
Abstract
Purpose
A single-use digital flexible ureteroscope (fURS) has become a cost-effective alternative option to reusable fURS. The requirement of large-diameter access sheath for passage of 9.5 Fr single-use fURS has not always achieved in the first attempt in all cases leading to stage stone clearance. Recently, two slimmest single-use digital disposable fURSs have been introduced by Bioradmedisys™ and Pusen™ to mitigate the accessibility problem, without or with small size access sheath.
Primary objective was to compare in vivo performance and surgical outcomes with two single-use fURS: 7.5Fr Indoscope (Bioradmedisys™, Pune, India) and 7.5Fr Uscope PU3033A (Pusen, Zhuhai, China).
Methods
60 patients undergoing Retrograde Intrarenal Surgery (RIRS) with < 2 cm renal stones were prospectively randomized into: Group A (30 patients) for Indoscope and Group B (30 patients) for Uscope PU3033A. Pre-operative, intra-operative, and post-operative parameters were evaluated. In vivo visibility and maneuverability were rated on 5-point Likert scale by the operating surgeon. At one-month stone clearance was assessed with ultrasound and X-ray KUB. Data were analyzed using SPSS 23.0.
Results
Patient demographics and stone characteristics were comparable in both groups. Indoscope had significantly higher visibility (p < 0.05) than Uscope; however, the maneuverability scores were comparable between both the groups (p > 0.05).
28 patients in group A and 26 patients in group B achieved complete stone clearance (p = 0.38). Scope failure was observed in 1 case of group B (p = 0.31).
Conclusion
We conclude that 7.5Fr Indoscope has better vision than 7.5Fr Uscope and the rest of in vivo performances were comparable with similar outcomes and complications among both scopes.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Several technological signs of progress have conveyed improvement in flexible ureteroscope (fURS) in terms of image quality, deflection mechanics, and miniaturization of scopes. Nowadays single-use fURS (su-fURS) are widely used, which were introduced to mitigate the drawbacks associated with reusable fURS. Many disposable digital fURS are already on the market, including LithoVue (Boston Scientific, Marlborough, MA, USA), FlexoVue (Cook Medical, Bloomington, IN, USA), PU3022A (Pusen, Zhuhai, China), Polyscope (Lumenis, Yokneam, Israel, Polydiagnost, Hallbergmoos, Germany), SemiFlex Scope (Maxiflex, Los Angeles, CA, USA), and Yc-FR-A (YouCare Tech, Wuhan, China) [1]. Several studies observed comparable in vitro characteristics concerning optics, deflection ability, and flow rate via working channel between reusable and disposable fURS [2,3,4]. The safety and efficacy of single-use fURS are also found comparable to reusable scope for the management of renal stones [5, 6]. However, the majority of available su-fURSs have outer shaft diameters beyond 9 Fr which requires the introduction of a large access sheath and sometimes needs staging of the procedure with prior double J stent placement [7, 8]. Technological advancement led to the development of thinner disposable digital fURS, outer shaft diameter of 7.5 Fr, without compromising working channel diameter which attenuated the accessibility problem associated with large-diameter fURS [9].
The primary objective was to compare in vivo comparison between the two slimmest disposable flexible ureteroscopes: 7.5 Fr Indoscope sleek (Bioradmedisys™, Pune, India) and 7.5 Fr Uscope PU3033A (Pusen, Zhuhai, China) in terms of their in vivo performance for the patients who underwent Retrograde Intrarenal surgery (RIRS). This prospective study also investigates the difference between post-operative outcomes between the two scopes.
Material and methods
A prospective single-center randomized study was conducted at Muljibhai Patel Urological Hospital, Nadiad, India from September 2021 to April 2022. Patients with radiological evidence of renal stones on abdominal CT scan and acceptable for RIRS procedure according to European Association of Urology (EAU) guidelines were registered in this prospective study. Patients 18 years or older were included. All procedures were performed by the two endourologists having experience of more than 200 RIRS procedures.
Institutional ethical board approval for this project was authorized. This study was conducted in accordance with the Declaration of Helsinki. Informed written consent was obtained from all participants in this study.
Exclusion criteria were age less than 18 or more than 75 years, anatomical anomalies (Horseshoe kidney, UPJO, Ureteric stricture), evidence of renal insufficiency, prior placement of double J stent, evidence of acute infection, presence of cardiovascular or pulmonary comorbidities.
Pre-operative, intra-operative, and post-operative parameters were evaluated. At the end of each case in vivo, visibility and maneuverability were graded on a 5-point Likert scale (1, bad; 2, poor; 3, fair; 4, good; 5, very good) by the operating surgeon. The 5-point Likert scale assessment was based on the Doizi et al. study where image quality and maneuverability of Lithovue™ scope were rated with the same scale [10]. Each patient underwent a urine examination for culture and sensitivity 72 h before RIRS before starting antibiotics prophylaxis.
Patients were randomized into two groups: Group A: 30 patients treated with RIRS with 7.5 Fr Indoscope (Bioradmedisys™, Pune, India); Group B: Remaining 30 patients treated with RIRS with 7.5 Fr Uscope PU3033A (Pusen, Zhuhai, China). Randomization was done as a result of computer-generated random numbers and the list was kept hidden with a third party which was opened at the time of surgery.
All procedures in respective groups were executed using fURS in a never used condition. The scopes were introduced into the pelvic calyceal system via Ureteral Access Sheath (9.5/11.5 Fr Flexor® COOK® Medical, USA or 10/12 ReTrace® Coloplast, USA) or without ureteral access sheath. The entire kidney collecting system was observed and assessed before initiating the stone dusting with a 200 μm laser fiber. Depending on the case, the lower pole stones were shifted to the upper poles utilizing a nitinol basket for treatment. A holmium laser, with an energy level of 0.8–1.0 J and a frequency of 8–12 Hz, was used for lasing the stone.
At one month stone clearance was evaluated with X-ray KUB and USG KUB.
Data were analyzed using Statistical Package for the Social Sciences (SPSS) software (version 23.0, Armonk, NY: BM crp). Continuous variables were analyzed with Mann–Whitney U tests and two proportion tests were used for other parameters.
Results
A total of 68 patients were enrolled for RIRS between September 2021 and April 2022. Eight patients were excluded: 3 patients had prior double J stent placed elsewhere, 2 patients did not sign the informed consent form, two patients had UTI, and one patient had deranged renal function. As a result, a total of 60 patients were taken for final analysis which was further prospectively randomized in two groups.
The patient's demographics and stone features were comparable as outlined in Table 1. Pre-operative serum creatinine was also comparable between the two arms.
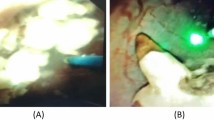
Intra-operatively Ureteral Access Sheath (UAS) could not be placed in two and three patients in Group "A" and "B," respectively, in which a flexible ureteroscope was inserted via the "No touch" technique. The pre-operative vision was sharp in each case (p = Not significant). Intra-operative representative image with 200-micron holmium laser fiber in a working channel, from both fURS, is shown in Fig. 1. There was a significant difference in the visibility score (4.63 ± 0.56 Vs. 3.83 ± 0.46; p < 0.001); however, maneuverability score was comparable (p = 0.82) between both groups. (Figs. 2, 3) (Table 2).

Comparative images from a Indoscope sleek and b Pusen PU3033A in the different patients. Images were recorded from Stryker and Pusen monitor, respectively

Comparison between visibility score between two groups

Comparison between maneuverability score between two groups
Scope failure was noticed in one case of Group "B" where the deflection mechanism was damaged in the terminal stage of lasing of stone. To report the complication rate, the Modified Clavien Classification System was used. Three patients in Group "A" and four patients in Group "B" had UTI and needed culture-sensitive antibiotic treatment. The stone-free rate at one month of follow-up was 93.33% and 86.67% in Group "A" and "B," respectively (p = 0.56). (Table 3).
Discussion
As per the EAU guidelines, RIRS is advocated as the preferred treatment choice for renal stones less than 2 cm and is the preferred option for renal stones between 1 and 2 cm [11]. Advent of su-fURS has conquered the limitations of conventional reusable scope in terms of high initial purchase cost, high maintenance cost, and risk of cross infection. Many studies compared su-fURS with reusable fURS in terms of image quality (resolution, field of view, image distortion) and performance (maneuverability, deflection angle, flow rate) in both in vitro and in vivo milieu [12, 13].
Meng et al. in their meta-analysis of 1020 patients concluded that su-fURS had similar effectiveness and better security for treating upper urinary calculi than reusable fURS [5]. The majority of available su-fURSs have an outer diameter of 9.5 Fr which demands insertion of wide caliber Ureteral Access Sheath (UAS). Auxiliary procedures like ureteric balloon dilatation or forceful mechanical dilatation may be performed for large UAS insertion, which can lead to ischemic injury to the ureteric wall and stenosis [14]. Sometimes pre-operative double J stent for a few days, and thus, staging the surgery is required due to the non-negotiability of fURS till stone [15].
With the advent of technical advancement, many manufacturers have introduced 7.5 Fr-outer shaft diameter su-fURS, keeping the working channel of 3.6 Fr, the same as large caliber 9.5Fr su-fURS. These scopes can be passed using small-diameter UAS or via the "No touch technique" [9]. In our study, two and three patients in Group "A" and "B," respectively, underwent Flexible ureteroscope insertion via “No touch” technique as in these cases ureteral access sheath could not be negotiated inside the narrow ureter.
Hudson et al. concluded that the ideal outer diameter for passage of a flexible ureteroscope with minimum need for ureteric dilatation is 7.4Fr [8]. Pusen introduced PU3033A scope with an outer shaft diameter of 7.5 Fr and subsequently Indoscope Sleek with an outer diameter of 7.5 Fr by Bioradmedisys™ was introduced.
There are some limitations in this study. It is a single-center study with a small sample size. We did not compare the cost-effectiveness between both scopes and did not compare with reusable flexible ureteroscopes.
Conclusion
We conclude that Indoscope Sleek scope outperforms Pusen PU3033A in terms of visibility, but they are comparable in rest of the clinical setting with similar outcome and complications.
References
Emiliani E, Traxer O (2017) Single use and disposable flexible ureteroscopes. Curr Opin Urol 27(2):176–181
Proietti S, Dragos L, Molina W, Doizi S, Giusti G, Traxer O (2016) Comparison of new single-use digital flexible ureteroscope versus nondisposable fiber optic and digital ureteroscope in a cadaveric model. J Endourol 30(6):655–659
Tom WR, Wollin DA, Jiang R, Radvak D, Simmons WN, Preminger GM, Lipkin ME (2017) Next-generation single-use ureteroscopes: an in vitro comparison. J Endourol 31(12):1301–1306
Dragos LB, Somani BK, Keller EX, De Coninck VM, Herrero MR, Kamphuis GM, Bres-Niewada E, Sener ET, Doizi S, Wiseman OJ, Traxer O (2019) Characteristics of current digital single-use flexible ureteroscopes versus their reusable counterparts: an in-vitro comparative analysis. Transl Androl Urol 8(Suppl 4):S359
Meng C, Peng L, Li J, Li Y, Li J, Wu J (2021) Comparison between single-use flexible ureteroscope and reusable flexible ureteroscope for upper urinary calculi: a systematic review and meta-analysis. Front Surg. 8:691170
Li Y, Chen J, Zhu Z, Zeng H, Zeng F, Chen Z, Yang Z, Cui Y, Chen H, Li Y (2021) Comparison of single-use and reusable flexible ureteroscope for renal stone management: a pooled analysis of 772 patients. Transl Androl Urol 10(1):483
Shvero A, Herzberg H, Zilberman D, Mor Y, Winkler H, Kleinmann N (2019) Is it safe to use a ureteral access sheath in an unstented ureter? BMC Urol 19(1):1–6
Hudson RG, Conlin MJ, Bagley DH (2005) Ureteric access with flexible ureteroscopes: effect of the size of the ureteroscope. BJU Int 95(7):1043–1044
Geavlete B, Cozma C, Geavlete P (2021) The, “no-touch” technique in the flexible ureteroscopic approach of renal stones. J Med Life 14(4):481
Doizi S, Kamphuis G, Giusti G, Andreassen KH, Knoll T, Osther PJ, Scoffone C, Pérez-Fentes D, Proietti S, Wiseman O, de la Rosette J (2017) First clinical evaluation of a new single-use flexible ureteroscope (LithoVue™): a European prospective multicentric feasibility study. World J Urol 35(5):809–818
Turk C, NeIsius A, Petrik A (2020) EAU guidelines on urolithiasis. EAU Guidelines. Edn. presented at the EAU Annual Congress Amsterdam
Wiseman O, Keeley F, Traxer O, Giusti G, Lipkin M, Preminger G (2016) MP51–03 comparison of a new single-use digital flexible ureteroscope (lithovue tm) to a non-disposable fibre-optic flexible ureteroscope in a live porcine model. J Urol 195(4):e682
Eisel M, Strittmatter F, Ströbl S, Freymüller C, Pongratz T, Sroka R (2020) Comparative investigation of reusable and single–use flexible endoscopes for urological interventions. Sci Rep 10(1):1–1
Cetti RJ, Biers S, Keoghane SR (2011) The difficult ureter: what is the incidence of pre-stenting? Ann R Coll Surg Engl 93(1):31–33
Salvadó JA, Olivares R, Cabello JM et al (2018) Retrograde intrarenal surgery using the single – use flexible ureteroscope uscope 3022 (PusenTM): evaluation of clinical results. Cent European J Urol 71:202–207
Author information
Authors and Affiliations
Contributions
SA was involved in protocol/project development, data collection, data analysis, and manuscript writing/editing. PS wrote the manuscript. AGS and RBS edited the manuscript. APG contributed to manuscript writing/editing. MRD performed data analysis and manuscript editing.
Corresponding author
Ethics declarations
Conflict of interest
None of the contributing authors have any conflicts of interest, including specific financial interests and relationships and affiliations relevant to the subject matter or materials discussed in this manuscript.
Research involving human participants and/or animals
This article does not contain any studies with animals performed by any of the authors. This study involves human subjects, after proper Institutional ethical committee presentation and clearance. This study has been performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in this study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Agrawal, S., Survase, P., Singh, A.G. et al. Initial experience of comparison between two slimmest single-use flexible ureteroscopes: Indoscope Sleek (Bioradmedisys™) Versus Uscope PU3033A (Pusen™): A single-center prospective study. World J Urol 41, 2817–2821 (2023). https://doi.org/10.1007/s00345-023-04532-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00345-023-04532-7