
Abstract
Objectives
To compare the clinical performance and surgical outcomes of the new digital single use flexible ureteroscope (WiScope®) with a reusable digital flexible ureteroscope.
Patient and methods
Our prospective study includes patients with renal stones less than 2 cm who underwent retrograde flexible ureteroscopy and laser lithotripsy. Patients were randomized into two groups: group A included patients who underwent laser lithotripsy using WiScope® Single use digital flexible ureteroscope and group B included patients who underwent laser lithotripsy using reusable flexible ureteroscope. Image quality, deflection, ease of insertion, maneuverability, and overall performance were assessed using either a visual analog or Likert scale. Operative outcomes and complications were collected and analyzed in both groups.
Results
A total of 242 patients were included in our study. There were 121 patients in the WiScope® group and 121 patients in reusable ureteroscope group. The WiScope® had higher maneuverability (9.3 ± 0.7 vs. 7.2 ± 0.8, P < 0.001) and less limb fatigue but had lower image quality when compared to reusable digital flexible ureteroscope (7.6 ± 0.9 vs. 9.2 ± 0.6, P < 0.001). There were no differences in operative time, complication rates and rates of relook ureteroscopy.
Conclusions
The WiScope® single use flexible ureteroscope has comparable outcomes to the reusable flexible ureteroscope with regard to maneuverability, limb fatigue, and deflection. However, it has a lower image quality.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
In the last decade, technological advances have led to improvements in the area of endourology and urinary stone management [1]. Ureteroscopes have been used to help manage urinary calculi since they were originally developed in 1912 by Young [2]. Since the first fiber-optic ureteroscope was developed by Marshall in 1964, there have been significant improvements in image quality, performance, and durability [3]. In the last century, flexible ureteroscopy has become widespread in the treatment of urinary tract stones [4, 5].
However, several problems are associated with reusable flexible ureteroscopes, including high costs for sterilization and repair, poor durability, and the risk of transmitting infection between patients [6, 7]. Several studies have reported that the use of disposable ureteroscopes is increasing, especially when there is a high risk of damage to a ureteroscope, such as when treating lower pole calculi [8, 9]. Damage to reusable ureteroscopes that requires repair is likely after 10–25 uses, and a ureteroscope that has been repaired once is more likely to be damaged again [10].
The purpose of this study is to evaluate the performance of the WiScope single-use digital flexible ureteroscope. Maneuverability, overall performance, visual quality, stone-free rate, and postoperative complications were used to evaluate the effectiveness of the WiScope ureteroscope for managing renal calculi. This paper also compares outcomes after treatment with the WiScope ureteroscope to those associated with reusable flexible ureteroscopes.
Patients and methods
All patients who presented at our outpatient clinic with renal stones suitable for treatment with flexible renoureteroscopy (FURS) between January 2020 and August 2021 were included in this prospective, randomized study. All included patients were at least 18 years old and had a renal stone burden up to 2 cm. Pregnant women, patients with an active UTI or known ureteral stricture, and those who had previously undergone surgical intervention or SWL for the same calculi were excluded from the study.
All included patients were randomly assigned to either group A or group B using the opaque envelope technique. Patients in group A were treated with laser lithotripsy using the WiScope single-use digital flexible ureteroscope. Those in group B underwent laser lithotripsy with a new reusable flexible ureteroscope. All participants provided informed consent before surgical intervention.
All surgical procedures were performed by a single well-trained surgeon using laser fragmentation with the Dormia basket stone extraction technique. Patients were blinded throughout the study. For each patient, we recorded the following preoperative data: age, gender, BMI, stone characteristics, and previous stent placement.
Some data on the scope were also collected during surgery. These included vision quality during the procedure, which was assessed through a scale from 1 (poor) to 10 (very good); maneuverability, which was assessed using a scale from 1 (difficult) to 10 (excellent); and ease of insertion, which was assessed using a scale from 1 (difficult) to 10 (very easy). Any scope failure during the procedure was also recorded. In addition, the surgeon provided an overall assessment of both scopes using a Likert scale from 1 (poor) to 10 (very good) [11] (Appendix 1).
Data about each procedure were collected as well. These included the placement of the ureteral access sheath, the amount of laser energy used through the 272-laser fiber, operative time, blood loss, and any intraoperative complications, including but not limited to ureteral avulsion, perforation, and bleeding. Postoperative complications were classified according to Clavien–Dindo classification.
Patients were evaluated for postoperative UTIs using a urine analysis, white blood cell counts, body temperature, and urine cultures. Patients were evaluated 1 week after surgery and again 4 weeks after surgery. All patients underwent post-operative imaging studies 1 month after surgery to assess whether they were free of stones. Patients with radio opaque stones were assessed with KUB X-rays and patients with radiolucent or poor radiopaque stones were evaluated with CT KUBs. Stone-free status is defined as the absence of fragments larger than 4 mm 30 days after surgery. The number of sessions required for complete stone fragmentation was also recorded.
The WiScope (OTU Medical Inc.) ureteroscope
The WiScope single-use digital flexible ureteroscope is a sterile, single-use scope composed of two parts: a flexible insertion tube and a control body with articulation controls, accessory access ports, and a cable (Fig. 1). Four models of the WiScope single-use digital flexible ureteroscope are available. These are the standard deflection left-handed model (OTU-100SL), the standard deflection right-handed model (OTU-100SR), the reverse deflection left-handed model (OTU-100RL), and the reverse deflection right-handed model (OTU-100RR). The WiScope has a maximum outer diameter of 9.5 Fr (3.25 mm), a working shaft length of 670 mm, a 7.4 French distal tip diameter, and a 3.6 French working channel. It provides a 100° field of view that is 2–50 mm deep and offers 275 bidirectional active defection.
The Flex-Xc reusable flexible ureteroscope
The reusable ureteroscope used in our study is the Flex-Xc ureteroscope made by Karl Storz SE and Co. KG, Tuttlingen, Germany. This ureteroscope has led technology, a maximum deflection of 270 in both directions, and a sheath circumference of 8.5 French with complementary metal oxide semiconductors (CMOS) chip technology.
Operative procedure
All procedures were performed under general anesthesia. Two grams of cefazolin were administered during anesthesia induction. Patients were placed in the lithotomy position, and a diagnostic cystoscopy was performed. A ureteric catheter size 5 French was advanced in the ureteric orifice, and a retrograde pyelogram was done. Next, a sensor guide wire (0.038 mm) was inserted to the kidney under fluoroscopic guidance. A 12/14 Fr or 10/12 Fr Coloplast Retrace® access sheath was then advanced over the sensor wire until it reached a satisfactory position in the ureter. In case of failure to advance the ureteral access sheath, a JJ stent was placed for 2 weeks and the patient was retaken to the operative theater to complete the procedure.
The flexible ureteroscope was introduced to the kidney through the ureteral access sheath. The entire collecting system was visualized before stone fragmentation. Stone fragmentation was done using a Holmium:YAG laser with a fiber size of 272 um. The energy settings were 800–1200 mJ per pulse with a frequency of 8–10 Hz. The stone fragments were then removed using the Dormia basket stone extraction technique. The flexible ureteroscope and the sheath were smoothly withdrawn from the ureter. Finally, a 6 Fr JJ stent was placed under fluoroscopic guidance.
Sample size calculation
Before the study, the minimum number of patients in each group was determined based on a power calculation using the data from the pilot study. In that study, the mean performance satisfaction score for group A was 8.1 ± 1.48; for group B it was 7.6 ± 1.27. It was then determined that a sample size of 121 patients in each group would provide 80% power for independent samples t-tests at a significance level of P ≤ 0.05. The power calculation was conducted using G Power 3.1 9.2 software.
Statistical methods
The collected data were coded, tabulated, and statistically analyzed using the Statistical Package for Social Sciences (SPSS) software version 25. Descriptive statistics were calculated for parametric (normally distributed) quantitative data, including the mean, standard deviation (SD), and minimum and maximum range. For non-parametric quantitative data, the median and interquartile range (IQR) were calculated. For qualitative data, the frequency and percentage were calculated. Data distribution was evaluated using the Kolmogorov–Smirnov test.
For parametric quantitative data, the groups were compared using independent samples t-tests. For non-parametric quantitative data, a Mann–Whitney U test was used to compare groups. Analyses were done between the two times for non-parametric quantitative data using the Wilcoxon Signed test. For qualitative data, the two groups were compared using a chi squared test (if up to 20% of the cells had an expected count of less than five) or Fisher’s exact test (if more than 20% of the cells had an expected count of more than five). Significance was set to P ≤ 0.05.
Results
A total of 242 patients who presented with renal stones and met the inclusion criteria were included in our study. Patients were randomly assigned to one of two groups. Group A included 121 patient who underwent retrograde FURS using the WiScope single-use digital flexible ureteroscope. Group B included 121 patients who underwent retrograde FURS using a standard reusable digital flexible ureteroscope. There were no significant differences in patient demographics or stone characteristics between the two groups (Table 1).
The rate of preoperative stenting in the two groups was similar (40.5% vs. 37.2%). In both groups, laser lithotripsy was performed using a 272 um fiber. Laser stone fragmentation was conducted using the Dormia basket stone extraction technique for all patients. The mean laser energy for group A was 955.4 ± 195.8 mJ; the mean laser frequency for group A was 8.8 ± 1 Hz. For group B, the mean laser energy was 955.4 ± 195.8 mJ, and the mean laser frequency was 8.8 ± 1 Hz (Table 1). The groups did not differ significantly in respect to operative time, laser time, laser frequency, or laser energy used. Post-operative evaluation of residual stones was done either by X ray KUB [11 patients (9%) in group A, 9 patients (7.5%) in group B] or by CT KUB for the rest of the patients in both groups. There were also no significant differences in success rates or in the need for additional sessions after the first procedure (Table 1).
The mean maneuverability score of the WiScope was higher than that of the reusable ureteroscope (9.3 ± 0.7 vs. 7.2 ± 0.8). The WiScope was also rated better than the reusable ureteroscope regarding wrist and thumb fatigue (P = 0.001). The reusable ureteroscope offered better visual acuity than the WiScope (9.2 ± 0.6 vs. 7.6 ± 0.9). There was no significant difference in pre- or post-operative scope deflection malfunction. No perioperative breakage occurred with the single-use ureteroscope during this study. Performance satisfaction with the single-use WiScope ureteroscope was comparable to that with the standard reusable digital flexible ureteroscope. The median preoperative WBCS counts for the two groups were similar; however, postoperative WBCS was higher in group B than in group A (P = 0.003) (Table 2).
Discussion
Bagley and Rittenberg were the first authors to describe the use of flexible ureteroscopes in clinical practice for treating urinary stones [12]. Flexible ureteroscopy has become more popular over time; in some countries, it has been reported to be superior to shockwave lithotripsy [13]. A range of fiberoptic and digital flexible ureteroscopes are available on the market. Fiberoptic ureteroscopes offer poorer image quality than digital ones [14]. While this technology has advanced, the limited durability and high costs of reusable flexible ureteroscopes limit their use worldwide [15]. Several factors affect the durability of ureteroscopes, including the location and size of the stone, the duration of use, the use of other devices, the surgeon’s experience, and sterilization methods [16]. Legmate et al. [17] reported that a flexible endoscope can be used 27 times; after this, shaft damage is common. However, Abraham et al. [18] found that sterilization techniques are the primary cause of damage to flexible ureteroscopes.
In our study, we used two new Flex-Xc digital flexible ureteroscopes to complete 121 procedures. After the first 49 procedures, the first scope underwent a mechanical failure; the scope was unable to pass the laser fiber. The scope was sent for repair, and we continued the study with a second new ureteroscope. After the first scope was repaired, we reused it to complete the study. Because the Flex-Xc ureteroscope is expensive, we used several precautions to increase the lifespan of the ureteroscope, including careful and correct manipulation, proper storage and cleaning, use of a ureteral access sheath, relocating the lower calyceal stone, avoiding prolonged use, and avoiding overstressing the deflection mechanism.
Reusable endoscopes are also associated with a risk of infection. Ofstead et al. [19] reported a 100% risk of contamination with such scopes. Chang et al. [7] reported an outbreak of urinary tract infections associated with a contaminated ureteroscope. To address this issue, single-use digital flexible ureteroscopes have been developed. These scopes offer several benefits, including excellent maneuverability, high-quality imaging, access to the entire collecting system, adequate active deflection, and good irrigation flow [15, 20, 21].
A number of single-use flexible ureteroscopes have been developed over the last few years, including the Maxiflex and Polyscope [22]. LithoVue™ was the first single-use digital flexible ureteroscope to be compared to standard reusable flexible ureteroscopes in laboratory and clinical settings. However, its widespread use has been limited by its high costs, as established by a cost–benefit analysis done by Martin et al. [8] who concluded that reusable scopes were preferable to the LithoVue scope.
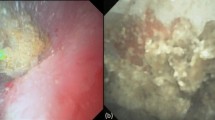
A ureteroscope’s optical properties are crucial, as clear visibility is necessary during intrarenal procedures. Poor visibility contributes to impaired diagnosis and poorer outcomes after treatment of kidney stones [23]. Our study found a significant difference between the image quality and maneuverability of single-use and reusable digital FURS. The WiScope offered better maneuverability and reduced limb fatigue, but its image quality was poorer than that of the reusable FURS. JK also found that a reusable FURS offered better image quality than single-use FURS [24], which aligns with previous studies [25,26,27].
Similarly, Qi et al. [28] found that a single-use FURS offers better maneuverability than a reusable one, which also explains the higher stone-free rate with the single-use FURS. Several studies have concluded that the image quality and maneuverability of the LithoVue scope are comparable to that of a reusable FURS [15, 29].
During intrarenal procedures, the deflection of a flexible ureteroscope plays a critical role in access to the renal calyces, especially when lower pole calculi are present [15, 30]. We found that the deflection ability of the WiScope single-use digital flexible ureteroscope was comparable to that of the reusable one, and both scopes maintained deflection when moving up and down directions. Wiseman et al. [31] found that the LithoVue could access all calyces and maintained 270° deflection when moving up and down directions.
In our study, operative time, laser characteristics, and perioperative complications for the two groups were similar. We also found no significant differences in success rates or rates of second look Similarly, Usawachintachit et al. [32] found that the LithoVue had comparable outcomes and complication rates to those of reusable flexible ureteroscopes. A randomized controlled trial by Ding et al. [33] also found that the Polyscope™ had similar stone clearance rates to a reusable ureteroscope.
Our study showed that the overall clinical performance of the WiScope single-use digital flexible ureteroscope approaches that of a reusable scope. Several previous studies have found that the clinical performance of the LithoVue is similar to that of reusable ureteroscopes [32, 34, 35]. A recent study found that stone-free rates after procedures performed using the Uscope mirrored those of reusable ureteroscopes [30].
In present study, post-operative WBCs count was higher in group B than group A; however, the difference was not clinically significant. Two patients in group B developed post-operative UTI symptoms with positive urine culture and sensitivity test results. Both patients were treated by antibiotics (Grade 2 according to Clavien–Dindo classification).
Cost plays a considerable role in the decision to purchase a reusable or single-use flexible ureteroscope. The acquisition cost of reusable flexible ureteroscopes is a considerable barrier to adoption of this device. Moreover, the total costs of reusable flexible ureteroscopes are not limited to the purchase price; there is also a cost associated with the technicians who process and sterilize the scopes after use, as well as repair costs [36].
The acquisition costs and effectiveness of the single-use flexible ureteroscope are the main questions related to this device. Acquisition costs vary locally and nationally; high-volume centers may be able to buy these scopes at significantly lower prices than low-volume centers. Given the complexity of the cost parameters, we have limited our study to evaluating the efficacy of this single-use flexible ureteroscope. Further studies comparing the global cost effectiveness of the WiScope ureteroscope and reusable ureteroscopes are recommended.
Our study has shown that the WiScope single-use digital flexible ureteroscope performed very well intraoperatively in terms of maneuverability, limb fatigue, and active deflection. This tool shows promise for the endoscopic treatment of urinary calculi.
Conclusion
The WiScope is a new single-use digital flexible ureteroscope. Its clinical performance and surgical outcomes are comparable to those of a reusable flexible ureteroscope. The WiScope flexible ureteroscope offers good maneuverability, low limb fatigue, and good deflection angles. It appears to be a good alternative to reusable flexible ureteroscopes due to its low cost, especially for treating challenging lower pole calculi, which pose a high risk of scope damage.

WiScope® single-use digital flexible ureteroscope
Abbreviations
- FURS:
-
Flexible ureteroscope
- CT:
-
Computed tomography
- KUB:
-
Kidney, ureter, bladder
References
Türk C et al (2016) EAU guidelines on diagnosis and conservative management of urolithiasis. Eur Urol 69(3):468–474
Fuchs G (2006) Milestones in endoscope design for minimally invasive urologic surgery: the sentinel role of a pioneer. Surg Endosc Other Interv Tech 20(2):S493–S499
Marshall VF (1964) Fiber optics in urology. J Urol 91(1):110–114
Ordon M et al (2015) A population based study of the changing demographics of patients undergoing definitive treatment for kidney stone disease. J Urol 193(3):869–874
Turney BW et al (2011) Trends in urological stone disease. BJU Int 109(7):1082–1087
Monga M et al (2006) Durability of flexible ureteroscopes: a randomized, prospective study. J Urol 176(1):137–141
Chang C-L et al (2013) Outbreak of ertapenem-resistant Enterobacter cloacae urinary tract infections due to a contaminated ureteroscope. J Hosp Infect 85(2):118–124
Martin CJ et al (2017) The economic implications of a reusable flexible digital ureteroscope: a cost-benefit analysis. J Urol 197(3):730–735
Taguchi K et al (2018) Micro-costing analysis demonstrates comparable costs for LithoVue compared to reusable flexible fiberoptic ureteroscopes. J Endourol 32(4):267–273
Hennessey DB et al (2018) Single-use disposable digital flexible ureteroscopes: an ex vivo assessment and cost analysis. BJU Int 121(3):55–61
Johnston TJ et al (2018) A clinical evaluation of the new digital single-use flexible ureteroscope (UscopePU3022): an international prospective multicentered study. Cent European J Urol 71(4):453
Bagley DH, Rittenberg MH (1986) Percutaneous antegrade flexible ureteroscopy. Urology 27(4):331–334
Ordon M et al (2014) The surgical management of kidney stone disease: a population based time series analysis. J Urol 192(5):1450–1456
Lusch A et al (2013) In vitro and in vivo comparison of optics and performance of a distal sensor ureteroscope versus a standard fiberoptic ureteroscope. J Endourol 27(7):896–902
Proietti S et al (2016) Comparison of new single-use digital flexible ureteroscope versus nondisposable fiber optic and digital ureteroscope in a cadaveric model. J Endourol 30(6):655–659
Carey RI, Martin CJ, Knego JR (2014) Prospective evaluation of refurbished flexible ureteroscope durability seen in a large public tertiary care center with multiple surgeons. Urology 84(1):42–45
Legemate JD et al (2019) Durability of flexible ureteroscopes: a prospective evaluation of longevity, the factors that affect it, and damage mechanisms. Eur Urol Focus 5(6):1105–1111
Abraham JBA (2007) Effects of Steris 1^< TM> sterilization and Cidex (! R) orthophthaldehyde high-level disinfection on durability of new-generation flexible ureteroscopes. J Endourol 21:985–992
Ofstead CL et al (2017) The effectiveness of sterilization for flexible ureteroscopes: a real-world study. Am J Infect Control 45(8):888–895
Emiliani E, Traxer O (2017) Single use and disposable flexible ureteroscopes. Curr Opin Urol 27(2):176–181
Traxer O (2008) Flexible ureterorenoscopic management of lower-pole stone: does the scope make the difference? J Endourol 22(9):1847–1850
Gu S-P et al (2013) Clinical effectiveness of the PolyScope™ endoscope system combined with holmium laser lithotripsy in the treatment of upper urinary calculi with a diameter of less than 2 cm. Exp Ther Med 6(2):591–595
Clayman RV (2005) A novel dual-diameter ureteroscope working channel: impact on irrigant flow. J Urol 174(1):173–173
Kam J et al (2019) Single use versus reusable digital flexible ureteroscopes: a prospective comparative study. Int J Urol 26(10):999–1005
Deininger S et al (2018) Single-use versus reusable ureterorenoscopes for retrograde intrarenal surgery (RIRS): systematic comparative analysis of physical and optical properties in three different devices. World J Urol 36(12):2059–2063
Bell JR et al (2017) Prospective evaluation of flexible ureteroscopes with a novel evaluation tool. Can J Urol 24(5):9004–9010
Doizi S et al (2017) First clinical evaluation of a new single-use flexible ureteroscope (LithoVue™): a European prospective multicentric feasibility study. World J Urol 35(5):809–818
Qi S et al (2020) Single-use versus reusable digital flexible ureteroscopes for the treatment of renal calculi: a prospective multicenter randomized controlled trial. J Endourol 34(1):18–24
Xu K et al (2018) Flexible ureteroscopic holmium laser lithotripsy with PolyScope for senile patients with renal calculi. Exp Ther Med 16(3):1723–1728
Salvadó JA et al (2018) Retrograde intrarenal surgery using the single–use flexible ureteroscope Uscope 3022 (Pusen™): evaluation of clinical results. Cent European J Urol 71(2):202
Wiseman O et al. (2016) V76 A single-use disposable digital flexible ureteroscope (Lithovue™) compared to a non-disposable fibre-optic flexible ureteroscope in a live porcine model. Eur Urol Suppl 3(15): p. eV76.
Usawachintachit M et al (2017) A prospective case–control study comparing LithoVue, a single-use, flexible disposable ureteroscope, with flexible, reusable fiber-optic ureteroscopes. J Endourol 31(5):468–475
Ding J et al (2015) Comparing the efficacy of a multimodular flexible ureteroscope with its conventional counterpart in the management of renal stones. Urology 86(2):224–229
Cho SY et al (2018) Evaluation of performance parameters of the disposable flexible ureterorenoscope (LITHOVUE) in patients with renal stones: a prospective, observational, single-arm, multicenter study. Sci Rep 8(1):1–6
Mager R et al (2018) Clinical outcomes and costs of reusable and single-use flexible ureterorenoscopes: a prospective cohort study. Urolithiasis 46(6):587–593
Marchini GS et al (2019) A comprehensive literature-based equation to compare cost-effectiveness of a flexible ureteroscopy program with single-use versus reusable devices. Int Braz J Urol 45:658–670
Author information
Authors and Affiliations
Contributions
AA: project development, protocol writing, manuscript writing and editing; AE: manuscript writing; AA: data analysis; MR: data collection; ME: manuscript editing; AH: manuscript writing.
Corresponding author
Ethics declarations
Conflict of Interest
None.
Ethical approval
All procedures performed in the study involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki Declaration and its later amendments. The study was approved by the Bioethical Committee of Port Saied University ( ERN:MED SO. (24) SPS/URS).
Informed consent
Informed consent was obtained from all research participants.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendices
Appendix 1:
Maneuverability during the procedure
1: poor / difficult, 10: excellent, easy.
1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
Quality of Vision during the procedure
1: poor, 10: very good.
1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
Overall assessment
1: poor, 10: very good.
1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
Rights and permissions
About this article

Cite this article
Ali, A.I., Eldakhakhny, A., Abdelfadel, A. et al. WiScope® single use digital flexible ureteroscope versus reusable flexible ureteroscope for management of renal stones: a prospective randomized study. World J Urol 40, 2323–2330 (2022). https://doi.org/10.1007/s00345-022-04095-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00345-022-04095-z