
Abstract
Introduction
Many studies have investigated the biomechanical influence of the acromioclavicular (AC) and coracoclavicular (CC) ligaments on the stability of the acromioclavicular joint (ACJ). It has been shown that augmentation of the CC ligaments alone can result in residual horizontal instability. Our hypothesis was that the DTF would have a significant stabilizing effect on horizontal ACJ stability.
Materials and methods
In a biomechanical in vitro study a sequential injury of the ACJ was created on eight shoulders from full body, which were placed in an upright sitting position. The translation and rotation of the clavicle were measured in relation to the acromion using an optical navigation system in various states during thoracic–humeral elevation, abduction, and horizontal adduction. The three states were: an intact shoulder, complete sectioning of the AC ligaments, and a circular lesion of the DTF.
Results
Compared to the intact state we found a significant increase in anterior rotation of the clavicle of 1.11° (p = 0.012) and a tendency in lateral translation of 2.71 mm (p = 0.017) in relation to the acromion, with a combined lesion of AC ligaments and DTF. No significant differences were found between the intact state and the isolated dissected AC ligaments as well in adduction as elevation.
Conclusion
A combined lesion of the AC ligaments and the DTF resulted in a quantitatively small but significant increase in anterior rotation and a tendency in lateral translation of the clavicle in relation to the acromion. These differences were quantitatively small, so that the clinical relevance of the stabilization effect of combined AC ligaments and DTF injuries is questionable.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Approximately 9 % of shoulder girdle injuries involve the acromioclavicular (AC) joint, with injuries appearing common in young athletes [1]. Acromioclavicular joint sprains are the most common injury of the clavicle or its articulations. The incidence rate is 9.2 per 1000 person-years, and males have a significantly higher incidence than females [2]. Based on the classification system of Rockwood [3], a sequential pattern of injury is assumed for acromioclavicular joint (ACJ) injuries, starting at the ACJ capsule and ligaments and progressing medially to a disruption of the coracoclavicular (CC) ligaments (≥grade 3). Rockwood also stated that a complete dislocation of the ACJ necessarily results in disruption of the DTF [1]. However, it has never been shown whether the disruption of the DTF should be considered simply as a (biomechanically irrelevant) consequence of ACJ dislocation, or whether a significant DTF lesion is rather the reason for high-grade ACJ instability, and therefore reflects the difference between a grade 3 and a grade 5 injury. Current studies have shown that the category of grade 3 injury includes patients with variable severity of horizontal instability [4]. Since by definition the AC and CC ligaments should be torn in such patients, the variability in horizontal instability may be due to different injury patterns to the DTF.
From a theoretical point of view, the DTF may serve as a static stabilizer of the clavicle, fixing its periosteal sleeve. On the other hand, it may act as a dynamic restraint, fixing the clavicle by load transmission from the deltoid and trapezius muscles to their insertions on the clavicle. These muscles are assumed to stabilize the ACJ in both contraction and extension [5]. As regards its anatomy, the fibers of the superior AC ligament have been shown to weave into the aponeurosis of the DTF [6], so that there may be a synergistic effect.
Urist et al. [7] assumed the DTF to be a basic horizontal restraint for the ACJ. Lizaur et al. [5] shared this view, and considered that many unsatisfactory results could be due to the lack of repair of the trapezius and deltoid after stabilization of the ACJ with temporary K-wire fixation. Furthermore, in 43 of 46 patients (93.5 %) they showed an injury to the trapezius or the deltoid, or both. However, this hypothesis has never been verified, neither clinically nor biomechanically. Although the biomechanical relevance of the AC and CC ligaments has been conclusively described, there are very few studies that have systematically investigated the biomechanical effect of the DTF.
Rochcongar et al. [8], who conducted a study on ten cadaveric shoulders using an optical tracking system, observed a significant increase in the distance between the superior part of the acromion and the superior part of the clavicle (D measure = 1.65 cm; p = 0.012) as well as that between the coracoid process and the inferior part of the clavicle (L measure = 1.24 cm; p = 0.018) after dissection of the CC ligament. They also showed a significant increase in the D (2.15 cm; p = 0.018) and L measures (1.59 cm; p = 0.0001) after arthroscopic sectioning of the AC and CC ligaments and additional open detachment of the insertions of the trapezius and deltoid muscles. But they observed no differences after the cut of the AC ligaments. However, there are no studies evaluating the effect of the DTF on anteroposterior translation and rotation in the ACJ.
This issue may be relevant, as current techniques of arthroscopically assisted ACJ stabilization focus primarily on synthetic or biological augmentation of the CC ligaments [9–16]. Such repair techniques have shown good to excellent clinical results [11, 17, 18]. Nevertheless, there is still a percentage of patients in whom CC ligament augmentation fails and who sustain a partial or complete recurrence of ACJ instability. There is some evidence that this is due to persistent horizontal ACJ instability, which inhibits healing of the CC ligaments and leads to fatigue/failure of the synthetic augmentation. Scheibel et al. [19] further showed that patients with persistent horizontal instability after CC augmentation had worse clinical results.
The purpose of the current study was to quantify the effect of the DTF and AC ligaments on multidirectional translation and rotation of the clavicle in relation to the acromion. Therefore, an in vitro set-up using whole-body specimens was used to keep the DTF intact and most realistically simulate the arm movements of the in vivo situation. Our hypothesis was that an injury to the DTF would have a significant influence on anteroposterior translation of the clavicle during passive abduction, elevation, and horizontal adduction of the arm.
Methods
We performed a biomechanical in vitro study testing eight shoulders from five human cadavers (male 1, female 4). The Ethics Committee of the Medical School Hannover gave approval for the study (No. 1694-2013). Full-body specimens were used so as to keep the vertebral insertion of the DTF intact and to allow physiologic examination during passive abduction, elevation, and horizontal adduction of the arm. A modified Thiel preservation technique from the Hannover Medical School was used to obtain the best possible flexibility of the cadavers with regard to passive arm movements. The rest of the set-up was adapted according to the established protocol of Oki et al. [20].
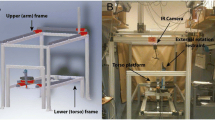
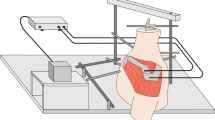
The bodies were placed upright on a custom-made examination chair and stabilized by lateral adjustable plates in the thorax area as well as in the head area (Fig. 1). In addition, tensioning straps were tightened around the forehead and thorax to fix the bodies without restricting the range of motion of the shoulder. The examination chair was developed to allow reproducible positioning of the specimens and minimize motion artefacts during the examination. To quantify the translation and rotation of the AC joint, an optical navigation system, (Type Polaris P4 Northern Digital Incorporation, Waterloo, Canada), and a custom-made software tool (NI LABview, National Instruments, Munich, Germany) were used. According to the product specification the system has a root mean square of 0.35 mm.

Experimental setup with sitting body in the special and fixation. Four marker of the optic navigation system (Polaris P4, NDI, Waterloo, Canada) (sternum, clavicle, acromion and humerus)
The system used two cameras and four optical markers. The four markers were fixed by 2 mm K-wires at predefined positions: middle third of the sternum, lateral third of the clavicle, lateral acromion, and lateral distal humeral shaft in the area of the attachment of the deltoid muscle (Fig. 1).
The recommendations of the International Society of Biomechanics (IBS) were implemented to define the coordinate system and to determine the orientation of the axes (Fig. 2) [21]. As specified by the IBS, the anatomical points were sampled with the exception of the spinous process of T8 and the acromial angle, and using these coordinates the position, orientation, and motion of the objects were calculated.

Coordinate systems for the clavicle (blue) and humerus (green) according to the recommendation of the IBS [21]. Defined motions for the blue coordinate system: Rotation around the z-axis—internal-external, rotation around the y-axis—anteroposterior and rotation around the x-axis—superoinferior. Translation X-anteroposterior direction, translation Y-superoinferior direction and translation Z-mediolateral direction (t thorax; c clavicle; s scapula and h humerus)
Three testing conditions were investigated: intact shoulder, complete sectioning of the AC ligaments (Fig. 3), and an additional circular lesion of the DTF (Fig. 4).

Left shoulder with skin incision over the clavicle and dissected AC ligaments. The marking arrows show the entire lesion of the ACJ (D:M deltoid; T:M trapezius)

Right shoulder with skin incision over the clavicle. The marking arrows show the detachment of the DTF (C Clavicle; D:M deltoid, T:M trapezius)
Surgical technique
After the intact shoulder measurement was made, the AC ligaments were dissected. For this purpose a 2 cm superior incision was made above the ACJ, having previously detected the ACJ with a 2 mm K-wire. The subcutaneous adipose tissue was also cut. Intact AC ligaments were found in all specimens. Subsequently, the AC ligaments and capsule were completely severed (Fig. 3). In order to restore the stabilizing effect of the skin, this was closed with interrupted sutures. For the cut through the DTF, the sutures were opened and the skin incision was extended medially to 8 cm. The DTF was intact in all specimens. This was followed by complete section of the DTF, which was then dissected from the anterior and posterior clavicle (Fig. 4). The skin was reclosed with interrupted sutures.
In order to mobilize the shoulder and to establish a reproducible passive range of motion, the arm was moved five times manually in all test directions (horizontal adduction, abduction, and anteversion) before the measurements were started.
The testing protocol consisted of two sets with eight repetitions of the movement for each state, and the translations and rotations of the clavicle were measured against the acromion. The following passive arm movements were performed manually by the same investigator: abduction in the frontal plane, horizontal adduction in the horizontal plane, and elevation in the sagittal plane. During abduction and elevation the elbow joint was extended and the thumb pointed up. During adduction the arm was elevated with the palm facing down, simulating a cross-body adduction stress test [22].
Data analysis
In order to obtain comparable results, the minimum range of motion of all body donors was determined for all movements. For data evaluation purposes, this minimum range was set as the end point of humerothoracic movement in all body donors. At the start and end points the position of the clavicle was determined in relation to the position of the acromion, and the motion of the clavicle was defined as ‘clavicle movement’. The clavicle movements were defined in relation to the acromion according to the predefined coordinates.
Statistical analysis
The results are given as means and standard errors (SE). The structural parameters obtained from the three testing conditions of the investigation were analysed using a nonparametric Wilcoxon’s test for connected samples. The statistical analysis was performed using SPSS 14.0 (SPSS Inc., Chicago, IL, USA), and p < 0.05 was considered significant. Because there were three paired comparisons, the use of the Bonferroni adjustment was needed, and the new significance level was calculated. This meant that the new adjusted significance level was p < 0.017.
Results
The minimum range of humerothoracic abduction was 65°. The minimum range of adduction was 60° and elevation 65°.
The observed motion of the clavicle against the acromion with an intact ACJ and DTF exhibited an internal rotation of 15.17°, anterior rotation of 6.61°, and superior rotation of 13.79° during adduction (Fig. 5). During the humerothoracic elevation of 65° internal rotation was 22.32°, anterior rotation was 6°, and superior rotation was 16.6° (Fig. 6). During abduction the clavicle presented an internal rotation of 14.13°, 2.27° anterior and 12.4° superior (Fig. 7).

Results of the adduction of all three states. Rotation (Phi z, Theta y and Psi x). Translation (X, Y and Z)

Results of the elevation of all three states. Rotation (Phi z, Theta y and Psi x). Translation (X, Y and Z)

Results of the abduction of all three states. Rotation (Phi z, Theta y and Psi x). Translation (X, Y and Z)
During adduction the clavicle showed an anterior translation of 8.59 mm, 15.87 mm superior and 8.09 mm lateral. The anterior translation during the elevation was 6.05 mm, superior translation was 17.35 mm and lateral was 5.97 mm. During abduction the results for translation were 3.14 mm anterior, 8.23 mm superior, and 3.59 mm lateral.
We found no significant differences between the intact state and the state after the dissected AC ligaments. Furthermore, no significant differences were found between the state of dissected AC ligaments and the dissected DTF. After additional separating the AC ligaments from the DTF we found a significant increase in anterior rotation of the clavicle of 1.11° (p = 0.012) against the acromion in abduction. In the same state of injury a tendency in lateral translation of 2.71 mm (p = 0.017) was observed (Fig. 7).
Discussion
The purpose of the present study was to investigate the influence of the DTF on the vertical and horizontal stability of the ACJ. For a combined injury of the AC ligaments and the DTF we found a significant but quantitatively small increase in anterior rotation of the clavicle relative to the acromion of 1.11°. We also found a tendency in lateral translation of 2.71 mm (movement of the distal clavicle beyond the acromion).
At the first view the increase in translational and rotational movements appear to be very small and may appear to be irrelevant, but the results should be compared with the range of motion of the intact ACJ. This has previously been investigated with abduction of the arm in the scapular plane using MRI or CT, or even after pin fixation and optical tracking.
In an open MRI study Sahara et al. [23] found anterior translation of the clavicle of 1.9 mm during abduction up to 90°, and posterior translation of 1.6 mm from 90° to maximum abduction in the coronal plane. The authors also found superoinferior translation of 0.9 mm at maximum abduction [23]. In a high-resolution CT study a maximum internal rotation of the distal clavicle of 37.1° was observed in 10 patients in abduction between 0° and 180° in the coronal plane. The shoulders were scanned at 0°, 60°, 120°, and 180° of active abduction. Between 0° and 60° of abduction the authors found a posterior translation of 4 mm and between 60° and 180° abduction an anterior translation of 1.9 mm [24]. The studies of Sahara et al. [23] and Seo et al.[24] showed that the range of horizontal and vertical translation of the intact ACJ is quite small, and significantly smaller than that in cadaver studies using direct force applied to the clavicle or scapula.
In an in vivo study using an optical tracking set-up with pins fixed in the clavicle, scapula, and humerus, Ludewig et al. [25] found a mean range of motion of 31° internal rotation, 16° posterior rotation, and 6° elevation during sagittal plane flexion, coronal plane abduction and scapular plane abduction. The range of motion of the clavicle was given in relation to the thorax. Ludewig et al. [25] found in their subjects a range of motion in sagittal plane flexion, coronal plane abduction and scapular plane abduction o at least 120°. In the studies of Sahara et al. [23, 26] subjects reached a range of motion for abduction of the shoulder from 0° to maximum abductions. Sahara et al. [26] observed the significant increase in retraction of the clavicle above 90° of abduction in their investigation of the three-dimensional clavicular and acromioclavicular rotations during arm abduction using vertically open MRI. Further, the elevation increased between 0° and 150° abduction as well as the axial posterior rotation increased above 60° abduction. The studies of Ludewig [25] and Sahara et al. [23, 26] showed clearly that an abduction of at least 60° must be achieved to emerge significant difference in the movement of the clavicle. The humerothoracic abduction was only 65°. The adduction was 60 and the elevation was 65°. In this study the minimum has been reached, but not much, which was a clar limitation of the study. The reason for this small range of motion was the type of fixation and the age of the specimens.
The biomechanical effect of the AC ligaments has been investigated by several authors, who showed the ligaments to be basic restraints against posterior and anterior translation, [27–29] and that dissection of the AC ligaments results in an increased in situ force of the CC ligaments [30]. In contrast to these studies, we did not apply a force directly to the clavicle but instead simulated a clinical patient examination, with passive movements of the affected arm. This approach led to smaller translations, but Teece et al. [31] further found that ACJ translations during passive movement of the arm in cadaver studies were similar to in vivo ACJ kinematics.
In the current study no significant increase in horizontal translation and rotation was found after isolated AC ligament dissection, but after a combined lesion of the AC ligaments and the DTF this reached a significant level. In effect, the circular lesion of the DTF aggravated the effect of the AC ligament dissection. This means that both structures act synergistically. This was comparable to Rochcongar et al. [8], who found also no difference in translation of the clavicle after the cut of the AC ligaments.
The protocol and set-up of the current study and protocol was adapted to that of Oki et al. [20], who, in contrast to our results, observed increased posterior rotation of the clavicle after separating the AC ligaments. This effect was found with elevation of the arm in the sagittal plane between 80° and 120° with 4° posterior rotation, and in adduction in the horizontal plane >45° with 4.7° posterior rotation of the clavicle.
As a limitation, despite our initial purpose we were unable to achieve a full range of shoulder motion during passive testing. The limited range of motion was caused by partial shoulder stiffness in most of the cadavers, even though a modified Thiel preservation technique was used. This issue needs to be kept in mind when our results are compared with those of other studies. Further the range of translational and rotational movements may have been inferior compared to other studies, since we did not perform additional dissection of the CC ligaments. One could argue that the injury pattern of a combined AC ligament and DFT lesion is unlikely to be seen in clinical practice, as the CC ligaments are known to tear with grade 3 injuries. Nevertheless, our aim was to specifically quantify the effect of the DTF. Therefore, additional sectioning of the CC ligaments would not have provided further information. Second, our aim was to evaluate the clinical situation of anatomically perfectly done CC ligament reconstruction (compared with intact CC ligaments) with that of an ongoing lesion of the AC ligaments and the DTF. This testing condition should represent the situation after optimal surgical CC augmentation. Based on our results, even in such cases the lesion of the AC ligaments and the DTF results in a small but significant increase in ACJ translation and rotation. However, the effect of the DTF lesion, and even that of the combined AC ligaments and DTF lesion, was smaller than we had expected.
In conclusion, the current study revealed significant but quantitatively small increases in rotation of the clavicle with a combined lesion of the AC ligaments and the DTF, so that can be concluded that the biomechanical influence of the DTF on the AC joint is low. But this study provides evidence that the DTF has a synergistic stabilizing effect with the AC ligaments.
References
Mazzocca AD, Arciero RA, Bicos J (2007) Evaluation and treatment of acromioclavicular joint injuries. Am J Sports Med 35:316–329. doi:10.1177/0363546506298022
Pallis M, Cameron KL, Svoboda SJ, Owens BD (2012) Epidemiology of acromioclavicular joint injury in young athletes. Am J Sports Med 40:2072–2077. doi:10.1177/0363546512450162
Rockwood C, Wirth M (1996) Injuries to the acromioclavicular joint. In: Rockwoood CA Green DP Buchholz RW Heckmann JA Eds Fract. Adults. Lippincott-Raven, Philadelphia, pp 1341–1414
Wellmann PDM, da Silva G, Lichtenberg S et al (2013) Instabilitätsmuster bei Akromioklavikulargelenkverletzungen vom Typ Rockwood III. Orthop 42:271–277. doi:10.1007/s00132-013-2085-1
Lizaur A, Marco L, Cebrian R (1994) Acute dislocation of the acromioclavicular joint. Traumatic anatomy and the importance of deltoid and trapezius. J Bone Joint Surg Br 76:602–606
Sellards R (2004) Anatomy and biomechanics of the acromioclavicular joint. Oper Tech Sports Med 12:2–5. doi:10.1053/j.otsm.2004.04.006
Urist MR (1946) Complete dislocations of the acromioclavicular joint. J Bone Jt Surg 28:813–837
Rochcongar G, Emily S, Lebel B et al (2012) Measure of horizontal and vertical displacement of the acromioclavicular joint after cutting ligament using X-ray and opto-electronic system. Surg Radiol Anat 34:639–643. doi:10.1007/s00276-012-0953-8
Beitzel K, Obopilwe E, Apostolakos J et al (2014) Rotational and translational stability of different methods for direct acromioclavicular ligament repair in anatomic acromioclavicular joint reconstruction. Am J Sports Med 42:2141–2148. doi:10.1177/0363546514538947
Hou Z, Graham J, Zhang Y et al (2014) Comparison of single and two-tunnel techniques during open treatment of acromioclavicular joint disruption. BMC Surg 14:53. doi:10.1186/1471-2482-14-53
Metzlaff S, Rosslenbroich S, Forkel PH et al (2014) Surgical treatment of acute acromioclavicular joint dislocations: hook plate versus minimally invasive reconstruction. Knee Surg Sports Traumatol Arthrosc Off J ESSKA. doi:10.1007/s00167-014-3294-9
Muccioli GMM, Manning C, Wright P et al (2014) Acromioclavicular joint reconstruction with the LARS ligament in professional versus non-professional athletes. Knee Surg Sports Traumatol Arthrosc. doi:10.1007/s00167-014-3231-y
Nüchtern JV, Sellenschloh K, Bishop N et al (2013) Biomechanical evaluation of 3 stabilization methods on acromioclavicular joint dislocations. Am J Sports Med 41:1387–1394. doi:10.1177/0363546513484892
Pan Z, Zhang H, Sun C et al (2014) Arthroscopy-assisted reconstruction of coracoclavicular ligament by Endobutton fixation for treatment of acromioclavicular joint dislocation. Arch Orthop Trauma Surg. doi:10.1007/s00402-014-2117-2
Virtanen KJ, Savolainen V, Tulikoura I et al (2014) Surgical treatment of chronic acromioclavicular joint dislocation with autogenous tendon grafts. SpringerPlus. doi:10.1186/2193-1801-3-420
Wellmann M, Kempka JP, Schanz S et al (2009) Coracoclavicular ligament reconstruction: biomechanical comparison of tendon graft repairs to a synthetic double bundle augmentation. Knee Surg Sports Traumatol Arthrosc 17:521–528. doi:10.1007/s00167-009-0737-9
Liu X, Huangfu X, Zhao J (2013) Arthroscopic treatment of acute acromioclavicular joint dislocation by coracoclavicular ligament augmentation. Knee Surg Sports Traumatol Arthrosc. doi:10.1007/s00167-013-2800-9
Fauci F, Merolla G, Paladini P et al (2013) Surgical treatment of chronic acromioclavicular dislocation with biologic graft vs synthetic ligament: a prospective randomized comparative study. J Orthop Traumatol 14:283–290. doi:10.1007/s10195-013-0242-2
Scheibel M, Dröschel S, Gerhardt C, Kraus N (2011) Arthroscopically Assisted Stabilization of Acute High-Grade Acromioclavicular Joint Separations. Am J Sports Med 39:1507–1516. doi:10.1177/0363546511399379
Oki S, Matsumura N, Iwamoto W et al (2012) The function of the acromioclavicular and coracoclavicular ligaments in shoulder motion: a whole-cadaver study. Am J Sports Med 40:2617–2626. doi:10.1177/0363546512458571
Wu G, van der Helm FCT, Veeger HEJD et al (2005) ISB recommendation on definitions of joint coordinate systems of various joints for the reporting of human joint motion–Part II: shoulder, elbow, wrist and hand. J Biomech 38:981–992
Chronopoulos E, Kim TK, Park HB et al (2004) Diagnostic value of physical tests for isolated chronic acromioclavicular lesions. Am J Sports Med 32:655–661. doi:10.1177/0363546503261723
Sahara W, Sugamoto K, Murai M et al (2006) 3D kinematic analysis of the acromioclavicular joint during arm abduction using vertically open MRI. J Orthop Res 24:1823–1831. doi:10.1002/jor.20208
Seo Y-J, Yoo Y-S, Noh K-C et al (2012) Dynamic function of coracoclavicular ligament at different shoulder abduction angles: a study using a 3-dimensional finite element model. Arthrosc J Arthrosc Relat Surg 28:778–787. doi:10.1016/j.arthro.2012.04.001
Ludewig PM, Phadke V, Braman JP et al (2009) Motion of the shoulder complex during multiplanar humeral elevation. J Bone Jt Surg 91:378–389. doi:10.2106/JBJS.G.01483
Sahara W, Sugamoto K, Murai M, Yoshikawa H (2007) Three-dimensional clavicular and acromioclavicular rotations during arm abduction using vertically open MRI. J Orthop Res 25:1243–1249. doi:10.1002/jor.20407
Fukuda K, Craig EV, An KN et al (1986) Biomechanical study of the ligamentous system of the acromioclavicular joint. J Bone Jt Surg 68:434–440
Klimkiewicz JJ, Williams GR, Sher JS et al (1999) The acromioclavicular capsule as a restraint to posterior translation of the clavicle: a biomechanical analysis. J Shoulder Elb Surg Am Shoulder Elb Surg Al 8:119–124
Lee KW, Debski RE, Chen CH et al (1997) Functional evaluation of the ligaments at the acromioclavicular joint during anteroposterior and superoinferior translation. Am J Sports Med 25:858–862
Debski RE, Parsons IM, Woo SL-Y, Fu FH (2001) Effect of capsular injury on acromioclavicular joint mechanics. J Bone Jt Surg 83:1344–1351
Teece RM, Lunden JB, Lloyd AS et al (2008) Three-dimensional acromioclavicular joint motions during elevation of the arm. J Orthop Sports Phys Ther 38:181–190. doi:10.2519/jospt.2008.2386
Acknowledgments
The study was funded by the German speaking society of arthroscopy and joint surgery (AGA, Porzellangasse 8/23, 1090 Vienna, Austria).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
None.
Rights and permissions
About this article

Cite this article
Pastor, M.F., Averbeck, A.K., Welke, B. et al. The biomechanical influence of the deltotrapezoid fascia on horizontal and vertical acromioclavicular joint stability. Arch Orthop Trauma Surg 136, 513–519 (2016). https://doi.org/10.1007/s00402-015-2389-1
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-015-2389-1