
Abstract
Introduction
Surgical versus orthopedic treatments of acromioclavicular disjunction are still debated. The aim of this study was to measure horizontal and vertical acromion’s displacement after cutting the ligament using standard X-ray and an opto-electronic system on cadaver.
Materials and methods
Ten cadaveric shoulders were studied. A sequential ligament’s section was operated by arthroscopy. The sequence of cutting was chosen to fit with Rockwood’s grade. The displacement of the acromion was measured on standard X-ray and with an opto-electronic system allowing measuring of the horizontal displacement. Statistical comparisons were performed using a paired Student’s t test with significance set at p < 0.05.
Results
Cutting the coracoclavicular ligament and delto-trapezius muscles cause a statistical downer displacement of the acromion, but not after sectioning the acromioclavicular ligament. The contact surface between the acromion and the clavicle decreases statistically after sectioning the acromioclavicular ligament and the coracoclavicular ligament with no effect of sectioning the delto-trapezius muscles. Those results are superposing with those dealing with the anterior translation.
Discussion
The measure concerning the acromioclavicular distance and the coracoclavicular distance are superposing with those of Rockwood. However, there is a significant horizontal translation after cutting the acromioclavicular ligament. Taking into account this displacement, it may be interesting to choose either surgical or orthopedic treatment.
Conclusion
There is a correlation between anatomical damage and importance of instability. Horizontal instability is misevaluated in clinical practice.
Level of evidence
Basic science study.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The anatomy and biomechanics of the acromioclavicular (AC) joint is now well known. This is a di-arthrodial joint, facing mostly laterally and superiorly [5, 15]. This articulation is stabilized by intrinsic (AC superior and inferior ligaments) and extrinsic (coracoclavicular ligaments) ligaments. The superior AC ligament has a very intimate contact with the delto-trapezius muscles. Those muscles stabilize the clavicle with its anterior and posterior insertions [13]. The AC ligaments limit the displacements of the clavicle backward, forward, and upward to small displacements. The coracoclavicular ligaments are conoid and trapezoid ligaments. They are anatomically additional. The first one is in the frontal plane, whereas the second one is in the sagittal plane. Concerning biomechanics, the conoid ligament resist to tearing and anteroposterior forces, mostly in large movements, while the trapezoid is opposed to axial compression [6, 8, 14]. Finally, trapezius and deltoid muscles are static and dynamic stabilizers because of their antagonistic action [13].
AC disjunction is a frequent cause of consultation at the emergency room. Males under 35 years are the most common cases. The trauma is mostly located on the upper part of the acromion with the arm in adduction [7, 14].The Rockwood classification is the most used to assess AC disjunction and guide operative therapeutics [14]. It classifies lesions into six grades by measuring the coracoclavicular distance on a Zenca X-ray view. Each grade is represented on a radiological displacement scale. From this measurement, Rockwood defines the anatomical lesion. Type 1, X-ray is normal and AC ligament are just sprained. Type II, injured shoulder as a widened AC joint but coracoclavicular distance is normal. Type III, AC joint is widened and coracoclavicular distance is widened 20–100 %. Type V corresponds to a complete disruption of AC joint. Coracoclavicular distance is widened 100–300 %.
From those grades, therapeutic we`re proposed [14]. Nevertheless, the management of grade III remains controversial. The actual trend in this case is to prefer functional treatment, because recent randomized studies do not show significant difference between functional and surgical treatment for long-term result [3, 16, 18].
However, the results of surgical or orthopedic treatment are sometimes disappointing [3, 4] and question remains. It’s established that the importance of residual laxity is not related with functional outcome [9]. The correlation between the amount of displacement of the clavicle and ligaments injuries is still unclear. The aim of this study was to investigate the correlation between progressive sections of the elements of stability of the AC joint and the importance of vertical and horizontal displacement of the acromion. After each ligamentary section, acromion’s displacement was assessed using Zenca view and an opto-electronic system. Our findings were compared to Rockwood class.
Materials and methods
Ten fresh frozen (five right and five left) cadaveric shoulders obtained from unclaimed body were used for this experimental study (mean age 64 ± 6 years). One was excluded from the study because of a moving acromial bone. The upper side of the body was fixed to the table using studs, allowing free motion of the arm. The clavicle was fixed by two Kirshner 25/10 pins (a claviculospinal pin and a costoclavicular pin). To achieve the stress radiographies and opto-electronic study avoiding parasitic glenohumeral movement, acromial traction was done using a transacromial lack with 4 kg weight. The posteroanterior traction was managed through a pulley hanged to a fixed point on the wall. Ligament section was realized by arthroscopy. The view portal was anterolateral and the instrumental portal was anterior. Arthroscopy begins with a resection of the subacromial bursa with a shaver. Then for each shoulder, we conducted a sequential section beginning with AC ligament, following by coracoclavicular ligament. Finally, a superior open surgery approach of the AC joint was realized to cut the insertions of the deltoid and trapezius muscles. This progressive section was realized to reproduce the II, III and V Rockwood’s class.
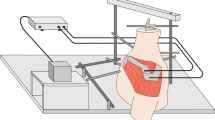
Displacement was measured on X-ray Zenca view. The radio equipment was not moved between each X-ray, allowing accurate comparison of images. Displacement was also measured using an optical tracking system (Strycker, Howmedica, Ruthefort, USA) composed of IGT cameras 580 mm (3 LED 50 mm active IGT) and a flashpoint (i5000, IGT, Leibinger, Strycker). Two trackers were used, placed on the medial part of the clavicle and on the spine of the scapula. At each stage, we realized a Zenca X-ray [20]. Image was analyzed using Osirix software (Pixmeo SARL, Bernex, Switzerland) measuring the distance between the superior part of the acromion and the superior part of the clavicle (D measure). Also the distance between the coracoid process and the inferior part of the clavicle was measured (L measure). Those measures are shown in Fig. 1. After the dissection, the distal part of the clavicle and the articular part of the acromion were digitalized to orientate the articular surface into the camera co-ordinate system. A numeric AC joint in three dimensions was obtained. The same D measure was done using those results. The percentage of the both articular surface in contact during the traction was also calculated when supero-inferior traction (S1 surface) and when postero-anterior traction (S2 surface) was performed. Finally, we measured the anterior displacement of the distal part of the clavicle in regards to the acromion (T measure). Those measures were done for each shoulder before cutting any ligament with and without traction. Then after each section, we realized using only stressed view.

Measure of D and L after cutting the AC and coracoclavicular ligament. Two trackers (T): one in the spine of the scapula and one in the clavicle
Those measures were compared with each other and with the results corresponding to the Rockwood’s classification. The different measures were statistically compared using a paired Student’s t test. Statistical difference was established at 5 %.
Results
Before any ligament section, no statistical difference was observed comparing loaded and unloaded conditions using either radiological or opto-electronic assessment.
Results of the radiological study were presented in Table 1 and Fig. 2. The cut of the AC ligament had no effect on D and L measure. The section of coracoclavicular ligament increased significantly the D distance (p = 0.012) and L distance (p = 0.018) and also the section of the delto-trapezius muscle’s insertions increased the D distance (p = 0.018) and the L distance (p = 0.0001).

Variation of the mean of distance D and L after cutting each ligament. CC coracoclavicular ligament, DT delto-trapezius insertion
Results of the opto-electronic study were presented in Table 2. The statistical analyses of D distance performed with the opto-electronic system highlighted the same differences with conventional X-ray. However, opto-electronic measurements were always higher.
Analyzing the T distance, a statistical difference was observed after cutting the AC ligament (p = 0.019) and after cutting the coracoclavicular ligament (p = 0.02) with no effect of the delto-trapezius muscle’s insertions section (p = 0.059). We analyzed surface of contact S1 and S2. There was a statistical influence of AC ligament section (p = 0.029 for S1 and p = 0.033 for S2) and coracoclavicular ligaments section (p = 0.01 for S1 and p = 0.029 for S2) in reducing the contact surfaces. Nevertheless, section of the muscle’s insertion had no effect on those contact surfaces (p = 0.11 for S1 and p = 0.14 for S2).
Discussion
The aim of this study was to evaluate the correlation between AC displacement and anatomical lesion reported to the Rockwood classification. This correlation is still to debate regarding to the lack of evidence with the treatment of type III AC disjunction [10]. Our results confirm the influence of anatomical damage on the superior displacement of the clavicle. We also investigate the anteroposterior displacement and the contact surface which was poorly related before.
This experimental model was intended to reproduce the real life condition, the fall of the scapula beside the clavicle. However, it is a small cadaveric series. To reproduce in vivo AC stress, weighted X-ray was realized. The utility of this X-ray is still debated in clinical practice [2]. But this kind of X-ray was also used by Sluming and all [17]. More over, X-ray analysis was carried out using standardized view and validates software used in previous study [11].
Our results are in concordance with the results of Rockwood [14]. The average increase of the L distance for grade II is 15 %, 71 % for grade III (31–120 %), and 122 % for grade V (85–181 %), while Rockwood defines the type III as an increase form 20–100 % and 100–300 % for type V [14]. This confirmed the role of the coracoclavicular ligament to stabilize the clavicle against upper displacement showed by Fukuda [8].
However, medical or surgical treatment option of type III is still undecided [3–5]. Some echographic studies pointed out that sometimes there is a disruption of the clavicular insertion of the deltoid and the trapezius in type III [10]. Moreover, when X-ray shows type III lesion, MRI can highlight a sprain of conoid and trapezoid ligaments or an isolated disruption of the coracoclavicular ligaments without lesion of the acromioclavicular ligament [1]. The correlation between measures carried out on X-ray and anatomical lesion is not so clear.
Concerning the distance T (anteroposterior translation), we also find an increased laxity after each cut of ligament. The higher augmentation is after sectioning the coracoclavicular ligament. The results concerning the articular contact corresponding to surface S2 follow the same tendency. This fits with the biomechanical study of Fukuda [8] which defines the conoid as the primary restrainers of anteroposterior displacement in big displacement. An isolated coracoclavicular ligament disruption predominantly might be responsible for instability mainly in the horizontal plan. In those cases, frontal X-ray is normal. The Rockwood’s classification misevaluates the severity.
The evaluation of this horizontal instability is very important in clinical practice. Indeed the study of Tauber [19] pointed out the variability of this instability in patient consulting for type II or III of Rockwood. As for us, we observe an anterior translation of the acromion about 3.1 mm after cutting the AC ligament. This grows to 7.3 mm after cutting the coracoclavicular ligament. There is only 0.3 mm anterior translation in a non-injured shoulder. The decrease of surface S2 corresponding to an anteroposterior instability can explain a stress peak. This may explain an AC arthropathy at mid-term. This horizontal instability is probably too neglected in clinical practice, explaining a part of poor results in some surgical or medical treatment in type II or III [4, 12].
Tauber et al. propose to analyze the horizontal instability in measuring an angle between glenoid and the acromioclavicular joint. This interesting option could be difficult to realize in daily practice in an acute trauma but much more difficult in chronic disorder. In fact, the study of horizontal instability is insufficient in clinical practice to better classify AC disjunction. Taking into account this instability could improve clinical results of AC disjunction treatment in types II and III.
Conclusion
This study confirms the importance of upper displacement of the clavicle after cutting not only the AC ligaments but also the coracoclavicular ligaments. It also quantifies the posterior displacement of the clavicle which is poorly measured in previous study. Quantifying this displacement in clinical practice is probably important. However, it needs an easy reproducible X-ray. Taking into account this instability should improve the clinical results of types II and III.
References
Alyas F, Crutis M, Speed C, Saifuddin A, Connell D (2008) MR imaging appearances of acromioclavicular joint dislocation. Radiographics 28:463–479. doi:10.1148/rg.282075714
Bossart MJ, Joyce FM, Manaster P, Packer M (1988) Lack of efficacy of ‘weighted’ radiographs in diagnosing acute acromioclavicular separation. Ann Emerg Med 17:20–24. doi:10.1016/S0196-0644(88)80497-9
Calvo E, López-Franco M, Arribas IM (2006) Clinical and radiologic outcomes of surgical and conservative treatment of type III acromioclavicular joint injury. J Shoulder Elbow Surg 15:300–305. doi:10.1016/j.jse.2005.10.006
Ceccarelli E, Bondi R, Alviti F, Garofalo R, Miulli F, Padua R (2008) Treatment of acute grade III acromioclavicular dislocation: a lack of evidence. J Orthop Traumatol 9:105–108. doi:10.1007/s10195-008-0013-7
Colegate-Stone T, Allom R, Singh R, Elias DA, Standring S, Sinha J (2010) Classification of the morphology of the acromioclavicular joint using cadaveric and radiological analysis. J Bone Joint Surg Br 92-B:743–746. doi:10.1302/0301-620X.92B5.22876
Debski R, Parsons IM, Fenwick J, Vangura A (2000) Ligament mechanics during three degree-of-freedom motion at the acromioclavicular joint. Ann Biomed Eng 28:612–618. doi:10.1114/1.1304848
Fraser-Moodie JA, Shortt NL, Robinson CM (2008) Injuries to the acromioclavicular joint. J Bone Joint Surg Br 90-B:697–707. doi:10.1302/0301-620X.90B6.20704
Fukuda K, Craig EV, An KN, Cofield RH, Chao EY (1986) Biomechanical study of the ligamentous system of the acromioclavicular joint. J Bone Joint Surg Am 68-A:434–440
Gstettner C, Tauber M, Hitzl W, Resch H (2008) Rockwood type III acromioclavicular dislocation: surgical versus conservative treatment. J Shoulder Elbow Surg 17:220–225. doi:10.1016/j.jse.2007.07.017
Heers G, Hedtmann A (2005) Correlation of ultrasonographic findings to Tossy’s and Rockwood’s classification of acromioclavicular joint injuries. Ultrasound Med Biol 31:725–732. doi:10.1016/j.ultrasmedbio.2005.03.002
Lee M, Chebli C, Mounce D, Bertelsen A, Richardson M, Matseniii F (2008) Intramedullary reaming for press-fit fixation of a humeral component removes cortical bone asymmetrically. J Shoulder Elbow Surg 17:150–155. doi:10.1016/j.jse.2007.03.032
Mikek M (2008) Long-term shoulder function after type I and II acromioclavicular joint disruption. Am J Sports Med 36:2147–2150. doi:10.1177/0363546508319047
Renfree KJ, Wright TW (2003) Anatomy and biomechanics of the acromioclavicular and sternoclavicular joints. Clin Sports Med 22:219–237
Rockwood C, Matsen F, Wirth M, Lippitt S (2009) The shoulder: acromioclavicular traumatic disorder, 4th edn. Saunders Elsevier, Philadelphia
Salter EG, Nasca RJ, Shelley BS (2007) Anatomical observations on the acromioclavicular joint and supporting ligaments. Am J Sports Med 15:199–206. doi:10.1177/036354658701500301
Simovitch R, Sanders B, Ozbaydar M, Lavery K, Warner JJP (2009) Acromioclavicular joint injuries: diagnosis and management. J Am Acad Orthop Surg 17:207–219
Sluming VA (1995) A comparison of the methods of distraction for stress examination of the acromioclavicular joint. Br J Radiol 68:1181–1184. doi:10.1259/0007-1285-68-815-1181
Tamaoki MJS, Belloti JC, Lenza M, Matsumoto MH, Dos Gomes Santos JB, Faloppa F (2010) Surgical versus conservative interventions for treating acromioclavicular dislocation of the shoulder in adults. Cochrane Database Syst Rev 4(8):CD007429. doi:10.1002/14651858.CD007429.pub2
Tauber M, Koller H, Hitzl W, Resch H (2010) Dynamic radiologic evaluation of horizontal instability in acute acromioclavicular joint dislocations. Am J Sports Med 38:1188–1195. doi:10.1177/0363546510361951
Zanca P (1971) Shoulder pain: involvement of the acromio-clavicular joint (analysis of 1,000 cases). Am J Roentgenol 112:493–506
Acknowledgments
The authors would like to acknowledge Miss Solène Gouzy for the technical support.
Conflict of interest
The authors affirm that there is non conflict of interest and no financial biases.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Rochcongar, G., Emily, S., Lebel, B. et al. Measure of horizontal and vertical displacement of the acromioclavicular joint after cutting ligament using X-ray and opto-electronic system. Surg Radiol Anat 34, 639–643 (2012). https://doi.org/10.1007/s00276-012-0953-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00276-012-0953-8