
Abstract
Donor livers marginally acceptable or acceptable according to extended criteria are more frequently transplanted due to the growing discrepancy between demand and availability of donor organs. One type of marginally acceptable graft is a steatotic donor liver, because it is more sensitive to ischemia-reperfusion injury. Thus, quantitative assessment of steatosis is crucial prior to liver transplantation. Extent of steatosis of 49 pre-reperfusion liver biopsies from patients who received orthotopic liver transplantation was assessed by three techniques: semi-quantitative histological evaluation, computerized histomorphometry, and NMR-based estimation of fat content. The findings were correlated to clinical data and to histological examination of corresponding post-reperfusion biopsies for quantification of ischemia-reperfusion injury. We found that values obtained through all three assessment methods were positively correlated. None of the values obtained by the three applied methods correlated with clinical outcome or extent of ischemia-reperfusion injury. Quantitative evaluation of steatosis by NMR yields results comparable to histological and morphometrical assessment. This technique is rapid (<5 min), accurately quantifies fat in donor livers, and provides results that can be used when evaluation by a pathologist is not available.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Due to increasing demand and shortage in organ supply, increasingly expanded criteria are applied to accept donor livers for transplantation [12, 17, 21]. As fatty liver disease is a worldwide health problem, evaluation of graft steatosis prior to transplantation has emerged as crucial in the process of liver transplantation [6, 20]. Grafts with steatosis are more sensitive to ischemia-reperfusion injury and are associated with adverse outcome [3, 5]. Steatosis can be estimated macroscopically by the explantation surgeon using liver texture criteria [23], which can be helpful especially if pathology services are not available. If they are, steatosis assessment in pre-transplant biopsies is currently performed by pathologists using hematoxylin and eosin (H&E)-stained frozen sections. The extent of interobserver variability and reproducibility of steatosis assessment has been the subject of intense discussion [4]. An easy and reliable method of steatosis assessment on frozen sections is the application of a special fat stain like Oil Red O (ORO) [16]. The additional value of software-based morphometrical approaches to steatosis quantification has been discussed in several studies. While some authors favor morphometrical analysis over semi-quantitative assessment by a pathologist [4, 15], other authors find the morphometrical approach not superior to assessment by a pathologist [16]. Most authors regard morphometric analysis as a possible auxiliary method in addition to pathologist assessment of steatosis and consider computerized analysis as a suitable, reliable method for reevaluation of lipid contents for scientific purposes [1]. An evolving field of steatosis assessment is the non-invasive radiological evaluation of liver steatosis using magnetic resonance imaging (MRI) [9, 19] and computerized tomography (CT) [18]. However, these methods are mostly not available prior to organ retrieval of brain dead donors.
In this study, we assessed liver fat content by NMR analysis and compared this to semi-quantitative histopathological evaluation and computerized analysis. This technique is already applied in the food industry to determine fat/lipid content in ice creams [11], cheese [2], or meat products [7]. In humans, this method has been used to quantify fecal fat of patients with malabsorption or chronic pancreatitis [8]. The objective of the present study is to determine whether this NMR-based technique is of value in the evaluation of lipid content in pre-transplantation liver biopsies.
Methods
Study design/patients
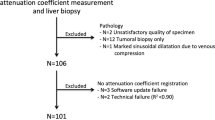
We obtained from the archives of the Institute of Pathology of the University Hospital of Essen 49 paired cases of pre-transplantation and post-reperfusion liver biopsies from patients who received an orthotopic liver transplant between May 2011 and May 2014. The study was approved by the local ethics committee (15-6284-BO).
Donor and recipient characteristics
Donor data included age, gender, BMI, cold ischemia time (CIT), and warm ischemia time (WIT). Recipient data included age, gender, indication for orthotopic liver transplantation, preoperative data including Model for End-Stage Liver Disease (MELD) score, length of intensive care unit (ICU) stay and ward stay, postoperative laboratory results within the first postoperative week including concentration of alanine transaminase (ALT), aspartate transaminase (AST), bilirubin (mg/dl), and international normalized ratio (INR). Data also included early allograft dysfunction (EAD) [13] and primary non-function (PNF) defined as retransplantation or death within 7 days of initial orthotopic liver transplantation (OLT).
Tissue samples
Fresh, unfixed pre-reperfusion biopsies were taken by explanting surgeons and obtained via the German Organ Transplantation Foundation (DSO), while post-reperfusion biopsies were taken intraoperatively, 1 h after reestablishing blood flow. Frozen sections of pre-reperfusion biopsies were cut at 3 μm and stained with H&E and ORO, according to institutional standards. Post-reperfusion biopsies were formalin fixed and paraffin embedded (FFPE). Slides were prepared and stained with H&E and naphthol-AS-d-chloroacetate esterase (ASDCL), according to institutional standards. For immunohistochemistry, antigen retrieval was carried out with Target Retrieval (Dako, Glostrup, Denmark) at pH 9.0 and 96 °C for 20 min. Sections were incubated with the primary antibody (M30, #10700; TECOmedical, Switzerland) at room temperature for 30 min. Antibody binding was detected with the ZytoChem Plus AP Polymer Kit (Zytomed Systems, Berlin, Germany). Positive controls were included in every run. Representative photomicrographs of H&E-frozen section, ASDCL staining, and M30 immunohistochemistry are given in Fig. 1.

a Representative frozen section of pre-reperfusion biopsy (H&E, ×100) showing a lower histopathological definition in comparison to permanent sections and technique-related crush artifacts. b Morphometrical analysis of pre-reperfusion biopsy (ORO, ×200). Macrosteatotic droplets are encircled with yellow, and microsteatotic droplets are encircled with green. c, d Post-reperfusion biopsies with ASDCL staining which highlights PMNs (c, ×200) and M30 immunohistochemistry to display hepatocyte apoptosis (d, ×400) as indicators of ischemia-reperfusion injury
Histopathological semi-quantitative assessment of steatosis
Steatosis of pre-reperfusion biopsies was determined on H&E- and ORO-stained sections prepared during intraoperative examination as the percentage of fatty hepatocytes relative to that of total hepatocytes by two independent observers (SB and CM) in terms of macrovesicular steatosis (MaSt) and microvesicular steatosis (MiSt). MaSt was defined as intracellular lipid droplets large enough to displace the nucleus from the center of the cytoplasm. MaSt lipid droplets were defined to be larger than the nucleus. MiSt was defined as at least one, usually numerous small lipid droplets smaller in size than the nucleus and not displacing the nucleus.
Computerized morphometrical evaluation of steatosis
Computerized morphometrical quantification of liver steatosis of pre-reperfusion ORO-stained biopsies was performed using a camera-equipped microscope (Zeiss Axioplan, Carl Zeiss Microscopy GmbH, Jena, Germany) and AxioVision software (V4.6.3.0, Carl Zeiss Microscopy GmbH, Jena, Germany). Five representative images per biopsy were recorded and evaluated at 400-fold magnification. The images were chosen not to contain large portal tracts. Non-tissue-covered areas and portal tracts were automatically subtracted from the total tissue area. The software detected intense red staining signals of ORO as fat droplets. The fat droplets were automatically overlaid green by the software. Subsequently, total steatosis (ToSt) was calculated and the percentage of fat-covered area to hepatocyte-covered area was calculated. The cutoff value for MiSt and MaSt was defined at 40 μm2. This cutoff value was chosen to ensure that the droplets classified as MaSt were larger than hepatocyte nuclei. Microsteatotic droplets were encircled green and macrosteatotic droplets yellow. Subsequently, values for MaSt and MiSt were calculated by the AxioVision software. For semi-quantitative and morphometrical evaluation, the same slides were used. A representative image of ORO staining with green- and yellow-encircled lipid droplets is given in Fig. 1.
Analysis of liver samples using NMR-based fat analysis
The device used for NMR-based fat analysis was the Smart Trac II system (CEM, Matthews, NC, USA) (http://cem.com/smart-trac-2/). The analyzer was operated according to the manufacturer’s recommendations. Prior to analysis, a calibration check was performed using liver samples in which the true lipid concentration was chemically determined using a standard protocol. Samples of liver tissue (ca. 5 g) were weighed on an analytical balance, mixed with 60 g sodium sulfate and 20 g glass powder, and homogenized in a blender. The powder was then transferred into a glass column (30 × 3.5 cm) containing a plug of silanized glass wool at the bottom. The fat was extracted by pouring 500 ml dichloromethane/cyclohexane at a ratio of 1:1 (v/v) through the column. After the solvent mixture passed the column, the extract was evaporated under a gentle stream of nitrogen and the fat content was weighed on an analytical balance.
For fat analysis with the Smart Trac II system, frozen samples of an initial weight of 0.01 to 0.14 g (mean 0.063 g) were defrosted and crushed to a paste-like mass and placed into the Smart Trac II system microwave chamber. After microwave drying, the samples were rolled in Trac film, placed in the Trac test tube, and inserted in the Smart Trac system II NMR chamber (permanent, thermally stabilized magnet, 0.55 T, 23.4 MHz proton) for measurement of fat content. Both the Trac film and Trac tube are proton-free components. The NMR sends a pulse of radio-frequency energy through the sample, which causes the hydrogen to generate a signal, known as free induction decay (FID). Fat protons decay more slowly than those in other tissue constituents (e.g., protein, carbohydrates). The intensity of the FID was analyzed to determine the amount of fat protons present in the sample.
Quantification of ischemia-reperfusion injury
The extent of the ischemia-reperfusion injury (I/R injury) was quantified by the number of infiltrating polymorphonuclear granulocytes (PMNs), apoptosis rate, and extent of necrosis. These parameters were evaluated in both pre- and post-reperfusion biopsies. For quantification of PMNs, slides were stained with ASDCL. PMNs were counted in three representative rectangular high-power fields (350 μm × 270 μm; 400-fold magnification). To quantify apoptotic cells, we used immunohistochemistry with the M30 antibody which detects a neo-epitope on caspase-cleaved cytokeratin 18 (CK18) in apoptotic cells, while uncleaved CK18 is not detected [10]. Apoptotic cells were counted in four rectangular medium-power fields (700 μm × 540 μm; 200-fold magnification). PMNs and apoptotic cells were counted by two observers (CM and SS). Subsequently, a mean value of the results was calculated. Results for PMNs and apoptotic cells were normalized to an area of 1 mm2. Necrosis was assessed semi-quantitatively using a scoring system (0% = 0; 1–2% = 1; 3–10% = 2; >10% = 3). The percentage values refer to the area of the slide covered with hepatocytes. This was assessed by two observers (SB and CM). A microscope with discussion unit was used to obtain consensus in difficult cases.
Statistical analysis
All statistical analyses were conducted in SPSS (V22; IBM, Armonk, NY, USA). Graphics were generated in SPSS and GraphPad Prism (GraphPad Software, La Jolla, CA, USA). Wilcoxon signed-rank test was used to assess the significance of differences between paired samples (pre- and post-reperfusion biopsies). When appropriate, values of the tested fat measurement techniques were dichotomized at median level. Subsequently, the Mann-Whitney U test was applied to evaluate statistical significance for continuous variables, Fisher’s exact test for binary variables. p values <0.05 were considered statistically significant and are to be understood as strictly descriptive. There was no adjustment for multiple testing. Spearman correlation was calculated since most variables did not show an acceptably normal distribution. For interobserver reliability, the intraclass correlation coefficient (ICC) was applied.
Results
Donors’ characteristics
Donor liver samples were obtained from 49 deceased patients with a median age of 61 years (range 18–88) and a median BMI of 27 kg/m2 (range 17–51 kg/m2). Of the donors, 23 were male and 26 female.
Relationship between methods used to measure liver fat content
Data obtained using the tested steatosis measurement techniques are provided in Table 1. Values obtained by a NMR technique moderately correlated with semi-quantitative assessment of MaSt (r = 0.473), morphometric assessment of MaSt (r = 0.466), and that of ToSt (r = 0.434) as shown in scatter plots, which include r and p values (Fig. 2 and Fig. S1 in the supplementary data). We calculated a median steatosis value for measurements by each method and also dichotomized the obtained values relative to the median (value above median versus value equal to or below median). Pairwise cross tabulation of the respective dichotomized values (three 2 × 2 tables for the three methods) is shown in the supplementary data (Table S1). Each of the three comparisons shows as many upward deviations (from below median in one method to above median in the other method) and downward deviations (from above median to in the first method to below median in the second method). As an example, values for 7 of 49 subjects deviated from below median in histomorphometry to above median in NMR-based method, while those for 7 other subjects deviated downward. This was found for all three methods tested. Semi-quantitative assessment of MaSt and MiSt by two observers was in good agreement (ICCs 0.881; 0.857), as also indicated by the scatter plots in Fig. 2.

Scatter plots of fat content measurements with NMR technique versus semi-quantitative assessment (a) and morphometric analysis (b) of macrovesicular steatosis showing moderate correlation (r = 0.473, r = 0.466; Spearman correlation). Scatter plots of semi-quantitative assessment of the two observers for macrosteatosis (c) and microsteatosis (d) reveal good and moderate correlations (r = 0.811, r = 0.736; Spearman correlation)
Comparison of histological parameters in paired pre- and post-transplant liver samples
There was a significant increase in the number of PMNs (data shown in Fig. 3), in the extent of necrosis [necrosis score prior to transplantation (median (Q1; Q3)) = 0 (0; 0), necrosis score after reperfusion = 0 (0; 1)] after reperfusion (p < 0.001, p < 0.001). As shown in Fig. 3, the number of apoptotic cells showed an increasing trend (p = 0.065).

Change of factors indicating I/R injury from pre- to post-reperfusion biopsies. a The number of polymorphonuclear granulocytes (PNMs). b The number of apoptotic cells (M30 immunohistochemistry). Values are normalized to an area of 1 mm2
Donor data and steatosis
The length of CIT was not significantly correlated with semi-quantitative or morphometric assessment of MiSt. A weak positive correlation was found between donor BMI and semi-quantitative assessment of MaSt (r = 0.374; p = 0.008), but not between donor BMI and morphometric assessment of MaSt or fat content assessed by the NMR technique (r = 0.04).
Donor data, I/R injury, and clinical outcome
A weak negative correlation was found in post-reperfusion biopsies between donor BMI and the number of PMNs (r = −0.295; p = 0.044). On post-reperfusion biopsies, a weak positive correlation was found between the length of CIT and the overall number of PMNs (r = 0.314; p = 0.034) and the number of apoptotic cells (r = 0.313; p = 0.039). Patients who received a graft from younger donors had a higher incidence for EAD [patients without EAD (median (Q1; Q3)) = 62 (57.0; 74.5) years, patients with EAD = 45 (38.0; 56.5) years; p = 0.003]. There was no significant relationship between donor BMI and clinical outcome [patients without EAD (median (Q1; Q3)) = 27.0 (24.4; 30.5) kg/m2, patients with EAD = 27.7 (24.5; 29.3) kg/m2; p = 1.000].
Steatosis, I/R injury, and clinical outcome
When donor liver samples were dichotomized according to the median level of steatosis, we found no significant differences between the two groups in the overall number of PMNs, the number of apoptotic cells, the extent of necrosis, the length of ward stay or ICU stay, and the incidence of EAD or PNF. p values (Mann-Whitney U test) are shown in supplementary Table S2. Cross tabulation with the binary parameter EAD after dichotomization at a median level of steatosis (Fisher’s exact test) is shown in supplementary Table S3. Noticeable are the differences in the number of apoptotic cells per square millimeter [group above median (median (Q1; Q3)) = 0.50 (0.0; 1.65) versus group below median = 0.0 (0.0; 0.66); p = 0.070] between the two groups after dichotomization on the basis of the fat measurement NMR technique. No significant correlation was found between fat measurement techniques and histological parameters and patient outcome (Spearman correlation). Data are shown in supplementary Table S4.
Recipients’ characteristics and clinical outcome
Patient characteristics and clinical outcome are listed in Table S4. All patients survived the first 7 days after OLT. One patient died within the observation period of 30 days, and another patient died within the first 3 months after OLT. Three patients exhibited a MELD score of ≥30 at the date of OLT (Table 2).
Discussion
We measured fat in liver tissue sample using the CEM Smart Trac® device. This system combines microwave drying with NMR technology and permits rapid (<5 min) quantification of lipid content in liver tissue. Values are expressed in percentage of fat in dry matter (i.d.m.). The NMR technique is applied in the food industry for rapid and accurate analysis of lipid content in meat and dairy products [2, 7, 11]. In patient care, this NMR technique is used to determine fecal fat content in patients with malabsorption and chronic pancreatitis [8]. To date, the gold standard for fat quantification in donor liver tissue is histological assessment on H&E-stained frozen sections at best supplemented with specific fat stains such as ORO [16]. However, poor agreement between pathologists in the histological assessment of steatosis has been subject to criticism [4]. We show that liver lipid content can be measured in pre-reperfusion biopsies of human donor livers using the NMR technique. The obtained values correlated significantly with those obtained through morphological assessment. However, in the range of fat content values in this case series, lipid content in pre-reperfusion biopsies was not significantly associated with post-transplantation I/R injury or clinical outcome.
Non-invasive imaging techniques, such as ultrasound- [22], CT- [18], and MRT-based [14, 19] techniques, for quantification of steatosis are available. These are usually applied to brain-dead and heart-beating donors while the technique we used can be applied after explantation of the donor liver and provides the percentage of fat in dry matter.
The NMR technique of assessing tissue fat has some obvious advantages. First, the method is independent of subjective estimations and yields a reproducible result. Second, the need for a 24-h pathology service is not necessary because manipulations are very simple and can be easily conducted by inexperienced personnel. The hardware is compact, making the method suitable for use in or near the operating room. Third, it is rapid because after drying the liver sample by microwave, the NMR measurement is completed within seconds and the whole analysis is finished in less than 5 min. The Smart Trac® system delivers results which are comparable to those of chemical fat analysis methods like ether extraction methods [7]. Compared to these methods, the NMR technique has the advantage that there is no exposure to hazardous chemicals, no need for costly chemical disposal, and no need for special extraction equipment. Finally, the method is acute and precise, which might not be necessary for patient care but would be an advantage for research purposes.
On the other hand, there are unquestionable disadvantages of the NMR technique. First of all, it is not possible to differentiate between macro- and microsteatosis, which is important because only macrosteatosis is believed to be predictive of the estimated I/R injury [3]. Another disadvantage is the fact that the tissue to be analyzed has to be homogenized before measurement and will be lost for further investigation while tissue processed for histological examination remains available for additional analysis.
A limitation of this study is the small number of investigated cases. In addition, the donor livers were selected because only organs with less than 30% of macrosteatosis were used for liver transplantation. This is may be the reason for the low degree of I/R injury and few patients with early allograft dysfunction or primary non-function, and this merits further study. Because percentage values of the NMR method (% fat i.d.m.) are correlated with but not individually equal to those obtained by optical methods (percentage of fatty hepatocytes or of fat covered area), cutoff values have to be defined first. The results of our study allow for conception and planning of an inferential study.
We conclude that the NMR technique as part of CEM Smart Trac® technology provides a novel, rapid, and easy method to quantify liver tissue fat content. However, only histopathological examination can discriminate between macro- and microsteatosis or diagnose fibrosis, cholangitis, or malignancy.
Abbreviations
- ASDCL:
-
Naphthol-AS-d-chloroacetate esterase
- BMI:
-
Body mass index
- CIT:
-
Cold ischemia time
- CK18:
-
Cytokeratin 18
- EAD:
-
Early allograft dysfunction
- i.d.m.:
-
In dry matter
- I/R injury:
-
Ischemia-reperfusion injury
- ICU:
-
Intensive care unit
- MaSt:
-
Macrovesicular steatosis
- MELD:
-
Model for End-Stage Liver Disease
- MiSt:
-
Microvesicular steatosis
- NMR:
-
Nuclear magnetic resonance
- OLT:
-
Orthotopic liver transplantation
- ORO:
-
Oil Red O
- PMN:
-
Polymorphonuclear granulocyte
- PNF:
-
Primary non-function
- Q1:
-
First quartile
- Q3:
-
Third quartile
- SD:
-
Standard deviation
- ToSt:
-
Total steatosis
- WIT:
-
Warm ischemia time
References
Boyles TH, Johnson S, Garrahan N, Freedman AR, Williams GT (2007) A validated method for quantifying macrovesicular hepatic steatosis in chronic hepatitis C Analytical and quantitative cytology and histology/the International Academy of Cytology [and] American Society of Cytology 29:244–250
Chaland B, Mariette F, Marchal P, De Certaines J (2000) 1H nuclear magnetic resonance relaxometric characterization of fat and water states in soft and hard cheese. The Journal of Dairy Research 67:609–618
de Graaf EL, Kench J, Dilworth P, Shackel NA, Strasser SI, Joseph D, Pleass H, Crawford M, McCaughan GW, Verran DJ (2012) Grade of deceased donor liver macrovesicular steatosis impacts graft and recipient outcomes more than the donor risk index. J Gastroenterol Hepatol 27:540–546. doi:10.1111/j.1440-1746.2011.06844.x
El-Badry AM, Breitenstein S, Jochum W, Washington K, Paradis V, Rubbia-Brandt L, Puhan MA, Slankamenac K, Graf R, Clavien PA (2009) Assessment of hepatic steatosis by expert pathologists: the end of a gold standard. Ann Surg 250:691–697. doi:10.1097/SLA.0b013e3181bcd6dd
El-Badry AM, Moritz W, Contaldo C, Tian Y, Graf R, Clavien PA (2007) Prevention of reperfusion injury and microcirculatory failure in macrosteatotic mouse liver by omega-3 fatty acids. Hepatology 45:855–863. doi:10.1002/hep.21625
Flechtenmacher C, Schirmacher P, Schemmer P (2015) Donor liver histology—a valuable tool in graft selection Langenbeck’s archives of surgery/Deutsche Gesellschaft fur Chirurgie. doi: 10.1007/s00423-015-1298-7
Keeton JT, Hafley BS, Eddy SM, Moser CR, McManus BJ, Leffler TP (2003) Rapid determination of moisture and fat in meats by microwave and nuclear magnetic resonance analysis—PVM 1:2003. J AOAC Int 86:1193–1202
Korpi-Steiner NL, Ward JN, Kumar V, McConnell JP (2009) Comparative analysis of fecal fat quantitation via nuclear magnetic resonance spectroscopy (1H NMR) and gravimetry. Clinica Chimica Acta 400:33–36. doi:10.1016/j.cca.2008.10.001
Lee MJ, Bagci P, Kong J, Vos MB, Sharma P, Kalb B, Saltz JH, Martin DR, Adsay NV, Farris AB (2013) Liver steatosis assessment: correlations among pathology, radiology, clinical data and automated image analysis software. Pathol Res Pract 209:371–379. doi:10.1016/j.prp.2013.04.001
Leers MP, Kolgen W, Bjorklund V, Bergman T, Tribbick G, Persson B, Bjorklund P, Ramaekers FC, Bjorklund B, Nap M, Jornvall H, Schutte B (1999) Immunocytochemical detection and mapping of a cytokeratin 18 neo-epitope exposed during early apoptosis. J Pathol 187:567–572. doi:10.1002/(SICI)1096-9896(199904)187:5<567::AID-PATH288>3.0.CO;2-J
Mariette F, Lucas T (2005) NMR signal analysis to attribute the components to the solid/liquid phases present in mixes and ice creams. J Agric Food Chem 53:1317–1327. doi:10.1021/jf049294o
McCormack L, Dutkowski P, El-Badry AM, Clavien PA (2011) Liver transplantation using fatty livers: always feasible? J Hepatol 54:1055–1062. doi:10.1016/j.jhep.2010.11.004
Olthoff KM, Kulik L, Samstein B, Kaminski M, Abecassis M, Emond J, Shaked A, Christie JD (2010) Validation of a current definition of early allograft dysfunction in liver transplant recipients and analysis of risk factors. Liver Transplantation 16:943–949. doi:10.1002/lt.22091
Pineda N, Sharma P, Xu Q, Hu X, Vos M, Martin DR (2009) Measurement of hepatic lipid: high-speed T2-corrected multiecho acquisition at 1H MR spectroscopy—a rapid and accurate technique. Radiology 252:568–576. doi:10.1148/radiol.2523082084
Rawlins SR, El-Zammar O, Zinkievich JM, Newman N, Levine RA (2010) Digital quantification is more precise than traditional semiquantitation of hepatic steatosis: correlation with fibrosis in 220 treatment-naive patients with chronic hepatitis C. Dig Dis Sci 55:2049–2057. doi:10.1007/s10620-010-1254-x
Reis H, Peterek PT, Wohlschlaeger J, Kaiser GM, Mathe Z, Juntermanns B, Sotiropoulos GC, Beckhove U, Canbay A, Wirges U, Scherag A, Treckmann JW, Paul A, Baba HA (2014) Oil Red O-assessed macrosteatosis in liver transplant donor biopsies predicts ischemia-reperfusion injury and clinical outcome. Virchows Archiv 464:165–174. doi:10.1007/s00428-013-1512-3
Renz JF, Kin C, Kinkhabwala M, Jan D, Varadarajan R, Goldstein M, Brown R Jr, Emond JC (2005) Utilization of extended donor criteria liver allografts maximizes donor use and patient access to liver transplantation. Ann Surg 242:556–563 discussion 563-555
Rogier J, Roullet S, Cornelis F, Biais M, Quinart A, Revel P, Bioulac-Sage P, Le Bail B (2015) Noninvasive assessment of macrovesicular liver steatosis in cadaveric donors based on computed tomography liver-to-spleen attenuation ratio. Liver Transplantation. doi:10.1002/lt.24105
Sharma P, Martin DR, Pineda N, Xu Q, Vos M, Anania F, Hu X (2009) Quantitative analysis of T2-correction in single-voxel magnetic resonance spectroscopy of hepatic lipid fraction. Journal of Magnetic Resonance Imaging 29:629–635. doi:10.1002/jmri.21682
Spitzer AL, Lao OB, Dick AA, Bakthavatsalam R, Halldorson JB, Yeh MM, Upton MP, Reyes JD, Perkins JD (2010) The biopsied donor liver: incorporating macrosteatosis into high-risk donor assessment. Liver Transplantation 16:874–884. doi:10.1002/lt.22085
Wertheim JA, Petrowsky H, Saab S, Kupiec-Weglinski JW, Busuttil RW (2011) Major challenges limiting liver transplantation in the United States. American Journal of Transplantation 11:1773–1784. doi:10.1111/j.1600-6143.2011.03587.x
Yang HT, Chen KF, Lu Q, Wei YG, Li B, Qin Y, Huang WQ (2014) Ultrasonic integrated backscatter in assessing liver steatosis before and after liver transplantation. Hepatobiliary & Pancreatic Diseases International 13:402–408
Yersiz H, Lee C, Kaldas FM, Hong JC, Rana A, Schnickel GT, Wertheim JA, Zarrinpar A, Agopian VG, Gornbein J, Naini BV, Lassman CR, Busuttil RW, Petrowsky H (2013) Assessment of hepatic steatosis by transplant surgeon and expert pathologist: a prospective, double-blind evaluation of 201 donor livers. Liver Transplantation 19:437–449. doi:10.1002/lt.23615
Acknowledgments
We thank Dorothe Möllmann and Laura Malkus for their excellent technical assistance and Heidrun Kuhlmann and Achim Konietzko for their assistance with data collection. The counter analyses of the liver fat determination through solvent extraction by Ludger Wessel at the Chemical and Veterinary Analytical Institute Münsterland-Emscher-Lippe (CVUA-MEL, Director: Prof. Dr. Peter Fürst) is gratefully acknowledged. The authors also wish to thank Frank Scholten and Ulf Sengutta (CEM GmbH, Kamp-Lintfort, German subsidiary of CEM) for their assistance and the possibility to use the Smart Trac II analysis system.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The study was approved by the local ethics committee (15-6284-BO).
Conflict of interest
The authors declare that they have no conflict of interest.
Funding
No grants or financial support was received for this study.
Rights and permissions
About this article

{kind=link}
Cite this article
Bertram, S., Myland, C., Swoboda, S. et al. Liver steatosis in pre-transplant liver biopsies can be quantified rapidly and accurately by nuclear magnetic resonance analysis. Virchows Arch 470, 197–204 (2017). https://doi.org/10.1007/s00428-016-2047-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00428-016-2047-1