
Abstract
Purpose
Data assessing the effectiveness of single-use flexible ureteropyeloscopy (FURS) are limited. This study evaluates and compares single-use FURS with conventional reusable FURS.
Methods
A systematic search using electronic databases (Pubmed and Embase) was performed for studies evaluating single-use FURS in the setting of urinary tract stone disease. Outcome measures included a comparative evaluation of their mechanical, optical and clinical outcomes.
Results
Eleven studies on 466 patients met inclusion criteria. In vitro comparative data were available on three single-use flexible ureteropyeloscopes (LithoVue™, Polyscope™ and SemiFlex™) and clinical data were available on two (LithoVue™ and Polyscope™). The overall stone-free rate and complication rate associated with single-use FURS was 87 ± 15% and 9.3 ± 9%, respectively. There were no significant differences in procedure duration, stone size, stone clearance and complication rates when single-use FURS and reusable FURS were compared (duration: 73 ± 27 versus 74 ± 13 min, p = 0.99; stone size: 1.36 ± 0.2 versus 1.34 ± 0.18 cm, p = 0.93; stone-free rate: 77.8 ± 18 versus 68.5 ± 33%, p = 0.76; complication rate 15.3 ± 10.6 versus 15 ± 1.6%, p = 0.3).
Conclusions
Single-use FURS demonstrates comparable efficacy with reusable FURS in treating renal calculi. Further studies on clinical efficacy and cost are needed to determine whether single-use FURS will reliably replace its reusable counterpart.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The first description of the conventional flexible ureteroscope was provided by Marshall in 1964 [1]. Limitations with this model included the absence of a working channel and restrictions with active deflection. The technique was refined more than 20 years later when Bagley pioneered the disposable flexible ureteroscope for accessing the upper urinary tracts [2]. The rationale behind the disposable flexible ureteroscope was to counterbalance significant costs that were associated with repair and sterilisation of conventional flexible ureteroscopes with a reliable, cost-effective, user-friendly, single-use alternative [3].
Innovative technical progression in this evolving field of endourology is reflected by the variety of single-use flexible ureteroscopes that are commercially available [3,4,5]. Despite the progression of single-use FURS into urological clinical practice, robust comparative data assessing technological design and clinical efficacy are lacking. The aim of this systematic review is to comparatively evaluate the mechanical, optical and clinical outcomes of single-use FURS with conventional reusable FURS for the treatment of stone disease in patients.
Methods
Overview of literature search
A systematic literature search was performed using Pubmed and Embase databases to identify original peer-reviewed articles that studied outcomes of single-use flexible ureteropyeloscopy for the evaluation and treatment of urinary tract calculi. The search was conducted using the following search algorithm: ‘ureteroscopy’ or ‘pyeloscopy or ‘ureteropyeloscopy’ and ‘single use’ and “flexible scope”. Two authors (NFD and MQ) independently examined the title and abstract of citations and the full texts of potentially eligible trials were obtained; disagreements were resolved by discussion. The reference lists of retrieved papers were further screened for additional eligible publications. If a patient group was reported twice, the most recent paper was chosen. If data were unclear or incomplete, the corresponding author was contacted to clarify data extraction. Institutional review board was not sought as this study was a systematic review. Case reports were excluded and the latest literature search was performed on the 1st of August 2017.
Eligibility criteria
Studies with in vitro (i.e. benchtop), animal, cadaveric and in vivo data on single-use FURS were included. In addition, comparative studies between single-use flexible ureteropyeloscopes and conventional (i.e. non-disposable) flexible ureteropyeloscopes were included to assess and compare mechanical, optical and clinical outcomes. The primary endpoint was to comparatively evaluate the efficacy of single-use FURS. Clinical efficacy was defined as the percentage of patients that were stone-free after treatment on imaging at follow-up. Exclusion criteria included single-use FURS without any published in vitro or in vivo data.
Data extraction and outcomes
The following information regarding each eligible study was recorded: author’s name, journal of publication, year of publication, country of origin, study type and total number of patients. Recorded data relating to FURS included type of single-use flexible ureteropyeloscope used, cost of scope, mechanical, irrigation and optical parameters, mean stone size, duration of surgery, stone-free rate at follow-up and imaging modality used to determine stone-free rate. Results for variables are reported as percentages based on the number of cases that had relevant data available. Data are presented as a mean ± standard deviation. Student’s t-tests with unequal variances were performed for pairwise comparisons. Differences were considered significant at p < 0.05 (SPSS 16.0 for Windows).
Results
Eligible studies
The search was performed based on the PRISMA statement [6]. Eleven studies published between 2009 and July 2017 that met inclusion criteria were retrieved. The initial search identified 234 articles and 80 full-text studies were assessed for eligibility; 54 of which were excluded (Fig. 1). These studies were excluded as they did not contain mechanical, optical or clinical data on single-use flexible ureteropyeloscopy. Included studies were reflective of modern clinical practice and are summarised in Table 1. The studies consisted of one randomised controlled trial [7], three single-centre prospective studies [8,9,10], two multi-institutional prospective studies [11, 12], one cadaveric feasibility study [13], one porcine feasibility study [14] and three comparative benchtop studies [5, 15, 16]. Data were available on LithoVue™, Polyscope™ and SemiFlex™ single-use flexible ureteropyeloscopes. As only one randomised controlled trial was retrieved and due to the heterogeneous nature of the available literature, a formal meta-analysis was not conducted [7].

Preferred reporting items in systematic reviews and meta-analyses (PRISMA) diagram [6]
Mechanical, optical and irrigation properties
Characteristics of single-use flexible ureteropyeloscopes are summarised and compared in Table 2. Seven studies that assessed and/or compared mechanical, optical and/or irrigation characteristics met inclusion criteria and were included in the analysis [5, 10, 12,13,14,15,16]. The LithoVueTM has a 7.7Fr operating tip diameter, 3.6Fr working channel and costs approximately $1500 US dollars [17]. It also has a 270° bidirectional deflection tip, a mean irrigation rate of 40 ml/min and the ureteroscope working length is 68 cm [3, 18]. Deflection and flow-rate do not decrease when endoscopic tools are applied [19]. In comparison, the PolyscopeTM has an 8Fr operating tip diameter, 3.6Fr working channel and costs approximately $700 US dollars [20]. It has a 180° unidirectional deflection tip, mean irrigation rate of 57 ml/min and the ureteroscope working length is 70 cm [3]. Deflection and flow-rate decrease by 10 and 50–68%, respectively, with application of endoscopic tools [3]. The SemiFlexTM scope has a 6.3Fr working channel operating tip diameter, 3.3Fr working channel and costs approximately $800 US dollars [5]. It has a 300°/265° bidirectional down/up deflection tip, mean irrigation rate of 25 ml/min and the ureteroscope working length is 65 cm. Deflection and flow-rate decrease with endoscopic tools by 35–39 and 51–65%, respectively [3, 5].
Clinical outcomes
Six studies on 466 patients described clinical outcomes on single-use FURS for the treatment of stone disease (Table 3) [6,7,8,9,10,11]. Four studies evaluated the clinical effectiveness of the PolyscopeTM [7,8,9,10] and two studies assess clinical outcomes with LithoVueTM [11, 12]. No published clinical data were available on the SemiFlexTM scope. In these studies, operative duration was 66 ± 29 min with a stone size of 1.13 ± 0.26 cm. The stone-free rate postoperatively was 87 ± 15% and complications occurred in 9.3 ± 9% of patients. There were no significant differences in procedure duration, stone size and stone-free rates when data on PolyscopeTM and LithovueTM were compared (duration: 78 ± 32 min versus 47 ± 10 min, p = 0.29; stone size: 1.05 ± 0.27 cm versus 1.28 ± 0.34 cm, p = 0.37; stone-free rate: 90 ± 6.4 versus 80 ± 28%, p = 0.46, respectively).
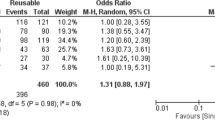
Two studies prospectively compared clinical outcomes of single-use FURS with reusable FURS [6, 10]. In these studies, the mean procedure duration was 73 ± 27 versus 74 ± 13 min (p = 0.99), the mean stone size was 1.36 ± 0.2 versus 1.34 ± 0.18 cm (p = 0.93), the complication rate was 15.3 ± 10.6 versus 15 ± 1.6% (p = 0.3) and the stone-free rate postoperatively was 77.8 ± 18 versus 68.5 ± 33%. (p = 0.76) for single-use and reusable FURS, respectively.
Discussion
We investigated and compared the mechanical, optical and irrigation properties of single-use FURS for the treatment of renal calculi. We also compared the clinical effectiveness of different commercially available single-use flexible ureteropyeloscopes with each other and with reusable flexible ureteropyeloscopes. The main findings were that in vitro, porcine and/or cadaveric data were available on LithoVue™, Polyscope™ and SemiFlex™ single-use flexible ureteropyeloscopes. Clinical data on patients undergoing treatment for stone disease was available with LithoVue™ and Polyscope™ single-use flexible ureteroscopes. When the clinical efficacy of both scopes was analysed, the single-use devices performed well when complication rates and stone-free rates were compared. These findings suggest that new disposable FURS are non-inferior to reusable FURS in terms of clinical outcomes.
The SemiFlex™ single-use flexible ureteroscope was initially described in 2009 and its basic components include a semi-flexible shaft, bidirectional deflection and with a 3.3Fr working channel [5]. Its mechanical, optical and irrigation characteristics were evaluated in vitro and were found to be similar to conventional fibreoptic reusable flexible ureteroscopes. However, no in vivo evaluation has been performed and the scope is not used in clinical practice. The PolyScope™ single-use flexible ureteroscope was developed shortly after the SemiFlex™ scope [9, 10]. The PolyScope™ is fibreoptic and composed of a single-use flexible catheter. It has a modular design to facilitate the reparation or disposal of individual components and the scope contains 10,000-pixel fibreoptic bundles. Its optical fibre bundle appears durable after 100 cycles of sterilisation [16]. An important limitation of the PolyScope™ is its unidirectional deflection up to 180°. Despite limited manoeuvrability, Ding et al. noted similar outcomes when the PolyScope™ was compared to the Olympus URF-P5 FURS for the treatment of renal stones except for lower pole stones [7]. The authors attribute this inferiority to several factors. The degree of deflection of the PolyScopeTM is regulated by the force to squeeze the handle constantly, so fingers become tired during prolonged operation in the lower calyces [7]. The PolyScopeTM only possesses a unidirectional active primary deflection mechanism. This limitation with manoeuvrability is negated by rotating the shaft by hand and upper arm movements while squeezing the handle by fingers simultaneously. Increased physical activity for the operator increases the difficulty level of the operation and leads to loss of navigation control which can lead to withdrawal of the scope for realignment purposes [7]. It is, therefore, arguable that the PolyScopeTM might not be suitable for treating lower pole stones among novice endourologists. LithoVue™ is a single-use digital flexible ureteroscope that was initially trialled in Europe in 2015 and in the United States in 2016 with the aim of mitigating costs associated with reusable flexible ureteroscopes [19]. Benchtop, porcine and cadaveric studies demonstrated that LithoVue™ is not inferior to reusable flexible ureteroscopes when image quality, manoeuvrability and ‘user-friendliness’ were compared [12,13,14,15].
Single-use flexible ureteropyeloscopes should demonstrate characteristics that make them favourable to the operator. Ideally, they should deliver optimal image quality, good irrigation, bidirectional manoeuvrability for accessing difficult calyces and have a relatively small operating tip diameter. Furthermore, they should exhibit minimal decreases in flow-rates and deflection with the administration of endoscopic tools as demonstrated by the LithoVueTM in benchtop, porcine, cadaver and in vivo studies [13, 15]. Their handles should be ergonomically user-friendly to allow for torque and easy handling and they should be financially feasible among urological departments. From a clinical perspective, disposable flexible ureteroscopes should demonstrate comparable perioperative complication rates and postoperative stone-free rates. One recent multi-institutional, prospective, comparative study by Usawachintachit et al. compared procedural outcomes between LithoVue™ and reusable ureteroscopes [11]. The authors found that the Lithovue™ was associated with a short learning curve and had comparable procedural outcomes and complication rates when compared with reusable flexible ureteropyeloscopes [11]. A randomised controlled trial by Ding et al. found that the PolyscopeTM performed well with similar overall stone clearance rates to a reusable flexible ureteropyeloscope for renal calculi < 3 cm in diameter. Notably, the URF-P5 reusable scope had better results with lower pole stones with a shorter operating time [7].
Recurring concern over durability and reparation costs associated with reusable flexible ureteropyeloscopes led to the initial development and evaluation of the disposable ureteroscope [21]. Risk factors that adversely affect reusable scope durability include cleaning techniques, surgeon experience and complexity of endourological procedures performed [22,23,24]. Reusable ureteroscopes undergo multiple reprocessing steps such as precleaning, leakage testing, formal cleaning, disinfection and/or sterilisation, drying and storage after each use [25]. Muggeo et al. investigated the costs of two reprocessing techniques by comparing low temperature sterilisation with high level disinfection. The costs ranged from $728.24 to $1294.14 per use and these findings emphasise the additional financial burden of labour-intensive reprocessing protocols [26].
Financing reusable flexible ureteroscopes is also dependent on the number of uses before repair, the initial purchasing cost and the reprocessing costs [27,28,29]. Costs of single-use flexible scopes appear to vary worldwide, and this should be considered by urology departments when performing a comparative cost–benefit analysis with reusable scopes. [5, 17, 20]. Martin et al. assessed the economic implications of reusable flexible ureteroscopes by performing a cost–benefit analysis on all flexible ureteroscopies performed over a 12-month period using Flex XC digital ureteroscopes and the potential costs of the LithoVueTM [30]. In total, 160 flexible ureteroscopies were performed with damage occurring in eight reusable scopes. The analysis demonstrated a cost of $848.10 per use and favoured reusable ureteroscopes after 99 procedures were performed. The authors conclude by suggesting that high-volume institutions (i.e. > 99 FURS/year) may find reusable ureteroscopes more cost beneficial and that disposable flexible ureteroscopes are cost beneficial in lower-volume centres.
A limitation with the present systematic review is that the number of studies was relatively small due to the lack of comparative data on single-use and conventional FURS. Also, the data was heterogenous and only one randomised controlled trial was retrieved thereby preventing the feasibility for a formal meta-analysis. To address this limitation, we advocate additional randomised controlled trials in the near future to compare clinical outcomes and cost–benefits of reusable FURS with single-use FURS [29, 31, 32]. Such studies would be beneficial in definitively determining whether single-use FURS are truly equivalent to its reusable counterpart.
Conclusion
Single-use FURS demonstrates comparable efficacy with reusable FURS in treating renal calculi as no statistically significant differences in perioperative complication rates and stone-free rates were found. Their selective usage in low-volume endourological centres may limit the costs associated with repairing reusable flexible ureteropyeloscopes. Further detailed evaluation of clinical outcomes and cost-benefit analyses in the form of randomised controlled trials will determine whether single-use FURS can reliably establish its position in daily endourological practice.
Abbreviations
- FURS:
-
Flexible ureteropyeloscopy
References
Marshall VF (1964) Fiber optics in urology. J Urol 91(1):110–114
Bagley DH (1987) Flexible ureteropyeloscopy with modular, “disposable” endoscope. Urology 29(3):296–300
Emiliani E, Traxer O (2017) Single use and disposable flexible ureteroscopes. Curr Opin Urol 27(2):176–181
Doizi S, Traxer O (2017) Re: Evaluation of a novel single-use flexible ureteroscope. Eur Urol 72(1):152–153
Boylu U, Oommen M, Thomas R, Lee BR (2009) In vitro comparison of a disposable flexible ureteroscope and conventional flexible ureteroscopes. J Urol 182(5):2347–2351
Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 6(7):e1000097. https://doi.org/10.1371/journal.pmed.1000097
Ding J, Xu D, Cao Q, Huang T, Zhu Y, Huang K et al (2015) Comparing the efficacy of a multimodular flexible ureteroscope with its conventional counterpart in the management of renal stones. Urology 86(2):224–229
Huang Y-T (2013) Clinical effectiveness of the PolyScopeTM endoscope system combined with holmium laser lithotripsy in the treatment of upper urinary calculi with a diameter of less than 2 cm. Exp Ther Med 6(2):591–595
Bansal H, Swain S, Sharma GK, Mathanya M, Trivedi S, Dwivedi US et al (2011) Polyscope: a new era in flexible ureterorenoscopy. J Endourol 25(2):317–321
Bader MJ, Gratzke C, Walther S, Schlenker B, Tilki D, Hocaoglu Y et al (2010) The PolyScope: a modular design, semidisposable flexible ureterorenoscope system. J Endourol 24(7):1061–1066
Usawachintachit M, Isaacson DS, Taguchi K, Tzou DT, Hsi RS, Sherer BA et al (2017) A prospective case–control study comparing LithoVue, a single-use, flexible disposable ureteroscope, with flexible, reusable fiber-optic ureteroscopes. J Endourol 31(5):468–475
Doizi S, Kamphuis G, Giusti G, Andreassen KH, Knoll T, Osther PJ et al (2017) First clinical evaluation of a new single-use flexible ureteroscope (LithoVueTM): a European prospective multicentric feasibility study. World J Urol 35(5):809–818
Proietti S, Dragos L, Molina W, Doizi S, Giusti G, Traxer O (2016) Comparison of new single-use digital flexible ureteroscope versus nondisposable fiber optic and digital ureteroscope in a cadaveric model. J Endourol 30(6):655–659
Wiseman O, Keeley F, Traxer O, Giusti G, Lipkin M, Preminger G (2016) Comparison of a new single-use digital flexible ureteroscope (LithoVue) to a non-disposable fibre-optic flexible ureteroscope in a live porcine model. J Urol 195(4):e682
Dale J, Kaplan AG, Radvak D, Shin R, Ackerman A, Chen T, et al (2017) Evaluation of a novel single-use flexible ureteroscope. J Endourol. https://doi.org/10.1089/end.2016.0237
Johnson MT, Khemees T a, Knudsen BE. Resilience of disposable endoscope optical fiber properties after repeat sterilization. J Endourol. 2013;27(1):71–4
Ghodoussipour S, Thompson E, Shah A, Mitra A, Deshmukh S, Dunn M (2017) Mp50-08 Limitations of the lithovue single use digital flexible ureteroscope. J Urol 197(4):e686–e687
Doersch K, Elmekresh A, Milburn PA, Machen G, Hart K, El Tayeb M (2017) Pd35-08 Utilization of pressurized vs non-pressurized irrigation during ureteroscopy in the absence of ureteral access sheath: comparative retrospective study. J Urol 197(4):e665–e666
Buttice S, Sener TE, Netsch C, Emiliani E, Pappalardo R, Magno C (2016) LithoVueTM: a new single-use digital flexible ureteroscope. Cent Eur J Urol 69(3):302–305
Siu JJ-Y, Chen H-Y, Liao P-C, Chiang J-H, Chang C-H, Chen Y-H et al (2016) The cost-effectiveness of treatment modalities for ureteral stones. Inq J Heal Care Organ Provis Financ 53(91):4695801666901
Pietrow PK, Auge BK, Delvecchio FC, Silverstein AD, Weizer AZ, Albala DM et al (2002) Techniques to maximize flexible ureteroscope longevity. Urology 60(5):784–788
Carey RI, Gomez CS, Maurici G, Lynne CM, Leveillee RJ, Bird VG (2006) Frequency of ureteroscope damage seen at a tertiary care center. J Urol 176(2):607–610
Defidio L, De Dominicis M, Di Gianfrancesco L, Fuchs G, Patel A (2012) Improving flexible ureterorenoscope durability up to 100 procedures. J Endourol 26(10):1329–1334
Sung JC, Springhart WP, Marguet CG, L’Esperance JO, Tan YH, Albala DM et al (2005) Location and etiology of flexible and semirigid ureteroscope damage. Urology 66(5):958–963
Semins MJ, George S, Allaf ME, Matlaga BR (2009) Ureteroscope cleaning and sterilization by the urology operating room team: the effect on repair costs. J Endourol 23(6):903–905
Muggeo E, Boissel A, Martin L, Sgro C, Michiels C (2015) Cost comparison of two reprocessing procedures of flexible ureteroscopes at the University Hospital of Dijon. Prog Urol 25(6):318–324
Landman J, Lee DI, Lee C, Monga M (2003) Evaluation of overall costs of currently available small flexible ureteroscopes. Urology 62(2):218–222
Kramolowsky E, McDowell Z, Moore B, Booth B, Wood N (2016) Cost analysis of flexible ureteroscope repairs: evaluation of 655 procedures in a community-based practice. J Endourol 30(3):254–256
Ozimek T, Schneider MH, Hupe MC, Wiessmeyer JR, Cordes J, Chlosta PL, Merseburger AS, Kramer MW (2017) Retrospective cost analysis of a single-center reusable flexible ureterorenoscopy (fURS) program: a comparative cost simulation of disposable fURS as an alternative. J Endourol. https://doi.org/10.1089/end.2017.0427 (epub ahead of print)
Martin CJ, McAdams SB, Abdul-Muhsin H, Lim VM, Nunez-Nateras R, Tyson MD et al (2017) The economic implications of a reusable flexible digital ureteroscope: a cost-benefit analysis. J Urol 197(3):730–735
Grasso M, Bagley D (1998) Small diameter, actively deflectable, flexible ureteropyeloscopy. J Urol 160(5):1648–1654
Fojecki G, Hennessey D, Lawrentschuk N, Bolton D (2017) Comparison of parameters of standard reusable flexible uretero-renoscopes with a single use uretero-renoscope (LithoVueTM). J Urol 197(4):e686
Author information
Authors and Affiliations
Contributions
Niall Davis: Data collection, Data analysis, Manuscript writing; Mark Quinlan: Data collection, Data analysis, Manuscript writing; Cliodhna Browne: Data collection; Nikita Bhatt: Data collection; Rustom Manecksha: Data analysis; Frank Darcy: Data analysis; Nathan Lawrentschuk: Project development, Manuscript editing; Damien Bolton: Project development, Manuscript editing.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest.
Statement of human and animal rights
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed consent
For this type of study formal consent is not required.
Rights and permissions
About this article

Cite this article
Davis, N.F., Quinlan, M.R., Browne, C. et al. Single-use flexible ureteropyeloscopy: a systematic review. World J Urol 36, 529–536 (2018). https://doi.org/10.1007/s00345-017-2131-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00345-017-2131-4