficacy, positive affect and optimism), for which we currently have minimal or unclear evidence, are required. Likewise, research focused on the relationship between sedentary behavior and mental health (i.e. stress, anxiety, negative affect, self-esteem, self-concept, self-efficacy, positive affect and optimism), for which there is also minimal evidence, are also needed. Even observational studies may be worthwhile, given the lack of research to date.
4.7 Limitations and Strengths
Our review has several limitations. First, the so-called grey literature (i.e. System for Information on Grey Literature in Europe [SIGLE] database, dissertations, conference proceedings, and trial registries) was not included in the review. Second, the search was conducted in only two databases (PubMed and Web of Science), although this is consistent with the AMSTAR critical appraisal tool for systematic reviews, i.e. at least two electronic sources should be searched to perform a comprehensive literature search. However, we could have missed eligible studies from other databases. Third, studies written in languages other than English and Spanish were excluded from our review. In addition, because of the heterogeneity of the outcome measures, it was not possible to conduct a meta-analysis of the prospective longitudinal studies. Lastly, because most of the intervention studies were focused on adolescents (12 in adolescents vs. 3 in children), and no studies were found in preschoolers, we cannot rule out a cause and effect relationship between physical activity and mental health in preschoolers and children.
The present review also has several strengths. First, this review employed stringent systematic review methodology as per the PRISMA guidelines to ensure relevant literature was identified and evaluated with the greatest possible scientific rigor. Second, this review provided an a priori design registered in the Prospero database. Therefore, research questions and inclusion criteria were established before conducting this review. Third, two electronic sources were searched, and the search strategies are reported in this article. Moreover, we provided a list of the studies included and excluded (together with the specific reason for exclusion per study) in electronic supplementary Table S2. In addition, the quality of the included studies was examined, and hence conclusions drawn by this review are strengthened by the use of the quality assessment tool. Finally, a meta-analysis was performed including intervention studies (RCTs and non-RCTs), making it possible to map the link between exercise and global mental health across childhood and adolescence for the first time.
5 Conclusions
Findings from the present research suggest that physical activity has a small but significant positive effect on adolescents’ mental health. Due to the small number of studies, it was not possible to determine the effect of physical activity on preschoolers’ and children’s mental health. In addition, physical activity (i.e. active commuting, outdoor play or sport participation) may influence mental health in children and adolescents. In regard to the type of physical activity, participation in team sports was found to be a consistent positive correlate of mental health in children and adolescents. Conversely, sedentary behavior was negatively associated with mental health in children and adolescents. In particular, higher levels of recreational screen time (i.e. beyond 2 h/day of recreational screen time) were associated with poorer mental health outcomes in children and adolescents. In summary, there is sufficient evidence to conclude that interventions targeting increases in physical activity, and decreases in sedentary behavior, are justified and will support the current and future mental health of children and adolescents.
References
Murray CJL, Lopez AD, World Health Organization, World Bank, Harvard School of Public Health. The global burden of disease: a comprehensive assessment of mortality and disability from diseases, injuries, and risk factors in 1990 and projected to 2020: summary. Geneva: World Health Organization; 1996. http://www.who.int/iris/handle/10665/41864.
Antaramian SP, Huebner ES, Hills KJ, Valois RF. A dual-factor model of mental health: toward a more comprehensive understanding of youth functioning. Am J Orthopsychiatry. 2010;80:462–72.
Seligman MEP, Csikszentmihalyi M. Positive psychology: an introduction. Am Psychol. 2000;55:5–14.
Schmithorst VJ, Yuan W. White matter development during adolescence as shown by diffusion MRI. Brain Cogn. 2010;72:16–25.
Lenroot RK, Giedd JN. Brain development in children and adolescents: insights from anatomical magnetic resonance imaging. Neurosci Biobehav Rev. 2006;30:718–29.
Nelson SC, Kling J, Wängqvist M, Frisén A, Syed M. Identity and the body: trajectories of body esteem from adolescence to emerging adulthood. Dev Psychol. 2018;54:1159–71.
Beauchamp MR, Puterman E, Lubans DR. Physical inactivity and mental health in late adolescence. JAMA Psychiatry. 2018;75:543.
Hofstra MB, van der Ende J, Verhulst FC. Child and adolescent problems predict DSM-IV disorders in adulthood: a 14-year follow-up of a dutch epidemiological sample. J Am Acad Child Adolesc Psychiatry. 2002;41:182–9.
Caspersen CJ, Powell KE, Christenson GM. Physical activity, exercise, and physical fitness: definitions and distinctions for health-related research. Public Health Rep. 1985;100:126–31.
Spruit A, Assink M, van Vugt E, van der Put C, Stams GJ. The effects of physical activity interventions on psychosocial outcomes in adolescents: a meta-analytic review. Clin Psychol Rev. 2016;45:56–71.
Tremblay MS, Aubert S, Barnes JD, Saunders TJ, Carson V, Latimer-Cheung AE, et al. Sedentary behavior research network (SBRN)—terminology consensus project process and outcome. Int J Behav Nutr Phys Act. 2017;14:75.
Dishman RK, O’Connor PJ. Lessons in exercise neurobiology: the case of endorphins. Ment Health Phys Act. 2009;2:4–9.
Cotman CW, Berchtold NC, Christie L-A. Exercise builds brain health: key roles of growth factor cascades and inflammation. Trends Neurosci. 2007;30:464–72.
Kleim JA, Cooper NR, VandenBerg PM. Exercise induces angiogenesis but does not alter movement representations within rat motor cortex. Brain Res. 2002;934:1–6.
Lubans D, Richards J, Hillman C, Faulkner G, Beauchamp M, Nilsson M, et al. Physical activity for cognitive and mental health in youth: a systematic review of mechanisms. Pediatrics. 2016;14:114.
Physical Activity Guidelines for Americans. 2nd edition. 2018; Washington, DC: US Department of Health and Human Services. https://health.gov/paguidelines/second-edition/pdf/Physical_Activity_Guidelines_2nd_edition.pdf. Accessed 15 Nov 2018
Biddle SJH, Asare M. Physical activity and mental health in children and adolescents: a review of reviews. Br J Sports Med. 2011;45:886–95.
Biddle SJH, Ciaccioni S, Thomas G, Vergeer I. Physical activity and mental health in children and adolescents: an updated review of reviews and an analysis of causality. Psychol Sport Exerc. 2019;42:146–55.
Brown HE, Pearson N, Braithwaite RE, Brown WJ, Biddle SJH. Physical activity interventions and depression in children and adolescents. Sports Med. 2013;43:195–206.
Babic MJ, Morgan PJ, Plotnikoff RC, Lonsdale C, White RL, Lubans DR. Physical activity and physical self-concept in youth: systematic review and meta-analysis. Sports Med. 2014;44:1589–601.
Liu M, Wu L, Ming Q. How does physical activity intervention improve self-esteem and self-concept in children and adolescents? Evidence from a meta-analysis. PLoS One. 2015;10:1–17.
Ruotsalainen H, Kyngäs H, Tammelin T, Kääriäinen M. Systematic review of physical activity and exercise interventions on body mass indices, subsequent physical activity and psychological symptoms in overweight and obese adolescents. J Adv Nurs. 2015;71:2461–77.
Poitras VJ, Gray CE, Borghese MM, Carson V, Chaput J-P, Janssen I, et al. Systematic review of the relationships between objectively measured physical activity and health indicators in school-aged children and youth. Appl Physiol Nutr Metab. 2016;41:197–239.
Cairns KE, Yap MBH, Pilkington PD, Jorm AF. Risk and protective factors for depression that adolescents can modify: a systematic review and meta-analysis of longitudinal studies. J Affect Disord. 2014;169:61–75.
Bursnall P. The relationship between physical activity and depressive symptoms in adolescents: a systematic review. Worldviews Evid Based Nurs. 2014;11:376–82.
Ferreira-Vorkapic C, Feitoza JM, Marchioro M, Simões J, Kozasa E, Telles S. Are there benefits from teaching yoga at schools? a systematic review of randomized control trials of yoga-based interventions. Evid Based Complement Altern Med. 2015;2015:1–17.
Tremblay MS, LeBlanc AG, Kho ME, Saunders TJ, Larouche R, Colley RC, et al. Systematic review of sedentary behaviour and health indicators in school-aged children and youth. Int J Behav Nutr Phys Act. 2011;8:98.
Hoare E, Milton K, Foster C, Allender S. The associations between sedentary behaviour and mental health among adolescents: a systematic review. Int J Behav Nutr Phys Act. 2016;13:108.
Cliff DP, Hesketh KD, Vella SA, Hinkley T, Tsiros MD, Ridgers ND, et al. Objectively measured sedentary behaviour and health and development in children and adolescents: systematic review and meta-analysis. Obes Rev. 2016;17:330–44.
Suchert V, Hanewinkel R, Isensee B. Sedentary behavior and indicators of mental health in school-aged children and adolescents: a systematic review. Prev Med. 2015;76:48–57.
von Klitzing K, Döhnert M, Kroll M, Grube M. Mental disorders in early childhood. Dtsch Arztebl Int. 2015;112:375–86.
Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6:e1000097.
Kho ME, Eva KW, Cook DJ, Brouwers MC. The Completeness of Reporting (CORE) index identifies important deficiencies in observational study conference abstracts. J Clin Epidemiol. 2008;61:1241–9.
Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327:557–60.
Sallis JF, Prochaska JJ, Taylor WC. A review of correlates of physical activity of children and adolescents. Med Sci Sports Exerc. 2000;32:963–75.
Lubans DR, Morgan PJ, Cliff DP, Barnett LM, Okely AD. Fundamental movement skills in children and adolescents. Sports Med. 2010;40:1019–35.
Smith JJ, Eather N, Morgan PJ, Lubans DR. The health benefits of muscular fitness for children and adolescents: a systematic review and meta-analysis. Sports Med. 2014;44(9):1209–23.
Higgins JPT, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928. https://doi.org/10.1136/bmj.d5928
Von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. PLoS Med. 2008;61:344–9.
Armijo-Olivo S, Stiles CR, Hagen NA, Biondo PD, Cummings GG. Assessment of study quality for systematic reviews: a comparison of the Cochrane Collaboration Risk of Bias Tool and the Effective Public Health Practice Project Quality Assessment Tool: methodological research. J Eval Clin Pract. 2012;18(1):12–8.
Smith S, Madden AM. Body composition and functional assessment of nutritional status in adults: a narrative review of imaging, impedance, strength and functional techniques. J Hum Nutr Diet. 2016;29:1–19.
Hasanpour M, Tabatabaei M, Alavi M, Zolaktaf V. Effect of aerobics exercise on self-esteem in Iranian female adolescents covered by welfare organization. Sci World J. 2014;29(6):714–32.
Goldfield GS, Alberga AS, Hadjiyannakis S, Phillips P, Malcolm J, Wells GA, et al. Effects of aerobic training, resistance training, or both on psychological health in adolescents with obesity: the HEARTY randomized controlled trial. J Consult Clin Psychol. 2015;83:1123–35.
Costigan SA, Eather N, Plotnikoff RC, Hillman CH, Lubans DR. High-intensity interval training for cognitive and mental health in adolescents. Med Sci Sports Exerc. 2016;48:1985–93.
Lee LYK, Chong YL, Li NY, Li MC, Lin LN, Wong LY, et al. Feasibility and effectiveness of a chen-style Tai Chi programme for stress reduction in junior secondary school students. Stress Health. 2013;29:117–24.
Staiano AE, Abraham AA, Calvert SL. Adolescent exergame play for weight loss and psychosocial improvement: a controlled physical activity intervention. Obesity. 2013;21:598–601.
Tubić T, Đorđić V. Exercise effects on mental health of preschool children. An Psicol. 2013;29:249–56.
Seabra AC, Seabra AF, Brito J, Krustrup P, Hansen PR, Mota J, et al. Effects of a 5-month football program on perceived psychological status and body composition of overweight boys. Scand J Med Sci Sport. 2014;24:10–6.
Peng S, Qi A, Yuan F. Experimental study on the effects of exercise prescription on the mental health of left-behind school children in rural areas. Rev Argent Clin Psic. 2015;24(3):267–76.
Das M, Deepeshwar S, Subramanya P, Manjunath NK. Influence of Yoga-based personality development program on psychomotor performance and self-efficacy in school children. Front Pediatr. 2016;4:62.
Eather N, Morgan PJ, Lubans DR. Effects of exercise on mental health outcomes in adolescents: findings from the CrossFitTM teens randomized controlled trial. Psychol Sport Exerc. 2016;26:14–23.
Cox AE, Ullrich-French S, Howe HS, Cole AN. A pilot yoga physical education curriculum to promote positive body image. Body Image. 2017;23:1–8.
Yook YS, Kang SJ, Park IK. Effects of physical activity intervention combining a new sport and mindfulness yoga on psychological characteristics in adolescents. Int J Sport Exerc Psychol. 2017;15:109–17.
Bunketorp Käll L, Malmgren H, Olsson E, Lindén T, Nilsson M. Effects of a curricular physical activity intervention on children’s school performance, wellness, and brain development. J Sch Health. 2015;85(10):704–13.
Romero-Perez M, De Paz-Fernandez A, Camberos-Castaneda A, Tanori-Tapia M, Bernal-Reyes F, Marquez-Rosa S. Assessment of depression and anxiety states of obese children after participating in an exercise program. Biotecnia. 2015;17:11–5.
Kyle TL, Mendo AH, Reigal Garrido RE, Sánchez VM. Effects of physical activity on self-concept and self-efficacy in preadolescents. RETOS. Nuevas Tendencias en Educacion Fisica Deporte y Recreacion. 2016;2041:61–5.
Telles S, Singh N, Bhardwaj A, Kumar A, Balkrishna A. Effect of yoga or physical exercise on physical, cognitive and emotional measures in children: a randomized controlled trial. Child Adolesc Psychiatry Ment Health. 2013;7:37.
Bao X, Jin K. The beneficial effect of Tai Chi on self-concept in adolescents. Int J Psychol. 2015;50:101–5.
Rinaldo N, Zaccagni L, Gualdi-Russo E. Soccer training programme improved the body composition of pre-adolescent boys and increased their satisfaction with their body image. Acta Paediatr. 2016;105:492–5.
Toseeb U, Brage S, Corder K, Dunn VJ, Jones PB, Owens M, et al. Exercise and depressive symptoms in adolescents. JAMA Pediatr. 2014;168:1093.
Van Dijk ML, Savelberg HHCM, Verboon P, Kirschner PA, De Groot RHM. Decline in physical activity during adolescence is not associated with changes in mental health. BMC Public Health. 2016;16:300.
Bilinski H, Henry C, Humbert L, Spriggs P. The connection between psychosocial health, health behaviors and the environment in rural children. Child Indic Res. 2013;6:659–72.
Martikainen S, Pesonen A-K, Lahti J, Heinonen K, Feldt K, Pyhälä R, et al. Higher levels of physical activity are associated with lower hypothalamic–pituitary–adrenocortical axis reactivity to psychosocial stress in children. J Clin Endocrinol Metab. 2013;98:E619–27.
Ahn JV, Sera F, Cummins S, Flouri E. Associations between objectively measured physical activity and later mental health outcomes in children: findings from the UK Millennium Cohort Study. J Epidemiol Community Health. 2018;72:94–100.
Nihill GFJ, Lubans DR, Plotnikoff RC. Associations between sedentary behavior and self-esteem in adolescent girls from schools in low-income communities. Ment Health Phys Act. 2013;6:30–5.
Ishii K, Shibata A, Adachi M, Mano Y, Oka K. Objectively measured sedentary behavior, obesity, and psychological well-being: a cross-sectional study of Japanese schoolchildren. J Phys Act Health. 2017;14:270–4.
McVeigh J, Smith A, Howie E, Straker L. Trajectories of television watching from childhood to early adulthood and their association with body composition and mental health outcomes in young adults. PLoS One. 2016;11:1–12.
Janssen I. Estimating whether replacing time in active outdoor play and sedentary video games with active video games influences youth’s mental health. J Adolesc Health. 2016;59:517–22.
Larun L, Nordheim LV, Ekeland E, Hagen KB. Heian F. Exercise in prevention and treatment of anxiety and depression among children and young people. Cochrane Database Syst Rev. 2006. https://doi.org/10.1002/14651858.CD004691.pub2.
Carter T, Morres ID, Meade O, Callaghan P. The effect of exercise on depressive symptoms in adolescents: a systematic review and meta-Analysis. J Am Acad Child Adolesc Psychiatry. 2016;55(7):580–90.
Kipp LE, Weiss MR. Physical activity and self-perceptions among children and adolescents. Routledge handbook of physical activity and mental health. New York: Routledge; 2013. p. 187–99.
Lubans DR, Lonsdale C, Cohen K, Eather N, Beauchamp MR, Morgan PJ, et al. Framework for the design and delivery of organized physical activity sessions for children and adolescents: Rationale and description of the “SAAFE” teaching principles. Int J Behav Nutr Phys Act. 2017;14:24.
Eisenmann JC. Physical activity and cardiovascular disease risk factors in children and adolescents: an overview. Can J Cardiol. 2004;20:295–301.
Schneider S, Weiß M, Thiel A, Werner A, Mayer J, Hoffmann H, et al. Body dissatisfaction in female adolescents: extent and correlates. Eur J Pediatr. 2013;172:373–84.
McPhie ML, Rawana JS. The effect of physical activity on depression in adolescence and emerging adulthood: a growth-curve analysis. J Adolesc. 2015;40:83–92.
Carter JS, Dellucci T, Turek C, Mir S. Predicting depressive symptoms and weight from adolescence to adulthood: stressors and the role of protective factors. J Youth Adolesc. 2015;44:2122–40.
Sabiston CM, Jewett R, Ashdown-Franks G, Belanger M, Brunet J, O’Loughlin E, et al. Number of years of team and individual sport participation during adolescence and depressive symptoms in early adulthood. J Sport Exerc Psychol. 2016;38:105–10.
Brunet J, Sabiston CM, Chaiton M, Barnett TA, O’Loughlin E, Low NCP, et al. The association between past and current physical activity and depressive symptoms in young adults: a 10-year prospective study. Ann Epidemiol. 2013;23:25–30.
Patrick Auerbach R, Bigda-Peyton JS, Eberhart NK, Webb CA, Ringo Ho M-H. Conceptualizing the prospective relationship between social support, stress, and depressive symptoms among adolescents. J Abnorm Child Psychol. 2010;39:475–87.
Vella SA, Swann C, Allen MS, Schweickle MJ, Magee CA. Bidirectional associations between sport involvement and mental health in adolescence. Med Sci Sport Exerc. 2017;49:687–94.
Adachi PJC, Willoughby T. It’s not how much you play, but how much you enjoy the game: the longitudinal associations between adolescents’ self-esteem and the frequency versus enjoyment of involvement in sports. J Youth Adolesc. 2014;43:137–45.
Wagnsson S, Lindwall M, Gustafsson H. Participation in organized sport and self-esteem across adolescence: the mediating role of perceived sport competence. J Sport Exerc Psychol. 2014;36:584–94.
Reigal R, Videra A, Gil J. Physical exercise, general self-efficacy and life satisfaction in adolescence. Rev Int Med Cienc Ac. 2014;14:561–76.
Ho FKW, Louie LHT, Chow CB, Wong WHS, Ip P. Physical activity improves mental health through resilience in Hong Kong Chinese adolescents. BMC Pediatr. 2015;15:48.
Hillman CH, Pontifex MB, Castelli DM, Khan NA, Raine LB, Scudder MR, et al. Effects of the FITKids randomized controlled trial on executive control and brain function. Pediatrics. 2014;134:e1063–71.
Leibrock J, Lottspeich F, Hohn A, Hofer M, Hengerer B, Masiakowski P, et al. Molecular cloning and expression of brain-derived neurotrophic factor. Nature. 1989;341:149–52.
Martinowich K, Manji H, Lu B. New insights into BDNF function in depression and anxiety. Nat Neurosci. 2007;10:1089–93.
Young SN. How to increase serotonin in the human brain without drugs. J Psychiatry Neurosci. 2007;32:394–9.
Lubans DR, Smith JJ, Morgan PJ, Beauchamp MR, Miller A, Lonsdale C, et al. Mediators of psychological well-being in adolescent boys. J Adolesc Health. 2016;58:230–6.
Hinkley T, Verbestel V, Ahrens W, Lissner L, Molnár D, Moreno LA, et al. Early childhood electronic media use as a predictor of poorer well-being. JAMA Pediatr. 2014;168:485.
Allen MS, Vella SA. Screen-based sedentary behaviour and psychosocial well-being in childhood: cross-sectional and longitudinal associations. Ment Health Phys Act. 2015;9:41–7.
Liu M, Wu L, Yao S. Dose-response association of screen time-based sedentary behaviour in children and adolescents and depression: a meta-analysis of observational studies. Br J Sports Med. 2015;50:1252–8.
Gunnell KE, Flament MF, Buchholz A, Henderson KA, Obeid N, Schubert N, et al. Examining the bidirectional relationship between physical activity, screen time, and symptoms of anxiety and depression over time during adolescence. Prev Med. 2016;88:147–52.
Hamer M, Coombs N, Stamatakis E. Associations between objectively assessed and self-reported sedentary time with mental health in adults: an analysis of data from the Health Survey for England. BMJ Open. 2014;4:e004580.
Maras D, Flament MF, Murray M, Buchholz A, Henderson KA, Obeid N, et al. Screen time is associated with depression and anxiety in Canadian youth. Prev Med. 2015;73:133–8.
Wu X, Kirk SFL, Ohinmaa A, Veugelers P. Health behaviours, body weight and self-esteem among grade five students in Canada. Springerplus. 2016;5:1099.
Hoare E, Milton K, Foster C, Allender S. Depression, psychological distress and Internet use among community-based Australian adolescents: a cross-sectional study. BMC Public Health. 2017;17:365.
Benson LP, Williams RJ, Novick MB. Pediatric obesity and depression: a cross-sectional analysis of absolute BMI as it relates to children’s depression index scores in obese 7- to 17-year-old children. Clin Pediatr (Phila). 2013;52:24–9.
Kremer P, Elshaug C, Leslie E, Toumbourou JW, Patton GC, Williams J. Physical activity, leisure-time screen use and depression among children and young adolescents. J Sci Med Sport. 2014;17:183–7.
Grøntved A, Hu FB. Television viewing and risk of type 2 diabetes, cardiovascular disease, and all-cause mortality. JAMA. 2011;305:2448–55.
Bickham DS, Hswen Y, Rich M. Media use and depression: exposure, household rules, and symptoms among young adolescents in the USA. Int J Public Health. 2015;60:147–55.
Grøntved A, Singhammer J, Froberg K, Møller NC, Pan A, Pfeiffer KA, et al. A prospective study of screen time in adolescence and depression symptoms in young adulthood. Prev Med. 2015;81:108–13.
Goldfield GS, Murray M, Maras D, Wilson AL, Phillips P, Kenny GP, et al. Screen time is associated with depressive symptomatology among obese adolescents: a HEARTY study. Eur J Pediatr. 2016;175:909–19.
Babic MJ, Smith JJ, Morgan PJ, Eather N, Plotnikoff RC, Lubans DR. Longitudinal associations between changes in screen-time and mental health outcomes in adolescents. Ment Health Phys Act. 2017;12:124–31.
Hoare E, Skouteris H, Fuller-Tyszkiewicz M, Millar L, Allender S. Associations between obesogenic risk factors and depression among adolescents: a systematic review. Obes Rev. 2014;15:40–51.
Primack BA, Swanier B, Georgiopoulos AM, Land SR, Fine MJ. Association between media use in adolescence and depression in young adulthood. Arch Gen Psychiatry. 2009;66:181.
Ohannessian CM. Media Use and adolescent psychological adjustment: an examination of gender differences. J Child Fam Stud. 2009;18:582–93.
Kraut R, Patterson M, Lundmark V, Kiesler S, Mukopadhyay T, Scherlis W. Internet paradox. A social technology that reduces social involvement and psychological well-being? Am Psychol. 1998;53:1017–31.
Raudsepp L, Neissaar I, Kull M. A longitudinal assessment of the links between physical activity and physical self-worth in adolescent females. Eur J Sport Sci. 2013;13:716–22.
Stavrakakis N, Oldehinkel AJ, Nederhof E, Oude Voshaar RC, Verhulst FC, Ormel J, et al. Plasticity genes do not modify associations between physical activity and depressive symptoms. Health Psychol. 2013;32:785–92.
Hoare E, Millar L, Fuller-Tyszkiewicz M, Skouteris H, Nichols M, Malakellis M, et al. Depressive symptomatology, weight status and obesogenic risk among Australian adolescents: a prospective cohort study. BMJ Open. 2016;6:e010072.
Ishii K, Shibata A, Adachi M, Oka K. Association of physical activity and sedentary behavior with psychological well-being among Japanese children. Percept Mot Skills. 2016;123:445–59.
Reddon H, Meyre D, Cairney J. Physical activity and global self-worth in a longitudinal study of children. Med Sci Sports Exerc. 2017;49:1606–13.
Conn AM, Calais C, Szilagyi M, Baldwin C, Jee SH. Youth in out-of-home care: Relation of engagement in structured group activities with social and mental health measures. Child Youth Serv Rev. 2014;36:201–5.
Jewett R, Sabiston CM, Brunet J, O’Loughlin EK, Scarapicchia T, O’Loughlin J. School sport participation during adolescence and mental health in early adulthood. J Adolesc Health. 2014;55:640–4.
Vella SA, Cliff DP, Magee CA, Okely AD. Associations between sports participation and psychological difficulties during childhood: a two-year follow up. J Sci Med Sport. 2015;18:304–9.
Shin K, You S. Leisure type, leisure satisfaction and adolescents’ psychological wellbeing. J Pac Rim Psychol. 2013;7:53–62.
Hoegh Poulsen P, Biering K, Andersen JH. The association between leisure time physical activity in adolescence and poor mental health in early adulthood: a prospective cohort study. BMC Public Health. 2015;16:3.
Bulhões C, Ramos E, Lindert J, Dias S, Barros H. Depressive symptoms and its associated factors in 13-year-old urban adolescents. Int J Environ Res Public Health. 2013;10:5026–38.
Shriver LH, Harrist AW, Page M, Hubbs-Tait L, Moulton M, Topham G. Differences in body esteem by weight status, gender, and physical activity among young elementary school-aged children. Body Image. 2013;10:78–84.
Fararouei M, Brown IJ, Akbartabar Toori M, Estakhrian Haghighi R, Jafari J. Happiness and health behaviour in Iranian adolescent girls. J Adolesc. 2013;36:1187–92.
Haugen T, Ommundsen Y, Seiler S. The relationship between physical activity and physical self-esteem in adolescents: the role of physical fitness indices. Pediatr Exerc Sci. 2013;25:138–53.
Skrove M, Romundstad P, Indredavik MS. Resilience, lifestyle and symptoms of anxiety and depression in adolescence: the Young-HUNT study. Soc Psychiatry Psychiatr Epidemiol. 2013;48:407–16.
Altıntaş A, Aşçı FH, Kin-İşler A, Güven-Karahan B, Kelecek S, Özkan A, et al. The role of physical activity, body mass index and maturity status in body-related perceptions and self-esteem of adolescents. Ann Hum Biol. 2014;41:395–402.
Marques R, Assis M, Maranhao Neto GA, Resende F, Palma A. Body image dissatisfaction among 14-15 year old females in Rio de Janeiro. Brazil. Int J Sport Psychol. 2014;45:39–56.
Gomes R, Gonçalves S, Costa J. Exercise, eating disordered behaviors and psychological well-being: a study with Portuguese adolescents. Rev Latinoam Psicol. 2015;47:66–74.
Kovacs E, Piko BF, Keresztes N. The interacting role of physical activity and diet control in Hungarian adolescents’ substance use and psychological health. Subst Use Misuse. 2014;49:1278–86.
Wang H, Fu J, Lu Q, Tao F, Hao J. Physical activity, body mass index and mental health in Chinese adolescents: a population based study. J Phys Fit Sports Med. 2014;54:518–25.
Park S. Associations of physical activity with sleep satisfaction, perceived stress, and problematic internet use in Korean adolescents. BMC Public Health. 2014;14:1143.
Moljord IEO, Moksnes UK, Espnes GA, Hjemdal O, Eriksen L. Physical activity, resilience, and depressive symptoms in adolescence. Ment Health Phys Act. 2014;7:79–85.
Zach S, Netz Y. Self-presentation concerns and physical activity in three-generation families. Soc Behav Personal. 2014;42:259–67.
Sun Y, An J, Wang X, Zu P, Tao F-B. Gender- and puberty-dependent association between physical activity and depressive symptoms: national survey among Chinese adolescents. J Phys Act Health. 2014;11:1430–7.
Hoare E, Millar L, Fuller-Tyszkiewicz M, Skouteris H, Nichols M, Jacka F, et al. Associations between obesogenic risk and depressive symptomatology in Australian adolescents: a cross-sectional study. J Epidemiol Community Health. 2014;68:767–72.
Trinh L, Wong B, Faulkner GE. The independent and interactive associations of screen time and physical activity on mental health, school connectedness and academic achievement among a population-based sample of youth. J Can Acad Child Adolesc Psychiatry. 2015;24:17–24.
Esmaeilzadeh S. The association between depressive symptoms and physical status including physical activity, aerobic and muscular fitness tests in children. Environ Health Prev Med. 2015;20:434–40.
Reid M-A, MacCormack J, Cousins S, Freeman JG. Physical Activity, school climate, and the emotional health of adolescents: findings from 2010 Canadian Health Behaviour in School-Aged Children (HBSC) Study. Sch Ment Health. 2015;7:224–34.
Asare M, Danquah SA. The relationship between physical activity, sedentary behaviour and mental health in Ghanaian adolescents. Child Adolesc Psychiatry Ment Health. 2015;9:11.
Hyakutake A, Kamijo T, Misawa Y, Washizuka S, Inaba Y, Tsukahara T, et al. Cross-sectional observation of the relationship of depressive symptoms with lifestyles and parents’ status among Japanese junior high school students. Environ Health Prev Med. 2016;21:265–73.
Alghadir AH, Gabr SA, Al-Eisa E. Effects of physical activity on trace elements and depression related biomarkers in children and adolescents. Biol Trace Elem Res. 2016;172:299–306.
Mak K-K, Cerin E, McManus AM, Lai C-M, Day JR, Ho S-Y. Mediating effects of body composition between physical activity and body esteem in Hong Kong adolescents: a structural equation modeling approach. Eur J Pediatr. 2016;175:31–7.
Mouissi F. Physical activity and sport and their impact on mental health of Algerian adolescents. J Phys Educ Sport Health Recr. 2015;4:1807–13.
Hayward J, Jacka FN, Skouteris H, Millar L, Strugnell C, Swinburn BA, et al. Lifestyle factors and adolescent depressive symptomatology: associations and effect sizes of diet, physical activity and sedentary behaviour. Aust N Z J Psychiatry. 2016;50:1064–73.
Baldursdottir B, Valdimarsdottir HB, Krettek A, Gylfason HF, Sigfusdottir ID. Age-related differences in physical activity and depressive symptoms among 10–19-year-old adolescents: a population based study. Psychol Sport Exerc. 2017;28:91–9.
Szamreta EA, Qin B, Ohman-Strickland PA, Devine KA, Stapleton JL, Ferrante JM, et al. Associations of anthropometric, behavioral, and social factors on level of body esteem in peripubertal girls. J Dev Behav Pediatr. 2017;38:58–64.
Chae SM, Kang HS, Ra JS. Body esteem is a mediator of the association between physical activity and depression in Korean adolescents. Appl Nurs Res. 2017;33:42–8.
McDowell CP, MacDonncha C, Herring MP. Brief report: associations of physical activity with anxiety and depression symptoms and status among adolescents. J Adolesc. 2017;55:1–4.
Khan A, Burton NW. Is physical inactivity associated with depressive symptoms among adolescents with high screen time? Evidence from a developing country. Ment Health Phys Act. 2017;12:94–9.
Matin N, Kelishadi R, Heshmat R, Motamed-Gorji N, Djalalinia S, Motlagh ME, et al. Joint association of screen time and physical activity on self-rated health and life satisfaction in children and adolescents: the CASPIAN-IV study. Int Health. 2017;9:58–68.
Min JH, Lee E-Y, Spence JC, Jeon JY. Physical activity, weight status and psychological well-being among a large national sample of South Korean adolescents. Ment Health Phys Act. 2017;12:44–9.
Tajik E, Abd Latiff L, Adznam SN, Awang H, Yit Siew C, Abu Bakar AS. A study on level of physical activity, depression, anxiety and stress symptoms among adolescents. J Sports Med Phys Fitness. 2017;57:1382–7.
McMahon EM, Corcoran P, O’Regan G, Keeley H, Cannon M, Carli V, et al. Physical activity in European adolescents and associations with anxiety, depression and well-being. Eur Child Adolesc Psychiatry. 2017;26:111–22.
Noack P, Kauper T, Benbow AEF, Eckstein K. Physical self-perceptions and self-esteem in adolescents participating in organized sports and religious groups [Internet]. Eur J Dev Psychol. 2013;10(6):663–75.
Karr TM, Davidson D, Bryant FB, Balague G, Bohnert AM. Sport type and interpersonal and intrapersonal predictors of body dissatisfaction in high school female sport participants. Body Image. 2013;10:210–9.
Gísladóttir TL, Matthíasdóttir Á, Kristjánsdóttir H. The effect of adolescents’ sports clubs participation on self-reported mental and physical conditions and future expectations. J Sports Sci. 2013;31:1139–45.
Booker CL, Skew AJ, Sacker A, Kelly YJ. Well-being in adolescence—an association with health-related behaviors. J Early Adolesc. 2014;34:518–38.
Fatiregun AA, Kumapayi TE. Prevalence and correlates of depressive symptoms among in-school adolescents in a rural district in southwest Nigeria. J Adolesc. 2014;37:197–203.
Dalton B, Wilson R, Evans JR, Cochrane S. Australian indigenous youth’s participation in sport and associated health outcomes: empirical analysis and implications. Sport Manag Rev. 2015;18:57–68.
Booker CL, Skew AJ, Kelly YJ, Sacker A. Media use, sports participation, and well-being in adolescence: cross-sectional findings from the UK household longitudinal study. Am J Public Health. 2015;105:173–9.
Sipos E, Jeges S, Tóth Á. Sport, sense of coherence, and self-esteem among 16 and 17-year-olds. Eur J Ment Health. 2015;10:62–78.
Asfour L, Koussa M, Perrino T, Stoutenberg M, Prado G. The association of organized and unorganized physical activity and sedentary behavior with internalizing and externalizing symptoms in Hispanic adolescents. Child Adolesc Ment Health. 2016;21:109–14.
Reverdito RS, Carvalho HM, Galatti LR, Scaglia AJ, Gonçalves CE, Paes RR. Effects of youth participation in extra-curricular sport programs on perceived self-efficacy: a multilevel analysis. Percept Mot Skills. 2017;124:569–83.
Sun Y, Liu Y, Tao F. Associations between active commuting to school, body fat, and mental well-being : population-based, cross-sectional study in China. J Adolesc Health. 2015;57:679–85.
Monteiro LA, Novaes JS, Santos ML, Fernandes HM. Body dissatisfaction and self-esteem in female students aged 9–15: the effects of age, family income, body mass index levels and dance practice. J Hum Kinet. 2014;43:25–32.
Herman KM, Hopman WM, Sabiston CM. Physical activity, screen time and self-rated health and mental health in Canadian adolescents. Prev Med. 2015;73:112–6.
Badura P, Geckova AM, Sigmundova D, van Dijk JP, Reijneveld SA. When children play, they feel better: organized activity participation and health in adolescents. BMC Public Health. 2015;15:1090.
Hamer M, Yates T, Sherar LB, Clemes SA, Shankar A. Association of after school sedentary behaviour in adolescence with mental wellbeing in adulthood. Prev Med. 2016;87:6–10.
Raudsepp L. Bidirectional association between sedentary behaviour and depressive symptoms in adolescent girls. Eur J Sport Sci. 2016;16:1153–8.
Suchert V, Hanewinkel R, Isensee B, Hansen J, Johannsen M, Krieger C, et al. Sedentary behavior, depressed affect, and indicators of mental well-being in adolescence: does the screen only matter for girls? J Adolesc. 2015;42:50–8.
Padilla-Moledo C, Castro-Piñero J, Ortega FB, Pulido-Martos M, Sjöström M, Ruiz JR. Television viewing, psychological positive health, health complaints and health risk behaviors in Spanish children and adolescents. J Sports Med Phys Fit. 2015;55:675–83.
Suchert V, Hanewinkel R, Isensee B. Screen time, weight status and the self-concept of physical attractiveness in adolescents. J Adolesc. 2016;48:11–7.
Mundy LK, Canterford L, Olds T, Allen NB, Patton GC. The association between electronic media and emotional and behavioral problems in late childhood. Acad Pediatr. 2017;17:620–4.
Ohannessian CMC. Video game play and anxiety during late adolescence: the moderating effects of gender and social context. J Affect Disord. 2018;226:216–9.
Webb OJ, Benjamin CC, Gammon C, McKee HC, Biddle SJH. Physical activity, sedentary behaviour and physical self-perceptions in adolescent girls: a mediation analysis. Ment Health Phys Act. 2013;6:24–9.
Acknowledgements
This work was part of María Rodriguez-Ayllon’s Ph.D. thesis (Biomedicine Doctoral Studies of the University of Granada, Spain).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
This review was supported by the Spanish Ministry of Economy and Competitiveness (DEP2013-47540 and DEP2016-79512-R), the European Regional Development Fund (ERDF), the European Commission (no. 667302) and the Alicia Koplowitz Foundation. In addition, this review was conducted with additional funding from the University of Granada, Plan Propio de Investigación 2016, Excellence actions: Units of Excellence; Unit of Excellence on Exercise and Health (UCEES), Junta de Andalucía, Consejería de Conocimiento, Investigación y Universidades, and the ERDF, (ref. SOMM17/6107/UGR). Cristina Cadenas-Sánchez and Fernando Estévez-López are supported by a Grant from the Spanish Ministry of Economy and Competitiveness (BES-2014-068829 and BES-2014-067612, respectively); Jose Mora-Gonzalez and Jairo H. Migueles are supported by the Spanish Ministry of Education, Culture and Sport (FPU14/06837 and FPU15/02645, respectively); and Irene Esteban-Cornejo is supported by a Grant from the Alicia Koplowitz Foundation. In addition, this work was further supported by the SAMID III network, RETICS, funded by the PN I+D+I 2017-2021 (Spain), ISCIII-Sub-Directorate General for Research Assessment and Promotion and the ERDF (ref. RD16/0022).
Conflict of interest
María Rodriguez-Ayllon, Cristina Cadenas-Sánchez, Fernando Estévez-López, Nicolas Ernesto Muñoz, Jose Mora-Gonzalez, Jairo H. Migueles, Pablo Molina-García, Hanna Henriksson, Alejandra Mena-Molina, Vicente Martínez-Vizcaíno, Andrés Catena, Marie Löf, Kirk I. Erickson, David Lubans, Francisco B. Ortega and Irene Esteban-Cornejo declare that they have no conflicts of interest relevant to the content of this review.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Rodriguez-Ayllon, M., Cadenas-Sánchez, C., Estévez-López, F. et al. Role of Physical Activity and Sedentary Behavior in the Mental Health of Preschoolers, Children and Adolescents: A Systematic Review and Meta-Analysis. Sports Med 49, 1383–1410 (2019). https://doi.org/10.1007/s40279-019-01099-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40279-019-01099-5