
Abstract
Introduction
The anatomy of the cochlea forms the basis for a successful cochlear implantation. Cochlear duct length (CDL) is defined as the length of the scala media as measured from the middle of the round window to helicotrema. Preoperative measurement of CDL is particularly important when precise intracochlear electrode array placement is desired. It can be done both histologically and radiologically. Preoperative high-resolution computed tomography (HRCT) scan which forms an integral part of cochlear implant workup is a useful tool to calculate CDL using 3D reconstructions.
Method
This study was done in SMS Medical College and Hospital, Jaipur, India, which is a tertiary care hospital and referral centre for cochlear implants. HRCT temporal bones of all children less than 6 years of age, with congenital bilateral severe-to-profound SNHL who were being worked up for cochlear implant were studied and analysed. 124 patients (56 females and 68 males) with hearing loss were evaluated for cochlear implantation. HRCT temporal bone of these patients was analysed and a variable A was measured which is defined as the linear measurement from the round window to the farthest point on the opposite wall of the cochlea on a reformatted CT scan slice.
Results
Mean of distance A for right ear of these patients was 8.10 mm (range 7.7–9.2 mm). Mean for the same in left ear of these patients was 8.14 mm (range 7.7–9.0 mm), giving an overall average of 8.12 mm. Using the formula, CDL = 4.16A−3.98, we calculated the length of cochlear duct. Mean cochlear duct length was 29.8 mm with a range from 28 to 34.3 mm.
Conclusion
To the best of our knowledge, this is the first large sample study of cochlear length in population of this part of the world. A smaller cochlear length in this part of the world as compared to the Caucasian cochlear duct is a significant finding in understanding of the cochlear anatomy and physiology. It would also have great implications on the insertion depth in cochlear implantation.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The anatomy of the cochlea forms the basis for a successful cochlear implantation. This anatomy is known to be variable in humans. Bony inner ear malformations are known to occur and even in normal cochleae, the length of cochlea and correspondingly, organ of Corti are variable [1]. Also the size of otic capsule is known to vary among individuals.
Cochlear duct length (CDL) is defined as the length of the scala media as measured from the middle of the round window to helicotrema. Preoperative measurement of the CDL in a patient can be valuable for the surgeon. This knowledge is particularly important when precise intracochlear electrode array placement is desired. Also, with variable lengths of electrodes available for implantation and reports of incomplete insertion of the longer electrodes, variability of the length of cochlear duct can be a significant variable in the depth of insertion. A preoperative estimation of the CDL can help the surgeon to choose an electrode array suitable for the patient’s anatomy and, therefore, increase the patients’ benefit after implantation.
Measurement of the CDL has been performed both histologically and radiographically. Routinely, all patients with congenital hearing loss undergo high-resolution computed tomography (HRCT) of temporal bone during workup for cochlear implantation. HRCT gives very precise quantitative information about the anatomy and morphology, especially through three-dimensional (3D) reconstructions. With the help of software and mathematical formulae we can calculate the length of cochlear duct. As per our knowledge, all the studies which have been done in this regard have been done on Caucasian skulls [2,3,4]. Asian race, and more specifically, Indian race, has smaller skulls. The aim of this study is to collect a normative data regarding the cochlear length in the Indian population. The results of this study would help the surgeons assess preoperatively about the insertion depth of the electrode array.
Materials and methods
This study was done in SMS Medical College and Hospital, Jaipur, India, which is a tertiary care hospital and referral centre for cochlear implants.
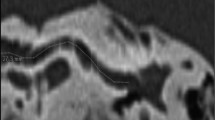
HRCT temporal bones of all the children less than 6 years of age, with congenital bilateral severe to profound SNHL who were being worked up for cochlear implant were studied and analysed. Philips Ingenuity CT machine with 128 slices was used on all these patients. A view of the basal turn of cochlea was made which showed one full turn of cochlea from round window onwards. As it is not possible to visualize the entire basal turn of cochlea using a single two-dimensional plane, a reconstruction was performed using 1-mm layer, minimum intensity projection. This cut showed entire basal turn of cochlea, round window, oval window and anterior parts of superior and lateral semicircular canals. In this view the largest distance from the round window to the lateral wall of cochlea, through the modiolus was calculated (A) (Fig. 1). For the same ear, this distance was calculated independently by two radiologists and average was taken for both values. In none of the cases was the difference of these two values more than 0.2 mm. Cochlear duct length was calculated for both sides in all patients. The formula used to calculate this was CDL = 4.16A−3.98, where CDL is cochlear duct length and A is the measured largest distance from round window to lateral wall of cochlea passing through modiolus (after G. Alexiades and C. Jolly) [5].

Measuring the variable A using high resolution computed tomography (HRCT) scan
Results
124 patients (56 females and 68 males) with hearing loss were evaluated for cochlear implantation. HRCT temporal bone of these patients was analysed. 20 patients were excluded from the study in view of vestibulocochlear anomaly. Data from the remaining 104 patients’ 208 ears (46 females and 58 males) regarding the measurement A were used to calculate the length of cochlear duct. The distance A of both the ears of these patients is depicted in Fig. 2. Mean of distance A for the right ear of these patients was 8.10 mm (range 7.7–9.2 mm). Mean for the same in the left ear of these patients was 8.14 mm (range 7.7–9.0 mm), giving an overall average of 8.12 mm. Using the formula, CDL = 4.16A−3.98, we calculated the length of cochlear duct. Mean cochlear duct length was 29.8 mm with a range from 28 to 34.3 mm.

Scatter diagram depicting the value of A in the study population
Discussion
The human cochlea was originally described by Bartholomeus Eustachius in 1564, but the description was first published by Albinus in Leyden. The human cochlea exhibits extensive anatomic variations. These variations influence the location of cochlear implant electrodes and affect the potential of hearing preservation surgery. The basis on which length of the cochlear implant electrode array has been made is the length of cochlear duct which is defined as the length of scala media as measured from the centre of round window to the helicotrema. Mary Hardy, in 1938, first described histologic measurements of CDL in 68 specimens [6]. Since then, there have been numerous publications on the variability of the size of the human cochlea, with lengths measuring from 25 to 45 mm. These measurements have been performed both in various temporal bone histology and HRCT temporal bone studies.
Measurement of the CDL can be valuable in the preoperative stage of cochlear implantation. It is particularly important when precise intracochlear placement of electrodes is desired. In patients with no residual hearing, the aim is to insert the electrode array as deep as possible to achieve a full coverage of the sensory range. In contrast, in patients with residual hearing, electrode arrays are designed to be placed only partially within the cochlea allowing electroacoustic stimulation. This precise intracochlear array positioning is important because humans, like other mammals, have tonotopically organized cochlea.
Two landmark studies have formed the basis of cochlear implant functioning. Study by Von Bekesy [2] was based on membrane elasticity and frequency position measures. He found that frequency response characteristics in all the mammals are similarly and exponentially distributed along the basilar membrane, with higher frequencies at the base and lower frequencies at the apex. Greenwood’s studies and equations [3] place a lot of importance on the length of cochlea and frequency response at a particular distance from the round window. The substantial variation found in human cochlear lengths implies that significant differences may exist in intracochlear frequency distribution. For cochlear implant recipients, understanding inter-individual frequency variations may be crucial.
Almost all the studies which have been done for estimating cochlear duct length are from the Western world where skull size and intracranial structures are larger than from the Indian subcontinent. It was important for us to study the length of cochlea in Indian population and to our knowledge and search of medical literature this is first such study from this part of the world.
In a study by Ulehlová et al. [4], they studied a group of 50 cochleae from 28 men aged 38–73 years and a great variability in the length of the cochlear duct was found ranging from 28.0 to 40.1 mm. In our study, we found mostly shorter cochlea with maximum length up to 34.3 mm. Sato et al. [7] did an interesting study in nine pairs of temporal bones from age-matched male and female individuals (1 day–76 years old) using a computer-aided three-dimensional reconstruction and measurement method. The mean cochlear length was significantly longer in males (37.1 ± 1.6 mm) than in females (32.3 ± 1.8 mm). They postulated that sexually dimorphic cochlear length may pose a new issue in auditory physiology in humans. Ketten et al. [1] applied 3D reconstructed CT of the spiral canal of cochlea in 20 patients in whom a Nucleus R cochlear implant was placed; the mean measured spiral canal length was 33.01 ± 2.31 mm in 3D CT, and the mean attained electrode depth was 20.19 ± 2.86 mm.
It was interesting to see that length of cochlear duct was less in our study. This could be due to smaller size of human skull in this geographical area. Smaller size of cochlea has its implications in understanding of hearing physiology. The frequency position map would be different for cochlea of different lengths, whether smaller or larger. Smaller length of cochlea would imply a comparatively crowded distribution of frequencies along the cochlear length. Similarly, a longer cochlear duct would mean a wider distribution of frequencies, so that an average smaller length of cochlea should necessitate a lesser insertion depth of electrode array of the cochlear implant. Also unknowingly, with the placement of a current electrode array into a smaller skull with shorter cochlear duct length inadvertent damage to the delicate inner ear structures may occur. However, large clinical studies are required and this may give more insight into whether this is a problem in cochlear implantation or not.
Conclusion
To the best of our knowledge, this is the first large sample study of cochlear length in population of this part of the world. An average smaller cochlear length is a significant finding in understanding of cochlear anatomy and physiology. It would also have great implications on the insertion depth in cochlear implantation. Presently, cochlear duct length is not even considered a factor influencing results of cochlear implantation. We propose that CDL measurement should be made an imperative part of preoperative workup for cochlear implantation and ultimately electrode array length should be tailor-made for every individual.
References
Ketten DR, Skinner MW, Wang G, Vannier MW, Gates GA, Elly JN (1998) In vivo measures of cochlear length and insertion depth of nucleus cochlear implant electrode arrays. Ann Otol Rhinol Laryngol 107:1–16
Von Bekesy G (1960) Experiments in hearing. Mc Graw Hill, New York
Greenwood DD (1990) A cochlear frequency-position function for several species—29 years later. J Acous Soc Am 87(6):2592–2605
Ulehlová L, Voldrich L, Janisch R (1987) Correlative study of sensory cell density and cochlear length in humans. Hear Res 28(2–3):149–151
Alexiades G, Dhanasingh A, Jolly C (2014) Method to estimate the complete and Two-turn cochlear duct length. Otol Neurotol 36:904–907. https://doi.org/10.1097/MAO.0000000000000620
Hardy M (1938) The length of the organ of Corti in man. Am J Anat 62:291–311. https://doi.org/10.1002/aja.1000620204
Sato H, Sando I, Takahashi H (1991) Sexual dimorphism and development of the human cochlea. Computer 3-D measurement. Acta Otolaryngol 111(6):1037–1040
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Grover, M., Sharma, S., Singh, S.N. et al. Measuring cochlear duct length in Asian population: worth giving a thought!. Eur Arch Otorhinolaryngol 275, 725–728 (2018). https://doi.org/10.1007/s00405-018-4868-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00405-018-4868-9